Self-Concept and Inattention or Hyperactivity–Impulsivity Symptomatology: The Role of Anxiety

 ,
,  ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Instruments
2.3. Procedure
2.4. Design and Data Analysis
3. Results
3.1. Preliminary Analyses
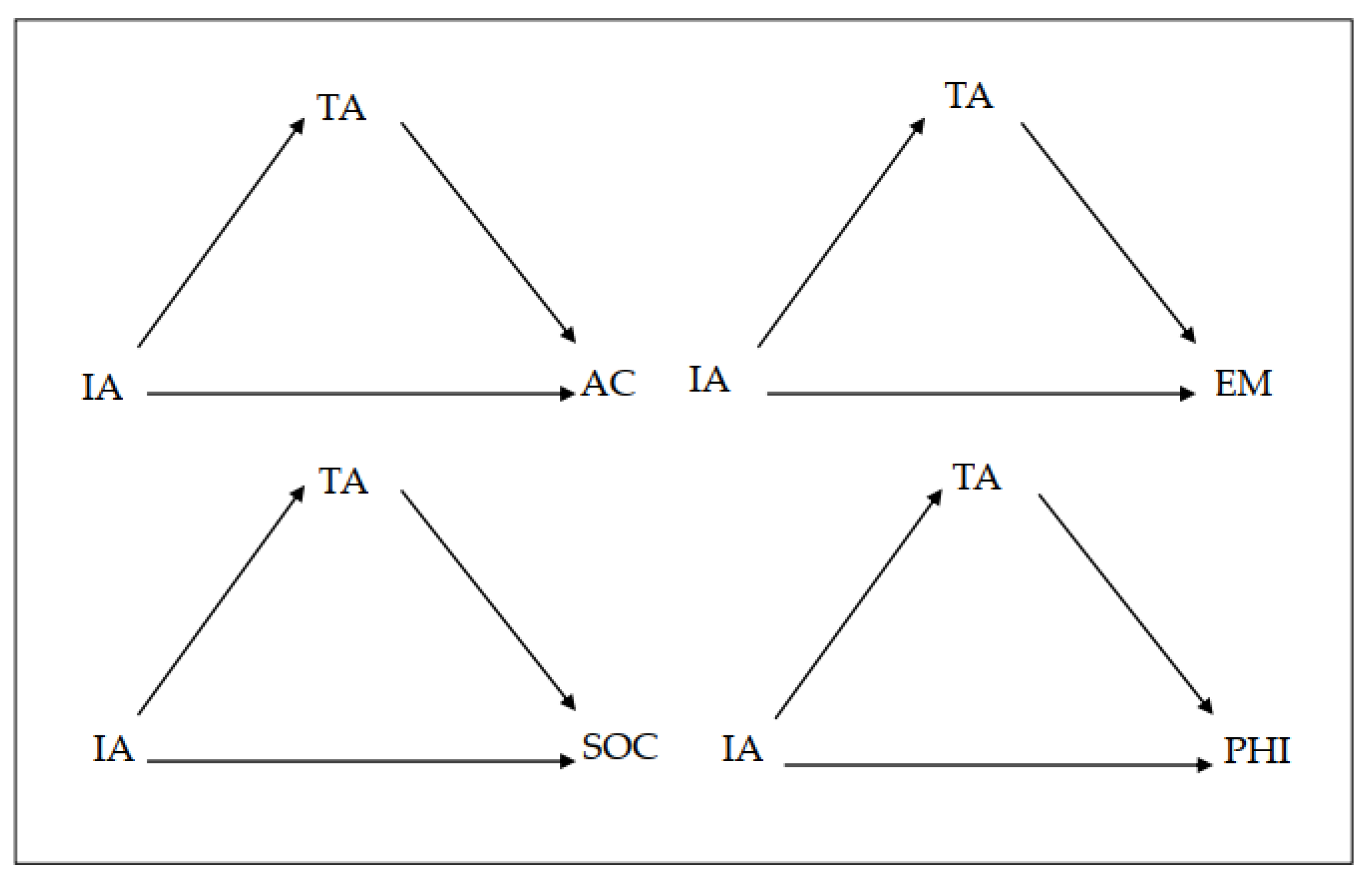
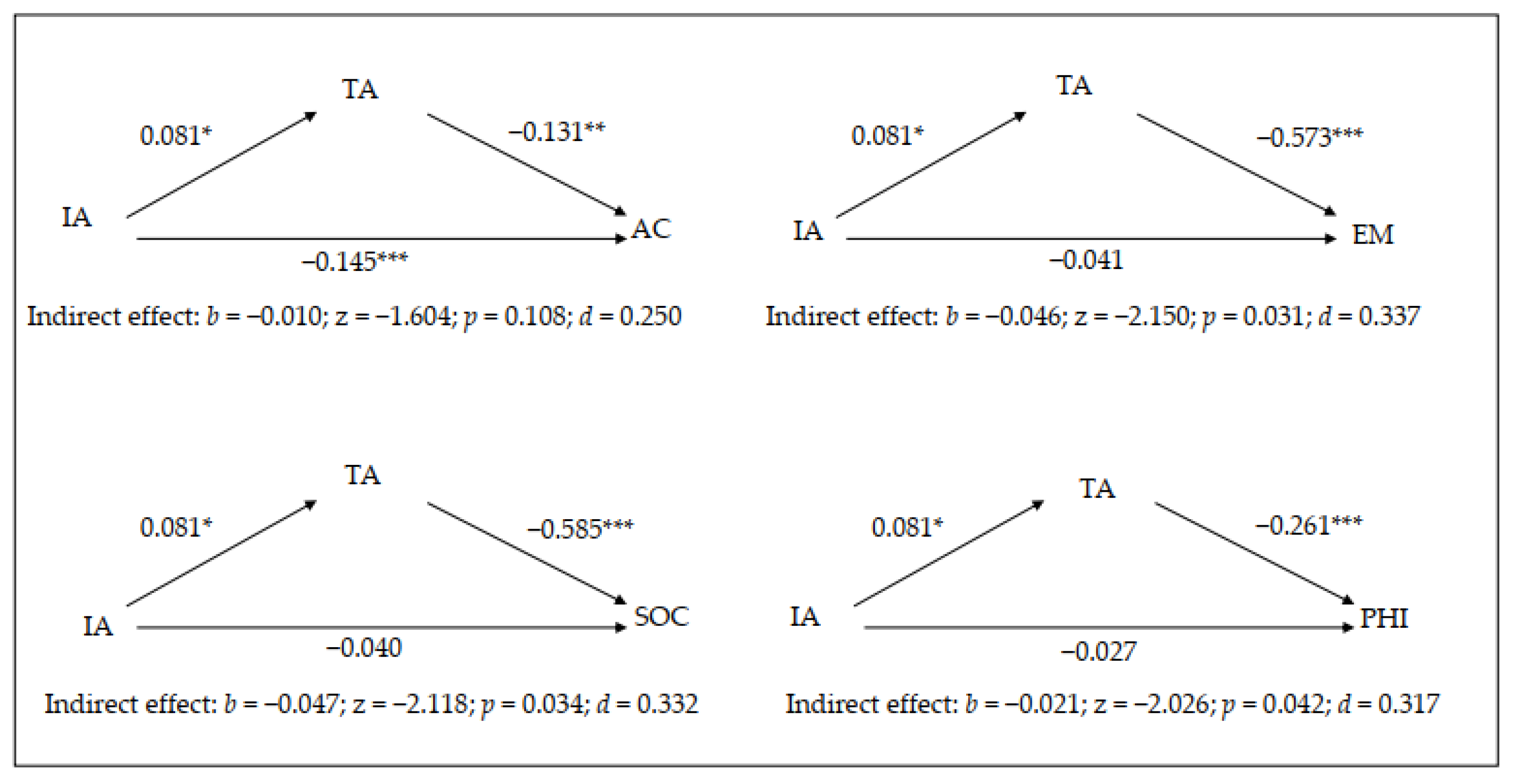
3.2. Mediation Analysis for Inattentive Symptomatology
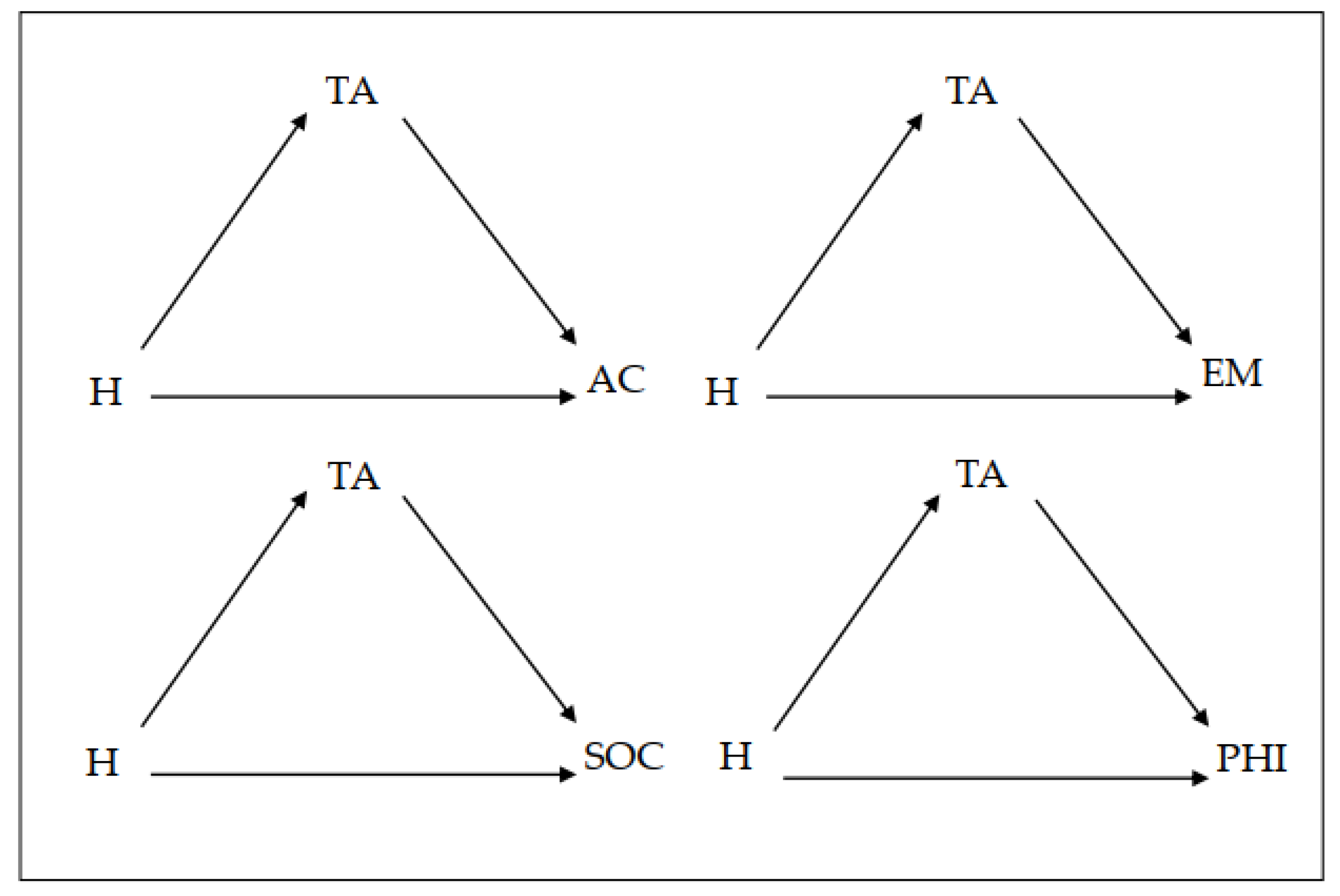
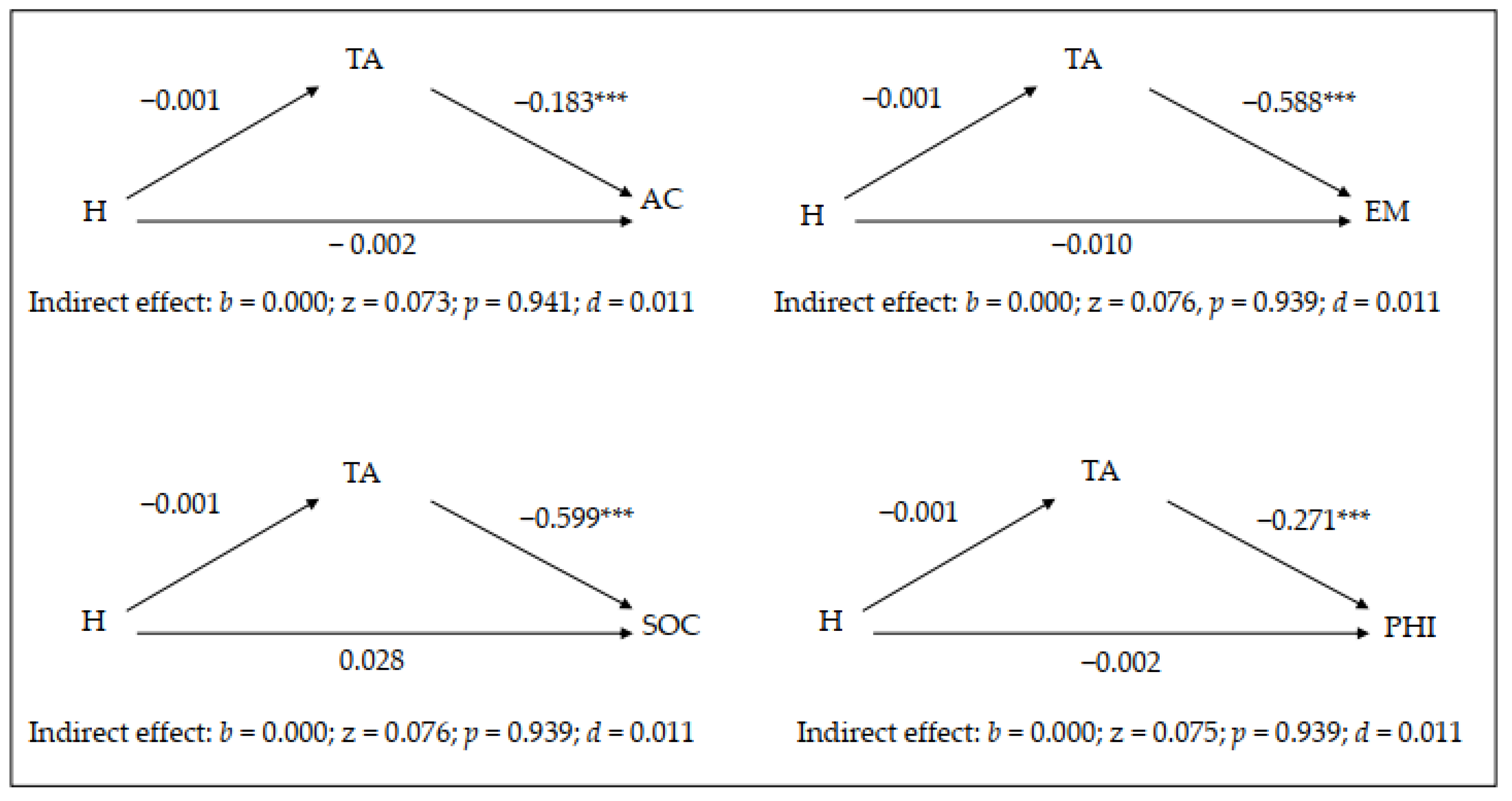
3.3. Mediation Analysis for Hyperactive Symptomatology
3.4. Moderation Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Publishing: Arlington, VA, USA, 2013; ISBN 978-0-89-042555-8. [Google Scholar]
- Polanczyk, G.V.; Willcutt, E.G.; Salum, G.A.; Kieling, C.; Rohde, L.A. ADHD prevalence estimates across three decades: An updated systematic review and meta-regression analysis. Int. J. Epidemiol. 2014, 43, 434–442. [Google Scholar] [CrossRef] [PubMed]
- Harpin, V.; Mazzone, L.; Raynaud, J.P.; Kahle, J.; Hodgkinsm, P. Long-term outcomes of ADHD: A systematic review of self-esteem and social function. J. Atten. Disord. 2016, 20, 295–305. [Google Scholar] [CrossRef] [PubMed]
- Bloemsma, J.M.; Boer, F.; Arnold, R.; Banaschewski, T.; Faraone, S.V.; Buitelaar, J.K.; Sergeant, J.A.; Rommelse, N.; Oosterlaan, J. Comorbid anxiety and neurocognitive dysfunctions in children with ADHD. Eur. Child Adolesc. Psychiatry 2013, 22, 225–234. [Google Scholar] [CrossRef] [Green Version]
- González-Castro, P.; Rodríguez, C.; Cueli, M.; Cabeza, L.; Álvarez, L. Math Competence and Executive Control Skills in Students with Attention Deficit/Hyperactivity Disorder and Mathematics Learning Disabilites. Rev. Psicodidact. 2014, 19, 125–143. [Google Scholar] [CrossRef] [Green Version]
