A Within-Sample Comparison of Two Innovative Neuropsychological Tests for Assessing ADHD

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.3. Neuropsychology
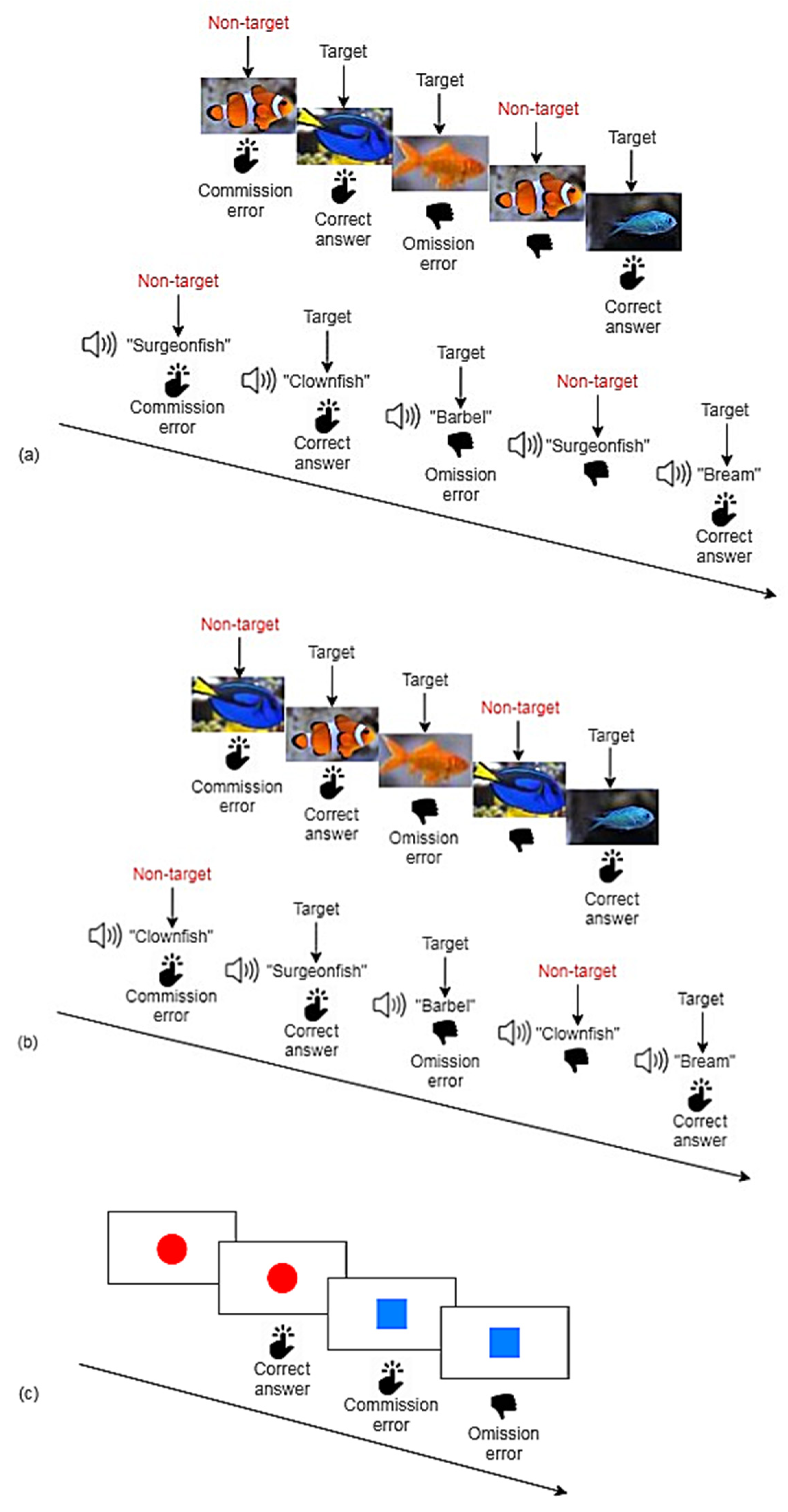
2.3.1. Nesplora Aquarium
2.3.2. Quantified Behavior Test
2.3.3. Diagnostic Interview for ADHD in adults (DIVA)
2.3.4. Wender–Reimherr Interview (WRI)
2.3.5. Wender–Utah Rating Scale (WURS-k)
2.3.6. UPPS Impulsive Behavior Scale (UPPS)
2.3.7. General Health Questionnaire-28 (GHQ-28)
2.4. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

Appendix B

{kind=link}
{kind=link}
| Variables | Description |
|---|---|
| Nesplora Aquarium | |
| Perseverative errors (n) | Deficit in cognitive flexibility: Measured by the errors occurring when falsely continuing to respond to the previous instructions of the last task instead of following the instructions of the next task |
| Switching reaction time (mean) (ms) | Suffering of reaction speed while adapting to a new task: Measured by the difference between the reaction time of correct answers in the last part of a task with the reaction time of correct answers in the beginning of the following task |
| Switching correct answers (n) | Suffering of task execution while adapting to a new task: Measured by the difference between the number of correct answers in the last part of a task with the number of correct answers in the beginning of the following task |
| Total commission errors (n) | Indicator of Impulsivity: Measured by errors occured when participant falsely reacts to non-target stimulus |
| Total omission errors (n) | Indicator of Inattention: Measured by errors occured when participant fails to react to target stimulus |
| Commission errors reaction time (mean) (ms) | Additional information on cause of commission errors: Measured by time passed until the button is falsely pressed on a non-target stimulus Higher scores represented by low reaction time are considered to indicate higher impulsivity and/or hyperactivity |
| Commission errors reaction time (SD) (ms) | Indicator of variability of reaction time in commission errors: Measured by standard deviation of reaction time |
| Correct answers reaction time (mean) (ms) | Indicator of processing speed: Measured by the time passed since the target stimulus is presented until the button is pressed |
| Correct answers reaction time (SD) (ms) | Indicator of sustained attention/fatigability: Measured by standard deviation of reaction time |
| Discrepancy of correct answers (n) | Additional measure of consistency/fatigability: Measured by the difference of correct answers in the first half of a task and the correct answers in the second half of a task |
| Dual task correct answers (n) | Indicator of Working Memory: Measured by the correct answers in visual and auditory target stimuli by parallel processing of sensory modalities Inverse interpretation: high scores indicate a good working memory performance |
| Sum of distance (mean) | Indicator of Movement: Measured by the sum of movement in pitch, roll and yaw shaft |
| Movement in the pitch shaft (mean) | Indicator of Movement in the pitch shaft |
| Movement in the roll shaft (mean) | Indicator of Movement in the roll shaft |
| Movement in the yaw shaft (mean) | Indicator of Movement in the yaw shaft |
| Qb-Test | |
| Time active | Indicator of Movement: Measured whenever participant moves more than 1 cm/s |
| Distance | Indicator of Movement: Measured by the reflective marker on the headband (in metres) |
| Area | Indicator of Movement: Measured in square centimetres to indicate the spatial distribution of movement |
