Trajectories of Immediate and Delayed Verbal Memory in the Spanish General Population of Middle-aged and Older Adults

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
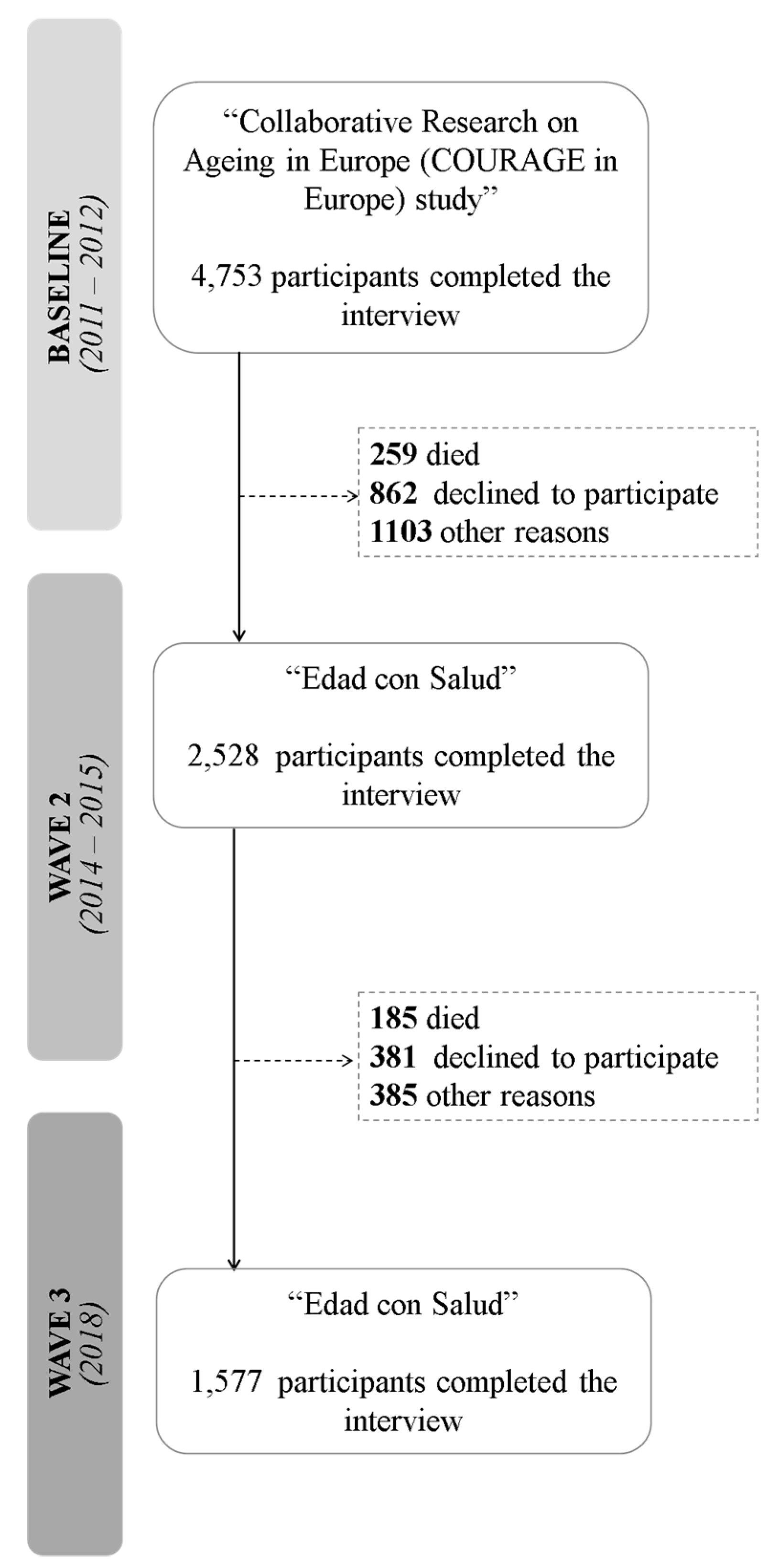
2.1. Study Design and Data Collection
2.2. Measures
2.3. Statistical Analyses
3. Results
3.1. Descriptive Analysis
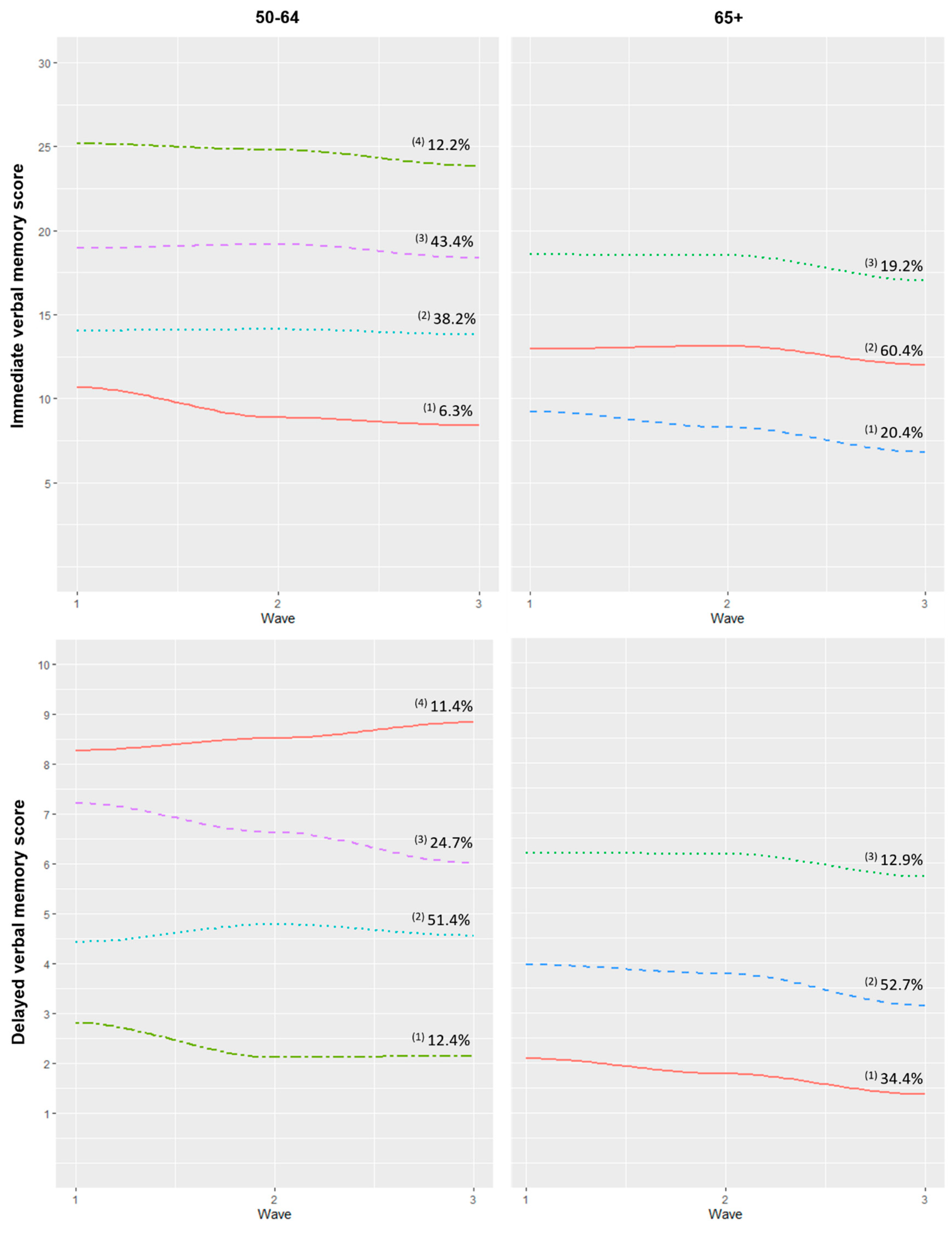
3.2. Verbal Memory Trajectories
3.3. Association between Verbal Memory Trajectories and Covariates
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- United Nations. Department of Economic and Social Affairs. Population Division Population Ageing and Sustainable Development. Available online: https://www.un.org/en/development/desa/population/publications/pdf/popfacts/PopFacts_2017-1.pdf (accessed on 15 November 2019).