- González-Castro, P.; Rodríguez, C.; Cueli, M.; García, T.; Álvarez-García, D. State, trait anxiety and selective attention differences in Attention Deficit Hyperactivity Disorder (ADHD) subtypes. Int. J. Clin. Health Psychol. 2015, 15, 105–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jarrett, M.A.; Ollendick, T.H. A conceptual review of the comorbidity of ADHD and anxiety: Implications for future research and practice. Clin. Psychol. Rev. 2008, 28, 1266–1280. [Google Scholar] [CrossRef] [PubMed]
- Cumyn, L.; French, L.; Hechtman, L. Comorbidity in adults with attention-deficit hyperactivity disorder. Can. J. Psychiatry 2009, 54, 673–683. [Google Scholar] [CrossRef] [Green Version]
- Brown, T.E. Attention-Deficit Disorders and Comorbidities in Children, Adolescents, and Adults; American Psychiatric Press: Washington, DC, USA, 2000; ISBN 978-0880487115. [Google Scholar]
- Pliszka, S.R.; Carlson, C.; Swanson, J.M. Adhd with Comorbid Disorders: Clinical Assessment and Management; The Guilford Press: New York, NY, USA, 1999; ISBN 978-1572304789. [Google Scholar]
- Castagna, P.J.; Calamia, M.; Davis, T.E. Childhood ADHD and Negative Self-Statements: Important Differences Associated with Subtype and Anxiety Symptoms. Behav. Ther. 2017, 48, 793–807. [Google Scholar] [CrossRef]
- Harter, S. Manual for the Self-Perception Profile for Children; University of Denver: Denver, CO, USA, 1985. [Google Scholar]
- Kita, Y.; Inoue, Y. The Direct/indirect association of aDhD/ODD symptoms with self-esteem, self-perception, and Depression in early adolescents. Front. Psychiatry 2017, 8, e137. [Google Scholar] [CrossRef] [Green Version]
