Inter-Rater Reliability, Concurrent Validity and Sensitivity of Current Methods to Assess Trunk Function in Boccia Players with Cerebral Palsy





Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure
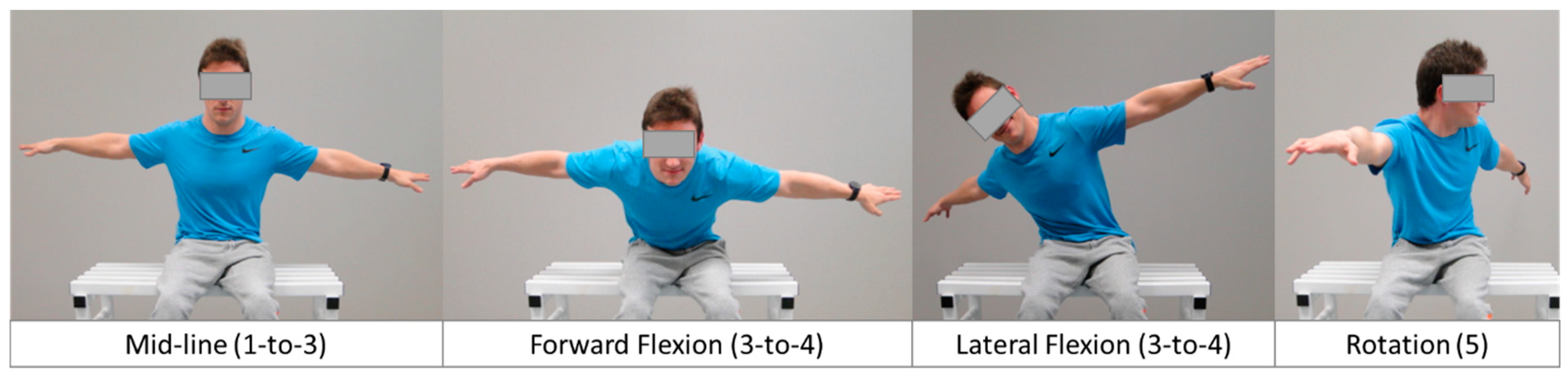
2.3. BISFed TFS
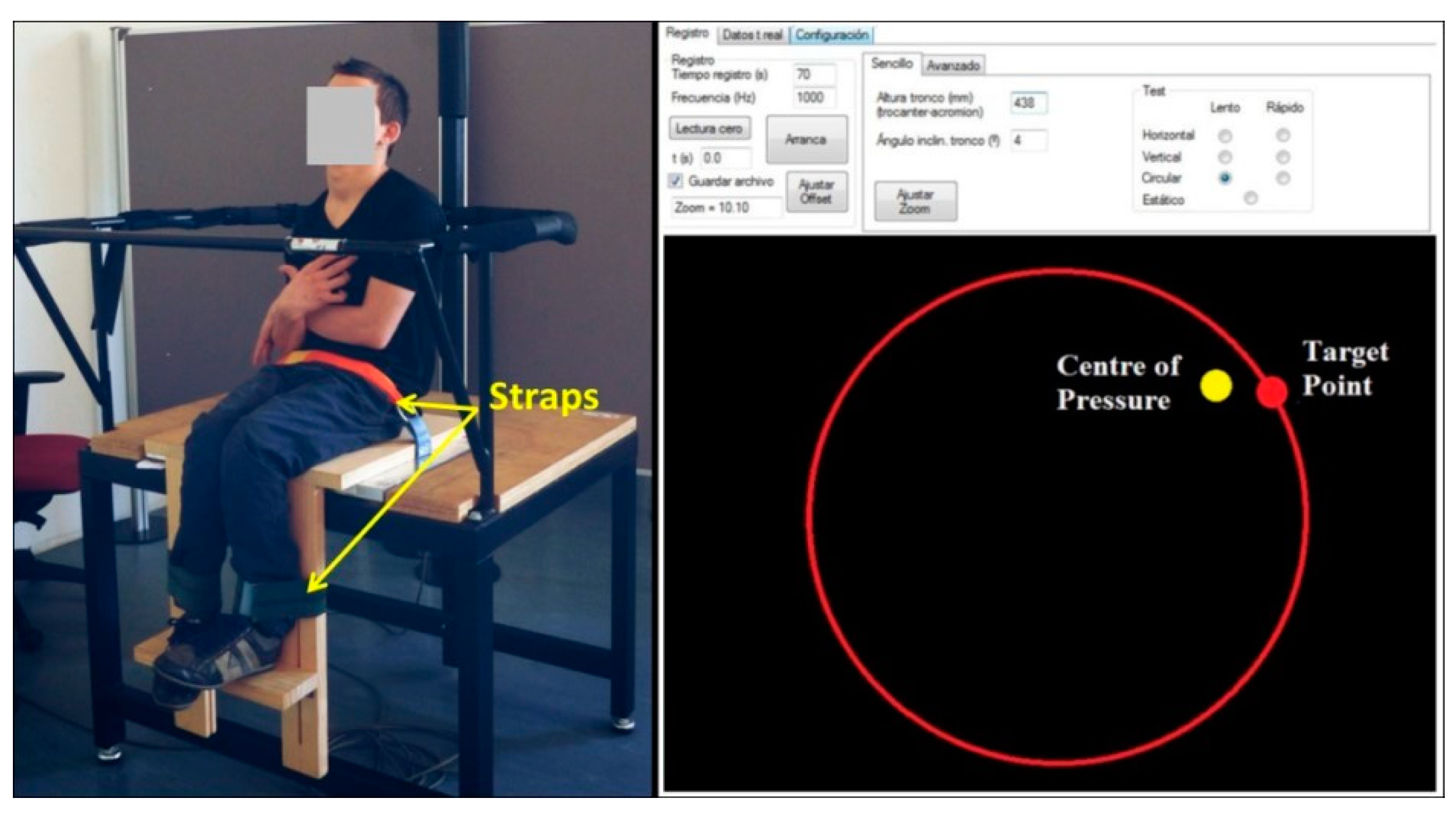
2.4. Posturographic Test Battery
Posturography Data Reduction
2.5. Statistical Analysis
2.5.1. Inter-Rater Reliability
2.5.2. Validity
2.5.3. Sensitivity
3. Results
3.1. Inter-Rater Reliability
3.2. Concurrent Validity between BISFed TFS and Posturography
3.3. Sensitivity of the BISFed TFS
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Boccia International Sports Federation (BISFed). Boccia Classification Rules, Fourth Edition. Available online: http://www.bisfed.com/wp-content/uploads/2018/12/Boccia-Classification-Rules-4th-Edition-October-2018.pdf (accessed on 22 February 2020).
- Tweedy, S.M.; Vanlandewijck, Y.C. International Paralympic Committee position stand--background and scientific principles of classification in Paralympic sport. Br. J. Sports Med. 2009, 45, 259–269. [Google Scholar] [CrossRef] [PubMed]
- Szopa, A.; Domagalska-Szopa, M. Postural stability in children with hemiplegia estimated for three postural conditions: Standing, sitting and kneeling. Res. Dev. Disabil. 2015, 39, 67–75. [Google Scholar] [CrossRef]
- Huang, P.-C.; Pan, P.-J.; Ou, Y.-C.; Yu, Y.-C.; Tsai, Y.-S. Motion analysis of throwing Boccia balls in children with cerebral palsy. Res. Dev. Disabil. 2014, 35, 393–399. [Google Scholar] [CrossRef]
- Miyake, Y.; Kobayashi, R.; Kelepecz, D.; Nakajima, M. Core exercises elevate trunk stability to facilitate skilled motor behavior of the upper extremities. J. Bodyw. Mov. Ther. 2013, 17, 259–265. [Google Scholar] [CrossRef]
- Palisano, R.; Rosenbaum, P.; Walter, S.; Russell, D.; Wood, E.; Galuppi, B. Development and reliability of a system to classify gross motor function in children with cerebral palsy. Dev. Med. Child Neurol. 1997, 39, 214–223. [Google Scholar] [CrossRef]
- Barbado, D.; Barbado, L.C.; Elvira, J.; Van Dieën, J.; Vera-Garcia, F.J. Sports-related testing protocols are required to reveal trunk stability adaptations in high-level athletes. Gait Posture 2016, 49, 90–96. [Google Scholar] [CrossRef] [Green Version]