- Feigin, V.L.; Nichols, E.; Alam, T.; Bannick, M.S.; Beghi, E.; Blake, N.; Culpepper, W.J.; Dorsey, E.R.; Elbaz, A.; Ellenbogen, R.G.; et al. Global, regional, and national burden of neurological disorders, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019, 18, 459–480. [Google Scholar] [CrossRef] [Green Version]
- Chodosh, J.; Miller-Martinez, D.; Aneshensel, C.S.; Wight, R.G.; Karlamangla, A.S. Depressive symptoms, chronic diseases, and physical disabilities as predictors of cognitive functioning trajectories in older Americans. J. Am. Geriatr. Soc. 2010, 58, 2350–2357. [Google Scholar] [CrossRef] [PubMed]
- Salthouse, T.A. When does age-related cognitive decline begin? Neurobiol. Aging 2009, 30, 507–514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deary, I.J.; Corley, J.; Gow, A.J.; Harris, S.E.; Houlihan, L.M.; Marioni, R.E.; Penke, L.; Rafnsson, S.B.; Starr, J.M.; Corley, J.; et al. Age-associated cognitive decline. Br. Med. Bull. 2009, 92, 135–152. [Google Scholar] [CrossRef] [PubMed]
- Murman, D.L. The Impact of Age on Cognition. Semin. Hear. 2015, 36, 111–121. [Google Scholar] [CrossRef] [PubMed]
- WHO Ageing and Health. Available online: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health (accessed on 11 December 2018).
- Salthouse, T.A. Memory aging from 18 to 80. Alzheimer Dis. Assoc. Disord. 2003, 17, 162–167. [Google Scholar] [CrossRef]
- Hayden, K.M.; Reed, B.R.; Manly, J.J.; Tommet, D.; Pietrzak, R.H.; Chelune, G.J.; Yang, F.M.; Revell, A.J.; Bennett, D.A.; Jones, R.N. Cognitive decline in the elderly: An analysis of population heterogeneity. Age Ageing 2011, 40, 684–689. [Google Scholar] [CrossRef] [Green Version]
- Terrera, G.M.; Brayne, C.; Matthews, F. One size fits all? Why we need more sophisticated analytical methods in the explanation of trajectories of cognition in older age and their potential risk factors. Int. Psychogeriatrics 2010, 22, 291–299. [Google Scholar] [CrossRef]
- Olaya, B.; Bobak, M.; Haro, J.M.; Demakakos, P. Trajectories of verbal episodic memory in middle-aged and older adults: Evidence from the English Longitudinal Study of Ageing. J. Am. Geriatr. Soc. 2017, 65, 1274–1281. [Google Scholar] [CrossRef] [Green Version]
- Zahodne, L.B.; Wall, M.M.; Schupf, N.; Mayeux, R.; Manly, J.J.; Stern, Y.; Brickman, A.M. Late-life memory trajectories in relation to incident dementia and regional brain atrophy. J. Neurol. 2015, 262, 2484–2490. [Google Scholar] [CrossRef] [Green Version]
- Zaninotto, P.; Batty, G.D.; Allerhand, M.; Deary, I.J. Cognitive function trajectories and their determinants in older people: 8 Years of follow-up in the English Longitudinal Study of Ageing. J. Epidemiol. Community Health 2018, 72, 685–694. [Google Scholar] [CrossRef] [PubMed]
- Wilson, R.S.; Beckett, L.A.; Barnes, L.L.; Schneider, J.A.; Bach, J.; Evans, D.A.; Bennett, D.A. Individual differences in rates of change in cognitive abilities of older persons. Psychol. Aging 2002, 17, 179–193. [Google Scholar] [CrossRef] [PubMed]
- Harada, C.N.; Natelson Love, M.C.; Triebel, K.L. Normal cognitive aging. Clin. Geriatr. Med. 2013, 29, 737–752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atkinson, R.C.; Shiffrin, R.M. Human Memory: A proposed system and its control processes. Psychol. Learn. Motiv. Adv. Res. Theory 1968, 2, 89–195. [Google Scholar]
- Haan, M.N.; Weldon, M. The influence of diabetes, hypertension, and stroke on ethnic differences in physical and cognitive functioning in an ethnically diverse older population. Ann. Epidemiol. 1996, 6, 392–398. [Google Scholar] [CrossRef]
- Loprinzi, P.D.; Herod, S.M.; Cardinal, B.J.; Noakes, T.D. Physical activity and the brain: A review of this dynamic, bi-directional relationship. Brain Res. 2013, 1539, 95–104. [Google Scholar] [CrossRef]
- Loprinzi, P.D. Multimorbidity, cognitive function, and physical activity. Age (Omaha) 2016, 38, 8. [Google Scholar] [CrossRef] [Green Version]
- Hötting, K.; Schauenburg, G.; Röder, B. Long-Term Effects of Physical Exercise on Verbal Learning and Memory in Middle-Aged Adults: Results of a One-Year Follow-Up Study. Brain Sci. 2012, 2, 332–346. [Google Scholar] [CrossRef] [Green Version]
