The Disengagement of Visual Attention: An Eye-Tracking Study of Cognitive Impairment, Ethnicity and Age



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Neuropsychological Assessments
2.3. Eye Tracking Tasks
2.3.1. Apparatus
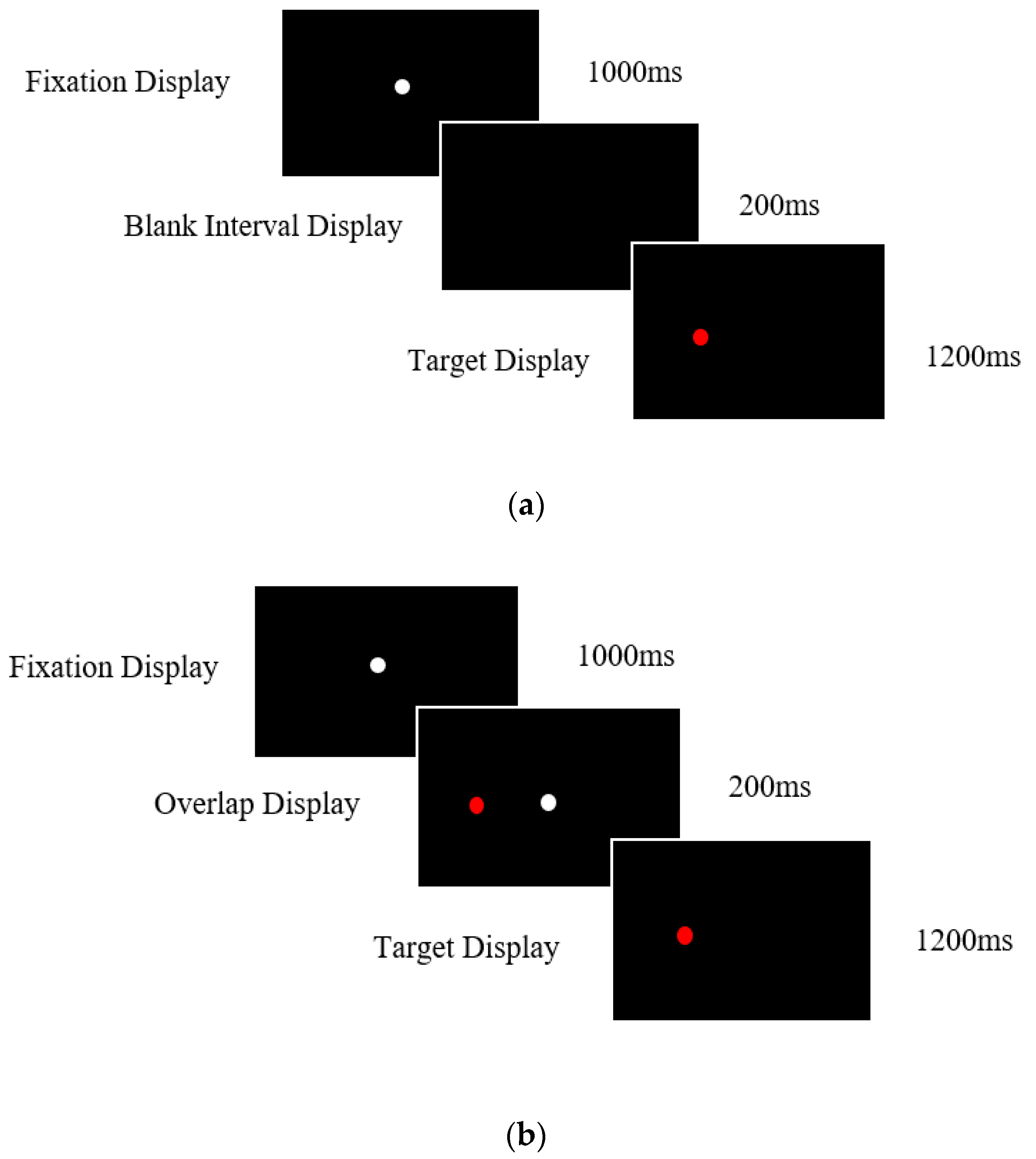
2.3.2. Prosaccade Task
2.4. Data Analysis
3. Results
3.1. Neuropsychological Tests
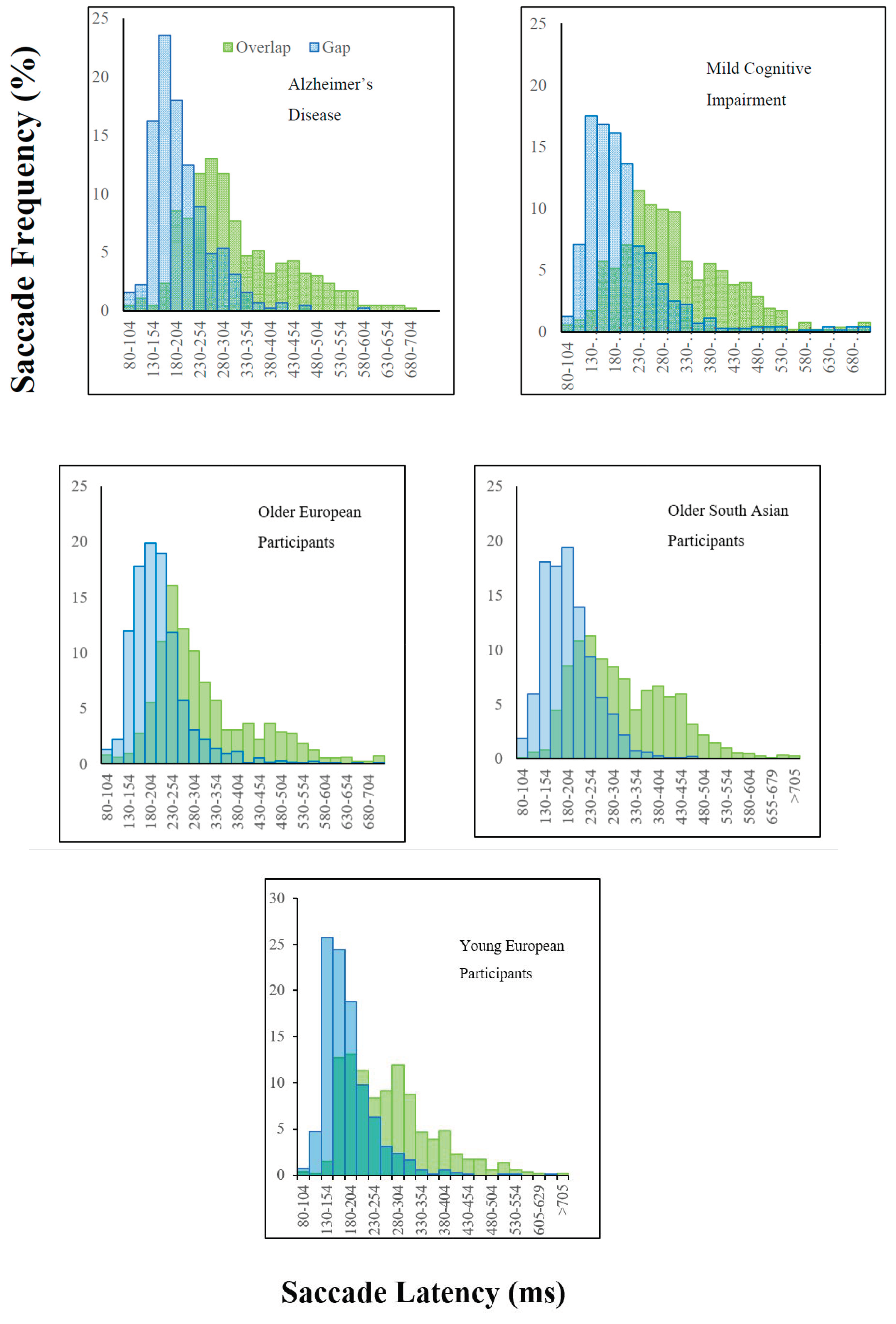
3.2. The “Gap” Effect
3.3. Attentional Disengagement: Effects of Ageing
3.4. Attentional Disengagement: Effects of Cognitive Impairment
3.5. Attentional Disengagement: Ethnicity/Cultural Effects
3.6. Correlations
4. Discussion
4.1. What Does the Gap Effect Reveal about the Integrity of the Alzheimer Brain?
4.2. Ageing
4.3. Ethnicity
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kaufman, L.D.; Pratt, J.; Levine, B.; Black, S.E. Antisaccades: A probe into the dorsolateral prefrontal cortex in Alzheimer’s disease. A critical review. J. Alzheimer’s Dis. 2010, 19, 781–793. [Google Scholar] [CrossRef] [Green Version]
- Belleville, S.; Bherer, L.; Lepage, É.; Chertkow, H.; Gauthier, S. Task switching capacities in persons with Alzheimer’s disease and mild cognitive impairment. Neuropsychologia 2008, 46, 2225–2233. [Google Scholar] [CrossRef] [PubMed]
- Baddeley, A.; Chincotta, D.; Adlam, A. Working memory and the control of action: Evidence from task switching. J. Exp. Psychol. Gen. 2001, 130, 641. [Google Scholar] [CrossRef]
- Solfrizzi, V.; Panza, F.; Torres, F.; Capurso, C.; D’Introno, A.; Colacicco, A.M.; Capurso, A. Selective attention skills in differentiating between Alzheimer’s disease and normal aging. J. Geriatr. Psychiatry Neurol. 2002, 15, 99–109. [Google Scholar] [CrossRef] [PubMed]
- Awh, E.; Jonides, J. Spatial working memory and spatial selective. In Attention in The Attentive Brain; Parasuraman, R., Ed.; MIT Press: Cambridge, MA, USA, 1998; pp. 353–380. [Google Scholar]
- Della Sala, S.; Laiacona, M.; Spinnler, H.; Ubezio, C.A. A Cancellation test: Its reliability in assessing attentional deficits in Alzheimer’s disease. Psychol. Med. 1992, 22, 885–901. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baddeley, A.; Baddeley, H.A.; Bucks, R.S.; Wilcock, G.K. Attentional control in Alzheimer’s disease. Brain 2001, 124, 1492–1508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perry, R.J.; Hodges, J.R. Attention and executive deficits in Alzheimer’s Disease; a critical review. Brain 1999, 122, 383–404. [Google Scholar] [CrossRef] [Green Version]