- Barbado, D.; Reina, R.; Roldán, A.; McCulloch, K.; Campayo-Piernas, M.; Vera-Garcia, F.J. How much trunk control is affected in adults with moderate-to-severe cerebral palsy? J. Biomech. 2019, 82, 368–374. [Google Scholar] [CrossRef]
- Lin, D.; Seol, H.; Nussbaum, M.A.; Madigan, M.L. Reliability of COP-based postural sway measures and age-related differences. Gait Posture 2008, 28, 337–342. [Google Scholar] [CrossRef]
- Borg, F.G.; Laxåback, G. Entropy of balance - some recent results. J. Neuroeng. Rehabilitation 2010, 7, 38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Dieën, J.; Koppes, L.L.J.; Twisk, J. Postural sway parameters in seated balancing; their reliability and relationship with balancing performance. Gait Posture 2010, 31, 42–46. [Google Scholar] [CrossRef] [PubMed]
- Hancock, G.R.; Butler, M.S.; Fischman, M.G. On the Problem of Two-Dimensional Error Scores: Measures and Analyses of Accuracy, Bias, and Consistency. J. Mot. Behav. 1995, 27, 241–250. [Google Scholar] [CrossRef] [PubMed]
- Witz, K.; Hinkle, D.E.; Wiersma, W.; Jurs, S.G. Applied Statistics for the Behavioral Sciences. J. Educ. Stat. 1990, 15, 84. [Google Scholar] [CrossRef]
- Hedges, L.V.; Olkin, I. Statistical Methods for Meta-Analysis; Academic Press: San Diego, CA, USA, 1985. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Lawrence Earlbaum Associates: Hillsdale, IL, USA, 1988. [Google Scholar]
- Hopkins, W.G.; Marshall, S.; Batterham, A.; Hanin, J. Progressive Statistics for Studies in Sports Medicine and Exercise Science. Med. Sci. Sports Exerc. 2009, 41, 3–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, W.; Zeng, N.; Wang, N. Sensitivity, specificity, accuracy, associated confidence interval and ROC analysis with practical SAS implementations. In NESUG Proceedings: Health Care and Life Sciences; SAS Institute Inc.: Baltimore, MA, USA, 2010; Volume 19, pp. 67–76. [Google Scholar]
- International Paralympic Committee. IPC´s Athletes Classification Code. Available online: https://www.paralympic.org/sites/default/files/document/170704160235698_2015_12_17%2BClassification%2BCode_FINAL2_0.pdf (accessed on 17 November 2019).
- Pham, H.P.; Eidem, A.; Hansen, G.; Nyquist, A.; Vik, T.; Sæther, R. Validity and Responsiveness of the Trunk Impairment Scale and Trunk Control Measurement Scale in Young Individuals with Cerebral Palsy. Phys. Occup. Ther. Pediatr. 2016, 36, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Santos, P.B.R.; Vigario, P.; Mainenti, M.R.M.; Ferreira, A.S.; Lemos, T. Seated limits-of-stability of athletes with disabilities with regard to competitive levels and sport classification. Scand. J. Med. Sci. Sports 2017, 27, 2019–2026. [Google Scholar] [CrossRef]
