Distinguishing and Biochemical Phenotype Analysis of Epilepsy Patients Using a Novel Serum Profiling Platform

 , , , ,
, , , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Direct Electrospray Mass Spectrometry (ESI-MS) of Sera from Patients With Epilepsy and Control Subjects
2.3. Statistical Analysis
2.4. Test Metrics
3. Results
3.1. Distinguishing Sera of a Patient Group with Epilepsy from a Control Individual Group Using LOOCV/PCV ESI-MS
3.2. Distinguishing Blinded Epilepsy Sera Samples, and LOOCV with a Low-Cost Desk Top Mass Spectrometer
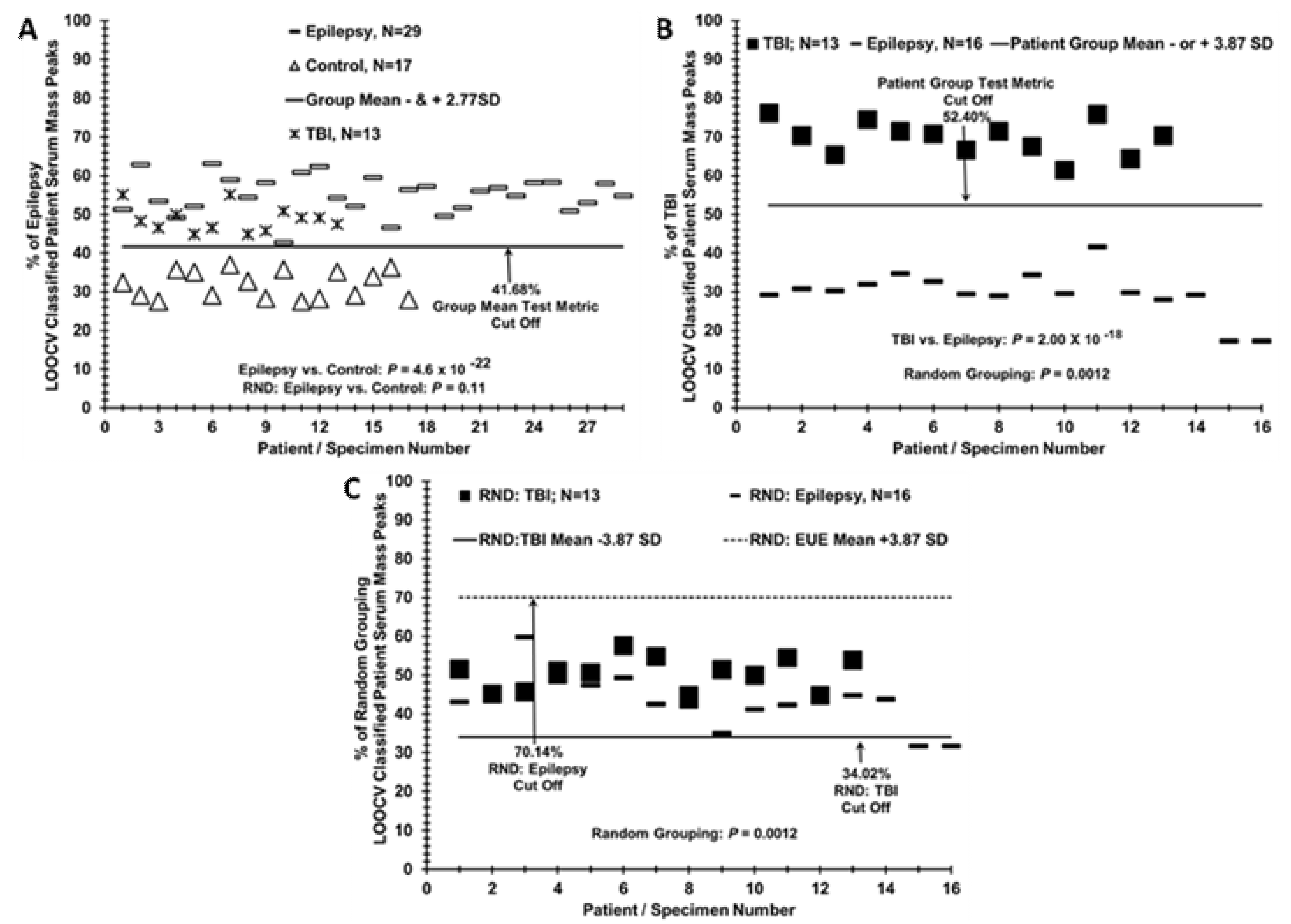
3.3. Epilepsy Patient Sera Segregates from TBI Patient Sera when Compared to Controls but Segregates from TBI Patient Sera when Compared Directly
3.4. Test Metric Data for Epilepsy, Control, and TBI Serum LOOCV Profiling Comparisons
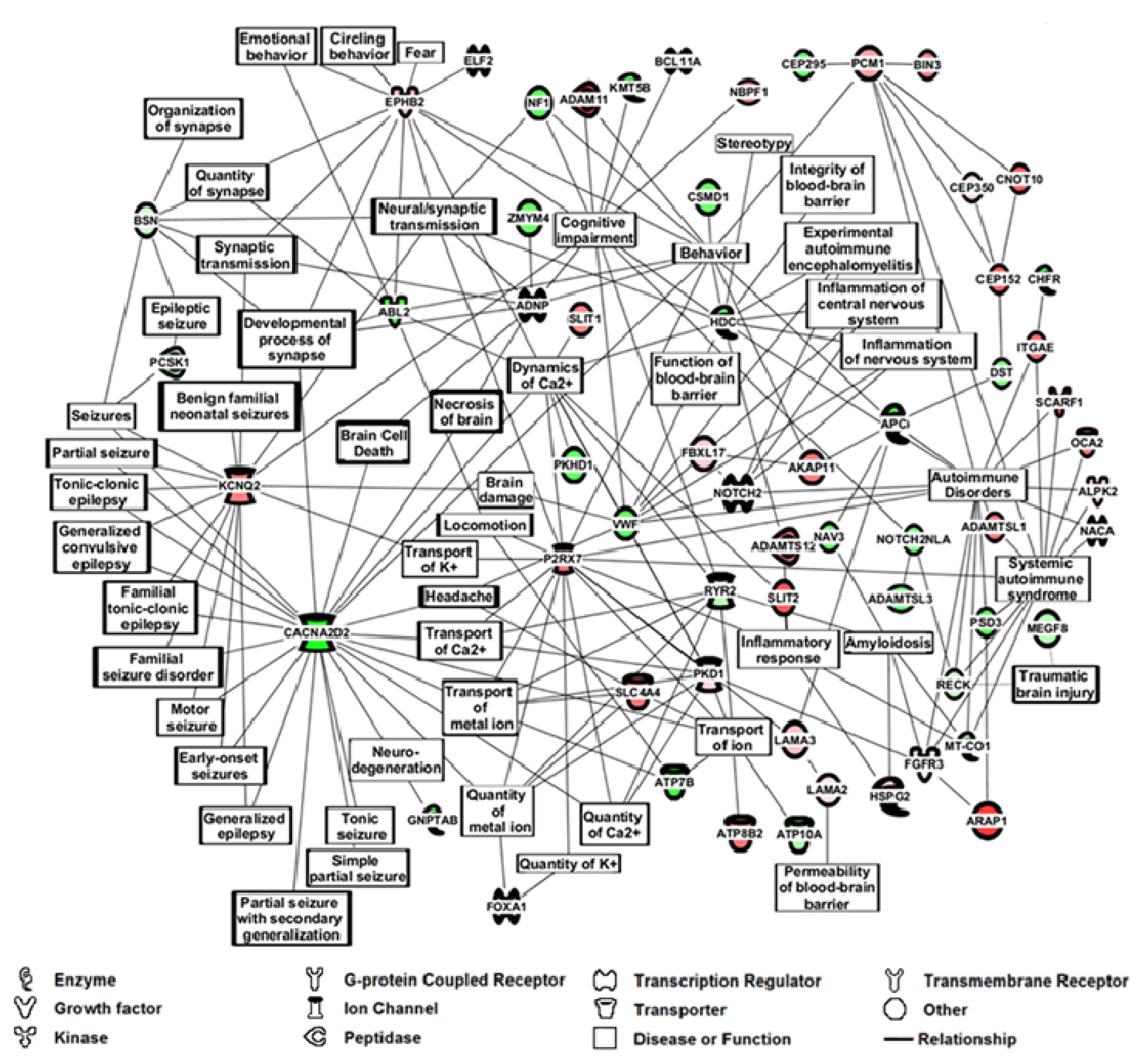
3.5. Phenotype Assessment of Epilepsy Patients versus Control Individuals Using TANDEM MS/MS of Serum Peptide/Proteins, and Bioinformatics Cell Pathway/Disease Mechanism Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Duncan, J.S.; Sander, J.W.; Sisodiya, S.M.; Walker, M.C. Adult epilepsy. Lancet 2006, 367, 1087–1100. [Google Scholar] [CrossRef]
- Vezzani, A.; French, J.; Bartfai, T.; Baram, T.Z. The role of inflammation in epilepsy. Nat. Rev. Neurol. 2011, 7, 31–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kilany, A.; Raouf, E.R.; Gaber, A.A.; Aloush, T.K.; Aref, H.A.; Anwar, M.; Henshall, D.C.; Abdulghani, M.O. Elevated serum Bcl-2 in children with temporal lobe epilepsy. Seizure 2012, 21, 250–253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, B.S.; Lowenstein, D.H. Epilepsy. N. Engl. J. Med. 2003, 349, 1257–1266. [Google Scholar] [CrossRef] [PubMed]