| Micro events | Indicator of Movement: Measured whenever participant moves more than 1 mm |
| Motion simplicity | Indicator of Complexity of movements: High scores represent small movements, low scores reflect complex movements |
| Omission errors | See above |
| Correct answers reaction time (mean) | See above |
| Correct answers reaction time (SD) | See above |
| Commission errors | See above |
| Normalized commission errors | Correction of commission error rate based on individual inattention levels Measured by the ratio of commission errors to correct responses |
References
- Spencer, T.J.; Biederman, J.; Mick, E. Attention-Deficit/Hyperactivity Disorder: Diagnosis, Lifespan, Comorbidities, and Neurobiology. Ambul. Pediatr. 2007, 7, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Sibley, M.H.; Mitchell, J.T.; Becker, S.P. Method of adult diagnosis influences estimated persistence of childhood ADHD: A systematic review of longitudinal studies. Lancet Psychiatry 2016, 3, 1157–1165. [Google Scholar] [CrossRef]
- Polanczyk, G.V.; Willcutt, E.G.; Salum, G.A.; Kieling, C.; Rohde, L.A. ADHD Prevalence Estimates across Three Decades: An Updated Systematic Review and Meta-Regression Analysis. Int. J. Epidemiol. 2014, 43, 434–442. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- Ohlmeier, M.D.; Peters, K.; Kordon, A.; Seifert, J.; Wildt, B.T.; Wiese, B.; Ziegenbein, M.; Emrich, H.M.; Schneider, U. Nicotine and Alcohol Dependence in Patients With Comorbid attention-deficit/hyperactivity Disorder (ADHD). Alcohol Alcohol 2007, 42, 539–543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kessler, R.C.; Adler, L.; Berkley, R.; Biederman, J.; Conners, C.K.; Demler, O.; Faraone, S.V.; Greenhill, L.L.; Howes, M.J.; Secnik, K.; et al. The prevalence and correlates of adult ADHD in the United States: Results from the National Comorbidity Survey Replication. Am. J. Psychiatry 2006, 163, 716–723. [Google Scholar] [CrossRef] [PubMed]
- Biederman, J.; Ball, S.W.; Monuteaux, M.C.; Mick, E.; Spencer, T.J.; McCreary, M.; Cote, M.; Faraone, S.V. New insights into the comorbidity between ADHD and major depression in adolescent and young adult females. J. Am. Acad. Child Adolesc. Psychiatry 2008, 47, 426–434. [Google Scholar] [CrossRef] [PubMed]
- Chang, Z.; Lichtenstein, P.; D’Onofrio, B.M.; Sjölander, A.; Larsson, H. Serious transport accidents in adults with attention-deficit/hyperactivity disorder and the effect of medication a population-based study. JAMA Psychiatry 2014, 71, 319–325. [Google Scholar] [CrossRef]
- Cortese, S.; Tessari, L. Attention-Deficit/Hyperactivity Disorder (ADHD) and Obesity: Update 2016. Curr. Psychiatry Rep. 2017, 19, 4. [Google Scholar] [CrossRef] [Green Version]
- Biederman, J.; Faraone, S.V.; Spencer, T.J.; Mick, E.; Monuteaux, M.C.; Aleardi, M. Functional impairments in adults with self-reports of diagnosed ADHD: A controlled study of 1001 adults in the community. J. Clin. Psychiatry 2006, 67, 524–540. [Google Scholar] [CrossRef]
- Biederman, J.; Faraone, S.V. The Effects of attention-deficit/hyperactivity Disorder on Employment and Household Income. Medscape Gen. Med. 2006, 8, 12. [Google Scholar]
- Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften (AWMF). Langfassung der Interdisziplinären Evidenz- und Konsensbasierten (S3) Leitlinie “Aufmerksamkeitsdefizit-/Hyperaktivitätsstörung (ADHS) im Kindes-, Jugend- und Erwachsenenalter”. 2017. Available online: https://www.awmf.org/leitlinien/detail/ll/028-045.html (accessed on 7 October 2020).