- Roldan, A.; Sabido, R.; Barbado, D.; Caballero, C.; Reina, R. Manual Dexterity and Intralimb Coordination Assessment to Distinguish Different Levels of Impairment in Boccia Players with Cerebral Palsy. Front. Neurol. 2017, 8, 582. [Google Scholar] [CrossRef]
- Chruscikowski, E.; Fry, N.R.D.; Noble, J.J.; Gough, M.; Shortland, A.P. Selective motor control correlates with gait abnormality in children with cerebral palsy. Gait Posture 2017, 52, 107–109. [Google Scholar] [CrossRef] [Green Version]
- Pavão, S.L.; Santos, A.N.; Oliveira, A.B.; Rocha, N.A.C.F. Postural control during sit-to-stand movement and its relationship with upright position in children with hemiplegic spastic cerebral palsy and in typically developing children. Braz. J. Phys. Ther. 2015, 19, 18–25. [Google Scholar] [CrossRef] [Green Version]
- Reina, R.; Domínguez-Díez, M.; Urban, T.; Roldan, A. Throwing distance constraints regarding kinematics and accuracy in high-level boccia players. Sci. Sports 2018, 33, 299–306. [Google Scholar] [CrossRef]
- Mason, B.S.; Van Der Woude, L.H.V.; Goosey-Tolfrey, V.L. The Ergonomics of Wheelchair Configuration for Optimal Performance in the Wheelchair Court Sports. Sports Med. 2012, 43, 23–38. [Google Scholar] [CrossRef] [Green Version]
- Ben Kibler, W.; Press, J.; Sciascia, A. The role of core stability in athletic function. Sports Med. 2006, 36, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Hyde, A.; Hogarth, L.; Sayers, M.G.; Beckman, E.; Connick, M.J.; Tweedy, S.; Burkett, B. The Impact of an Assistive Pole, Seat Configuration, and Strength in Paralympic Seated Throwing. Int. J. Sports Physiol. Perform. 2017, 12, 977–983. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Connick, M.J.; Beckman, E.; Vanlandewijck, Y.C.; A Malone, L.; Blomqvist, S.; Tweedy, S.M. Cluster analysis of novel isometric strength measures produces a valid and evidence-based classification structure for wheelchair track racing. Br. J. Sports Med. 2017, 52, 1123–1129. [Google Scholar] [CrossRef] [PubMed]
