Insomnia Might Influence the Thickness of Choroid, Retinal Nerve Fiber and Inner Plexiform Layer


Abstract
:1. Introduction
2. Materials and Methods
2.1. Procedure
2.2. Clinical Measurments
2.3. Statistical Analysis
3. Results
3.1. Sample Characteristics
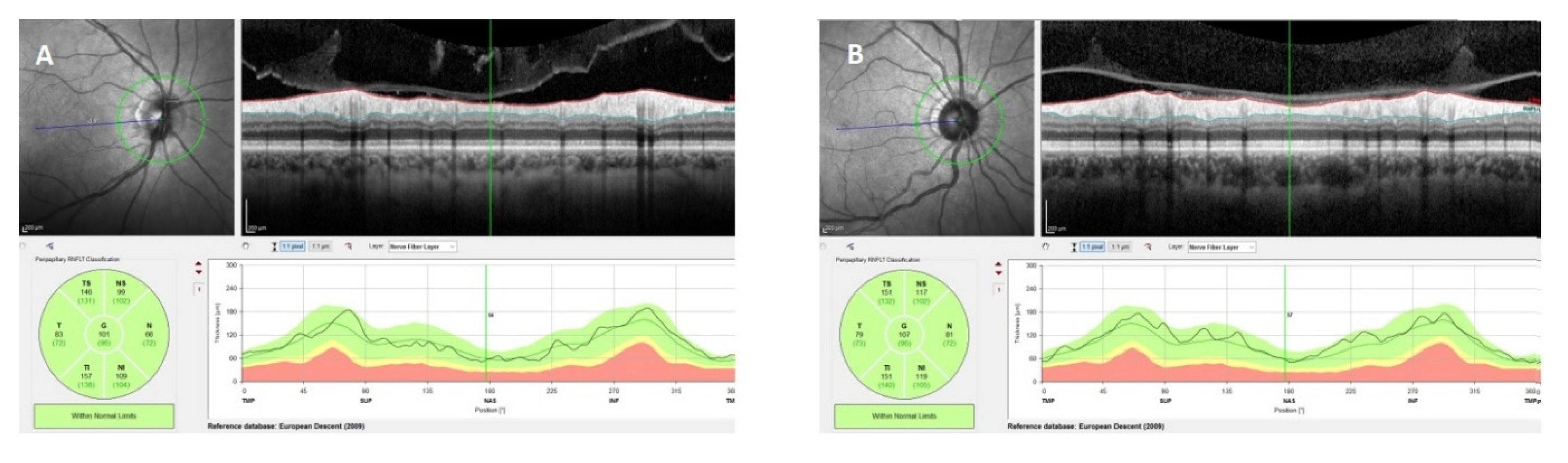
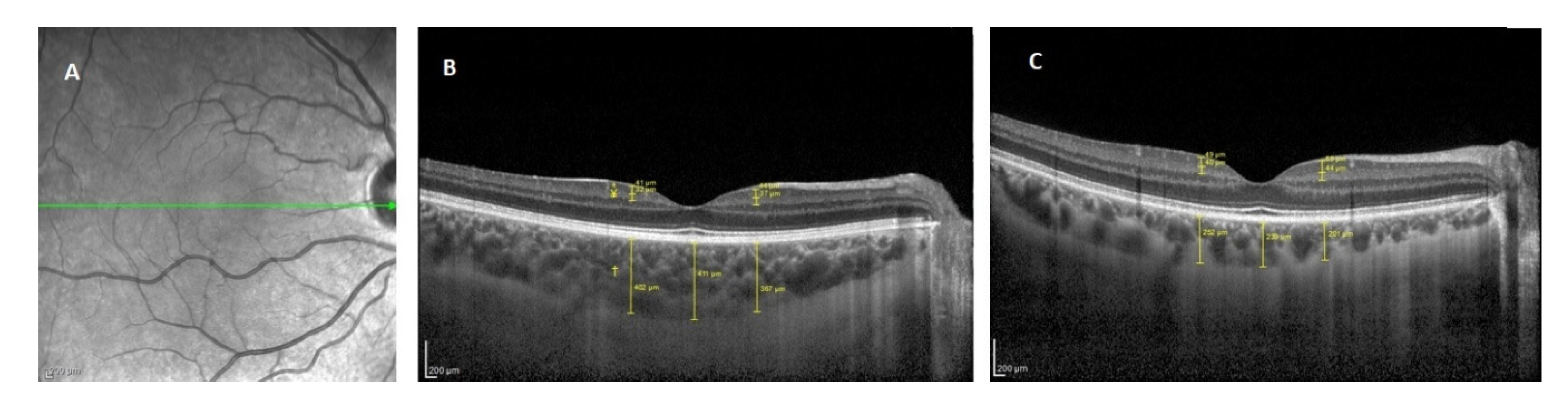
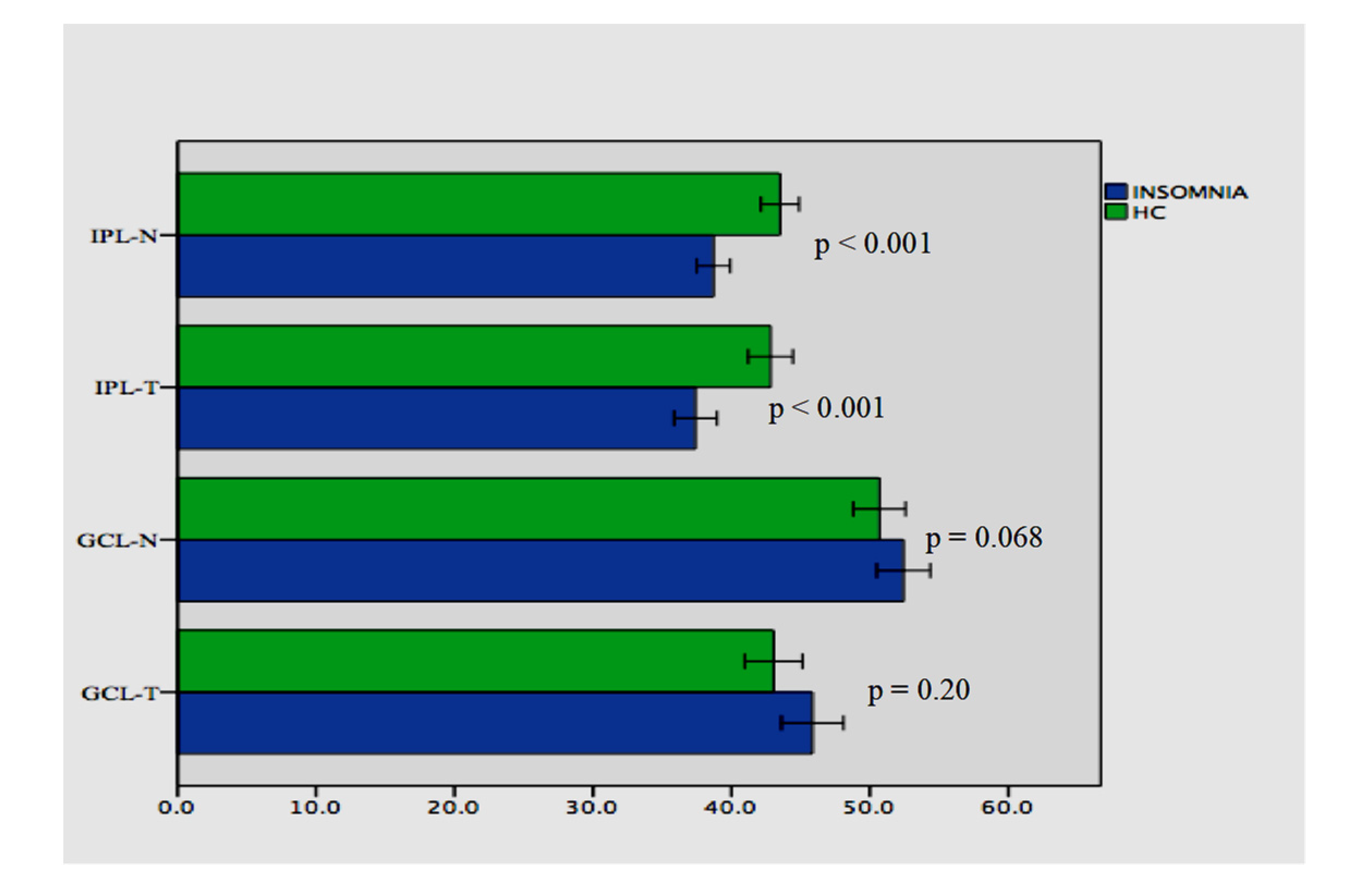
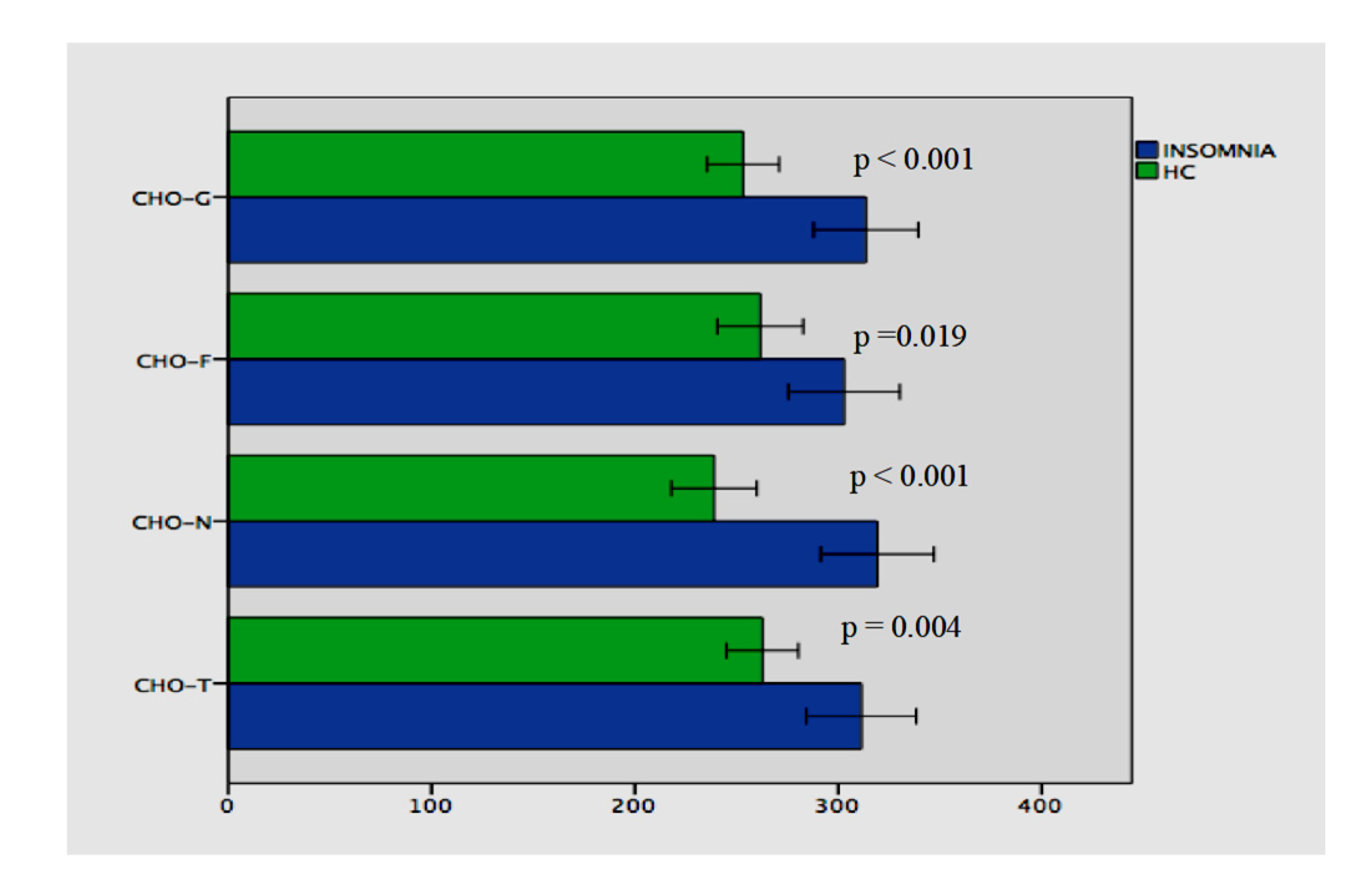
3.2. Group Comparisons according to the Optical Coherence Tomography Results
3.3. Correlation of the Clinical Variables with the Optical Coherence Tomography Measurements
3.4. Stepwise Linear Regression Results
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Riemann, D.; Nissen, C.; Palagini, L.; Otte, A.; Perlis, M.L.; Spiegelhalder, K. The neurobiology, investigation, and treatment of chronic insomnia. Lancet. Neurol. 2015, 14, 547–558. [Google Scholar] [CrossRef]
- Ohayon, M.M. Epidemiology of insomnia: What we know and what we still need to learn. Sleep Med. Rev. 2002, 6, 97–111. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Mendoza, J.; Vgontzas, A.N. Insomnia and its impact on physical and mental health. Curr. Psychiatry Rep. 2013, 15, 418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chu, E.M.; Kolappan, M.; Barnes, T.R.E.; Joyce, E.M.; Ron, M.A. A window into the brain: An in vivo study of the retina in schizophrenia using optical coherence tomography. Psychiatry Res. 2012, 203, 89–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Appaji, A. Retinal vascular tortuosity in schizophrenia and bipolar disorder. Schizophr. Res. 2019, 212, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Ko, G.Y. Circadian regulation in the retina: From molecules to network. Eur. J. Neurosci. 2018, 51, 194–216. [Google Scholar] [CrossRef] [Green Version]