- Cullum, S.; Huppert, F.A.; McGee, M.; Dening, T.; Ahmed, A.; Paykel, E.S.; Brayne, C. Decline across different domains of cognitive function in normal ageing: Results of a longitudinal population-based study using CAMCOG. Int. J. Geriatr. Psychiatry 2000, 15, 853–862. [Google Scholar] [CrossRef]
- Leonardi, M.; Chatterji, S.; Koskinen, S.; Ayuso-Mateos, J.L.; Haro, J.M.; Frisoni, G.; Frattura, L.; Martinuzzi, A.; Tobiasz-Adamczyk, B.; Gmurek, M.; et al. Determinants of health and disability in ageing population: The COURAGE in Europe Project (Collaborative Research on Ageing in Europe). Clin. Psychol. Psychother. 2014, 21, 193–198. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Morris, J.C.; Heyman, A.; Mohs, R.C.; Hughes, J.P.; van Belle, G.; Fillenbaum, G. The consortium to establish a registry for Alzheimer’s disease (CERAD). Part I. Clinical and neuropsychological assesment of Alzheimer’s disease. Neurology 1989, 39, 1159–1165. [Google Scholar] [CrossRef] [PubMed]
- Kowal, P.; Chatterji, S.; Naidoo, N.; Biritwum, R.; Fan, W.; Lopez Ridaura, R.; Maximova, T.; Arokiasamy, P.; Phaswana-Mafuya, N.; Williams, S.; et al. Data resource profile: The World Health Organization study on global AGEing and adult health (SAGE). Int. J. Epidemiol. 2013, 41, 1639–1649. [Google Scholar] [CrossRef] [PubMed]
- Ronald, C.; Kessler, T.B.Ü. The World Mental Health (WMH) survey initiative version of the World Health Organization (WHO) Composite Diagnostic Interview (CIDI). Int. J. Methods Psychiatr. Res. 2004, 13, 93–121. [Google Scholar]
- WHO. Global Physical Activity Questionnaire (GPAQ) Analysis Guide; WHO: Geneva, Switzerland, 2012. [Google Scholar]
- Ustun, T.B.; Kostanjsek, N.; Chatterji, S.; Rehm, J.; WHO. Developing the World Health Organization Disability Assessment Schedule 2.0. Bull World Health Organ 2010, 88, 815–823. [Google Scholar] [CrossRef]
- Caballero, F.; Miret, M.; Power, M.; Chatterji, S.; Tobiasz-Adamczyk, B.; Koskinen, S.; Leonardi, M.; Olaya, B.; Haro, J.; Ayuso-Mateos, J. Validation of an instrument to evaluate quality of life in the aging population: WHOQOL-AGE. Health Qual. Life Outcomes 2013, 11, 177. [Google Scholar] [CrossRef] [Green Version]
- Berlin, K.S.; Parra, G.R.; Williams, N.A. An Introduction to Latent Variable Mixture Modeling (Part 2): Longitudinal Latent Class Growth Analysis and Growth Mixture Models. J. Pediatr. Psychol. 2014, 39, 188–203. [Google Scholar] [CrossRef]
- Muthén, L.K.; Muthén, B.O. Mplus User’s Guide, 7th ed.; Muthén, M.: Los Angeles, CA, USA, 2012. [Google Scholar]
- Tein, J.Y.; Coxe, S.; Cham, H. Statistical power to detect the correct number of classes in latent profile analysis. Struct. Equ. Model. 2013, 20, 640–657. [Google Scholar] [CrossRef]
- Nylund-Gibson, K.; Choi, A.Y. Ten frequently asked questions about latent class analysis. Transl. Issues Psychol. Sci. 2018, 4, 440–461. [Google Scholar] [CrossRef]
- R Development Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2019. [Google Scholar]
- Rabbitt, P.; Diggle, P.; Holland, F.; McInnes, L. Practice and drop-out effects during a 17-year longitudinal study of cognitive aging. J. Gerontol. B. Psychol. Sci. Soc. Sci. 2004, 59, 84–97. [Google Scholar] [CrossRef] [Green Version]
- Wilson, R.S.; Li, Y.; Bienias, J.L.; Bennett, D.A. Cognitive decline in old age: Separating retest effects from the effects of growing older. Psychol. Aging 2006, 21, 774–789. [Google Scholar] [CrossRef] [PubMed]
- Stern, Y. Cognitive reserve. Neuropsychologia 2009, 47, 2015–2028. [Google Scholar] [CrossRef] [PubMed]
- Lyu, J.; Burr, J.A. Socioeconomic Status across the life course and cognitive function among older adults: An examination of the latency, pathways, and accumulation hypotheses. J. Aging Health 2016, 28, 40–67. [Google Scholar] [CrossRef] [PubMed]
- Zilliox, L.A.; Chadrasekaran, K.; Kwan, J.Y.; Russell, J.W. Diabetes and cognitive impairment. Curr. Diab. Rep. 2016, 16, 87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anstey, K.J.; Sargent-Cox, K.; Garde, E.; Cherbuin, N.; Butterworth, P. Cognitive development over 8 years in midlife and its association with cardiovascular risk factors. Neuropsychology 2014, 28, 653–665. [Google Scholar] [CrossRef] [PubMed]
