Behavioral and Autonomic Responses in Treating Children with High-Functioning Autism Spectrum Disorder: Clinical and Phenomenological Insights from Two Case Reports




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.1.1. Subject 1—J
2.1.2. Subject 2—B
2.2. The c.m.i.® Approach
2.3. Training According to the Cognitive Motivational Intervention (c.m.i.®)
- Interview with the parents: During the interview, the parents were informed about the aims and modalities of the training approach and their involvement in the process. In addition, informed consent was obtained from the parents of the two girls enrolled, after receiving an exhaustive explanation of the study. Such explanation included: (a) the description of the theory of the cognitive motivational intervention; (b) the rationale of physiological signal acquisition and the procedures for data collection; (c) detailed description of home procedures; (d) the description of the re-elaboration of acquired experiences through drawing; (e) the modalities of using icons by the children.
- Observation of the two girls: This aimed at identifying the individual characteristics of the two girls. J. loves drawing and adds plenty of particulars in her drawings, although images look quite static. Conversely, B. is constantly in motion and uses continuous, redundant, sophisticated and dyspragmatic language. She does not like drawing, but rather prefers moving and talking. She has difficulties in maintaining task concentration. In order to manage individual differences among the subjects, meetings with parents were organized in order to explain to them the individual phenotypic profile of their child and how to manage the emotional experience of the child as well as their own. Specifically, therapists contacted the parents four times a month after the initial meeting.