- Danckaerts, M.; Sonuga-Barke, E.J.; Banaschewski, T.; Buitelaar, J.; Döpfner, M.; Hollis, C.; Santosh, P.; Rothenberger, A.; Sergeant, J.; Steinhausen, H.C.; et al. The quality of life of children with attention deficit/hyperactivity disorder: A systematic review. Eur. Child Adolesc. Psychiatry 2010, 19, 83–105. [Google Scholar] [CrossRef] [Green Version]
- Emeh, C.C.; Mikami, A.Y.; Teachman, B.A. Explicit and implicit positive illusory bias in children with ADHD. J. Atten. Disord. 2018, 22, 994–1001. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jia, M.; Jiang, Y.; Mikami, A.Y. Positively Biased Self-Perceptions in Children with ADHD: Unique Predictor of Future Maladjustment. J. Abnorm. Child. Psychol. 2016, 44, 575–586. [Google Scholar] [CrossRef] [PubMed]
- Hoza, B.; McQuade, J.D.; Murray-Close, D.; Shoulberg, E.; Molina, B.S.G.; Arnold, L.E.; Hechtman, L. Does childhood positive self-perceptual bias mediate adolescent risky behavior in youth from the MTA study? J. Consult. Clin. Psychol. 2013, 8, 846–858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, Y.; Johnston, C. Co-occurring aggressive and depressive symptoms as related to overestimations of competence in children with attention-deficit/ hyperactivity disorder. Clin. Child. Fam. Psychol. Rev. 2014, 17, 157–172. [Google Scholar] [CrossRef]
- Gobitta, M.; Guzzo, R.S.L. Initial Study of the Self-Esteem Inventory (SEI) Form A. Psicol-Reflex. Crit. 2002, 15, 143–150. [Google Scholar] [CrossRef]
- Sisto, F.F.; Martinelli, S.C. Escala de Autoconceito Infanto–Juvenil (EAC-IJ); Vetor Editora: São Paulo, Brasil, 2004. [Google Scholar]
- Piers, E.V. The Piers–Harris Children’s Self-Concept Scale, Revised Manual; Western Psychological Services: Los Angeles, CA, USA, 1986. [Google Scholar]
- Barber, S.; Grubbs, L.; Cottrell, B. Self-Perception in children with attention deficit/hyperactivity disorder. J. Pediatr. Nurs. 2005, 20, 235–245. [Google Scholar] [CrossRef]