- Caracciolo, B.; Gatz, M.; Xu, W.; Marengoni, A.; Pedersen, N.L.; Fratiglioni, L. Relationship of subjective cognitive impairment and cognitive impairment no dementia to chronic disease and multimorbidity in a nation-wide twin study. J. Alzheimer’s Dis. 2013, 36, 275–284. [Google Scholar] [CrossRef] [Green Version]
- Vassilaki, M.; Aakre, J.A.; Cha, R.H.; Kremers, W.K.; St. Sauver, J.L.; Mielke, M.M.; Geda, Y.E.; Machulda, M.M.; Knopman, D.S.; Petersen, R.C.; et al. Multimorbidity and risk of mild cognitive impairment. J. Am. Geriatr. Soc. 2015, 63, 1783–1790. [Google Scholar] [CrossRef]
- Li, C.; Liu, T.; Sun, W.; Wu, L.; Zou, Z.-Y. Prevalence and risk factors of arthritis in a middle-aged and older Chinese population: The China health and retirement longitudinal study. Rheumatology (Oxford) 2015, 54, 697–706. [Google Scholar] [CrossRef] [Green Version]
- Smith, J.; Nielson, K.; Woodard, J.; Seidenberg, M.; Rao, S. Physical Activity and Brain Function in Older Adults at Increased Risk for Alzheimer’s Disease. Brain Sci. 2013, 3, 54–83. [Google Scholar] [CrossRef] [Green Version]
- Plassman, B.L.; Williams, J.W.; Burke, J.R.; Holsinger, T.; Benjamin, S. Systematic review: Factors associated with risk for and possible prevention of cognitive decline in later life. Ann. Intern. Med. 2010, 153, 182–193. [Google Scholar] [CrossRef] [Green Version]
- Huntley, A.L.; Johnson, R.; Purdy, S.; Valderas, J.M.; Salisbury, C. Measures of multimorbidity and morbidity burden for use in primary care and comminuty settings: A systematic review and guide. Ann. Fam. Med. 2012, 10, 134–141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van der Elst, W.; Molenberghs, G.; Van Boxtel, M.P.J.; Jolles, J. Establishing normative data for repeated cognitive assessment: A comparison of different statistical methods. Behav. Res. Methods 2013, 45, 1073–1086. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagin, D.S. Group-Based Trajectory Modeling: An Overview. Ann. Nutr. Metab. 2014, 65, 205–210. [Google Scholar] [CrossRef]
- Nagin, D.S.; Tremblay, R.E.; Sampson, R.J.; Laub, J.H. Developmental trajectory groups: Fact or a useful statistical fiction? Criminology 2005, 43, 873–904. [Google Scholar] [CrossRef]
- Karr, J.E.; Graham, R.B.; Hofer, S.M.; Muniz-Terrera, G. When does cognitive decline begin? A systematic review of change point studies on accelerated decline in cognitive and neurological outcomes preceding mild cognitive impairment, dementia, and death. Psychol. Aging 2018, 33, 95–218. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | 50–64 (n = 633) | 65+ (n = 456) | p-Value 1 |
|---|---|---|---|
| Age, mean [IQR] | 56.62 [60.00, 53.00] | 73.01 [77.00, 68.00] | <0.001 |
| Women, n (%) | 329 (52.0) | 249 (54.6) | 0.236 |
| Marital status, n (%) | <0.001 | ||
| Never married | 65 (10.3) | 29 (6.4) | |
| Married | 453 (71.6) | 268 (58.8) | |
| Divorced | 68 (10.7) | 15 (3.3) | |
| Widowed | 47 (7.4) | 144 (31.6) | |
| Level of education, n (%) | <0.001 | ||
| Less than primary education | 105 (16.6) | 212 (46.5) | |
| Primary education | 198 (31.3) | 136 (28.8) | |
| Secondary education | 225 (35.6) | 76 (16.7) | |
| Tertiary education | 105 (16.6) | 32 (7.0) | |
| Ever worked, n (%) | 587 (92.7) | 365 (80.0) | <0.001 |
| Household income quintiles, n (%) | <0.001 | ||
| 1st (lowest) | 108 (17.1) | 70 (15.4) | |
| 2nd | 111 (17.5) | 111 (24.3) | |
| 3rd | 105 (16.6) | 99 (21.7) | |
| 4th | 112 (17.7) | 100 (21.9) | |
| 5th (highest) | 118 (18.6) | 39 (8.6) | |
| Urban, n (%) | 543 (85.8) | 390 (85.5) | 0.399 |
| No. diseases, mean [IQR] | 0.95 [1.00, 0.00] | 1.52 [2.00, 1.00] | <0.001 |
| Diseases, n (%) | |||
| Diabetes | 73 (11.5) | 102 (22.4) | <0.001 |
| Hypertension | 217 (34.3) | 224 (49.1) | <0.001 |
| Asthma | 38 (6.0) | 47 (10.3) | 0.002 |
| COPD | 35 (5.5) | 57 (12.5) | <0.001 |
| Arthritis | 124 (19.6) | 153 (33.4) | <0.001 |
| Angina pectoris | 27 (4.3) | 41 (9.0) | <0.001 |
| Stroke | 18 (2.8) | 27 (6.0) | <0.001 |