- Training to realize the procedures: The parents were instructed how to guide the two girls in the acquisition of specific procedures, which consisted in cooking the girls’ favorite foods (spaghetti for J. and biscuits for B.). Then, the girls were helped in acquiring information about the environments in which they were supposed to cook (which objects to use and where they are located). Once a week, the two girls were involved in making up their favorite food.
2.4. Evaluation of the Acquired Procedure
2.5. Physiological Signal Acquisition
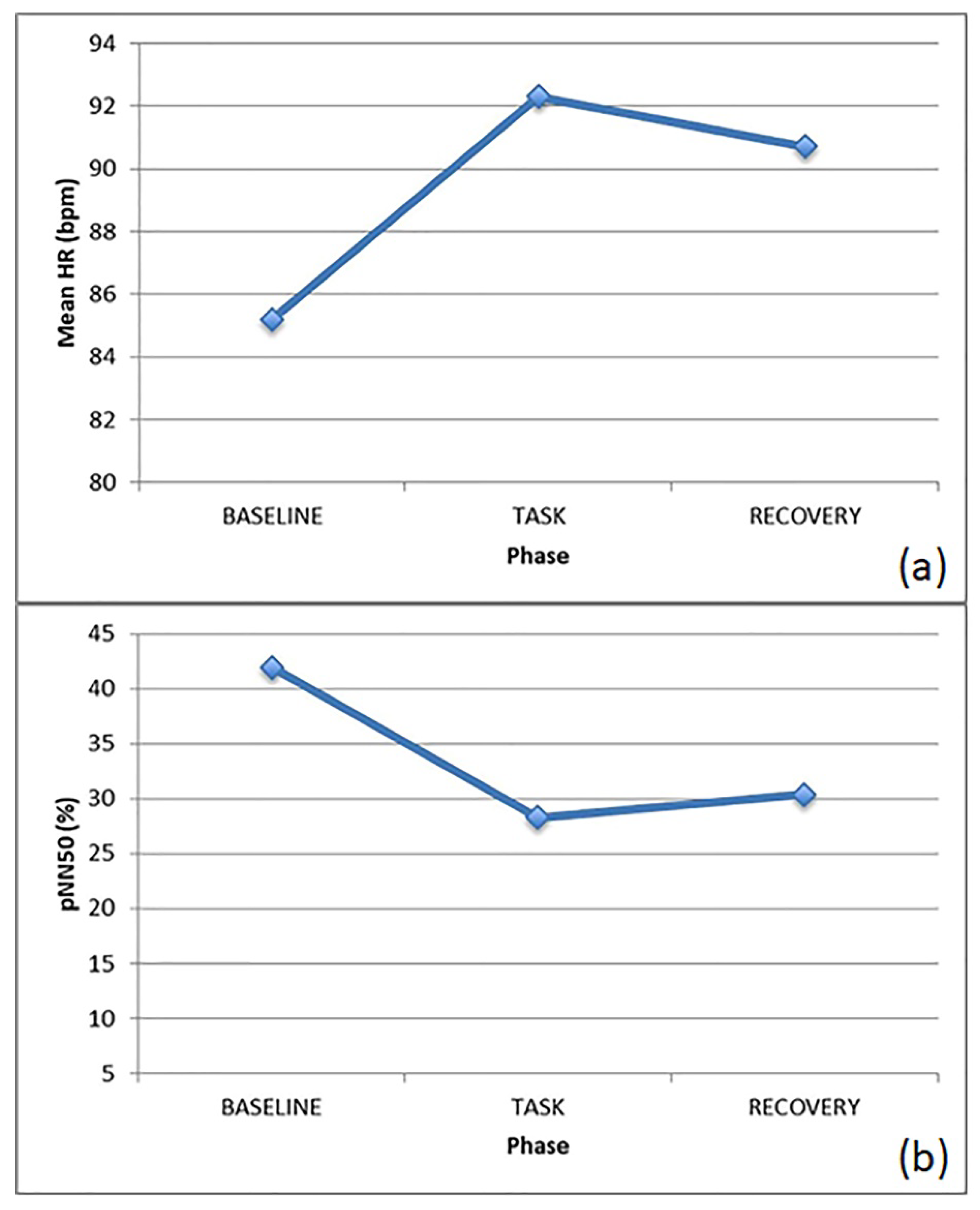
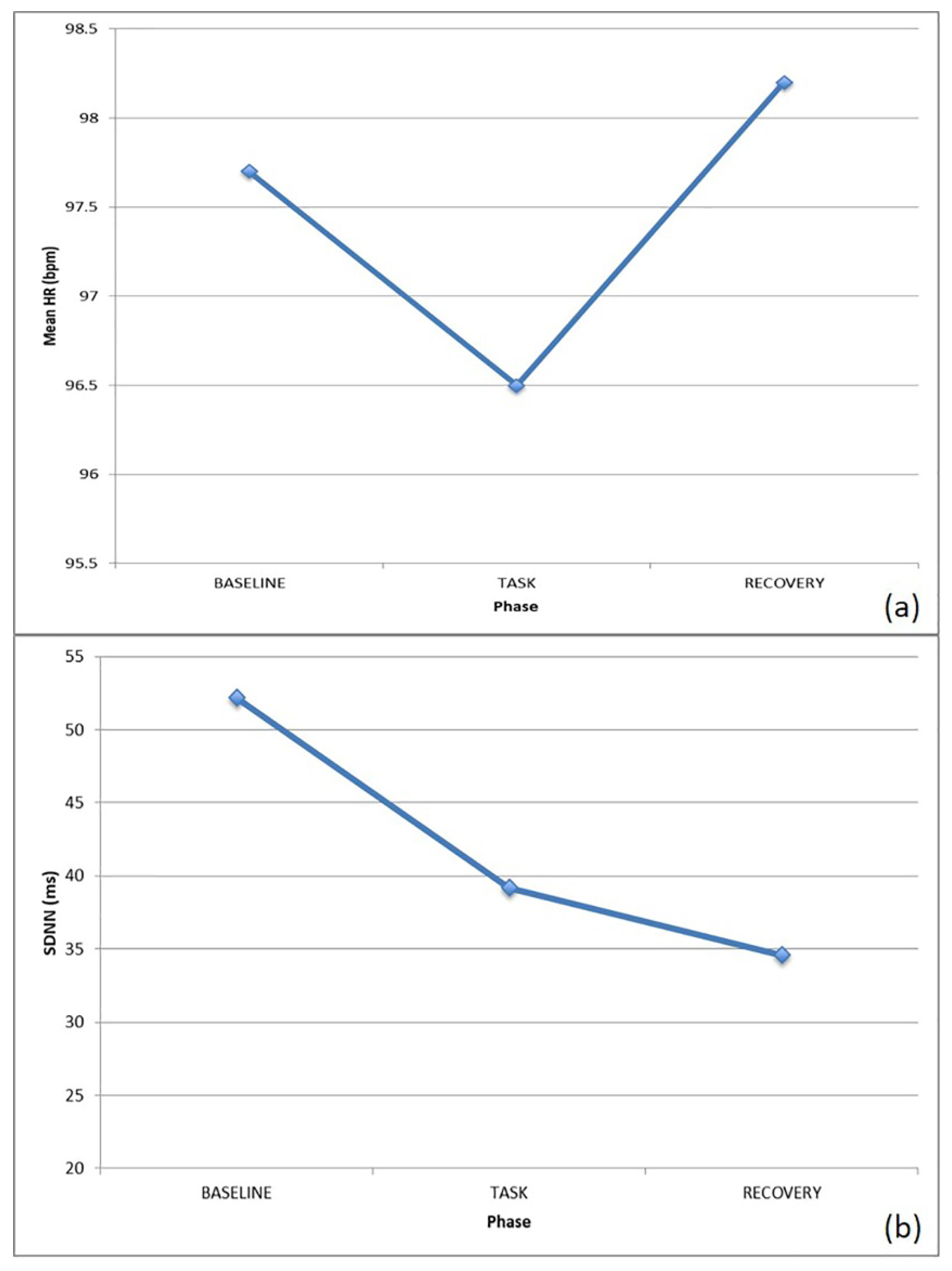
- Baseline (3′): Basal measurement. Here, the subject was asked to stay as still as possible.
- Task (15′): Signal acquisition during the proposed tasks.
- Recovery (3′): Post-task basal measurement. The subject was required to stay as still as possible, similar to baseline.
2.6. Physiological Signal Analysis
- Heart rate (HR): the number of contractions of the heart occurring per time unit, expressed in bpm;
- Standard deviation of normal to normal RR intervals (SDNN): measure of heart rate variability (HRV), expressed in ms;
- Normalized component of the power spectral density of the ECG signal at low frequency (0.04–0.15 Hz) (nLF), which is related both to the sympathetic and parasympathetic response;
- Normalized component of the power spectral density of the ECG spectrum at high frequency (0.15–0.4 Hz) (nHF), which is mainly related to the parasympathetic response;
- Low versus high frequency components of the power spectral density of the ECG spectrum (LF/HF Ratio), which expresses the balance between the sympathetic and parasympathetic nervous system branches.
3. Results
3.1. Behavioral Observations
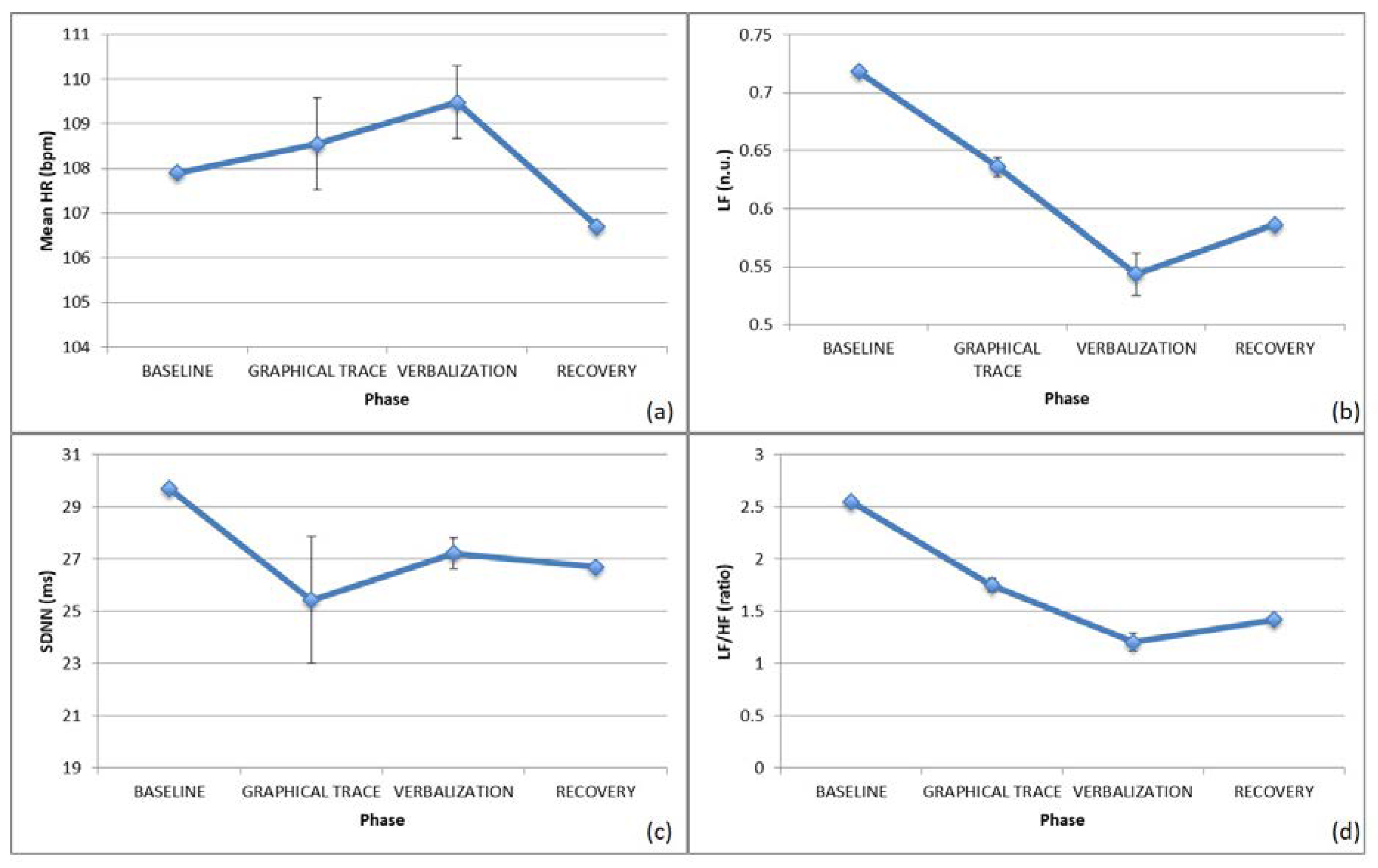
3.2. Autonomic Nervous System Response—Graphical Trace
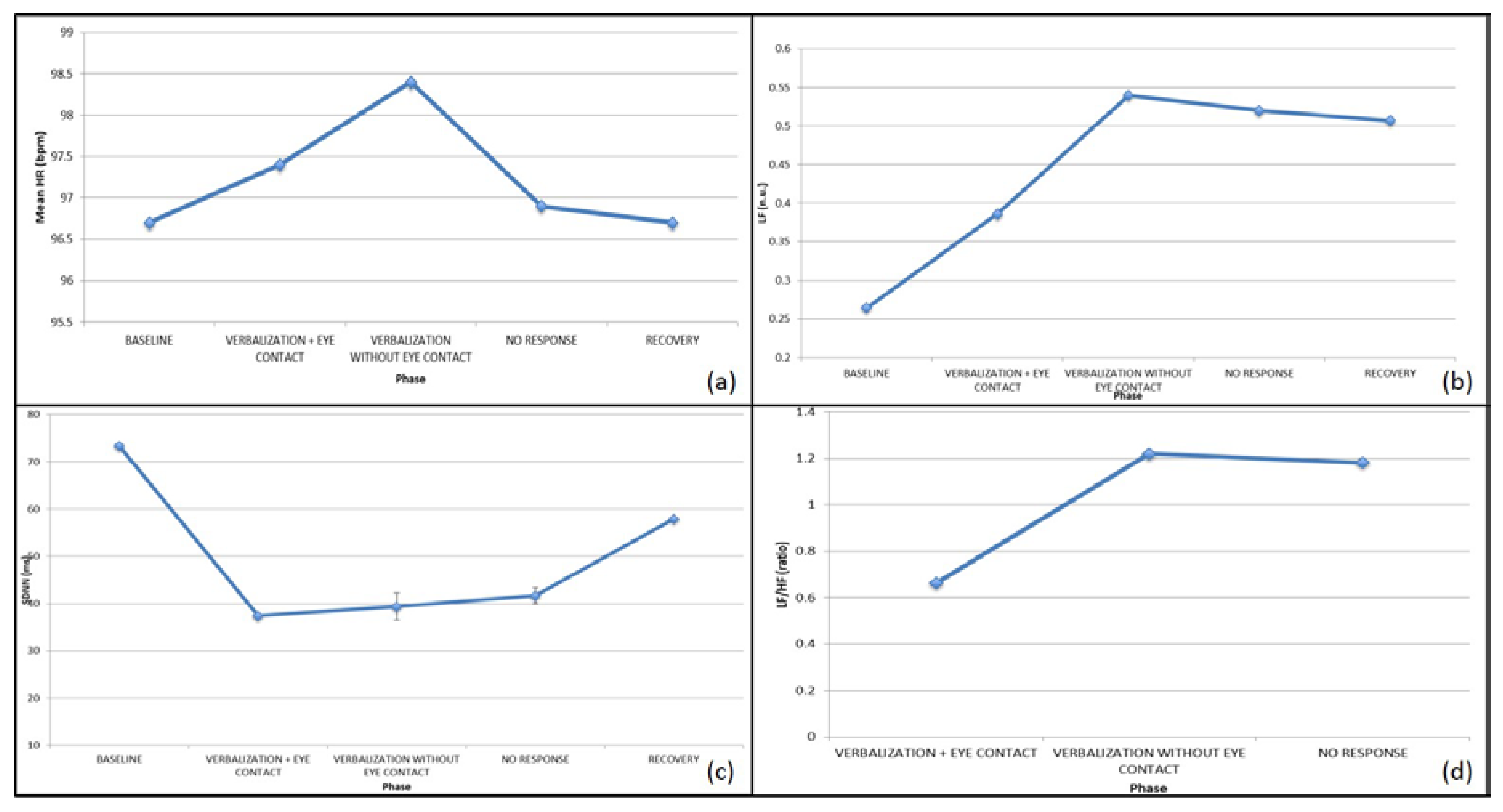
3.3. Autonomic Nervous System Response—Action on the Represented