- Ruan, G.X.; Zhang, D.Q.; Zhou, T.; Yamazaki, S.; McMahon, D.G. Circadian organization of the mammalian retina. Proc. Natl. Acad. Sci. USA 2006, 103, 9703–9708. [Google Scholar] [CrossRef] [Green Version]
- DeVera, C.; Baba, K.; Tosini, G. Retinal Circadian Clocks are Major Players in the Modulation of Retinal Functions and Photoreceptor Viability. Yale J. Biol. Med. 2019, 92, 233–240. [Google Scholar]
- McMahon, D.G.; Iuvone, P.M.; Tosini, G. Circadian organization of the mammalian retina: From gene regulation to physiology and diseases. Prog. Retin. Eye Res. 2014, 39, 58–76. [Google Scholar] [CrossRef] [Green Version]
- Mukherjee, C.; Al-Fahad, Q.; Elsherbiny, S. The role of optical coherence tomography in therapeutics and conditions, which primarily have systemic manifestations: A narrative review. Ther. Adv. Ophthalmol. 2019, 11, 2515841419831155. [Google Scholar] [CrossRef]
- Gordon-Lipkin, E.; Chodkowski, B.; Reich, D.S.; Smith, S.A.; Pulicken, M.; Balcer, L.J.; Frohman, E.M.; Cutter, G.; Calabresi, P.A. Retinal nerve fiber layer is associated with brain atrophy in multiple sclerosis. Neurology 2007, 69, 1603–1609. [Google Scholar] [CrossRef] [PubMed]
- Grazioli, E.; Zivadinov, R.; Weinstock-Guttman, B.; Lincoff, N.; Baier, M.; Wong, J.R.; Hussein, S.; Cox, J.L.; Hojnacki, D.; Ramanathan, M. Retinal nerve fiber layer thickness is associated with brain MRI outcomes in multiple sclerosis. J. Neurol. Sci. 2008, 268, 12–17. [Google Scholar] [CrossRef] [PubMed]
- Silverstein, S.M.; Paterno, D.; Cherneski, L.; Green, S. Optical coherence tomography indices of structural retinal pathology in schizophrenia. Psychol. Med. 2018, 48, 2023–2033. [Google Scholar] [CrossRef] [PubMed]
- Lizano, P.; Bannai, D.; Lutz, O.; Kim, L.A.; Miller, J.; Keshavan, M. A Meta-analysis of Retinal Cytoarchitectural Abnormalities in Schizophrenia and Bipolar Disorder. Schizophr. Bull. 2019, 46, 43–53. [Google Scholar] [CrossRef] [Green Version]