| Depression | 72 (11.4) | 47 (10.3) | 0.453 |
| Tobacco, n (%) | <0.001 | ||
| Never smoked | 273 (43.1) | 280 (61.4) | |
| Daily smoker | 169 (26.7) | 41 (9.0) | |
| Not daily smoker | 14 (2.2) | 6 (1.3) | |
| Not current smoker | 177 (28.0) | 129 (28.3) | |
| Alcohol, n (%) | <0.001 | ||
| Lifetime abstainers | 168 (26.5) | 158 (34.7) | |
| Occasional drinkers | 170 (26.9) | 132 (29.0) | |
| Infrequent heavy drinker | 11 (1.7) | 2 (0.4) | |
| Frequent heavy drinker | 284 (44.9) | 164 (36.0) | |
| Physical activity level, n (%) | <0.001 | ||
| Low | 199 (31.4) | 134 (29.4) | |
| Moderate | 225 (35.6) | 201 (44.1) | |
| High | 209 (33.0) | 121 (26.5) | |
| WHODAS, mean [IQR] | 7.60 [8.33, 0.00] | 15.02 [25.00, 0.00] | <0.001 |
| WHOQOL-Age, mean [IQR] | 73.68 [83.10, 66.67] | 72.54 [82.42, 64.15] | <0.001 |
| Immediate verbal memory, mean [IQR] | 17.36 [21.00, 14.00] | 13.41 [16.00, 10.00] | <0.001 |
| Delayed verbal memory, mean [IQR] | 5.35 [7.00, 4.00] | 3.74 [5.00, 2.00] | <0.001 |
| Age Groups | No. of Latent Classes | Immediate Verbal Memory | Delayed Verbal Memory | ||
|---|---|---|---|---|---|
| aBIC | Entropy | aBIC | Entropy | ||
| 50–64 | 2 | 11125.778 | 0.676 | 8037.546 | 0.726 |
| 3 | 11008.528 | 0.706 | 7971.521 | 0.691 | |
| 4 | 10999.151 | 0.688 | 7955.357 | 0.653 | |
| 5 | 11002.767 | 0.681 | 7955.693 | 0.69 | |
| 65+ | 2 | 7722.539 | 0.646 | 5555.695 | 0.692 |
| 3 | 7680.159 | 0.654 | 5541.606 | 0.547 | |
| 4 | 7674.616 | 0.698 | 5541.611 | 0.642 | |
| 5 | 7673.520 | 0.712 | 5542.644 | 0.626 | |
| 50–64 | ||||||
|---|---|---|---|---|---|---|
| “Very Low/Decline” (n = 31, 6.3%) | “Low/Stable” (n = 248, 38.2%) | “Medium/Slow Decline” (n = 281, 43.4%) | “High/Slow Decline” (n = 73, 12.2%) | p-Value 1 | Effect Size2 | |
| Age | 58.41 [61.5, 55.5] | 57.85 [61.0, 55.0] | 55.75 [59.0, 52.0] | 55.01 [57.0, 52.0] | <0.001 | 0.07 |
| Women, n (%) | 13 (41.9) | 118 (47.6) | 152 (54.1) | 46 (63.0) | 0.064 | 0.10 |
| Marital status, n (%) | 0.104 | 0.09 | ||||
| Never married | 5 (16.1) | 20 (8.1) | 25 (9.0) | 15 (20.6) | ||
| Married | 20 (64.5) | 186 (75.0) | 203 (72.2) | 44 (60.3) | ||
| Divorced | 4 (13.0) | 20 (8.1) | 36 (12.8) | 8 (11.0) | ||
| Widowed | 2 (6.5) | 22 (8.9) | 17 (6.1) | 6 (8.2) | ||
| Level of education, n (%) | <0.001 | 0.32 | ||||
| Less than primary education | 15 (48.4) | 67 (27.0) | 22 (7.8) | 1 (1.4) | ||
| Primary education | 14 (45.2) | 104 (41.9) | 73 (26.0) | 7 (9.6) | ||
| Secondary education | 1 (3.2) | 60 (24.2) | 138 (49.1) | 26 (35.6) | ||
| Tertiary education | 1 (3.2) | 17 (6.9) | 48 (17.1) | 39 (53.4) | ||
| Ever worked, n (%) | 28 (90.3) | 219 (88.3) | 267 (95.0) | 73 (100.0) | 0.001 | 0.15 |
| Household income quintiles, n (%) | <0.001 | 0.17 | ||||
| 1st (lowest) | 3 (13.6) | 38 (17.4) | 51 (20.6) | 16 (24.6) | ||
| 2nd | 6 (27.3) | 55 (25.1) | 36 (14.5) | 14 (21.5) | ||
| 3rd | 6 (27.3) | 54 (24.7) | 40 (16.1) | 5 (7.7) | ||
| 4th | 7 (31.8) | 45 (20.6) | 54 (21.8) | 6 (9.2) | ||
| 5th (highest) | 0 (0.0) | 27 (12.3) | 67 (27.0) | 24 (36.9) | ||
| Urban, n (%) | 21 (67.7) | 215 (86.7) | 241 (85.8) | 66 (90.4) | 0.021 | 0.12 |
| No. Diseases | 1.52 [3.0, 1.5] | 1.17 [3.0, 1.0] | 0.76 [2.0, 1.0] | 0.66 [2.0, 1.0] | <0.001 | 0.04 |
| Diseases, n (%) | ||||||
| Diabetes | 7 (22.6) | 41 (16.5) | 18 (6.4) | 7 (9.6) | <0.001 | 0.16 |
| Hypertension | 13 (43.3) | 93 (38.8) | 93 (33.7) | 18 (25.0) | 0.123 | 0.09 |
| Asthma | 2 (6.5) | 19 (7.7) | 12 (4.3) | 5 (6.9) | 0.422 | 0.06 |
| COPD | 3 (9.7) | 20 (8.1) | 10 (3.6) | 2 (2.7) | 0.064 | 0.10 |
| Arthritis | 9 (29.0) | 64 (25.8) | 44 (15.6) | 7 (9.6) | 0.001 | 0.15 |
| Angina pectoris | 2 (6.9) | 12 (5.1) | 10 (3.6) | 3 (4.2) | 0.783 | 0.04 |
| Stroke | 3 (9.7) | 9 (3.6) | 6 (2.14) | 0 (0.0) | 0.037 | 0.11 |
| Depression | 8 (25.8) | 37 (14.9) | 21 (7.5) | 6 (8.2) | 0.002 | 0.15 |
| Tobacco, n (%) | 0.495 | 0.06 | ||||
| Never smoked | 17 (54.8) | 114 (46.0) | 114 (40.6) | 28 (38.4) | ||
| Daily smoker | 7 (22.6) | 62 (25.0) | 80 (28.5) | 20 (27.4) | ||
| Not daily smoker | 1 (3.2) | 4 (1.6) | 5 (1.8) | 4 (5.5) | ||
| Not current smoker | 6 (19.4) | 68 (27.4) | 82 (29.2) | 21 (28.8) | ||