- Bussing, R.; Zima, B.T.; Perwien, A.R. Self-esteem in special education children with ADHD: Relationship to disorder characteristics and medication use. J. Am. Acad. Child Adolesc. Psychiatry 2000, 39, 1260–1269. [Google Scholar] [CrossRef]
- Gershon, J. A meta-analytic review of gender differences in ADHD. J. Atten. Disord. 2002, 5, 143–154. [Google Scholar] [CrossRef]
- Rucklidge, J.J. Gender differences in ADHD: Implications for psychosocial treatments. Expert. Rev. Neurother. 2008, 8, 643–655. [Google Scholar] [CrossRef]
- Houck, G.; Kendall, J.; Miller, A.; Morrell, P.; Wiebe, G. Self-Concept in Children and Adolescents with Attention Deficit Hyperactivity Disorder. J. Pediatr. Nurs. 2011, 26, 239–247. [Google Scholar] [CrossRef] [Green Version]
- McLennan, J.D. Understanding attention deficit hyperactivity disorder as a continuum. Can. Fam. Physician 2016, 62, 979–982. [Google Scholar] [PubMed]
- Wechsler, D. The Wechsler Intelligence Scale for Children, 4th ed.; Spanish Version; TEA Editions: Madrid, Spain, 2005. [Google Scholar]
- Spielberger, C.D. Manual for the State-Trait Anxiety Inventory; Spanish Version; TEA Editions: Madrid, Spain, 1990. [Google Scholar]
- Farre, A.; Narbona, J. EDAH: Scale for the Assessment of Attention Deficit Hyperactivity Disorder; TEA Editions: Madrid, Spain, 2013. [Google Scholar]
- Morris, K. Revising the Declaration of Helsinki. World Rep. 2013, 381, 1889–1890. [Google Scholar] [CrossRef]
- Hayes, A.F. Introduction to Mediation, Moderation and Conditional Processs Analysis. A Regression Based Approach; Guildford Press: New York, NY, USA, 2013; ISBN 978-1-60918-230-4. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum: Mahwah, NJ, USA, 1988; ISBN 0-8058-0283-5. [Google Scholar]