- Parasuraman, R.; Haxby, J.V. Attention and brain function in Alzheimer’s disease: A review. Neuropsychology 1993, 7, 242–272. [Google Scholar] [CrossRef]
- Parasuraman, R.; Greenwood, P.M. Selective attention in aging and dementia. In The Attentive Brain; Parasuraman, R., Ed.; MIT Press: Cambridge, MA, USA, 1998; pp. 461–487. [Google Scholar]
- Posner, M.I.; Cohen, Y.; Rafal, R.D. Neural systems control of spatial orienting. Philos. Trans. R. Soc. Lond. Ser. B Biol. Sci. 1982, 298, 187–198. [Google Scholar]
- Posner, M.I.; Petersen, S.E. The attention system of the human brain. Annu. Rev. Neurosci. 1990, 13, 25–42. [Google Scholar] [CrossRef]
- Caffarra, P.; Riggio, L.; Malvezzi, L.; Scaglioni, A.; Freedman, M. Orienting of visual attention in Alzheimer’s disease: Its implication in favor of the interhemispheric balance. Neuropsychiatry Neuropsychol. Behav. Neurol. 1997, 10, 90–95. [Google Scholar] [PubMed]
- Faust, M.E.; Balota, D.A. Inhibition of return and visuospatial attention in healthy older adults and individuals with dementia of the Alzheimer type. Neuropsychology 1997, 11, 13–29. [Google Scholar] [CrossRef] [PubMed]
- Boxer, A.L.; Garbutt, S.; Rankin, K.P.; Hellmuth, J.; Neuhaus, J.; Miller, B.L.; Lisberger, S.G. Medial versus lateral frontal lobe contributions to voluntary saccade control as revealed by the study of patients with frontal lobe degeneration. J. Neurosci. 2006, 26, 6354–6363. [Google Scholar] [CrossRef] [PubMed]
- Crawford, T.J.; Higham, S.; Renvoize, T.; Patel, J.; Dale, M.; Suriya, A.; Tetley, S. Inhibitory control of saccadic eye movements and cognitive impairment in Alzheimer’s disease. Biol. Psychiatry 2005, 57, 1052–1060. [Google Scholar] [CrossRef]
- Crawford, T.J.; Higham, S.; Mayes, J.; Dale, M.; Shaunak, S.; Lekwuwa, G. The role of working memory and attentional disengagement on inhibitory control: Effects of aging and Alzheimer’s disease. Age 2013, 35, 1637–1650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crawford, T.J. The disengagement of visual attention in Alzheimer’s disease: A longitudinal eye-tracking study. Front. Aging Neurosci. 2015, 7, 118. [Google Scholar] [CrossRef] [Green Version]