- Fisher, R.S.; Acevedo, C.; Arzimanoglou, A.; Bogacz, A.; Cross, J.H.; Elger, C.E.; Engel, J.; Forsgren, L.; French, J.A.; Glynn, M.; et al. ILAE Official Report: A practical clinical definition of epilepsy. Epilepsia 2014, 55, 475–482. [Google Scholar] [CrossRef] [Green Version]
- Scheffer, I.E.; Berkovic, S.; Capovilla, G.; Connolly, M.B.; French, J.; Guilhoto, L.; Hirsch, E.; Jain, S.; Mathern, G.W.; Moshe, S.L.; et al. ILAE classification of the epilepsies: Position paper of the ILAE Commission for Classification and Terminology. Epilepsia 2017, 58, 512–521. [Google Scholar] [CrossRef] [Green Version]
- Pitkanen, A.; Ekolle Ndode-Ekane, X.; Lapinlampi, N.; Puhakka, N. Epilepsy biomarkers–Toward etiology and pathology specificity. Neurobiol. Dis. 2019, 123, 42–58. [Google Scholar] [CrossRef]
- Hanas, J.S.; Hocker, J.R.; Ramajayam, G.; Prabhakaran, V.; Rajshekhar, V.; Oommen, A.; Manoj, J.J.; Anderson, M.P.; Drevets, D.A.; Carabin, H. Distinguishing neurocysticercosis epilepsy from epilepsy of unknown etiology using a minimal serum mass profiling platform. Exp. Parasitol. 2018, 192, 98–107. [Google Scholar] [CrossRef]
- Steinlein, O.K. Genetics and epilepsy. Dialogues Clin. Neurosci. 2008, 10, 29–38. [Google Scholar]
- Lukasiuk, K.; Becker, A.J. Molecular biomarkers of epileptogenesis. Neurotherapeutics 2014, 11, 319–323. [Google Scholar] [CrossRef] [Green Version]
- Sueri, C.; Gasparini, S.; Balestrini, S.; Labate, A.; Gambardella, A.; Russo, E.; Leo, A.; Casarotto, S.; Pittau, F.; Trimboli, M.; et al. Diagnostic Biomarkers of Epilepsy. Curr. Pharm. Biotechnol. 2018, 19, 440–450. [Google Scholar] [CrossRef]
- Willert, C.; Spitzer, C.; Kusserow, S.; Runge, U. Serum neuron-specific enolase, prolactin, and creatine kinase after epileptic and psychogenic non-epileptic seizures. Acta Neurol. Scand. 2004, 109, 318–323. [Google Scholar] [CrossRef] [PubMed]