- Yildiz, M.; Alim, S.; Batmaz, S.; Demir, S.; Songur, E.; Ortak, H.; Demirci, K. Duration of the depressive episode is correlated with ganglion cell inner plexifrom layer and nasal retinal fiber layer thicknesses: Optical coherence tomography findings in major depression. Psychiatry Res. Neuroimaging 2016, 251, 60–66. [Google Scholar] [CrossRef]
- Moschos, M.M.; Gonidakis, F.; Varsou, E.; Markopoulos, I.; Rouvas, A.; Ladas, I.; Papadimitriou, G.N. Anatomical and functional impairment of the retina and optic nerve in patients with anorexia nervosa without vision loss. Br. J. Ophthalmol. 2011, 95, 1128–1133. [Google Scholar] [CrossRef]
- Palagini, L.; Bastien, C.H.; Marazziti, D.; Ellis, J.G.; Riemann, D. The key role of insomnia and sleep loss in the dysregulation of multiple systems involved in mood disorders: A proposed model. J. Sleep Res. 2019, 28, e12841. [Google Scholar] [CrossRef]
- Logan, R.W.; McClung, C.A. Rhythms of life: Circadian disruption and brain disorders across the lifespan. Nat. Rev. Neurosci. 2019, 20, 49–65. [Google Scholar] [CrossRef]
- Katz, D.A.; McHorney, C.A. Clinical correlates of insomnia in patients with chronic illness. Arch. Int. Med. 1998, 158, 1099–1107. [Google Scholar] [CrossRef] [Green Version]
- Lane, J.M.; Jones, S.E.; Dashti, H.S.; Wood, A.R.; Aragam, K.G.; van Hees, V.T.; Strand, L.B.; Winsvold, B.S.; Wang, H.; Bowden, J.; et al. Biological and clinical insights from genetics of insomnia symptoms. Nat. Genet. 2019, 51, 387–393. [Google Scholar] [CrossRef] [Green Version]
- Gracitelli, C.P.; Duque-Chica, G.L.; Roizenblatt, M.; Moura, A.L.; Nagy, B.V.; de Ragot, M.G.; Borba, P.D.; Teixeira, S.H.; Tufik, S.; Ventura, D.F.; et al. Intrinsically photosensitive retinal ganglion cell activity is associated with decreased sleep quality in patients with glaucoma. Ophthalmology 2015, 122, 1139–1148. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.Y.; Riangwiwat, T.; Rattanawong, P.; Nesmith, B.L.W.; Deobhakta, A. Association Of Obstructive Sleep Apnea With Central Serous Chorioretinopathy And Choroidal Thickness: A Systematic Review and Meta-Analysis. Retina 2018, 38, 1642–1651. [Google Scholar] [CrossRef] [PubMed]
- Schaal, S.; Sherman, M.P.; Nesmith, B.; Barak, Y. Untreated Obstructive Sleep Apnea Hinders Response to Bevacizumab in Age-Related Macular Degeneration. Retina 2016, 36, 791–797. [Google Scholar] [CrossRef] [PubMed]
- Xin, C.; Wang, J.; Zhang, W.; Lang, L.; Peng, X. Retinal and choroidal thickness evaluation by SD-OCT in adults with obstructive sleep apnea-hypopnea syndrome (OSAS). Eye 2014, 28, 415–421. [Google Scholar] [CrossRef] [Green Version]
- Bastien, C.H.; Vallieres, A.; Morin, C.M. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001, 2, 297–307. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F., III; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Malhotra, R.K. Neurodegenerative Disorders and Sleep. Sleep Med. Clin. 2018, 13, 63–70. [Google Scholar] [CrossRef]
- Ortuno-Lizaran, I.; Esquiva, G.; Beach, T.G.; Serrano, G.E.; Adler, C.H.; Lax, P.; Cuenca, N. Degeneration of human photosensitive retinal ganglion cells may explain sleep and circadian rhythms disorders in Parkinson’s disease. Acta Neuropathol. Commun. 2018, 6, 90. [Google Scholar] [CrossRef] [Green Version]
- Dinkin, M. Trans-synaptic Retrograde Degeneration in the Human Visual System: Slow, Silent, and Real. Curr. Neurol. Neurosci. Rep. 2017, 17, 16. [Google Scholar] [CrossRef]
- Jindahra, P.; Petrie, A.; Plant, G.T. Retrograde trans-synaptic retinal ganglion cell loss identified by optical coherence tomography. Brain 2009, 132 (Pt 3), 628–634. [Google Scholar] [CrossRef] [Green Version]