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Beadle-Brown, J.; Wilkinson, D.; Richardson, L.; Shaughnessy, N.; Trimingham, M.; Leigh, J.; Whelton, B.; Himmerich, J. Imagining Autism: Feasibility of a drama-based intervention on the social, communicative and imaginative behaviour of children with autism. Autism 2018, 22, 915–927. [Google Scholar] [CrossRef]
- Gava, M.L.; Caterino, E. Autismo: Pensiero, azione, comunicazione. L’applicazione del metodo c.m.i.® (cognitivo-motivazionale-individualizzato) a soggetti con autismo a basso funzionamento. Autismo Disturbi Dello Svilupp. 2014, 12, 249–271. [Google Scholar]
- Pennington, B.F.; Rogers, S.J.; Bennetto, L.; Griffith, E.M.; Reed, D.T.; Shyu, V. Validity tests of the executive dysfunction hypothesis of autism. In Autism as an Executive Disorder; Russell, J., Ed.; Oxford University Press (OUP): Oxford, UK, 1997; pp. 143–178. [Google Scholar]
- Peristeri, E.; Baldimtsi, E.; Andreou, M.; Tsimpli, I.M. The impact of bilingualism on the narrative ability and the executive functions of children with autism spectrum disorders. J. Commun. Disord. 2020, 85, 105999. [Google Scholar] [CrossRef]
- Narzisi, A.; Muratori, F.; Calderoni, S.; Fabbro, F.; Urgesi, C. Neuropsychological Profile in High Functioning Autism Spectrum Disorders. J. Autism Dev. Disord. 2012, 43, 1895–1909. [Google Scholar] [CrossRef]
- Gava, M.L. La Comunicazione Aumentativa Alternativa tra Pensiero e Parola; Franco Angeli: Milan, Italy, 2013. [Google Scholar]
- King, D.; Dockrell, J.E.; Stuart, M. Event narratives in 11-14 year olds with autistic spectrum disorder. Int. J. Lang. Commun. Disord. 2013, 48, 522–533. [Google Scholar] [CrossRef] [PubMed]
- Losh, M.; Capps, L. Narrative ability in high-functioning children with autism or Asperger’s syndrome. J. Autism Dev. Disord. 2003, 33, 239–251. [Google Scholar] [CrossRef] [PubMed]