- NICE (National Institute for Health and Care Excellence). NICE guideline [NG87] Attention Deficit h Hyper Yperactivity Activity Disorder: Diagnosis and Management. 2018. Available online: https://www.nice.org.uk/guidance/ng87 (accessed on 7 October 2020).
- Areces, D.; García, T.; Cueli, M.; Rodríguez, C. Is a virtual reality test able to predict current and retrospective ADHD symptoms in adulthood and adolescence? Brain Sci. 2019, 9, 274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Areces, D.; Rodríguez, C.; García, T.; Cueli, M.; González-Castro, P. Efficacy of a Continuous Performance Test Based on Virtual Reality in the Diagnosis of ADHD and Its Clinical Presentations. J. Atten. Disord. 2018, 22, 1081–1091. [Google Scholar] [CrossRef] [PubMed]
- Parsons, T.D.; Duffield, T.; Asbee, J. A Comparison of Virtual Reality Classroom Continuous Performance Tests to Traditional Continuous Performance Tests in Delineating ADHD: A Meta-Analysis. Neuropsychol. Rev. 2019, 29, 338–356. [Google Scholar] [CrossRef] [PubMed]
- Hult, N.; Kadesjö, J.; Kadesjö, B.; Gillberg, C.; Billstedt, E. ADHD and the QbTest: Diagnostic Validity of QbTest. J. Atten. Disord. 2018, 22, 1074–1080. [Google Scholar] [CrossRef]
- Walker, A.J.; Shores, E.A.; Trollor, J.N.; Lee, T.; Sachdev, P.S. Neuropsychological functioning of adults with attention deficit hyperactivity disorder. J. Clin. Exp. Neuropsychol. 2000, 22, 115–124. [Google Scholar] [CrossRef]
- Brunkhorst-Kanaan, N.; Verdenhalven, M.; Kittel-Schneider, S.; Vainieri, I.; Reif, A.; Grimm, O. The Quantified Behavioral Test—A Confirmatory Test in the Diagnostic Process of Adult ADHD? Front. Psychiatry 2020, 11, 216. [Google Scholar] [CrossRef] [Green Version]
- Baggio, S.; Hasler, R.; Giacomini, V.; El-Masri, H.; Weibel, S.; Perroud, N.; Deiber, M.P. Does the Continuous Performance Test Predict ADHD Symptoms Severity and ADHD Presentation in Adults? J. Atten. Disord. 2020, 24, 840–848. [Google Scholar] [CrossRef]
- Nikolas, M.A.; Marshall, P.; Hoelzle, J.B. The role of neurocognitive tests in the assessment of adult attention-deficit/hyperactivity disorder. Psychol. Assess. 2019, 31, 685–698. [Google Scholar] [CrossRef] [Green Version]
- Insel, T.R. The nimh research domain criteria (rdoc) project: Precision medicine for psychiatry. Am. J. Psychiatry 2014, 171, 395–397. [Google Scholar] [CrossRef] [Green Version]
- Willcutt, E.G.; Doyle, A.E.; Nigg, J.T.; Faraone, S.V.; Pennington, B.F. Validity of the executive function theory of attention-deficit/hyperactivity disorder: A meta-analytic review. Biol. Psychiatry 2005, 57, 1336–1346. [Google Scholar] [CrossRef]
- Sonuga-Barke, E.J.S. Causal models of attention-deficit/hyperactivity disorder: From common simple deficits to multiple developmental pathways. Biol. Psychiatry 2005, 57, 1231–1238. [Google Scholar] [CrossRef] [PubMed]
- Climent, G.; Rodríguez, C.; García, T.; Areces, D.; Mejías, M.; Aierbe, A.; Moreno, M.; Cueto, E.; Castellá, J.; Feli González, M. New virtual reality tool (Nesplora Aquarium) for assessing attention and working memory in adults: A normative study. Appl. Neuropsychol. 2019. [Google Scholar] [CrossRef] [PubMed]
- QbTech, A. QbTest plus Technical Manual; QbTech: Gotheborg, Sweden, 2010. [Google Scholar]
- Rodríguez, C.; Areces, D.; García, T.; Cueli, M.; González-Castro, P. Comparison between two continuous performance tests for identifying ADHD: Traditional vs. virtual reality. Int. J. Clin. Health Psychol. 2018, 18, 254–263. [Google Scholar] [CrossRef]
- Kooij, J.J.S. Adult ADHD: Diagnostic Assessment and Treatment, 3rd ed.; Springer: London, UK, 2012. [Google Scholar]
- Von Rösler, M.; Retz-Junginger, P.; Retz, W.; Stieglitz, R.-D. HASE, Homburger ADHS-Skalen für Erwachsene; Hogrefe: Göttingen, Germany, 2008. [Google Scholar]