- Kaufman, L.D.; Pratt, J.; Levine, B.; Black, S.E. Executive deficits detected in mild Alzheimer’s disease using the antisaccade task. Brain Behav. 2012, 2, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Wilcockson, T.D.; Mardanbegi, D.; Xia, B.; Taylor, S.; Sawyer, P.; Gellersen, H.W.; Crawford, T.J. Abnormalities of saccadic eye movements in dementia due to Alzheimer’s disease and mild cognitive impairment. Aging 2019, 2019 11, 5389. [Google Scholar]
- Crawford, T.J.; Higham, S. Distinguishing between impairments of working memory and inhibitory control in cases of early dementia. Neuropsychologia 2016, 81, 61–67. [Google Scholar] [CrossRef] [Green Version]
- Fischer, B.; Boch, R. Saccadic eye movements after extremely short reaction times in the monkey. Brain Res. 1983, 260, 21–26. [Google Scholar] [CrossRef]
- Fischer, B.; Weber, H. Express saccades and visual attention. Behav. Brain Sci. 1993, 16, 553–567. [Google Scholar] [CrossRef] [Green Version]
- Goldring, J.; Fischer, B. Reaction times of vertical prosaccades and antisaccades in gap and overlap tasks. Exp. Brain Res. 1997, 113, 88–103. [Google Scholar] [CrossRef] [PubMed]
- Crawford, T.J.; Parker, E.; Solis-Trapala, I.; Mayes, J. Is the relationship of prosaccade reaction times and antisaccade errors mediated by working memory? Exp. Brain Res. 2011, 208, 385–397. [Google Scholar] [CrossRef] [PubMed]
- Saslow, M.G. Effects of components of displacement-step stimuli upon latency for saccadic eye movement. Josa 1967, 57, 1024–1029. [Google Scholar] [CrossRef]
- Rolfs, M.; Vitu, F. On the limited role of target onset in the gap task: Support for the motor-preparation hypothesis. J. Vis. 2007, 7, 7. [Google Scholar] [CrossRef] [Green Version]
- Vernet, M.; Yang, Q.; Gruselle, M.; Trams, M.; Kapoula, Z. Switching between gap and overlap pro-saccades: Cost or benefit? Exp. Brain Res. 2009, 197, 49. [Google Scholar] [CrossRef]
- Kapoula, Z.; Yang, Q.; Vernet, M.; Dieudonné, B.; Greffard, S.; Verny, M. Spread deficits in initiation, speed and accuracy of horizontal and vertical automatic saccades in dementia with Lewy bodies. Front. Neurol. 2010, 1, 138. [Google Scholar] [CrossRef] [Green Version]