- Peristeri, E.; Andreou, M.; Tsimpli, I.M. Syntactic and Story Structure Complexity in the Narratives of High- and Low-Language Ability Children with Autism Spectrum Disorder. Front. Psychol. 2017, 8, 2027. [Google Scholar] [CrossRef] [Green Version]
- Dawson, G.; Finley, C.; Phillips, S.; Lewy, A. A comparison of hemispheric asymmetries in speech-related brain potentials of autistic and dysphasic children. Brain Lang. 1989, 37, 26–41. [Google Scholar] [CrossRef]
- Romanczyk, R.; Gillis, J.M.; Baron, M.G.; Groden, J.; Groden, G.; Lipsitt, L.P. Autism and the Physiology of Stress and Anxiety. In Stress and Coping in Autism; Baron, M.G., Groden, J., Groden, G., Lipsitt, L., Eds.; Oxford University Press (OUP): Oxford, UK, 2006; pp. 183–204. [Google Scholar]
- Faja, S.; Murias, M.; Beauchaine, T.P.; Dawson, G. Reward-based decision making and electrodermal responding by young children with autism spectrum disorders during a gambling task. Autism Res. 2013, 6, 494–505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sheinkopf, S.J.; Neal-Beevers, A.R.; Levine, T.P.; Miller-Loncar, C.; Lester, B. Parasympathetic Response Profiles Related to Social Functioning in Young Children with Autistic Disorder. Autism Res. Treat. 2013, 2013, 868396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neuhaus, E.; Bernier, R.; Beauchaine, T.P. Brief Report: Social Skills, Internalizing and Externalizing Symptoms, and Respiratory Sinus Arrhythmia in Autism. J. Autism Dev. Disord. 2013, 44, 730–737. [Google Scholar] [CrossRef]
- Porges, S.W. The polyvagal theory: Phylogenetic substrates of a social nervous system. Int. J. Psychophysiol. 2001, 42, 123–146. [Google Scholar] [CrossRef]
- Porges, S.W. The Polyvagal Theory: Phylogenetic contributions to social behavior. Physiol. Behav. 2003, 79, 503–513. [Google Scholar] [CrossRef]