- Lugaresi, E. The thalamus and insomnia. Neurology 1992, 42 (Suppl. S6), 28–33. [Google Scholar]
- Liu, C.; Kong, X.Z.; Liu, X.; Zhou, R.; Wu, B. Long-term total sleep deprivation reduces thalamic gray matter volume in healthy men. Neuroreport 2014, 25, 320–323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spiegelhalder, K.; Regen, W.; Baglioni, C.; Riemann, D.; Winkelman, J.W. Neuroimaging studies in insomnia. Curr. Psychiatry Rep. 2013, 15, 405. [Google Scholar] [CrossRef] [PubMed]
- Kang, J.M.K.; Joo, S.W.; Son, Y.; Kim, H.K.; Ko, K.; Lee, J.S.; Kang, S. Low white-matter integrity between the left thalamus and inferior frontal gyrus in patients with insomnia disorder. J. Psychiatry Neurosci. 2018, 43, 366–374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koo, D.L.; Shin, J.H.; Lim, J.S.; Seong, J.K.; Joo, E.Y. Changes in subcortical shape and cognitive function in patients with chronic insomnia. Sleep Med. 2017, 35, 23–26. [Google Scholar] [CrossRef]
- Usrey, W.M.; Alitto, H.J. Visual Functions of the Thalamus. Annu. Rev. Vis. Sci. 2015, 1, 351–371. [Google Scholar] [CrossRef] [Green Version]
- La Morgia, C.; Di Vito, L.; Carelli, V.; Carbonelli, M. Patterns of Retinal Ganglion Cell Damage in Neurodegenerative Disorders: Parvocellular vs Magnocellular Degeneration in Optical Coherence Tomography Studies. Front. Neurol. 2017, 8, 710. [Google Scholar] [CrossRef]
- Polo, V.; Satue, M.; Gavin, A.; Vilades, E.; Orduna, E.; Cipres, M.; Garcia-Campayo, J.; Navarro-Gil, M.; Larrosa, J.M. Ability of swept source OCT to detect retinal changes in patients with bipolar disorder. Eye 2019, 33, 549–556. [Google Scholar] [CrossRef]
- Hogan, M.J.; Alvarado, J.A.; Weddell, J.E. Histology of the Human Eye; An atlas and textbook; Saunders: Philadelphia, PA, USA, 1971. [Google Scholar]