- Hocker, J.R.; Deb, S.J.; Li, M.; Lerner, M.R.; Lightfoot, S.A.; Quillet, A.A.; Hanas, R.J.; Reinersman, M.; Thompson, J.L.; Vu, N.T.; et al. Serum Monitoring and Phenotype Identification of Stage I Non-Small Cell Lung Cancer Patients. Cancer Invest. 2017, 35, 573–585. [Google Scholar] [CrossRef] [PubMed]
- Hanas, J.S.; Hocker, J.R.S.; Lerner, M.R.; Couch, J.R. Distinguishing and phenotype monitoring of traumatic brain injury and post-concussion syndrome including chronic migraine in serum of Iraq and Afghanistan war veterans. PLoS ONE 2019, 14, e0215762. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hocker, J.R.; Postier, R.G.; Li, M.; Lerner, M.R.; Lightfoot, S.A.; Peyton, M.D.; Deb, S.J.; Baker, C.M.; Williams, T.L.; Hanas, R.J.; et al. Discriminating patients with early-stage pancreatic cancer or chronic pancreatitis using serum electrospray mass profiling. Cancer Lett. 2015, 359, 314–324. [Google Scholar] [CrossRef] [Green Version]
- Vachani, A.; Pass, H.I.; Rom, W.N.; Midthun, D.E.; Edell, E.S.; Laviolette, M.; Li, X.J.; Fong, P.Y.; Hunsucker, S.W.; Hayward, C.; et al. Validation of a multiprotein plasma classifier to identify benign lung nodules. J. Thorac. Oncol. 2015, 10, 629–637. [Google Scholar] [CrossRef] [Green Version]
- Villanueva, J.; Shaffer, D.R.; Philip, J.; Chaparro, C.A.; Erdjument-Bromage, H.; Olshen, A.B.; Fleisher, M.; Lilja, H.; Brogi, E.; Boyd, J.; et al. Differential exoprotease activities confer tumor-specific serum peptidome patterns. J. Clin. Invest. 2006, 116, 271–284. [Google Scholar] [CrossRef]
- Bianchi, M.E. DAMPs, PAMPs and alarmins: All we need to know about danger. J. Leukoc. Biol. 2007, 81, 1–5. [Google Scholar] [CrossRef]
- Wie Borsheim, A.; Engeland, A.; Gilhus, N.E. Epilepsy and autoimmune diseases: Comorbidity in a national patient cohort. Seizure 2020, 75, 89–95. [Google Scholar] [CrossRef] [Green Version]