- Yang, Q.; Wang, T.; Su, N.; Xiao, S.; Kapoula, Z. Specific saccade deficits in patients with Alzheimer’s disease at mild to moderate stage and in patients with amnestic mild cognitive impairment. Age 2013, 35, 1287–1298. [Google Scholar] [CrossRef] [Green Version]
- Chehrehnegar, N.; Nejati, V.; Shati, M.; Esmaeili, M.; Rezvani, Z.; Haghi, M.; Foroughan, M. Behavioral and cognitive markers of mild cognitive impairment: Diagnostic value of saccadic eye movements and Simon task. Aging Clin. Exp. Res. 2019, 31, 1591–1600. [Google Scholar] [CrossRef]
- Rad, M.S.; Martingano, A.J.; Ginges, J. Toward a psychology of Homo sapiens: Making psychological science more representative of the human population. Proc. Natl. Acad. Sci. USA 2018, 115, 11401–11405. [Google Scholar] [CrossRef] [Green Version]
- Knox, P.C.; Amatya, N.; Jiang, X.; Gong, Q. Performance deficits in a voluntary saccade task in Chinese “express saccade makers”. PLoS ONE 2012, 7, e47688. [Google Scholar] [CrossRef]
- Mardanbegi, D.; Wilcockson, T.D.W.; Killick, R.; Xia, B.; Gellersen, H.; Sawyer, P.; Crawford, T.J. A comparison of post-saccadic oscillations in European-Born and China-Born British University Undergraduates. PLoS ONE 2020, 15, e0229177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lenoble, Q.; Bubbico, G.; Szaffarczyk, S.; Pasquier, F.; Boucart, M. Scene categorization in Alzheimer’s disease: A saccadic choice task. Dement. Geriatr. Cogn. Disord. Extra 2015, 5, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Wechsler, D. WAIS-III: Administration and Scoring Manual: Wechsler Adult Intelligence Scale, 3rd ed.; Psychological Corporation: New York, NY, USA, 1997. [Google Scholar]
- Mardanbegi, D.; Wilcockson, T.; Sawyer, P.; Gellersen, H.; Crawford, T. SaccadeMachine: Software for analyzing saccade tests (anti-saccade and pro-saccade). In Proceedings of the 11th ACM Symposium on Eye Tracking Research & Applications, Denver, CO, USA, 25–28 June 2019; pp. 1–8. [Google Scholar]
- Dorris, M.C.; Munoz, D.P. A neural correlate for the gap effect on saccadic reaction times in monkey. J. Neurophysiol. 1995, 73, 2558–2562. [Google Scholar] [CrossRef]
- Dorris, M.C.; Pare, M.; Munoz, D.P. Neuronal activity in monkey superior colliculus related to the initiation of saccadic eye movements. J. Neurosci. 1997, 17, 8566–8579. [Google Scholar] [CrossRef] [Green Version]