- Bal, E.; Harden, E.; Lamb, D.; Van Hecke, A.V.; Denver, J.W.; Porges, S.W. Emotion Recognition in Children with Autism Spectrum Disorders: Relations to Eye Gaze and Autonomic State. J. Autism Dev. Disord. 2010, 40, 358–370. [Google Scholar] [CrossRef] [PubMed]
- Neuhaus, E.; Bernier, R.A.; Beauchaine, T.P. Children with Autism Show Altered Autonomic Adaptation to Novel and Familiar Social Partners. Autism Res. 2016, 9, 579–591. [Google Scholar] [CrossRef] [PubMed]
- Stifter, C.A.; Dollar, J.M.; Cipriano, E.A. Temperament and emotion regulation: The role of autonomic nervous system reactivity. Dev. Psychobiol. 2011, 53, 266–279. [Google Scholar] [CrossRef] [PubMed]
- Diamond, L.M.; Cribbet, M.R. Links between adolescent sympathetic and parasympathetic nervous system functioning and interpersonal behavior over time. Int. J. Psychophysiol. 2013, 88, 339–348. [Google Scholar] [CrossRef] [PubMed]
- Hubert, B.; Wicker, B.; Monfardini, E.; Deruelle, C. Electrodermal reactivity to emotion processing in adults with autistic spectrum disorders. Autism 2009, 13, 9–19. [Google Scholar] [CrossRef]
- Mathersul, D.C.; McDonald, S.; Rushby, J. Autonomic arousal explains social cognitive abilities in high-functioning adults with autism spectrum disorder. Int. J. Psychophysiol. 2013, 89, 475–482. [Google Scholar] [CrossRef]
- Lord, C.; Risi, S.; Lambrecht, L., Jr.; Cook, E.H.; Leventhal, B.L.; DiLavore, P.C.; Pickles, A.; Rutter, M. The Autism Diagnostic Observation Schedule—Generic: A Standard Measure of Social and Communication Deficits Associated with the Spectrum of Autism. J. Autism Dev. Disord. 2000, 30, 205–223. [Google Scholar] [CrossRef] [PubMed]
- Lewis, M.; Norbury, C.; Luyster, R.; Schmitt, L.; McDuffie, A.; Haebig, E.; Murray, D.S.; Timler, G.; Frazier, T.; Holmes, D.L.; et al. Leiter International Performance Scale-Revised (Leiter-R). In Encyclopedia of Autism Spectrum Disorders; Volkmar, F.R., Ed.; Springer: New York, NY, USA, 2013. [Google Scholar]