- Tuck, M.K.; Chan, D.W.; Chia, D.; Godwin, A.K.; Grizzle, W.E.; Krueger, K.E.; Rom, W.; Sanda, M.; Sorbara, L.; Stass, S.; et al. Standard operating procedures for serum and plasma collection: Early detection research network consensus statement standard operating procedure integration working group. J. Proteome Res. 2009, 8, 113–117. [Google Scholar] [CrossRef] [Green Version]
- Garcia, H.H.; del Brutto, O.H. Cysticercosis Working Group in Peru Neurocysticercosis: Updated concepts about an old disease. Lancet Neurol. 2005, 4, 653–661. [Google Scholar] [CrossRef]
- Prabhakaran, V.; Rajshekhar, V.; Murrell, K.D.; Oommen, A. Conformation-sensitive immunoassays improve the serodiagnosis of solitary cysticercus granuloma in Indian patients. Trans. R. Soc. Trop. Med. Hyg. 2007, 101, 570–577. [Google Scholar] [CrossRef] [PubMed]
- Kramer, A.; Green, J.; Pollard, J., Jr.; Tugendreich, S. Causal analysis approaches in Ingenuity Pathway Analysis. Bioinformatics 2014, 30, 523–530. [Google Scholar] [CrossRef] [PubMed]
- Guan, W.; Zhou, M.; Hampton, C.Y.; Benigno, B.B.; Walker, L.D.; Gray, A.; McDonald, J.F.; Fernández, F.M. Ovarian cancer detection from metabolomic liquid chromatography/mass spectrometry data by support vector machines. BMC Bioinform. 2009, 10, 259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ransohoff, D.F. Rules of evidence for cancer molecular-marker discovery and validation. Nat. Rev. Cancer 2004, 4, 309–314. [Google Scholar] [CrossRef] [PubMed]
- Baker, S.G.; Kramer, B.S.; Srivastava, S. Markers for early detection of cancer: Statistical guidelines for nested case-control studies. BMC Med. Res. Methodol. 2002, 2, 4. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J.R.; Johnson, H.; Eaton, S.; Sterman, H.; Wise, L. Surgical procedures in patients during the tenth decade of life. Surgery 1988, 104, 646–651. [Google Scholar]
- Soper, D.S. Post-hoc Statistical Power Calculator for a Student t-Test [Software]. Available online: http://www.danielsoper.com/statcalc (accessed on 12 June 2020).