- Findlay, J.M.; Walker, R. A model of saccade generation based on parallel processing and competitive inhibition. Behav. Brain Sci. 1999, 22, 661–674. [Google Scholar] [CrossRef]
- Hutton, S.B.; Ettinger, U. The antisaccade task as a research tool in psychopathology: A critical review. Psychophysiology 2006, 43, 302–313. [Google Scholar] [CrossRef] [Green Version]
- Broerse, A.; Crawford, T.J.; Den Boer, J.A. Parsing cognition in schizophrenia using saccadic eye movements: A selective overview. Neuropsychologia 2001, 39, 742–756. [Google Scholar] [CrossRef]
- Crawford, T.; Taylor, S.; Mardanbegi, D.; Polden, M.; Wilcockson, T.; Killick, R.; Sawyer, P.; Gellersen, H.; Leroi, I. The Effects of Previous Error and Success in Alzheimer’s Disease and Mild Cognitive Impairment. Sci. Rep. 2019, 9. [Google Scholar] [CrossRef]
- Fischer, P.; Jungwirth, S.; Zehetmayer, S.; Weissgram, S.; Hoenigschnabl, S.; Gelpi, E.; Krampla, W.; Tragl, K.H. Conversion from subtypes of mild cognitive impairment to Alzheimer dementia. Neurology 2007, 68, 288–291. [Google Scholar] [CrossRef] [PubMed]
- Yaffe, K.; Petersen, R.C.; Lindquist, K.; Kramer, J.; Miller, B. Subtype of mild cognitive impairment and progression to dementia and death. Dement. Geriatr. Cogn. Disord. 2006, 22, 312–319. [Google Scholar] [CrossRef]
- Ward, A.; Tardiff, S.; Dye, C.; Arrighi, H.M. Rate of conversion from prodromal Alzheimer’s disease to Alzheimer’s dementia: A systematic review of the literature. Dement. Geriatr. Cogn. Dis. Extra 2013, 3, 320–332. [Google Scholar] [CrossRef]
- Salthouse, T.A. The processing-speed theory of adult age differences in cognition. Psychol. Rev. 1996, 103, 403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crawford, T.J.; Smith, E.; Berry, D. Eye gaze and Ageing: Selective and combined effects of working memory and inhibitory control. Front. Hum. Neurosci. 2017, 11, 563. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salthouse, T.A. When does age-related cognitive decline begin? Neurobiol. Aging 2009, 30, 507–514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peltsch, A.; Hemraj, A.; Garcia, A.; Munoz, D.P. Age-related trends in saccade characteristics among the elderly. Neurobiol. Aging 2011, 32, 669–679. [Google Scholar] [CrossRef]
- Amatya, N.; Gong, Q.; Knox, P.C. Differing proportions of ‘express saccade makers’ in different human populations. Exp. Brain Res. 2011, 210, 117–129. [Google Scholar] [CrossRef] [Green Version]