- Ward, M.F.; Wender, P.H.; Reimherr, F.W. The Wender Utah rating scale: An aid in the retrospective diagnosis of childhood attention deficit hyperactivity disorder. Am. J. Psychiatry 1993, 150, 885–890. [Google Scholar] [PubMed]
- Whiteside, S.P.; Lynam, D.R. The five factor model and impulsivity: Using a structural model of personality to understand impulsivity. Pers. Individ. Dif. 2001, 30, 669–689. [Google Scholar] [CrossRef]
- Goldberg, D.P. Manual of the General Health Questionnaire; NFER-Nelson: Windsor, UK, 1978. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th ed.; American Psychiatric Association: Washington, DC, USA, 2000. [Google Scholar]
- Wender, P.H. Attention-Deficit Hyperactivity Disorder in Adults; Oxford University Press: New York, NY, USA, 1995. [Google Scholar]
- Retz-Junginger, P.; Retz, W.; Blocher, D.; Stieglitz, R.D.; Georg, T.; Supprian, T.; Wender, P.H.; Rösler, M. Reliabilität und validität der Wender-Utah-Rating-Scale-Kurzform: Retrospektive erfassung von symptomen aus dem spektrum der aufmerksamkeitsdefizit/hyperaktivitätsstörung. Nervenarzt 2003, 74, 987–993. [Google Scholar] [CrossRef]
- Schmidt, R.E.; Gay, P.; D’Acremont, M.; Van Der Linden, M. A German adaptation of the upps impulsive behavior scale: Psychometric properties and factor structure. Swiss J. Psychol. 2008, 67, 107–112. [Google Scholar] [CrossRef] [Green Version]
- IBM Corp. IBM SPSS Statistics for Macintosh, Version 25.0; IBM Corp: Armonk, NY, USA, 2017. [Google Scholar]
- Sliz, E.; Shin, J.; Syme, C.; Black, S.; Seshadri, S.; Paus, T.; Pausova, Z. Thickness of the cerebral cortex shows positive association with blood levels of triacylglycerols carrying 18-carbon fatty acids. Commun. Biol. 2020, 3, 1–9. [Google Scholar] [CrossRef]
- Gao, X.; Starmer, J.; Martin, E.R. A multiple testing correction method for genetic association studies using correlated single nucleotide polymorphisms. Genet. Epidemiol. 2008, 32, 361–369. [Google Scholar] [CrossRef]
- Emser, T.S.; Johnston, B.A.; Steele, J.D.; Kooij, S.; Thorell, L.; Christiansen, H. Assessing ADHD symptoms in children and adults: Evaluating the role of objective measures. Behav. Brain Funct. 2018, 14, 11. [Google Scholar] [CrossRef] [Green Version]
- Reh, V.; Schmidt, M.; Lam, L.; Schimmelmann, B.G.; Hebebrand, J.; Rief, W.; Christiansen, H. Behavioral Assessment of Core ADHD Symptoms Using the QbTest. J. Atten. Disord. 2015, 19, 1034–1045. [Google Scholar] [CrossRef] [PubMed]
- Mitra, S.; Knight, A.; Munn, A. Divergent effects of cognitive load on quiet stance and task-linked postural coordination. J. Exp. Psychol. Hum. Percept. Perform. 2013, 39, 323. [Google Scholar] [CrossRef] [PubMed]
- Hirsch, O.; Christiansen, H. Factorial Structure and Validity of the Quantified Behavior Test Plus (Qb+©). Assessment 2017, 24, 1037–1049. [Google Scholar] [CrossRef] [PubMed]
- Caswell, A.J.; Bond, R.; Duka, T.; Morgan, M.J. Further evidence of the heterogeneous nature of impulsivity. Pers. Individ. Dif. 2015, 76, 68–74. [Google Scholar] [CrossRef] [Green Version]
- Linhartová, P.; Širůček, J.; Ejova, A.; Barteček, R.; Theiner, P.; Kašpárek, T. Dimensions of Impulsivity in Healthy People, Patients with Borderline Personality Disorder, and Patients with Attention-Deficit/Hyperactivity Disorder. J. Atten. Disord. 2019. [Google Scholar] [CrossRef]
- Stahl, C.; Voss, A.; Schmitz, F.; Nuszbaum, M.; Tüscher, O.; Lieb, K.; Klauer, K.C. Behavioral components of impulsivity. J. Exp. Psychol. Gen. 2014, 143, 850–886. [Google Scholar] [CrossRef]
- Kapur, S.; Phillips, A.G.; Insel, T.R. Why has it taken so long for biological psychiatry to develop clinical tests and what to do about it. Mol. Psychiatry 2012, 17, 1174–1179. [Google Scholar] [CrossRef] [Green Version]