- Samani, N.N.; Proudlock, F.A.; Siram, V.; Suraweera, C.; Hutchinson, C.; Nelson, C.P.; Al-Uzri, M.; Gottlob, I. Retinal Layer Abnormalities as Biomarkers of Schizophrenia. Schizophr. Bull. 2018, 44, 876–885. [Google Scholar] [CrossRef]
- Balasubramanian, R.; Gan, L. Development of Retinal Amacrine Cells and Their Dendritic Stratification. Curr. Ophthalmol. Rep. 2014, 2, 100–106. [Google Scholar] [CrossRef] [Green Version]
- Morgan, P.T.; Pace-Schott, E.F.; Mason, G.F.; Forselius, E.; Fasula, M.; Valentine, G.W.; Sanacora, G. Cortical GABA levels in primary insomnia. Sleep 2012, 35, 807–814. [Google Scholar] [CrossRef] [PubMed]
- Winkelman, J.W.; Buxton, O.M.; Jensen, J.E.; Benson, K.L.; O’Connor, S.P.; Wang, W.; Renshaw, P.F. Reduced brain GABA in primary insomnia: Preliminary data from 4T proton magnetic resonance spectroscopy (1H-MRS). Sleep 2008, 31, 1499–1506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Plante, D.T.; Jensen, J.E.; Schoerning, L.; Winkelman, J.W. Reduced gamma-aminobutyric acid in occipital and anterior cingulate cortices in primary insomnia: A link to major depressive disorder? Neuropsychopharmacology 2012, 37, 1548–1557. [Google Scholar] [CrossRef] [Green Version]
- Kay, D.B.; Buysse, D.J. Hyperarousal and Beyond: New Insights to the Pathophysiology of Insomnia Disorder through Functional Neuroimaging Studies. Brain Sci. 2017, 7, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saidha, S.; Syc, S.B.; Durbin, M.K.; Eckkstein, C.; Oakley, J.D.; Meyer, S.A.; Conger, A.; Frohman, T.C.; Newsome, S.; Ratchford, J.N.; et al. Visual dysfunction in multiple sclerosis correlates better with optical coherence tomography derived estimates of macular ganglion cell layer thickness than peripapillary retinal nerve fiber layer thickness. Mult. Scler. J. 2011, 17, 1449–1463. [Google Scholar] [CrossRef]