- Delinte, A.; Gomez, C.M.; Decostre, M.F.; Crommelinck, M.; Roucoux, A. Amplitude transition function of human express saccades. Neurosci. Res. 2002, 42, 21–34. [Google Scholar] [CrossRef]
- Rayner, K.; Li, X.; Williams, C.C.; Cave, K.R.; Well, A.D. Eye movements during information processing tasks: Individual differences and cultural effects. Vis. Res. 2007, 47, 2714–2726. [Google Scholar] [CrossRef] [Green Version]
- Alotaibi, A.; Underwood, G.; Smith, A.D. Cultural differences in attention: Eye movement evidence from a comparative visual search task. Conscious. Cogn. 2017, 55, 254–265. [Google Scholar] [CrossRef] [PubMed]
- Chua, H.F.; Boland, J.E.; Nisbett, R.E. Cultural variation in eye movements during scene perception. Proc. Natl. Acad. Sci. USA 2005, 102, 12629–12633. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knox, P.C.; Wolohan, F.D. Cultural diversity and saccade similarities: Culture does not explain saccade latency differences between Chinese and European participants. PLoS ONE 2014, 9, e94424. [Google Scholar] [CrossRef]
- Kim, H.S.; Sherman, D.K.; Taylor, S.E.; Sasaki, J.Y.; Chu, T.Q.; Ryu, C.; Xu, J. Culture, serotonin receptor polymorphism and locus of attention. Soc. Cogn. Affect. Neurosci. 2010, 5, 212–218. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Older European Participants | Older South Asian Participants | Alzheimer’s Disease | MCI | Young European Participants | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | M | SD | M | SD | |
| MoCA | 27.80 | 2.04 | 22.04 | 4.99 | 20.19 | 5.45 | 22.98 | 5.40 | 28.14 | 1.94 |
| Digit Span Task | 17.91 | 4.60 | 13.27 | 3.71 | 15.23 | 4.56 | 15.95 | 4.12 | 19.86 | 4.33 |
| Spatial Span Task | 13.89 | 2.44 | 12.47 | 2.24 | 11.42 | 3.75 | 12.93 | 3.08 | 17.38 | 2.08 |
| Post Hoc Contracts (p Values) | |||||
|---|---|---|---|---|---|
| Disease Effects | Ageing Effects | Ethnicity Effects | |||
| AD vs. OEP | AD vs. MCI | MCI vs. OEP | OEP vs. YEP | OEP vs. OSP | |
| MoCA | <0.001 * | 0.007 * | <0.001 * | 0.025 | <0.001 * |
| Digit Span Task | 0.015 * | 0.496 | 0.043 | 0.015 * | <0.001 * |
| Spatial Span Task | <0.001 * | 0.021 * | 0.077 | <0.001 * | 0.002 * |