| Alcohol, n (%) | 0.165 | 0.17 | ||||
| Lifetime abstainer | 8 (25.8) | 81 (32.7) | 63 (22.4) | 16 (21.9) | ||
| Occasional drinker | 9 (29.0) | 69 (27.8) | 77 (27.4) | 15 (20.6) | ||
| Infrequent heavy drinker | 0 (0.0) | 5 (2.0) | 6 (2.1) | 0 (0.0) | ||
| Frequent heavy drinker | 14 (45.2) | 93 (37.5) | 135 (48.0) | 42 (57.5) | ||
| Physical activity level, n (%) | 0.001 | 0.13 | ||||
| Low | 15 (48.4) | 86 (34.7) | 85 (30.3) | 13 (17.8) | ||
| Moderate | 10 (32.3) | 85 (34.3) | 109 (38.8) | 21 (28.8) | ||
| High | 6 (19.4) | 77 (31.0) | 87 (31.0) | 39 (53.4) | ||
| WHODAS | 12.72 [18.0, 0.0] | 9.84 [13.8, 0.0] | 5.73 [5.5, 0.0] | 5.02 [2.7, 0.0] | <0.001 | 0.04 |
| WHOQOL-Age | 63.34 [74.2, 50.7] | 71.88 [80.0, 65.0] | 75.00 [84.5, 67.7] | 79.88 [90.2, 71.3] | <0.001 | 0.04 |
| Immediate verbal memory | 10.68 [13.0, 8.5] | 14.09 [17.0, 12.0] | 18.95 [21.0, 17.0] | 25.18 [27.0, 23.0] | <0.001 | 0.54 |
| Delayed verbal memory | 2.94 [4.0, 1.5] | 4.28 [5.0, 3.0] | 5.91 [7.0, 5.0] | 7.88 [9.0, 7.0] | <0.001 | 0.32 |
| 65+ | |||||
|---|---|---|---|---|---|
| “Low/Decline” (n = 87, 20.4%) | “Medium/Slow Decline” (n = 287, 60.4%) | “High/Slow Decline” (n = 82, 19.2%) | p-Value 1 | Effect Size2 | |
| Age | 76.10 [79.3, 73.0] | 72.80 [77.0, 68.0] | 70.68 [73.0, 67.0] | <0.001 | 0.08 |
| Women, n (%) | 54 (62.1) | 154 (53.7) | 41 (50.0) | 0.251 | 0.08 |
| Marital status, n (%) | 0.202 | 0.11 | |||
| Never married | 6 (7.0) | 17 (5.6) | 7 (8.5) | ||
| Married | 53 (61.0) | 165 (57.5) | 50 (61.0) | ||
| Divorced | 1 (1.2) | 8 (2.8) | 6 (7.3) | ||
| Widowed | 27 (31.0) | 98 (34.2) | 19 (23.2) | ||
| Level of education, n (%) | <0.001 | 0.33 | |||
| Less than primary education | 59 (67.8) | 140 (48.8) | 13 (15.9) | ||
| Primary education | 24 (27.6) | 94 (32.2) | 18 (22.0) | ||
| Secondary education | 4 (4.6) | 37 (12.9) | 35 (42.7) | ||
| Tertiary education | 0 (0.0) | 16 (5.6) | 16 (19.5) | ||
| Ever worked, n (%) | 61 (70.1) | 228 (79.4) | 76 (92.7) | 0.001 | 0.17 |
| Household income quintiles, n (%) | <0.001 | 0.22 | |||
| 1st (lowest) | 7 (9.3) | 47 (17.6) | 16 (20.8) | ||
| 2nd | 32 (42.7) | 73 (27.3) | 6 (7.8) | ||
| 3rd | 20 (26.7) | 65 (24.3) | 14 (18.2) | ||
| 4th | 10 (13.3) | 65 (24.3) | 25 (32.5) | ||
| 5th (highest) | 6 (8.0) | 17 (6.4) | 16 (20.8) | ||
| Urban, n (%) | 67 (77.0) | 250 (87.1) | 73 (89.0) | 0.039 | 0.12 |
| No. Diseases | 1.64 [3.0, 2.0] | 1.53 [3.0, 2.0] | 1.35 [3.0, 2.0] | 0.430 | 0.14 |
| Diseases, n (%) | |||||
| Diabetes | 28 (32.2) | 64 (22.3) | 10 (12.2) | 0.007 | 0.15 |
| Hypertension | 38 (45.8) | 143 (51.1) | 43 (53.1) | 0.609 | 0.05 |
| Asthma | 7 (8.1) | 34 (11.9) | 6 (7.3) | 0.366 | 0.07 |
| COPD | 11 (12.6) | 35 (12.2) | 11 (13.4) | 0.956 | 0.01 |
| Arthritis | 39 (44.8) | 92 (32.1) | 22 (26.8) | 0.031 | 0.12 |
| Angina pectoris | 10 (12.5) | 24 (8.8) | 7 (8.97) | 0.605 | 0.05 |
| Stroke | 6 (6.9) | 15 (5.2) | 6 (7.3) | 0.710 | 0.04 |
| Depression | 11 (12.6) | 32 (11.1) | 4 (4.9) | 0.187 | 0.09 |
| Tobacco, n (%) | 0.013 | 0.13 | |||
| Never smoked | 64 (73.6) | 176 (61.3) | 40 (48.8) | ||
| Daily smoker | 3 (3.5) | 31 (10.8) | 7 (8.5) | ||
| Not daily smoker | 2 (2.3) | 3 (1.1) | 1 (1.2) | ||
| Not current smoker | 18 (20.7) | 77 (26.8) | 34 (41.5) | ||
| Alcohol, n (%) | 0.023 | 0.14 | |||
| Lifetime abstainer | 43 (49.4) | 96 (33.5) | 19 (23.2) | ||
| Occasional drinker | 22 (25.3) | 87 (30.3) | 23 (28.1) | ||
| Infrequent heavy drinker | 0 (0.0) | 2 (0.7) | 0 (0.0) | ||
| Frequent heavy drinker | 22 (25.3) | 102 (35.5) | 40 (48.8) | ||
| Physical activity level, n (%) | 0.004 | 0.13 | |||
| Low | 36 (41.5) | 82 (28.6) | 16 (19.5) | ||
| Moderate | 36 (41.4) | 131 (45.6) | 34 (41.5) | ||
| High | 15 (17.2) | 74 (25.8) | 32 (39.0) | ||
| WHODAS | 24.10 [39.5, 5.5] | 14.44 [25.0, 0.0] | 8.06 [11.1, 0.0] | <0.001 | 0.07 |
| WHOQOL-Age | 66.15 [75.0, 59.2] | 73.01 [80.9, 65.3] | 77.23 [86.9, 68.3] | <0.001 | 0.06 |
| Immediate verbal memory | 9.49 [12.0, 7.0] | 13.02 [15.0, 11.0] | 18.62 [21.0, 16.0] | <0.001 | 0.38 |
| Delayed verbal memory | 2.59 [4.0, 1.75] | 3.54 [4.0, 2.0] | 5.59 [7.0, 4.0] | <0.001 | 0.22 |