- Fang, M.; Liu, G.W.; Pan, Y.M.; Shen, L.; Li, C.S.; Xi, Z.Q.; Xiao, F.; Wang, L.; Chen, D.; Wang, X.F. Abnormal expression and spatiotemporal change of Slit2 in neurons and astrocytes in temporal lobe epileptic foci: A study of epileptic patients and experimental animals. Brain Res. 2010, 1324, 14–23. [Google Scholar] [CrossRef]
- Conroy, J.; McGettigan, P.A.; McCreary, D.; Shah, N.; Collins, K.; Parry-Fielder, B.; Moran, M.; Hanrahan, D.; Deonna, T.W.; Korff, C.M.; et al. Towards the identification of a genetic basis for Landau-Kleffner syndrome. Epilepsia 2014, 55, 858–865. [Google Scholar] [CrossRef]
- Camacho, A.; Nunez, N.; Dekomien, G.; Hernandez-Lain, A.; de Aragon, A.M.; Simon, R. LAMA2-related congenital muscular dystrophy complicated by West syndrome. Eur. J. Paediatr. Neurol. 2015, 19, 243–247. [Google Scholar] [CrossRef]
- Hsia, H.E.; Tushaus, J.; Brummer, T.; Zheng, Y.; Scilabra, S.D.; Lichtenthaler, S.F. Functions of ‘A disintegrin and metalloproteases (ADAMs)’ in the mammalian nervous system. Cell. Mol. Life Sci. 2019, 76, 3055–3081. [Google Scholar] [CrossRef] [PubMed]
- Engel, T.; Jimenez-Pacheco, A.; Miras-Portugal, M.T.; Diaz-Hernandez, M.; Henshall, D.C. P2X7 receptor in epilepsy; role in pathophysiology and potential targeting for seizure control. Int. J. Physiol. Pathophysiol. Pharm. 2012, 4, 174–187. [Google Scholar]
- Khakipoor, S.; Ophoven, C.; Schrodl-Haussel, M.; Feuerstein, M.; Heimrich, B.; Deitmer, J.W.; Roussa, E. TGF-beta signaling directly regulates transcription and functional expression of the electrogenic sodium bicarbonate cotransporter 1, NBCe1 (SLC4A4), via Smad4 in mouse astrocytes. Glia 2017, 65, 1361–1375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pechmann, A.; Wellmann, S.; Stoecklin, B.; Kruger, M.; Zieger, B. Increased von Willebrand factor parameters in children with febrile seizures. PLoS ONE 2019, 14, e0210004. [Google Scholar] [CrossRef] [Green Version]
- Lehnart, S.E.; Mongillo, M.; Bellinger, A.; Lindegger, N.; Chen, B.X.; Hsueh, W.; Reiken, S.; Wronska, A.; Drew, L.J.; Ward, C.W.; et al. Leaky Ca2+ release channel/ryanodine receptor 2 causes seizures and sudden cardiac death in mice. J. Clin. Invest. 2008, 118, 2230–2245. [Google Scholar] [CrossRef] [Green Version]
- Du, Y.; Chi, X.; An, W. Downregulation of microRNA-200c-3p reduces damage of hippocampal neurons in epileptic rats by upregulating expression of RECK and inactivating the AKT signaling pathway. Chem. Biol. Interact. 2019, 307, 223–233. [Google Scholar] [CrossRef]
- Freitas, M.E.; Ruiz-Lopez, M.; Dalmau, J.; Erro, R.; Privitera, M.; Andrade, D.; Fasano, A. Seizures and movement disorders: Phenomenology, diagnostic challenges and therapeutic approaches. J. Neurol. Neurosurg. Psychiatry 2019, 90, 920–928. [Google Scholar] [CrossRef] [Green Version]
- Ren, M.; Li, K.; Wang, D.; Guo, J.; Li, J.; Yang, G.; Long, X.; Shen, W.; Hu, R.; Wang, X.; et al. Neurofibromin Regulates Seizure Attacks in the Rat Pilocarpine-Induced Model of Epilepsy. Mol. Neurobiol. 2016, 53, 6069–6077. [Google Scholar] [CrossRef]