- McQuade, J.D.; Tomb, M.; Hoza, B.; Waschbusch, D.A.; Hurt, E.A.; Vaughn, A.J. Cognitive Deficits and Positively Biased Self-Perceptions in Children with ADHD. J. Abnorm. Child Psychol. 2011, 39, 307–319. [Google Scholar] [CrossRef] [Green Version]
- Hoza, B.; Murray-Close, D.; Arnold, L.E.; Hinshaw, S.P.; MTA Cooperative Group. Time-dependent changes in positive illusory self-perceptions of children with ADHD: A developmental psychopathology perspective. Dev. Psychopathol. 2010, 22, 375–390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaiser, N.M.; Hoza, B.; Pelham, W.E.; Gnagy, E.; Greiner, A.R. ADHD status and degree of positive illusions: Moderational and meditational relations with actual behavior. J. Atten. Disord. 2008, 12, 227–238. [Google Scholar] [CrossRef] [PubMed]
- Hoza, B.; Mrug, S.; Gerdes, A.C.; Bukowski, W.M.; Gold, J.A.; Kraemer, H.S.; Pelham, W.E.; Wigal, T.; Arnold, L.E. What aspects of peer relationships are impaired in children with Attention-Deficit/Hyperactivity Disorder? J. Consult. Clin. Psychol. 2005, 73, 411–423. [Google Scholar] [CrossRef] [Green Version]
- Hodgens, J.B.; Cole, J.; Boldizar, J. Peer-based differences among boys with ADHD. J. Clin. Child Psychol. 2000, 29, 443–452. [Google Scholar] [CrossRef] [PubMed]
- Christiansen, H.; Hirsch, O.; Albrecht, B.; Chavanon, M. Attention-Deficit/Hyperactivity Disorder (ADHD) and Emotion Regulation over the Life Span. Curr. Psychiatry Rep. 2019, 21, e17. [Google Scholar] [CrossRef] [PubMed]
- Bériault, M.; Turgeon, L.; Labrosse, M.; Berthiaume, C.; Verreault, M.; Berthiaume, C.; Godbout, R. Comorbidity of ADHD and Anxiety Disorders in School-Age Children: Impact on Sleep and Response to a Cognitive-Behavioral Treatment. J. Atten. Disord. 2018, 22, 414–424. [Google Scholar] [CrossRef]