- Villardita, C. Raven’s colored Progressive Matrices and intellectual impairment in patients with focal brain damage. Cortex 1985, 21, 627–634. [Google Scholar] [CrossRef]
- Wechsler, D. WPPSI-III: Technical and Interpretative Manual; The Psychological Corporation: San Antonio, TX, USA, 2002. [Google Scholar]
- Schreibman, L.; Dawson, G.; Stahmer, A.C.; Landa, R.J.; Rogers, S.J.; McGee, G.G.; Kasari, C.; Ingersoll, B.; Kaiser, A.; Bruinsma, Y.; et al. Naturalistic Developmental Behavioral Interventions: Empirically Validated Treatments for Autism Spectrum Disorder. J. Autism Dev. Disord. 2015, 45, 2411–2428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Green, J.; Charman, T.; McConachie, H.; Aldred, C.; Slonims, V.; Howlin, P.; Le Couteur, A.; Leadbitter, K.; Hudry, K.; Byford, S.; et al. Parent-mediated communication-focused treatment in children with autism (PACT): A randomised controlled trial. Lancet 2010, 375, 2152–2160. [Google Scholar] [CrossRef] [Green Version]
- Johnson-Glenberg, M.C.; Megowan-Romanowicz, C. Embodied science and mixed reality: How gesture and motion capture affect physics education. Cogn. Res. Princ. Implic. 2017, 2, 27. [Google Scholar] [CrossRef] [Green Version]
- Pan, J.; Tompkins, W.J. A real-time QRS detection algorithm. IEEE Trans. Biomed. Eng. 1985, 32, 230–236. [Google Scholar] [CrossRef]
- Benedek, M.; Kaernbach, C. A continuous measure of phasic electrodermal activity. J. Neurosci. Methods 2010, 190, 80–91. [Google Scholar] [CrossRef] [Green Version]
- Billeci, L.; Tonacci, A.; Narzisi, A.; Manigrasso, Z.; Varanini, M.; Fulceri, F.; Lattarulo, C.; Calderoni, S.; Muratori, F. Heart Rate Variability During a Joint Attention Task in Toddlers With Autism Spectrum Disorders. Front. Physiol. 2018, 9, 467. [Google Scholar] [CrossRef] [Green Version]