- Bhowmik, M.; Khanam, R.; Vohora, D. Histamine H3 receptor antagonists in relation to epilepsy and neurodegeneration: A systemic consideration of recent progress and perspectives. Br. J. Pharm. 2012, 167, 1398–1414. [Google Scholar] [CrossRef] [Green Version]
- Punetha, J.; Karaca, E.; Gezdirici, A.; Lamont, R.E.; Pehlivan, D.; Marafi, D.; Appendino, J.P.; Hunter, J.V.; Akdemir, Z.C.; Fatih, J.M.; et al. Biallelic CACNA2D2 variants in epileptic encephalopathy and cerebellar atrophy. Ann. Clin. Transl. Neurol. 2019, 6, 1395–1406. [Google Scholar] [CrossRef] [Green Version]
- Lo-Castro, A.; Curatolo, P. Epilepsy associated with autism and attention deficit hyperactivity disorder: Is there a genetic link? Brain Dev. 2014, 36, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Bai, J.; Yang, Y.; Wang, J.; Zhang, L.; Wang, F.; He, A. Variability of serum novel serum peptide biomarkers correlates with the disease states of multiple myeloma. Clin. Proteom. 2019, 16, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barclay, J.; Balaguero, N.; Mione, M.; Ackerman, S.L.; Letts, V.A.; Brodbeck, J.; Canti, C.; Meir, A.; Page, K.M.; Kusumi, K.; et al. Ducky mouse phenotype of epilepsy and ataxia is associated with mutations in the Cacna2d2 gene and decreased calcium channel current in cerebellar Purkinje cells. J. Neurosci. 2001, 21, 6095–6104. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Category | Epilepsy a | Control |
|---|---|---|---|
| Sample Size | 29 | 17 | |
| Gender | Male | 19 (66%) | 7 (41%) |
| Age | Mean (SD) | 26.9 (7.2) | 34.0 (9.2) |
| Education | <Secondary | 11 (38%) | 5 (29%) |
| ≥Secondary | 18 (62%) | 12 (71%) | |
| Consumed Pork | Yes | 2 (7%) | 1 (6%) |
| Living near a house that raised pigs b,c | Yes | 4 (14%) | 0 (0%) |
| Own pigs | Yes | 0 (0%) | 0 (0%) |
| Utilize toilet to defecate? c | Never | 22 (76%) | 16 (94%) |
| Cigarette smoking b | Yes | 4 (14%) | 0 (0%) |
| Paan use b | Yes | 3 (10%) | 0 (0%) |
| Headaches | Yes | 0 (0%) | 16 (94%) |
| Time since last seizure | ≤3 months | 21 (72%) | NA |
| 3–7 months | 8 (28%) | NA | |
| No of lifetime seizures a | 1 | 0 (0%) | NA |
| 2–5 | 9 (31%) | NA | |
| 6–10 | 2 (7%) | NA | |
| >10 | 18 (62%) | NA | |
| Type of last seizure | Generalized | 24 (83%) | NA |
| Partial | 1 (3%) | NA | |
| Partial then generalized | 4 (14%) | NA | |
| Panel I | % LOOCV Mean (SD) Group 1 | % LOOCV Mean (SD) Group 2 | True Positive Group 1 | False Positive Group 2 | True Negative Group 2 | False Negative Group 1 | N | Figure # | |||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Group 1 vs. Group 2 | |||||||||||
| Ion-Trap MS LOOCV Data Sets: | |||||||||||
| Epilepsy vs. Control | 55.09% | 31.81% | 29/29 | 0/17 | 17/17 | 0/29 | Epilepsy = 29; Control = 17 | Figure 1C | |||
| (4.84%) | (3.58%) | (100%) | (0%) | (100%) | (0%) | ||||||
| Training: Epilepsy vs. Control | 56.98% | 28.60% | 23/23 | 0/13 | 23/23 | 0/23 | Epilepsy = 6; Control = 4 | Figure 2B | |||