| 50–64 | ||||||
|---|---|---|---|---|---|---|
| “Very Low/Decline” (n = 68, 12.4%) | “Low/Stable” (n = 346, 51.4%) | “Medium/Accelerated Decline” (n = 150, 24.7%) | “High/Slow Increase” (n = 69, 11.4%) | p-Value 1 | Effect Size2 | |
| Age | 58.94 [62.0, 56.0] | 56.91 [60.0, 54.0] | 55.64 [59.0, 52.0] | 54.97 [58.0, 51.0] | <0.001 | 0.07 |
| Women, n (%) | 26 (38.2) | 170 (49.1) | 84 (56.0) | 49 (71.0) | <0.001 | 0.17 |
| Marital status, n (%) | 0.858 | 0.06 | ||||
| Never married | 7 (10.3) | 32 (9.3) | 17 (11.3) | 9 (13.0) | ||
| Married | 49 (72.1) | 249 (72.0) | 107 (71.3) | 48 (69.6) | ||
| Divorced | 7 (10.3) | 36 (10.4) | 19 (12.7) | 6 (8.7) | ||
| Widowed | 5 (7.4) | 29 (8.4) | 7 (4.7) | 6 (8.7) | ||
| Level of education, n (%) | <0.001 | 0.25 | ||||
| Less than primary education | 18 (26.5) | 72 (20.8) | 11 (7.3) | 4 (5.8) | ||
| Primary education | 39 (57.4) | 117 (33.8) | 32 (21.3) | 10 (14.5) | ||
| Secondary education | 9 (13.2) | 121 (35.0) | 71 (47.3) | 24 (34.8) | ||
| Tertiary education | 2 (3.0) | 36 (10.4) | 36 (24.0) | 31 (44.9) | ||
| Ever worked, n (%) | 60 (88.2) | 318 (91.9) | 141 (94.0) | 68 (98.6) | 0.101 | 0.10 |
| Household income quintiles, n (%) | <0.001 | 0.15 | ||||
| 1st (lowest) | 9 (15.8) | 54 (17.6) | 33 (25.0) | 12 (20.7) | ||
| 2nd | 20 (35.1) | 58 (18.9) | 22 (16.7) | 11 (19.0) | ||
| 3rd | 16 (28.1) | 66 (21.5) | 16 (12.1) | 7 (12.1) | ||
| 4th | 6 (10.5) | 75 (24.4) | 23 (17.4) | 8 (13.8) | ||
| 5th (highest) | 6 (10.5) | 54 (17.6) | 38 (28.8) | 20 (34.5) | ||
| Urban, n (%) | 53 (78.0) | 290 (84.0) | 139 (92.7) | 61 (88.4) | 0.013 | 0.13 |
| No. Diseases | 2.29 [3.0, 1.0] | 1.99 [2.0, 1.0] | 1.84 [2.0, 1.0] | 1.61 [2.0, 1.0] | 0.135 | 0.05 |
| Diseases, n (%) | ||||||
| Diabetes | 14 (20.6) | 41 (11.9) | 14 (9.3) | 4 (5.8) | 0.037 | 0.12 |
| Hypertension | 30 (45.5) | 123 (36.3) | 47 (32.2) | 17 (25.4) | 0.084 | 0.10 |
| Asthma | 3 (4.4) | 26 (7.5) | 4 (2.7) | 5 (7.3) | 0.182 | 0.09 |
| COPD | 4 (5.9) | 24 (6.9) | 6 (4.0) | 1 (1.5) | 0.240 | 0.08 |
| Arthritis | 18 (26.5) | 68 (19.7) | 29 (19.3) | 9 (13.0) | 0.269 | 0.08 |
| Angina pectoris | 3 (4.6) | 15 (4.5) | 7 (4.8) | 2 (2.9) | 0.937 | 0.03 |
| Stroke | 6 (8.8) | 9 (2.6) | 3 (2.0) | 0 (0.0) | 0.010 | 0.13 |
| Depression | 10 (14.7) | 41 (11.9) | 17 (11.3) | 4 (5.8) | 0.398 | 0.07 |
| Tobacco, n (%) | 0.060 | 0.09 | ||||
| Never smoked | 26 (38.2) | 163 (47.1) | 60 (40.0) | 24 (34.8) | ||
| Daily smoker | 18 (26.5) | 92 (26.6) | 38 (25.3) | 21 (30.4) | ||
| Not daily smoker | 1(1.5) | 6 (1.7) | 2 (1.3) | 5 (7.3) | ||
| Not current smoker | 23 (33.8) | 85 (24.6) | 50 (33.3) | 19 (27.5) | ||
| Alcohol, n (%) | 0.109 | 0.09 | ||||
| Lifetime abstainer | 18 (26.5) | 92 (26.6) | 39 (26.0) | 19 (27.5) | ||
| Occasional drinker | 14 (20.6) | 105 (30.4) | 37 (24.7) | 14 (20.3) | ||
| Infrequent heavy drinker | 4 (5.9) | 3 (0.9) | 4 (2.7) | 0 (0.0) | ||
| Frequent heavy drinker | 32 (47.1) | 146 (42.2) | 70 (46.7) | 36 (52.2) | ||
| Physical activity level, n (%) | <0.001 | 0.14 | ||||
| Low | 29 (42.7) | 117 (33.8) | 42 (28.0) | 11 (15.9) | ||
| Moderate | 21 (30.9) | 128 (37.0) | 56 (37.3) | 20 (29.0) | ||
| High | 18 (26.5) | 101 (29.2) | 52 (34.7) | 38 (55.1) | ||
| WHODAS | 10.91 [16.7, 0.0] | 7.99 [11.1, 0.0] | 6.82 [8.3, 0.0] | 4.11 [2.8, 0.0] | 0.005 | 0.02 |
| WHOQOL-Age | 70.01 [77.7, 65.8] | 72.91 [82.9, 66.2] | 74.58 [82.5, 67.0] | 79.21 [88.6, 70.6] | 0.002 | 0.02 |
| Immediate verbal memory | 12.41 [15.0, 10.0] | 15.84 [19.0, 13.0] | 20.45 [23.0, 18.0] | 23.16 [27.0, 21.0] | <0.001 | 0.37 |
| Delayed verbal memory | 2.81 [4.0, 2.0] | 4.45 [5.0, 4.0] | 7.23 [8.0, 6.0] | 8.28 [10.0, 7.0] | <0.001 | 0.60 |
| 65+ | |||||
|---|---|---|---|---|---|
| “Low/Slow Decline” (n = 138, 34.4%) | “Medium/Decline” (n = 263, 52.7%) | “High/Slow Decline” (n = 55, 12.9%) | p-Value 1 | Effect Size2 | |
| Age | 75.46 [79.3, 70.0] | 72.23 [76.0, 68.0] | 70.93 [73.0, 67.3] | <0.001 | 0.08 |
| Women, n (%) | 74 (53.6) | 141 (53.6) | 34 (61.8) | 0.518 | 0.05 |
| Marital status, n (%) | 0.013 | 0.15 | |||
| Never married | 8 (5.8) | 16 (6.1) | 5 (9.1) | ||