- Thorell, L.B.; Sjöwall, D.; Diamatopoulou, S.; Rydell, A.M.; Bohlin, G. Emotional functioning, ADHD symptoms, and peer problems: A longitudinal investigation of children age 6–9.5 years. Infant. Child Dev. 2017, 26, 1–13. [Google Scholar] [CrossRef]
- Jensen, P.S.; Hinshaw, S.P.; Kraemer, H.C.; Lenora, N.; Newcorn, J.H.; Abikoff, H.B.; March, J.S.; Arnold, L.E.; Cantwell, D.P.; Conners, C.K.; et al. ADHD comorbidity findings from the MTA study: Comparing comorbid subgroups. J. Am. Acad. Child Adolesc. Psychiatry 2001, 40, 147–158. [Google Scholar] [CrossRef] [PubMed]
- García, T.; Rodríguez, C.; Rodríguez, J.; Fernández-Suárez, A.; Richarte, V.; Ramos-Quiroga, J.A. Psychosocial profiles of adults with ADHD: A comparative study of prison and outpatient psychiatric samples. Eur. J. Psychol. Appl. Leg. Context 2014, 11, 41–49. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Academic | Emotional | Social | Physical | TA | IA | H | Age | |
|---|---|---|---|---|---|---|---|---|
| Academic | − | |||||||
| Emotional | 0.364 *** | − | ||||||
| Social | 0.181 * | 0.456 *** | − | |||||
| Physical | 0.314 *** | 0.472 *** | 0.468 *** | − | ||||
| TA | −0.250 *** | −0.613 *** | −0.516 *** | −0.423 *** | − | |||
| IA | −0.424 *** | −0.146 | −0.158 * | −0.112 | 0.116 | − | ||
| H | −0.011 | −0.026 | 0.101 | 0.002 | −0.022 | 0.047 | − | |
| Age | −0.163 * | 0.022 | 0.172 * | −0.073 | −0.055 | 0.038 | −0.073 | − |
| M | 14.24 | 26.00 | 30.32 | 18.56 | 34.89 | 89.28 | 64.78 | 13.77 |
| SD | 5.33 | 7.15 | 8.19 | 4.88 | 7.37 | 15.51 | 28.30 | 1.24 |
| SK | 0.43 | −0.53 | −1.07 | −0.68 | 0.50 | −3.09 | −0.52 | 0.16 |
| K | −0.14 | −0.14 | 0.48 | −0.15 | −0.09 | 10.81 | −0.92 | −0.67 |
| Min | 4 | 5 | 7 | 5 | 20 | 10 | 5 | 11 |