- Altmann, V.; Groen, B.; Hart, A.L.; Vanlandewijck, Y.C.; Keijsers, N.L.W. Classifying trunk strength impairment according to the activity limitation caused in wheelchair rugby performance. Scand. J. Med. Sci. Sports 2017, 28, 649–657. [Google Scholar] [CrossRef] [PubMed]
- Ozinga, S.J.; Koop, M.M.; Linder, S.M.; Machado, A.G.; Dey, T.; Alberts, J.L. Three-dimensional evaluation of postural stability in Parkinson’s disease with mobile technology. Neurorehabilit. 2017, 41, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Barbado, D.; Irles-Vidal, B.; Prat-Luri, A.; García-Vaquero, M.P.; Vera-Garcia, F.J. Training intensity quantification of core stability exercises based on a smartphone accelerometer. PLoS ONE 2018, 13, e0208262. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Demographic Variables | BC1 n = 13 | BC2 n = 23 | Overall n = 36 |
|---|---|---|---|
| Age (year) | 39.00 ± 13.20 | 34.50 ± 14.14 | 36.33 ± 13.69 |
| Body Mass (kg) | 53.65 ± 10.96 | 51.56 ± 11.89 | 52.02 ± 11.04 |
| Trunk Height (cm) | 43.50 ± 2.12 | 54.67 ± 7.36 | 52.64 ± 8.02 |
| Impairment type (muscle tone) | |||
| Spasticity | 7 (53.85) | 13 (56.52) | 20 (55.56) |
| Athetosis/Dystonia | 1 (7.69) | 4 (17.39) | 5 (13.89) |
| Mixed (spastic/athetoid) | 5 (38.46) | 6 (26.09) | 11 (30.56) |
| Sex | |||
| Male, n (%) | 6 (46.15) | 14 (60.87) | 20 (55.56) |
| Female, n (%) | 7 (53.85) | 9 (39.13) | 16 (44.44) |
| Competition Level | |||
| Regional, n (%) | 9 (69.23) | 10 (43.48) | 19 (52.78) |
| National, n (%) | 3 (23.08) | 11 (47.83) | 14 (38.89) |
| International, n (%) | 1 (7.69) | 2 (8.69) | 3 (8.33) |
| GMFCS (level), median (range) | 4 (4–4) | 4 (2–4) | 4 (2–4) |
| Level II, n (%) | -- | 6 (26.09) | 6 (16.67) |
| Level III, n (%) | -- | 5 (21.74) | 5 (13.89) |
| Level IV, n (%) | 13 (100) | 12 (52.17) | 25 (69.44) |
| Demographic Variables | Classifier/Tester #1 | Classifier/Tester #2 |
|---|---|---|
| Age (year) | 48 | 39 |
| Sex | Female | Male |
| Background | Physiotherapist | Sports Sciences PhD |
| BISFed Classification Level | Level 3 | Level 3 |
| Classification Experience in Boccia | ||
| International (year) | 12 | 6 |
| National (year) | 22 | 16 |
| Experience in other Paralympic sports | Cerebral Palsy Football | Cerebral Palsy Football |
| World Para Athletics | World Para Athletics | |
| Para Equestrian | Wheelchair Slalom |
| BISFed TFS | SNVF | SVF | DML | DAP | DC | Comp. Static | Comp. Dynamic | |
|---|---|---|---|---|---|---|---|---|