- Tonacci, A.; Di Monte, J.; Meucci, M.B.; Sansone, F.; Pala, A.P.; Billeci, L.; Conte, R. Wearable Sensors to Characterize the Autonomic Nervous System Correlates of Food-Like Odors Perception: A Pilot Study. Electronics 2019, 8, 1481. [Google Scholar] [CrossRef] [Green Version]
- Sahin, M.; Sur, M. Genes, circuits, and precision therapies for autism and related neurodevelopmental disorders. Science 2015, 350, aab3897. [Google Scholar] [CrossRef] [Green Version]
- Waschbusch, D.A.; Willoughby, M.T.; Haas, S.M.; Ridenour, T.; Helseth, S.; Crum, K.I.; Altszuler, A.R.; Ross, J.M.; Coles, E.K.; Pelham, W.E. Effects of Behavioral Treatment Modified to Fit Children with Conduct Problems and Callous-Unemotional (CU) Traits. J. Clin. Child Adolesc. Psychol. 2019, 1–12. [Google Scholar] [CrossRef]
- Grove, R.; Roth, I.; Hoekstra, R.A. The motivation for special interests in individuals with autism and controls: Development and validation of the special interest motivation scale. Autism Res. 2016, 9, 677–688. [Google Scholar] [CrossRef] [PubMed]
- White, S.W.; Schry, A.R.; Miyazaki, Y.; Ollendick, T.H.; Scahill, L. Effects of Verbal Ability and Severity of Autism on Anxiety in Adolescents With ASD: One-Year Follow-Up After Cognitive Behavioral Therapy. J. Clin. Child Adolesc. Psychol. 2015, 44, 839–845. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hesselmark, E.; Plenty, S.; Bejerot, S. Group cognitive behavioural therapy and group recreational activity for adults with autism spectrum disorders: A preliminary randomized controlled trial. Autism 2014, 18, 672–683. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirkovski, M.; Enticott, P.; Fitzgerald, P.B. A Review of the Role of Female Gender in Autism Spectrum Disorders. J. Autism Dev. Disord. 2013, 43, 2584–2603. [Google Scholar] [CrossRef]