| Max | 29 | 39 | 42 | 26 | 57 | 99 | 99 | 16.83 |
| Coefficient | SE | t | p | d | LLCI | ULCI | |
|---|---|---|---|---|---|---|---|
| DV: Trait Anxiety | |||||||
| IA | 0.081 | 0.036 | 2.223 | 0.027 | 0.349 | 0.091 | 0.154 |
| Gender | 3.995 | 1.246 | 3.204 | 0.001 | 0.511 | 1.533 | 6.456 |
| DV: Academic self−concept | |||||||
| TA | −0.131 | 0.051 | −2.541 | 0.012 | 0.401 | −0.233 | −0.029 |
| IA | −0.145 | 0.024 | −5.913 | 0.000 | 1.029 | −0.194 | −0.097 |
| Gender | −1.076 | 0.850 | −1.265 | 0.207 | 0.196 | −2.756 | 0.603 |
| DV: Emotional self−concept | |||||||
| TA | −0.573 | 0.061 | −9.258 | 0.000 | 2.053 | −0.695 | −0.451 |
| IA | −0.041 | 0.029 | −1.418 | 0.158 | 0.220 | −0.100 | 0.016 |
| Gender | −0.904 | 1.019 | −0.887 | 0.376 | 0.137 | −2.917 | 1.108 |
| DV: Social self−concept | |||||||
| TA | −0.585 | 0.076 | −7.654 | 0.000 | 1.470 | −0.736 | −0.434 |
| IA | −0.040 | 0.036 | −1.102 | 0.271 | 0.171 | −0.112 | 0.031 |
| Gender | 1.645 | 1.258 | 1.307 | 0.193 | 0.203 | −0.840 | 4.131 |
| DV: Physical self−concept | |||||||
| TA | −0.261 | 0.048 | −5.393 | 0.000 | 0.918 | −0.357 | −0.165 |
| IA | −0.027 | 0.023 | −1.184 | 0.238 | 0.184 | −0.073 | 0.018 |
| Gender | −0.964 | 0.798 | −1.208 | 0.228 | 0.187 | −2.540 | 0.611 |
| Coefficient | SE | t | P | d | LLCI | ULCI | |
|---|---|---|---|---|---|---|---|
| DV: Trait Anxiety | |||||||
| H | −0.001 | 0.020 | −0.076 | 0.939 | 0.011 | −0.040 | 0.037 |
| Gender | 3.359 | 1.236 | 2.716 | 0.007 | 0.429 | 0.917 | 5.800 |
| DV: Academic self−concept | |||||||
| TA | −0.183 | 0.056 | −3.273 | 0.001 | 0.523 | −0.294 | −0.072 |
| H | −0.002 | 0.014 | −0.202 | 0.839 | 0.031 | −0.031 | 0.025 |
| Gender | 0.207 | 0.908 | 0.228 | 0.819 | 0.035 | −1.586 | 2.001 |
| DV: Emotional self−concept | |||||||