| n Demographics | 29 |
| Age (M (years)) ± SD | 35.24 ± 11.05 |
| Sex | |
| Males | 10 (34.5%) |
| Females | 19 (65.5%) |
| Diagnosis | |
| ADHD | 23 (79.3%) |
| Non-ADHD | 6 (20.7%) |
| Comorbid disorders among ADHD patients | 17 (73.9%) |
| Depression | 13 (56.5%) |
| Substance abuse disorders | 3 (13.0%) |
| Personality disorders | 2 (8.7%) |
| Delusional disorders | 1 (4.3%) |
| ADHD testing | |
| DIVA-ADHD subtypes among ADHD patients | |
| Inattentive | 1 (4.3%) |
| Hyperactive/Impulsive | 1 (4.3%) |
| Combined | 13 (56.5%) |
| WRI (n = 27, mean, (±SD)) | |
| Attention disorder | 6.81 (±3.03) |
| Overactivity | 3.7 (±1.82) |
| Temperament | 2.89 (±2.29) |
| Affective lability | 3.85 (±2.48) |
| Stress intolerance | 3.74 (±2.19) |
| Disorganization | 6.93 (±2.97) |
| Impulsiveness | 5.41 (±2.1) |
| Total | 4.76 (±1.7) |
| WURS-k total (n = 26 mean, (±SD)) | 36.81 (±11.23) |
| Psychological Questionnaires | |
| GHQ-28 (n = 25 mean, (±SD)) | 1.17 (±0.47) |
| Somatic symptoms | 1.17 (±0.52) |
| Anxiety/insomnia | 1.35 (±0.61) |
| Social dysfunction | 1.39 (±0.53) |
| Severe depression | 0.77 (±0.6) |
| UPPS (n = 22 mean, (±SD)) | |
| Urgency | 2.53 (±0.39) |
| Lack of premeditation | 2.53 (±0.48) |
| Lack of perseverance | 2.54 (±0.26) |
| Sensation seeking | 2.56 (±0.33) |
| Total | 2.54 (±0.15) |
| Neuropsychological testing | |
| Nesplora principal components (n = 29 mean, (±SD)) | |
| Motor activity | 0.00 (±1.00) |
| Inattention | 0.00 (±1.00) |
| Switching | 0.00 (±1.00) |
| Reaction time | 0.00 (±1.00) |
| Impulsivity | 0.00 (±1.00) |
| Qb-Test principal components (n = 29 mean, (±SD)) | |
| Activity | 1.95 (±1.19) |
| Impulsivity | 1.08 (±1.01) |
| Inattention | 0.94 (±1.17) |
| Nesplora variables (n = 29 mean, (±SD)) | |
| Perseverative errors (n) | 16.66 (±6.78) |
| Switching reaction time (mean) (ms) | −8894.12 (±2611.34) |
| Switching correct answers (n) | −16.67 (±2.72) |
| Total commission errors (n) | 18.17 (±7.28) |
| Commission errors reaction time (mean) (ms) | 747.97 (±189.27) |
| Commission errors reaction time (SD) (ms) | 133,201.5 (±82,565.08) |
| Discrepancy of correct answers (n) | −0.121 (±3.18) |
| Correct answers reaction time (mean) (ms) | 953.83 (±119.48) |
| Correct answers reaction time (SD) (ms) | 98,724.49 (±35,981.23) |
| Sum of distance (mean) | 0.2914 (±0.26) |
| Dual task correct answers (n) | 119.64 (±10.34) |
| Total omission errors (n) | 22.55 (±19.5) |
| Movement in the pitch shaft (mean) | 0.10 (±0.07) |
| Movement in the roll shaft (mean) | 0.08 (±0.08) |
| Movement in the yaw shaft (mean) | 0.11 (±0.12) |
| Qb-Test variables (n = 29 mean, (±SD)) | |
| Time active (>1 cm/s) | 23.62 (±16.91) |
| Distance (m) | 12.71 (±10.44) |
| Area (cm2) | 49.10 (±39.04) |
| Micro events (>1 mm) | 6301.9 (±4149.57) |
| Motion simplicity (n) | 44.24 (±12.34) |
| Total omission errors (n) | 12.39 (±13.91) |
| Total commission errors (n) | 1.74 (±1.67) |
| Correct answers reaction time (mean) | 609.9 (±109.69) |
| Correct answers reaction time (SD) | 177.52 (±61.35) |
| Rotated Factor Loadings | |||||
|---|---|---|---|---|---|
| Motor Activity | Inattention | Switching | Reaction Time | Impulsivity | |
| Sum of distance (mean) | 0.98 | ||||
| Movement in the yaw shaft (mean) | 0.96 | ||||
| Movement in the pitch shaft (mean) | 0.95 | ||||
| Movement in the roll shaft (mean) | 0.93 | ||||
| Total omission errors (n) | 0.95 | ||||
| Dual task correct answers (n) | −0.92 | ||||
| Correct answers reaction time (SD) (ms) | 0.92 | ||||
| Commission errors reaction time (SD) (ms) | 0.73 | 0.49 | |||
| Perseverative errors (n) | 0.67 | 0.31 | 0.48 | ||
| Switching reaction time (mean) (ms) | 0.91 | ||||