- Di Palma, S.; Tonacci, A.; Narzisi, A.; Domenici, C.; Pioggia, G.; Muratori, F.; Billeci, L. Monitoring of autonomic response to sociocognitive tasks during treatment in children with Autism Spectrum Disorders by wearable technologies: A feasibility study. Comput. Biol. Med. 2017, 85, 143–152. [Google Scholar] [CrossRef] [PubMed]
- Billeci, L.; Tonacci, A.; Tartarisco, G.; Narzisi, A.; Di Palma, S.; Corda, D.; Baldus, G.; Cruciani, F.; Anzalone, S.M.; Calderoni, S.; et al. An Integrated Approach for the Monitoring of Brain and Autonomic Response of Children with Autism Spectrum Disorders during Treatment by Wearable Technologies. Front. Mol. Neurosci. 2016, 10, 799. [Google Scholar] [CrossRef] [Green Version]






© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Billeci, L.; Caterino, E.; Tonacci, A.; Gava, M.L. Behavioral and Autonomic Responses in Treating Children with High-Functioning Autism Spectrum Disorder: Clinical and Phenomenological Insights from Two Case Reports. Brain Sci. 2020, 10, 382. https://doi.org/10.3390/brainsci10060382
Billeci L, Caterino E, Tonacci A, Gava ML. Behavioral and Autonomic Responses in Treating Children with High-Functioning Autism Spectrum Disorder: Clinical and Phenomenological Insights from Two Case Reports. Brain Sciences. 2020; 10(6):382. https://doi.org/10.3390/brainsci10060382
Chicago/Turabian StyleBilleci, Lucia, Ettore Caterino, Alessandro Tonacci, and Maria Luisa Gava. 2020. "Behavioral and Autonomic Responses in Treating Children with High-Functioning Autism Spectrum Disorder: Clinical and Phenomenological Insights from Two Case Reports" Brain Sciences 10, no. 6: 382. https://doi.org/10.3390/brainsci10060382
APA StyleBilleci, L., Caterino, E., Tonacci, A., & Gava, M. L. (2020). Behavioral and Autonomic Responses in Treating Children with High-Functioning Autism Spectrum Disorder: Clinical and Phenomenological Insights from Two Case Reports. Brain Sciences, 10(6), 382. https://doi.org/10.3390/brainsci10060382