- Tan, C.S.; Ouyang, Y.; Ruiz, H.; Sadda, S.R. Diurnal variation of choroidal thickness in normal, healthy subjects measured by spectral domain optical coherence tomography. Investig. Ophthalmol. Vis. Sci. 2012, 53, 261–266. [Google Scholar] [CrossRef]
- Brainard, G.C.; Morgan, W.W. Light-induced stimulation of retinal dopamine: A dose-response relationship. Brain Res. 1987, 424, 199–203. [Google Scholar] [CrossRef]
- Huemer, K.H.; Garhofer, G.; Aggermann, T.; Kolodjascna, J.; Schmetterer, L.; Fuchsjager-Mayrl, G. Role of nitric oxide in choroidal blood flow regulation during light/dark transitions. Investig. Ophthalmol. Vis. Sci. 2007, 48, 4215–4219. [Google Scholar] [CrossRef] [Green Version]
- Read, S.A.; Pieterse, E.C.; Alanso-Caneiro, D.; Bormann, R.; Hong, S.; Lo, C.; Richer, R.; Syed, A.; Tran, L. Daily morning light therapy is associated with an increase in choroidal thickness in healthy young adults. Sci. Rep. 2018, 8, 8200. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Insomnia N = 52 | Healthy Controls N = 45 | χ2 (df)/t (df) | p Value | |
|---|---|---|---|---|
| Age (mean ± SD) | 43.0 ± 11.7 | 40.3 ± 12.2 | 1.125 (91.7) | 0.26 |
| Gender (female, number) | 40 | 31 | 0.794 (1) | 0.49 |
| BMI | 26.7 ± 5.8 | 27.6 ± 5.8 | −0.780 (92.3) | 0.43 |
| Smoking (yes, number) | 16 | 21 | 0.270 (1) | 0.66 |
| PSQI (mean ± SD) | 12.3 ± 3.3 | 4.3 ± 2.0 | 14.436 (85.4) | <0.001 |
| ISI (mean ± SD) | 19.9 ± 4.2 | 5.7 ± 2.1 | −21.577 | <0.001 |
| Duration of the insomnia (month, mean ± SD) | 31.6 ± 45.2 |
| Insomnia N = 52 | Healthy Controls N = 45 | z/t | p Value | |
|---|---|---|---|---|
| RNFL-G (mean ± SD) | 101.32 ± 9.12 | 105.48 ± 7.81 | z = −2.260 | 0.024 * |
| RNFL-T (mean ± SD) | 73.53 ± 12.35 | 76.53 ± 12.41 | z = −1.299 | 0.194 |
| RNFL-TS (mean ± SD) | 140.94 ± 19.69 | 141.71 ± 19.01 | z = −0.416 | 0.677 |
| RNFL-TI (mean ± SD) | 144.19 ± 26.93 | 139.28 ± 29.98 | z = −0.651 | 0.515 |