| (4.28%) | (−4.42%) | (−100%) | (0%) | (100%) | (0%) | ||||||
| Blind: Epilepsy vs. Control | 47.58% | 29.69% | 13/13 | 0/16 | 16/16 | 0/13 | Epilepsy = 23; Control = 13 | Figure 2A | |||
| (3.6%) | (1.18%) | (100%) | (0%) | (100%) | (0%) | ||||||
| TBI vs. Epilepsy | 69.73% | 29.69% | 13/13 | 0/16 | 16/16 | 0/13 | TBI = 13; Epilepsy = 16 | Figure 3B | |||
| (4.48%) | (5.87%) | (100%) | (0%) | (100%) | (0%) | ||||||
| Single Quadrupole MS LOOCV Set: | |||||||||||
| Epilepsy vs. Control | 47.98% (10.48%) | 24.10% (9.05%) | 27/29 (93.1%) | 2/17 (12%) | 15/17 (88.2%) | 2/29 (6.9%) | Epilepsy, N = 29; Control, N = 17 | Figure 2C | |||
| Panel II | Sens-itivity | Efficiency/ [accuracy] | True Positive Rate | False Positive Rate | Spec-ificity | P- value | Random Database P-value | Coh-en’sd | ROC AUC | Figure# | |
| group 1 vs. group 2 | |||||||||||
| Ion-Trap MS LOOCV Data Sets | |||||||||||
| Epilepsy, N = 29 vs. Control, N = 17 | 1 | 1 | 1 | 0 | 0.97 | 4.56 × 10−22 | 0.108 | 5.46 | 1 | Figure 1C,D | |
| Training: Epilepsy, N = 23 vs. Control, N = 13 | 1 | 1 | 1 | 0 | 1 | 3.02 × 10−16 | 0.054 | 6.52 | 1 | Figure 2A | |
| Blind: Epilepsy, N = 6 vs. Control N = 4 | 1 | 0.9 | 1 | 0.25 | 0.75 | 5.62 × 10−3 | na | 2.07 | 1 | Figure 2B | |
| TBI, N = 13 vs. Epilepsy, N = 16 | 1 | 1 | 1 | 0 | 1 | 2.00 × 10−15 | 0.0012 | 7.66 | 1 | Figure 3B, | |
| Single Quadrupole MS LOOCV Set: | |||||||||||
| Epilepsy, N = 29 vs. Control, N = 17 | 0.9 | 0.87 | 0.9 | 0.018 | 0.82 | 3.95 × 10−10 | 0.37 | 2.43 | 0.953 | Figure 2C,D | |
| Symbol | Epilepsy: Control | Symbol | Epilepsy: Control | Symbol | Epilepsy: Control |
|---|---|---|---|---|---|
| [#Sera (#Hits)] | [#Sera (#Hits)] | [#Sera (#Hits)] | |||
| FBN3 | 6(62): 0(0) | PEAR1 1,2 | 4(44): 1(3) | ITGAE 1,2,3 | 3(32): 0(0) |
| MUC17 4 | 6(83): 3(15) | ALPK2 1 | 4(38): 1(10) | ATP8B2 | 3(30): 0(0) |
| SLIT2 1,3 | 5(65): 0(0) | PKD1 1,4 | 4(27): 1(9) | ZNF562 | 3(30): 0(0) |
| PCM1 1,4 | 5(72): 1(6) | DACT2 1 | 4(22): 1(9) | ADAMTSL1 2 | 3(28): 0(0) |
| OTOGL | 5(39): 2(10) | FBXL17 | 4(13): 1(3) | SLC4A4 1,3,4,5 | 3(28): 0(0) |
| ARAP1 1,2 | 4(137): 0(0) | HSPG2 1,2,4,5 | 4(83): 2(23) | ADAMTS12 1,2 | 3(26): 0(0) |
| USP19 1 | 4(135): 0(0) | LAMA2 1,2,3,5 | 4(67): 2(30) | CNST 1 | 3(25): 0(0) |
| CTCFL | 4(126): 0(0) | CEP350 1,2 | 4(33): 2(12) | KLHL4 | 3(25): 0(0) |
| SCARF1 2 | 4(86): 0(0) | NACA 1 | 4(14): 2(9) | KCNQ2 1,3,4,5 | 3(24): 0(0) |
| FAT4 1,3 | 4(83): 0(0) | LCE1A 2 | 3(178): 0(0) | NBPF10 | 3(24): 0(0) |
| CNOT10 | 4(52): 0(0) | ADAM11 1,2,3,4,5 | 3(87): 0(0) | BIN3 1,2,3 | 3(23): 0(0) |
| CLINT1 1,2 | 4(46): 0(0) | VPS13D 1,2,3 | 3(66): 0(0) | AMBN 2 | 3(22): 0(0) |
| CEP152 | 4(43): 0(0) | ADAMTS18 1 | 3(50): 0(0) | BCL11A | 3(22): 0(0) |
| OCA2 1,3,4 | 4(32): 0(0) | ISM2 | 3(34): 0(0) | ABCA12 2 | 3(21): 0(0) |
| AKAP11 1,4 | 4(29): 0(0) | P2RX7 1,2,3,4,5 | 3(34): 0(0) | ZNRF3 1 | 3(21): 0(0) |
| LAMA3 2 | 4(102): 1(21) | POTED | 3(33): 0(0) | SLIT1 1 | 3(20): 0(0) |