| BISFed TFS | -- | −0.23 | −0.31 | −0.38 * | −0.35 | −0.46 * | −0.27 | −0.51 ** |
| SNVF | 0.85 ** | 0.46 ** | 0.53 ** | 0.40 * | 0.97 ** | 0.61 ** | ||
| SVF | 0.39 * | 0.54 ** | 0.36 | 0.95 ** | 0.58 ** | |||
| DML | 0.90 ** | 0.73 ** | 0.45 ** | 0.94 ** | ||||
| DAP | 0.79 ** | 0.56 ** | 0.96 ** | |||||
| DC | 0.40 * | 0.92 ** | ||||||
| Comp. Static | 0.63 ** | |||||||
| Comp. Dynamic |
| Variable | NBC1 + NBC2 = N | BC1 (Mean ± SD) | BC2 (Mean ± SD) | F | p | dg |
|---|---|---|---|---|---|---|
| BISFed TFS (unitless) | 13 + 23 = 36 | 2.2 ± 1.1 | 2.3 ± 1.1 | 0.02 | 0.892 | 0.05 |
| SNVF (mm) | 13 + 23 = 36 | 7.9 ± 6.8 | 3.4 ± 2.0 | 8.93 | 0.005 | 1.01 |
| SVF (mm) | 13 + 23 = 36 | 6.2 ± 4.9 | 2.7 ± 2.3 | 8.43 | 0.006 | 0.99 |
| DML (mm) | 12 + 22 = 34 | 8.3 ± 4.7 | 7.9 ± 4.3 | 0.06 | 0.811 | 0.09 |
| DAP (mm) | 12 + 20 = 32 | 8.8 ± 4.3 | 7.5 ± 3.8 | 0.81 | 0.374 | 0.32 |
| DC (mm) | 11 + 15 = 26 | 11.7 ± 4.4 | 8.6 ± 4.5 | 2.96 | 0.098 | 0.67 |
| Composite Static (mm) | 13 + 23 = 36 | 7.0 ± 5.7 | 3.0 ± 1.8 | 9.62 | 0.004 | 1.06 |
| Composite Dynamic (mm) | 11 + 15 = 26 | 9.4 ± 4.1 | 7.3 ± 3.4 | 1.97 | 0.173 | 0.55 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roldan, A.; Barbado, D.; Vera-Garcia, F.J.; Sarabia, J.M.; Reina, R. Inter-Rater Reliability, Concurrent Validity and Sensitivity of Current Methods to Assess Trunk Function in Boccia Players with Cerebral Palsy. Brain Sci. 2020, 10, 130. https://doi.org/10.3390/brainsci10030130
Roldan A, Barbado D, Vera-Garcia FJ, Sarabia JM, Reina R. Inter-Rater Reliability, Concurrent Validity and Sensitivity of Current Methods to Assess Trunk Function in Boccia Players with Cerebral Palsy. Brain Sciences. 2020; 10(3):130. https://doi.org/10.3390/brainsci10030130
Chicago/Turabian StyleRoldan, Alba, David Barbado, Francisco J. Vera-Garcia, José M. Sarabia, and Raul Reina. 2020. "Inter-Rater Reliability, Concurrent Validity and Sensitivity of Current Methods to Assess Trunk Function in Boccia Players with Cerebral Palsy" Brain Sciences 10, no. 3: 130. https://doi.org/10.3390/brainsci10030130
APA StyleRoldan, A., Barbado, D., Vera-Garcia, F. J., Sarabia, J. M., & Reina, R. (2020). Inter-Rater Reliability, Concurrent Validity and Sensitivity of Current Methods to Assess Trunk Function in Boccia Players with Cerebral Palsy. Brain Sciences, 10(3), 130. https://doi.org/10.3390/brainsci10030130