| Switching correct answers (n) | 0.31 | 0.87 | |||
| Discrepancy of correct answers (n) | 0.41 | −0.73 | |||
| Commission errors reaction time (mean) (ms) | 0.89 | ||||
| Correct answers reaction time (mean) (ms) | 0.80 | ||||
| Total commission errors (n) | 0.95 | ||||
| Qb-Test | |||
|---|---|---|---|
| Hyperactivity | Impulsivity | Inattention | |
| Nesplora Aquarium | r | r | r |
| Motor activity | 0.23 | −0.29 | 0.28 |
| Inattention | 0.26 | −0.02 | 0.49 * |
| Switching | 0.26 | 0.23 | −0.25 |
| Reaction time | −0.22 | −0.21 | −0.35 |
| Impulsivity | 0.06 | 0.04 | −0.007 |
| Qb-Test | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Hyperactivity | Inattention | Impulsivity | ||||||||
| Time Active (>1 cm/s) | Distance (m) | Area (cm2) | Micro Events (>1 mm) | Motion Simplicity (n) | Omission Errors (n) | Correct Answers Reaction Time (mean) | Correct Answers Reaction Time (SD) | Commission Errors (n) | Normalized Commission Errors (n) | |
| Nesplora Aquarium | ||||||||||
| Perseveration errors (n) | 0.12 | 0.14 | 0.23 | 0.15 | 0.40 * | 0.41 * | −0.05 | 0.22 | −0.21 | −0.20 |
| Switching reaction time (mean) (ms) | 0.18 | 0.28 | 0.29 | 0.23 | 0.03 | 0.03 | −0.36 | −0.009 | 0.14 | 0.13 |
| Switching correct answers (n) | 0.26 | 0.26 | 0.28 | 0.28 | 0.19 | 0.11 | −0.27 | 0.02 | 0.15 | 0.16 |
| Total commission errors (n) | 0.18 | 0.10 | 0.16 | 0.16 | 0.27 | 0.05 | −0.08 | 0.12 | 0.14 | 0.14 |
| Total omission errors (n) | 0.08 | 0.18 | 0.24 | 0.13 | 0.39 | 0.58 **,† | 0.27 | 0.50 * | −0.03 | 0.03 |
| Commission errors reaction time (mean) (ms) | −0.38 | −0.41 * | −0.41 * | −0.41 * | −0.38 | −0.02 | −0.34 | −0.28 | −0.20 | −0.19 |
| Commission errors reaction time (SD) (ms) | −0.03 | 0.03 | 0.13 | 0.02 | 0.36 | 0.33 | 0.07 | 0.17 | −0.23 | −0.21 |
| Correct answers reaction time (mean) (ms) | −0.11 | −0.11 | −0.09 | −0.11 | −0.02 | −0.04 | −0.12 | −0.19 | −0.25 | −0.26 |
| Correct answers reaction time (SD) (ms) | 0.03 | 0.09 | 0.17 | 0.06 | 0.43 * | 0.48 * | 0.38 | 0.52 **,† | 0.15 | 0.19 |
| Discrepancy of correct answers (n) | −0.36 | −0.27 | −0.32 | −0.34 | −0.19 | 0.18 | 0.42 * | 0.35 | 0.23 | 0.26 |
| Dual task correct answers (n) | −0.13 | −0.19 | −0.27 | −0.17 | −0.44 * | −0.53 **,† | −0.21 | −0.48 * | −0.02 | −0.08 |
| Sum of distance (mean) | 0.10 | 0.08 | 0.17 | 0.12 | 0.38 | 0.46 * | 0.14 | 0.20 | −0.08 | −0.05 |
| Movement in the pitch shaft (mean) | 0.11 | 0.07 | 0.15 | 0.13 | 0.35 | 0.35 | 0.01 | 0.08 | −0.10 | −0.06 |
| Movement in the roll shaft (mean) | 0.08 | 0.04 | 0.13 | 0.09 | 0.36 | 0.53 **,† | 0.17 | 0.18 | −0.20 | −0.17 |
| Movement in the yaw shaft (mean) | 0.09 | 0.11 | 0.20 | 0.12 | 0.38 | 0.45 * | 0.18 | 0.27 | 0.02 | 0.06 |
| WRI | |||||||||||
| Attention Disorder | Overactivity | Temperament | Affective Lability | Stress Intolerance | Disorganization | Impulsiveness | TOTAL | Total WURS-k | |||
| Nesplora Aquarium | |||||||||||
| Motor activity | 0.25 | 0.52 * | 0.36 | 0.61 * | 0.32 | 0.30 | 0.53 * | 0.58 * | −0.08 | ||
| Inattention | 0.48 | 0.08 | −0.17 | 0.22 | 0.40 | 0.30 | 0.30 | 0.34 | 0.33 | ||
| Switching | 0.41 | 0.56 * | 0.37 | 0.39 | −0.02 | 0.08 | −0.03 | 0.34 | 0.06 | ||
| Reaction time | −0.36 | 0.12 | 0.26 | 0.03 | 0.008 | −0.15 | −0.18 | −0.07 | 0.10 | ||
| Impulsivity | −0.14 | −0.32 | −0.46 | −0.62 ** | −0.34 | −0.36 | −0.17 | −0.50 * | −0.32 | ||
| QB-Test | |||||||||||
| Hyperactivity | 0.45 | 0.71 **,† | 0.52 * | 0.47 | 0.20 | −0.02 | 0.47 | 0.54 * | 0.50 * | ||
| Impulsivity | 0.34 | −0.22 | −0.46 | −0.21 | 0.08 | 0.37 | −0.08 | −0.003 | −0.09 | ||
| Inattention | 0.28 | −0.29 | −0.42 | 0.02 | 0.37 | 0.20 | 0.13 | 0.09 | 0.16 | ||
| UPPS | GHQ−28 | ||||||||||