| Older European Participants N = 96 | Older South Asian Participants N = 94 | Alzheimer’s Disease N = 32 | MCI N = 45 | Young European Participants N = 44 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | M | SD | M | SD | |
| Gap | 195 | 38.87 | 212 | 37.06 | 206 | 30.93 | 200 | 42.18 | 185 | 31.60 |
| Overlap | 305 | 75.06 | 315 | 75.06 | 312 | 51.32 | 310 | 66.86 | 272 | 58.83 |
| Gap Effect (ms) (Overlap-Gap) | 110 | 57.30 | 103 | 58.66 | 106 | 48.06 | 110 | 59.54 | 87 | 48.53 |
| Post Hoc Contracts (p Values) | |||||
|---|---|---|---|---|---|
| Disease Effects | Ageing Effects | Ethnicity Effects | |||
| AD vs. OEP | AD vs. MCI | MCI vs. OEP | OEP vs. YEP | OEP vs. OSP | |
| Gap | 0.004 * | 0.161 | <0.001 * | 0.007 * | <0.001 * |
| Overlap | 0.718 | 0.972 | 0.706 | <0.001 * | 0.016 * |
| Gap Effect (Overlap-Gap) | 0.707 | 0.885 | 0.803 | 0.022 * | 0.383 |
| Variable | MoCA | Digit Span Total | Digit Span Forward | Digit Span Backward | Spatial Span Total | Spatial Span Forward | Spatial Span Backward | |
|---|---|---|---|---|---|---|---|---|
| Gap Effect (Overlap-Gap) | AD | −0.063 | 0.120 | 0.048 | 0.169 | 0.157 | 0.242 | 0.058 |
| MCI | −0.096 | −0.076 | −0.118 | −0.015 | −0.168 | 0.021 | −0.318 * | |
| OEP | −0.095 | −0.004 | −0.014 | −0.031 | −0.014 | 0.025 | −0.045 | |
| OSP | 0.213 | 0.153 | 0.144 | 0.126 | −0.024 | −0.028 | −0.013 | |
| YEP | 0.147 | −0.013 | 0.070 | −0.088 | 0.074 | 0.071 | 0.043 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Polden, M.; Wilcockson, T.D.W.; Crawford, T.J. The Disengagement of Visual Attention: An Eye-Tracking Study of Cognitive Impairment, Ethnicity and Age. Brain Sci. 2020, 10, 461. https://doi.org/10.3390/brainsci10070461
Polden M, Wilcockson TDW, Crawford TJ. The Disengagement of Visual Attention: An Eye-Tracking Study of Cognitive Impairment, Ethnicity and Age. Brain Sciences. 2020; 10(7):461. https://doi.org/10.3390/brainsci10070461
Chicago/Turabian StylePolden, Megan, Thomas D. W. Wilcockson, and Trevor J. Crawford. 2020. "The Disengagement of Visual Attention: An Eye-Tracking Study of Cognitive Impairment, Ethnicity and Age" Brain Sciences 10, no. 7: 461. https://doi.org/10.3390/brainsci10070461
APA StylePolden, M., Wilcockson, T. D. W., & Crawford, T. J. (2020). The Disengagement of Visual Attention: An Eye-Tracking Study of Cognitive Impairment, Ethnicity and Age. Brain Sciences, 10(7), 461. https://doi.org/10.3390/brainsci10070461