| TA | −0.588 | 0.061 | −9.602 | 0.000 | 2.220 | −0.709 | −0.467 |
| H | −0.010 | 0.015 | −0.689 | 0.491 | 0.106 | −0.041 | 0.020 |
| Gender | −0.584 | 0.992 | −0.588 | 0.556 | 0.091 | −2.543 | 1.375 |
| DV: Social self−concept | |||||||
| TA | −0.599 | 0.075 | −7.975 | 0.000 | 1.568 | −0.747 | −0.450 |
| H | 0.028 | 0.019 | 1.484 | 0.139 | 0.231 | −0.009 | 0.066 |
| Gender | 2.142 | 1.216 | 1.761 | 0.080 | 0.275 | −0.258 | 4.543 |
| DV: Physical self−concept | |||||||
| TA | −0.271 | 0.048 | −5.657 | 0.000 | 0.973 | −0.366 | −0.176 |
| H | −0.002 | 0.012 | −0.230 | 0.817 | 0.035 | −0.027 | 0.021 |
| Gender | −0.734 | 0.776 | −0.945 | 0.345 | 0.146 | −2.267 | 0.799 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cueli, M.; Rodríguez, C.; Cañamero, L.M.; Núñez, J.C.; González-Castro, P. Self-Concept and Inattention or Hyperactivity–Impulsivity Symptomatology: The Role of Anxiety. Brain Sci. 2020, 10, 250. https://doi.org/10.3390/brainsci10040250
Cueli M, Rodríguez C, Cañamero LM, Núñez JC, González-Castro P. Self-Concept and Inattention or Hyperactivity–Impulsivity Symptomatology: The Role of Anxiety. Brain Sciences. 2020; 10(4):250. https://doi.org/10.3390/brainsci10040250
Chicago/Turabian StyleCueli, Marisol, Celestino Rodríguez, Laura M. Cañamero, José Carlos Núñez, and Paloma González-Castro. 2020. "Self-Concept and Inattention or Hyperactivity–Impulsivity Symptomatology: The Role of Anxiety" Brain Sciences 10, no. 4: 250. https://doi.org/10.3390/brainsci10040250
APA StyleCueli, M., Rodríguez, C., Cañamero, L. M., Núñez, J. C., & González-Castro, P. (2020). Self-Concept and Inattention or Hyperactivity–Impulsivity Symptomatology: The Role of Anxiety. Brain Sciences, 10(4), 250. https://doi.org/10.3390/brainsci10040250