| Urgency | Lack of Premeditation | Lack of Perseverance | Sensation Seeking | Total | Somatic Symptoms | Anxiety/Insomnia | Social Dysfunction | Depression | Total | ||
| Nesplora Aquarium | |||||||||||
| Motor activity | 0.15 | −0.09 | 0.08 | 0.16 | 0.14 | −0.14 | 0.03 | 0.06 | −0.001 | −0.01 | |
| Inattention | −0.37 | 0.15 | 0.07 | 0.02 | −0.05 | 0.20 | 0.18 | 0.12 | −0.01 | 0.15 | |
| Switching | 0.32 | −0.45 | −0.41 | 0.17 | −0.24 | 0.12 | 0.23 | 0.42 | −0.11 | 0.21 | |
| Reaction time | 0.04 | −0.18 | 0.19 | 0.03 | −0.03 | 0.21 | 0.41 | 0.23 | 0.39 | 0.39 | |
| Impulsivity | 0.08 | 0.27 | −0.05 | −0.46 | −0.03 | 0.13 | −0.19 | −0.02 | 0.33 | 0.06 | |
| QB-Test | |||||||||||
| Hyperactivity | 0.44 | −0.44 | −0.27 | 0.25 | −0.06 | 0.28 | 0.44 | 0.46 | 0.15 | 0.42 | |
| Impulsivity | −0.49 * | 0.04 | 0.07 | −0.13 | −0.28 | −0.20 | −0.28 | −0.23 | −0.07 | −0.24 | |
| Inattention | −0.44 | 0.48 | 0.34 | −0.12 | 0.19 | −0.32 | −0.19 | −0.13 | −0.31 | −0.29 | |
| WRI | ||||||||||
| Attention Disorder | Overactivity | Temperament | Affective Lability | Stress Intolerance | Disorganization | Impulsiveness | Total | Total WURS-k | ||
| Nesplora Aquarium | ||||||||||
| Perseveration errors (n) | 0.50 * | 0.52 * | 0.11 | 0.33 | 0.21 | 0.09 | 0.14 | 0.38 | 0.29 | |
| Switching reaction time (mean) (ms) | 0.50 * | 0.55 * | 0.25 | 0.43 | 0.03 | 0.19 | −0.03 | 0.39 | 0.009 | |
| Switching correct answers (n) | 0.48 | 0.45 | 0.19 | 0.27 | 0.02 | 0.13 | 0.11 | 0.33 | 0.1 | |
| Total commission errors (n) | 0.11 | −0.11 | −0.39 | −0.38 | −0.17 | −0.21 | 0.08 | −0.22 | −0.29 | |
| Total omission errors (n) | 0.50 * | 0.12 | −0.08 | 0.33 | 0.42 | 0.37 | 0.37 | 0.43 | 0.25 | |
| Commission errors reaction time (mean) (ms) | −0.50 * | −0.20 | 0.01 | −0.22 | −0.08 | −0.16 | −0.33 | −0.30 | −0.10 | |
| Commission errors reaction time (SD) (ms) | 0.21 | 0.37 | 0.29 | 0.50 * | 0.48 | 0.17 | 0.28 | 0.46 | 0.35 | |
| Correct answers reaction time (mean) (ms) | −0.29 | 0.11 | 0.19 | 0.01 | 0.02 | −0.08 | −0.10 | −0.04 | 0.26 | |
| Correct answers reaction time (SD) (ms) | 0.35 | −0.05 | −0.26 | −0.005 | 0.26 | 0.19 | 0.18 | 0.15 | 0.26 | |
| Discrepancy of correct answers (n) | −0.22 | −0.63 ** | −0.60 * | −0.43 | 0.04 | 0.08 | −0.04 | −0.34 | −0.02 | |
| Dual task correct answers (n) | −0.56 * | −0.09 | 0.21 | −0.22 | −0.38 | −0.32 | −0.42 | −0.38 | −0.17 | |
| Sum of distance (mean) | 0.42 | 0.53 * | 0.24 | 0.58 * | 0.33 | 0.36 | 0.53 * | 0.61 * | −0.07 | |
| Movement in the pitch shaft (mean) | 0.36 | 0.43 | 0.28 | 0.53 * | 0.28 | 0.34 | 0.54 * | 0.56 * | −0.18 | |
| Movement in the roll shaft (mean) | 0.38 | 0.60 * | 0.32 | 0.54 * | 0.24 | 0.18 | 0.58 * | 0.56 * | 0.06 | |
| Movement in the yaw shaft (mean) | 0.44 | 0.53 * | 0.17 | 0.59 * | 0.39 | 0.42 | 0.46 | 0.61 ** | −0.05 | |
| Qb−Test | ||||||||||
| Time active (>1 cm/s) | 0.27 | 0.55 * | 0.42 | 0.18 | −0.10 | −0.04 | 0.26 | 0.29 | 0.45 | |
| Distance (m) | 0.51 * | 0.58 * | 0.42 | 0.33 | 0.06 | 0.19 | 0.3 | 0.48 | 0.58 * | |
| Area (cm2) | 0.60 * | 0.63 ** | 0.44 | 0.38 | 0.09 | 0.17 | 0.31 | 0.52 * | 0.55 * | |
| Micro events (>1 mm) | 0.4 | 0.61 * | 0.48 | 0.29 | −0.02 | 0.06 | 0.32 | 0.41 | 0.53 * | |
| Motion simplicity (n) | 0.64 **,† | 0.45 | 0.44 | 0.41 | 0.25 | −0.07 | 0.39 | 0.49 * | 0.38 | |
| Omission errors (n) | 0.28 | 0.07 | −0.27 | 0.23 | 0.47 | 0.22 | 0.35 | 0.29 | 0.37 | |
| Correct answers reaction time (mean) (ms) | 0.02 | −0.37 | −0.38 | −0.13 | 0.22 | −0.02 | 0.22 | −0.08 | 0.24 | |
| Correct answers reaction time (SD) (ms) | 0.3 | −0.22 | −0.35 | 0.04 | 0.37 | 0.35 | 0.11 | 0.15 | 0.26 | |
| Commission errors (n) | 0.26 | −0.23 | −0.34 | −0.18 | 0.07 | 0.32 | 0.06 | 0.02 | 0.03 | |
| Normalized commission errors(n) | 0.26 | −0.26 | −0.39 | −0.17 | 0.11 | 0.34 | 0.12 | 0.03 | 0.04 | |