| Married | 71 (51.5) | 167 (63.5) | 30 (54.6) | ||
| Divorced | 3 (2.2) | 8 (3.0) | 4 (7.3) | ||
| Widowed | 56 (40.6) | 72 (27.4) | 16 (29.1) | ||
| Level of education, n (%) | <0.001 | 0.19 | |||
| Less than primary education | 80 (58.0) | 116 (44.1) | 16 (29.1) | ||
| Primary education | 43 (31.2) | 80 (30.4) | 13 (23.6) | ||
| Secondary education | 9 (6.5) | 47 (17.9) | 20 (36.4) | ||
| Tertiary education | 6 (4.4) | 20 (7.6) | 6 (11.0) | ||
| Ever worked, n (%) | 101 (73.2) | 217 (82.5) | 47 (85.5) | 0.048 | 0.12 |
| Household income quintiles, n (%) | 0.345 | 0.10 | |||
| 1st (lowest) | 17 (13.8) | 44 (18.0) | 9 (17.3) | ||
| 2nd | 42 (34.2) | 61 (25.0) | 8 (15.4) | ||
| 3rd | 28 (22.8) | 59 (24.2) | 12 (23.1) | ||
| 4th | 25 (20.3) | 58 (23.8) | 17 (32.7) | ||
| 5th (highest) | 11 (9.0) | 22 (9.0) | 6 (11.5) | ||
| Urban, n (%) | 108 (78.3) | 232 (88.2) | 50 (90.9) | 0.012 | 0.14 |
| No. Diseases | 2.63 [3.0, 2.0] | 2.49 [3.0, 2.0] | 2.35 [3.0, 1.0] | 0.395 | 0.13 |
| Diseases, n (%) | |||||
| Diabetes | 37 (26.8) | 57 (21.7) | 8 (14.6) | 0.166 | 0.09 |
| Hypertension | 67 (50.0) | 131 (51.0) | 26 (49.1) | 0.960 | 0.01 |
| Asthma | 16 (11.6) | 27 (10.3) | 4 (7.3) | 0.671 | 0.04 |
| COPD | 23 (16.7) | 26 (9.9) | 8 (14.6) | 0.132 | 0.09 |
| Arthritis | 48 (34.8) | 90 (34.2) | 15 (27.3) | 0.571 | 0.05 |
| Angina pectoris | 11 (8.7) | 24 (9.6) | 6 (11.5) | 0.837 | 0.03 |
| Stroke | 11 (8.0) | 13 (5.0) | 3 (5.5) | 0.469 | 0.06 |
| Depression | 19 (13.8) | 25 (9.5) | 3 (5.5) | 0.185 | 0.09 |
| Tobacco, n (%) | 0.138 | 0.10 | |||
| Never smoked | 89 (64.5) | 159 (60.5) | 32 (58.2) | ||
| Daily smoker | 8 (5.8) | 31 (11.8) | 2 (3.6) | ||
| Not daily smoker | 1 (0.7) | 3 (1.1) | 2 (3.6) | ||
| Not current smoker | 40 (29.0) | 70 (26.6) | 19 (34.6) | ||
| Alcohol, n (%) | 0.390 | 0.09 | |||
| Lifetime abstainer | 39 (40.6) | 103 (31.2) | 22 (36.4) | ||
| Occasional drinker | 43 (31.2) | 76 (29.0) | 13 (23.6) | ||
| Infrequent heavy drinker | 0 (0.0) | 2 (0.8) | 0 (0.0) | ||
| Frequent heavy drinker | 39 (28.3) | 103 (39.2) | 22 (40.0) | ||
| Physical activity level, n (%) | 0.003 | 0.13 | |||
| Low | 48 (34.8) | 75 (28.5) | 11 (20.0) | ||
| Moderate | 62 (44.9) | 121 (46.0) | 18 (32.7) | ||
| High | 28 (20.3) | 67 (25.5) | 26 (47.3) | ||
| WHODAS | 19.57 [33.3, 2.7] | 13.66 [19.4, 0.0] | 10.75 [15.9, 0.0] | <0.001 | 0.04 |
| WHOQOL-Age | 68.58 [78.9, 60.6] | 73.61 [82.6, 65.4] | 76.79 [86.4, 65.6] | <0.001 | 0.03 |
| Immediate verbal memory | 10.64 [13.0, 8.0] | 13.91 [17.0, 11.0] | 17.57 [21.0, 15.0] | <0.001 | 0.21 |
| Delayed verbal memory | 2.20 [3.0, 1.0] | 3.97 [5.0, 3.0] | 6.31 [7.8, 5.0] | <0.001 | 0.39 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bayes-Marin, I.; Fernández, D.; Lara, E.; Martín-María, N.; Miret, M.; Moreno-Agostino, D.; Ayuso-Mateos, J.L.; Sanchez-Niubo, A.; Haro, J.M.; Olaya, B. Trajectories of Immediate and Delayed Verbal Memory in the Spanish General Population of Middle-aged and Older Adults. Brain Sci. 2020, 10, 249. https://doi.org/10.3390/brainsci10040249
Bayes-Marin I, Fernández D, Lara E, Martín-María N, Miret M, Moreno-Agostino D, Ayuso-Mateos JL, Sanchez-Niubo A, Haro JM, Olaya B. Trajectories of Immediate and Delayed Verbal Memory in the Spanish General Population of Middle-aged and Older Adults. Brain Sciences. 2020; 10(4):249. https://doi.org/10.3390/brainsci10040249
Chicago/Turabian StyleBayes-Marin, Ivet, Daniel Fernández, Elvira Lara, Natalia Martín-María, Marta Miret, Darío Moreno-Agostino, José Luis Ayuso-Mateos, Albert Sanchez-Niubo, Josep Maria Haro, and Beatriz Olaya. 2020. "Trajectories of Immediate and Delayed Verbal Memory in the Spanish General Population of Middle-aged and Older Adults" Brain Sciences 10, no. 4: 249. https://doi.org/10.3390/brainsci10040249
APA StyleBayes-Marin, I., Fernández, D., Lara, E., Martín-María, N., Miret, M., Moreno-Agostino, D., Ayuso-Mateos, J. L., Sanchez-Niubo, A., Haro, J. M., & Olaya, B. (2020). Trajectories of Immediate and Delayed Verbal Memory in the Spanish General Population of Middle-aged and Older Adults. Brain Sciences, 10(4), 249. https://doi.org/10.3390/brainsci10040249