| RNFL-N (mean ± SD) | 77.53 ± 12.88 | 78.35 ± 14.58 | z = −0.916 | 0.360 |
| RNFL-NS (mean ± SD) | 122.28 ± 25.13 | 117.06 ± 25.13 | t = 1.062 | 0.288 |
| RNFL-NI (mean ± SD) | 109.76 ± 21.84 | 118.84 ± 25.64 | z = −2.591 | 0.010 * |
| Dependent Variable | Predictor/s | B | SE | β | t | p |
|---|---|---|---|---|---|---|
| CHO-G | Age | −3.806 | 1.088 | −0.451 | −3.497 | 0.001 |
| CHO-T | Age | −3.811 | 1.022 | −0.474 | −3.727 | 0.001 |
| CHO-N | Age ISI | −4.421 | 0.923 | −0.566 | −4.731 | <0.001 |
| −218.185 | 100.660 | −0.260 | −2.168 | 0.035 | ||
| CHO-F | Age | −4.256 | 1.047 | −0.506 | −4.065 | <0.001 |
| RNFL-G | ISI | −25.422 | 11.419 | −0.306 | −2.226 | 0.031 |
| RNFL-NI | ISI | −64.947 | 27.003 | −0.328 | −2.405 | 0.020 |
| RNFL-TI | Gender | 27.623 | 8.230 | 0.436 | 3.356 | 0.002 |
| IPL-N | Gender | 3.303 | 1.392 | 0.324 | 2.373 | 0.022 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sahbaz, C.; Elbay, A.; Ozcelik, M.; Ozdemir, H. Insomnia Might Influence the Thickness of Choroid, Retinal Nerve Fiber and Inner Plexiform Layer. Brain Sci. 2020, 10, 178. https://doi.org/10.3390/brainsci10030178
Sahbaz C, Elbay A, Ozcelik M, Ozdemir H. Insomnia Might Influence the Thickness of Choroid, Retinal Nerve Fiber and Inner Plexiform Layer. Brain Sciences. 2020; 10(3):178. https://doi.org/10.3390/brainsci10030178
Chicago/Turabian StyleSahbaz, Cigdem, Ahmet Elbay, Mine Ozcelik, and Hakan Ozdemir. 2020. "Insomnia Might Influence the Thickness of Choroid, Retinal Nerve Fiber and Inner Plexiform Layer" Brain Sciences 10, no. 3: 178. https://doi.org/10.3390/brainsci10030178
APA StyleSahbaz, C., Elbay, A., Ozcelik, M., & Ozdemir, H. (2020). Insomnia Might Influence the Thickness of Choroid, Retinal Nerve Fiber and Inner Plexiform Layer. Brain Sciences, 10(3), 178. https://doi.org/10.3390/brainsci10030178