| EPHB2 1,2,3,4 | 4(62): 1(12) | PCNX2 1,3 | 3(33): 0(0) |
| Symbol | Control: Epilepsy | Symbol | Control: Epilepsy | Symbol | Control: Epilepsy |
|---|---|---|---|---|---|
| [#Sera (#Hits)] | [#Sera (#Hits)] | [#Sera (#Hits)] | |||
| NOTCH2 1,2,4 | 8(32): 1(3) | RYR2 1,2,3,4 | 4(47): 1(7) | FAT1 1,2 | 3(51): 0(0) |
| NOTCH2NL 1 | 7(49): 1(2) | TNXA 1 | 4(41): 1(23) | NF1 1,2,3,4 | 3(44): 0(0) |
| ZFP1 | 7(190): 3(21) | RECK 1,2,3,5 | 4(34): 1(7) | PSD3 1,4 | 3(44): 0(0) |
| PKHD1 2 | 5(41): 0(0) | ELF2 1 | 4(28): 1(3) | USP28 1,2 | 3(42): 0(0) |
| DST 1,2 | 5(192): 1(9) | THSD7A 1 | 4(20): 1(3) | KMT5B 1,2,3 | 3(38): 0(0) |
| VWF 1,2,3,4,5 | 5(182): 1(3) | C16orf96 | 4(12): 1(3) | CEP295 | 3(35): 0(0) |
| MEGF8 | 5(52): 1(9) | MEGF11 1 | 4(56): 2(21) | ZMYM4 1 | 3(35): 0(0) |
| ATP10A 1,3,4 | 5(40): 1(4) | ASS1 1,2,3 | 4(40): 2(21) | LAMB4 2 | 3(34): 0(0) |
| BS 1,2,3,4 | 5(20): 1(5) | FGFR3 1,3 | 4(37): 2(25) | HDC 1,2,3,4,5 | 3(31): 0(0) |
| CACNA2D2 1,3,4 | 4(222): 0(0) | KIF9 2 | 3(150): 0(0) | FOXA1 1,2,4 | 3(29): 0(0) |
| APC 1,2,3 | 4(57): 0(0) | NRAP | 3(120): 0(0) | ADAMTSL3 1,2 | 3(28): 0(0) |
| ZNF300 1,2 | 4(36): 0(0) | ATP7B 1,2,3,4,5 | 3(98): 0(0) | NAV3 1 | 3(28): 0(0) |
| CSMD1 1,2,3 | 4(32): 0(0) | ABL2 1,2,3 | 3(67): 0(0) | GNPTAB 1,2 | 3(27): 0(0) |
| PCSK1 1 | 4(90): 1(11) | ADGRG4 | 3(67): 0(0) | ASTN2 1,3,4 | 3(25): 0(0) |
| MT-CO1 1,3 | 4(86): 1(15) | RAPGEF6 1 | 3(58): 0(0) | ADNP 1,2,3,4 | 3(23): 0(0) |
| RNF213 1,2,3 | 4(78): 1(15) | MAGED4 1 | 3(52): 0(0) | DMAC1 | 3(23): 0(0) |
| CRIM1 1 | 4(76): 1(9) | CHFR 1,2 | 3(51): 0(0) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hanas, J.S.; Hocker, J.R.S.; Vannarath, C.; Evangeline, B.; Prabhakaran, V.; Oommen, A.; Couch, J.; Anderson, M.; Rajshekhar, V.; Carabin, H.; et al. Distinguishing and Biochemical Phenotype Analysis of Epilepsy Patients Using a Novel Serum Profiling Platform. Brain Sci. 2020, 10, 504. https://doi.org/10.3390/brainsci10080504
Hanas JS, Hocker JRS, Vannarath C, Evangeline B, Prabhakaran V, Oommen A, Couch J, Anderson M, Rajshekhar V, Carabin H, et al. Distinguishing and Biochemical Phenotype Analysis of Epilepsy Patients Using a Novel Serum Profiling Platform. Brain Sciences. 2020; 10(8):504. https://doi.org/10.3390/brainsci10080504
Chicago/Turabian StyleHanas, Jay S., James R. S. Hocker, Christian Vannarath, Betcy Evangeline, Vasudevan Prabhakaran, Anna Oommen, James Couch, Michael Anderson, Vedantam Rajshekhar, Hélène Carabin, and et al. 2020. "Distinguishing and Biochemical Phenotype Analysis of Epilepsy Patients Using a Novel Serum Profiling Platform" Brain Sciences 10, no. 8: 504. https://doi.org/10.3390/brainsci10080504
APA StyleHanas, J. S., Hocker, J. R. S., Vannarath, C., Evangeline, B., Prabhakaran, V., Oommen, A., Couch, J., Anderson, M., Rajshekhar, V., Carabin, H., & Drevets, D. (2020). Distinguishing and Biochemical Phenotype Analysis of Epilepsy Patients Using a Novel Serum Profiling Platform. Brain Sciences, 10(8), 504. https://doi.org/10.3390/brainsci10080504