| UPPS | GHQ-28 | |||||||||
| Urgency | Lack of Premeditation | lack of Perseverance | Sensation Seeking | Total | Somatic Symptoms | Anxiety/Insomnia | Social Dysfunction | Depression | Total | |
| Nesplora Aquarium | ||||||||||
| Switching correct answers (n) | 0.16 | −0.32 | −0.34 | 0.08 | −0.25 | 0.07 | 0.22 | 0.39 | 0.09 | 0.24 |
| Total commission errors (n) | 0.06 | 0.25 | −0.12 | −0.40 | −0.05 | 0.13 | −0.17 | 0.02 | 0.26 | 0.06 |
| Total omission errors (n) | −0.35 | 0.12 | −0.05 | −0.01 | −0.13 | 0.18 | 0.2 | 0.1 | −0.08 | 0.13 |
| Commission errors reaction time (mean) (ms) | −0.10 | 0.02 | 0.33 | −0.08 | 0.04 | 0.12 | 0.22 | 0.12 | 0.43 | 0.27 |
| Commission errors reaction time (SD) (ms) | −0.18 | −0.07 | 0.21 | 0.17 | 0.02 | 0.23 | 0.46 | 0.3 | 0.13 | 0.35 |
| Correct answers reaction time (mean) (ms) | −0.01 | −0.19 | 0.13 | 0.08 | −0.06 | 0.21 | 0.38 | 0.09 | 0.27 | 0.3 |
| Correct answers reaction time (SD) (ms) | −0.38 | 0.18 | 0.16 | 0.05 | 0.02 | 0.22 | 0.14 | 0.17 | 0.23 | 0.23 |
| Discrepancy of correct answers (n) | −0.41 | 0.53 * | 0.47 | −0.11 | 0.3 | −0.24 | −0.43 | −0.51 * | −0.08 | −0.39 |
| Dual task correct answers (n) | 0.34 | −0.21 | 0.09 | 0.15 | 0.15 | −0.24 | −0.15 | −0.11 | 0.001 | −0.16 |
| Sum of distance (mean) | 0.13 | −0.06 | 0.04 | 0.15 | 0.12 | −0.15 | −0.04 | 0.08 | −0.06 | −0.05 |
| Movement in the pitch shaft (mean) | 0.11 | −0.02 | −0.02 | 0.1 | 0.09 | −0.08 | −0.007 | 0.09 | 0.03 | 0.01 |
| Movement in the roll shaft (mean) | 0.33 | −0.11 | −0.06 | 0.16 | 0.16 | −0.006 | 0.06 | 0.12 | 0.05 | 0.07 |
| Movement in the yaw shaft (mean) | 0.02 | −0.08 | 0.13 | 0.17 | 0.1 | −0.24 | −0.09 | 0.05 | −0.15 | −0.13 |
| Qb−Test | ||||||||||
| Time active (>1 cm/s) | 0.50 * | −0.51 * | −0.39 | 0.28 | −0.11 | 0.31 | 0.36 | 0.3 | 0.21 | 0.37 |
| Distance (m) | 0.43 | −0.42 | −0.30 | 0.38 | 0.01 | 0.1 | 0.22 | 0.09 | −0.22 | 0.07 |
| Area (cm2) | 0.43 | −0.40 | −0.29 | 0.37 | 0.02 | 0.14 | 0.27 | 0.09 | −0.20 | 0.1 |
| Micro events (>1 mm) | 0.52 * | −0.49 * | −0.36 | 0.34 | −0.04 | 0.23 | 0.33 | 0.23 | 0.04 | 0.26 |
| Motion simplicity (n) | 0.26 | −0.11 | −0.22 | 0.13 | 0.05 | 0.3 | 0.42 | 0.23 | 0 | 0.3 |
| Omission errors (n) | −0.34 | 0.21 | 0.37 | −0.06 | 0.09 | −0.21 | 0.1 | −0.04 | 0.04 | −0.03 |
| Correct answers reaction time (mean) (ms) | −0.34 | 0.4 | 0.26 | −0.10 | 0.16 | −0.31 | −0.17 | −0.17 | −0.13 | −0.24 |
| Correct answers reaction time (SD) (ms) | −0.51 * | 0.22 | 0.22 | 0.02 | −0.01 | −0.21 | −0.19 | −0.17 | −0.38 | −0.29 |
| Commission errors (n) | −0.40 | 0.03 | 0.03 | 0.03 | −0.16 | −0.21 | −0.35 | −0.25 | −0.19 | −0.31 |
| Normalized commission errors(n) | −0.47 | 0.09 | 0.04 | −0.02 | −0.19 | −0.24 | −0.33 | −0.27 | −0.17 | −0.32 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baader, A.; Kiani, B.; Brunkhorst-Kanaan, N.; Kittel-Schneider, S.; Reif, A.; Grimm, O. A Within-Sample Comparison of Two Innovative Neuropsychological Tests for Assessing ADHD. Brain Sci. 2021, 11, 36. https://doi.org/10.3390/brainsci11010036
Baader A, Kiani B, Brunkhorst-Kanaan N, Kittel-Schneider S, Reif A, Grimm O. A Within-Sample Comparison of Two Innovative Neuropsychological Tests for Assessing ADHD. Brain Sciences. 2021; 11(1):36. https://doi.org/10.3390/brainsci11010036
Chicago/Turabian StyleBaader, Anna, Behnaz Kiani, Nathalie Brunkhorst-Kanaan, Sarah Kittel-Schneider, Andreas Reif, and Oliver Grimm. 2021. "A Within-Sample Comparison of Two Innovative Neuropsychological Tests for Assessing ADHD" Brain Sciences 11, no. 1: 36. https://doi.org/10.3390/brainsci11010036
APA StyleBaader, A., Kiani, B., Brunkhorst-Kanaan, N., Kittel-Schneider, S., Reif, A., & Grimm, O. (2021). A Within-Sample Comparison of Two Innovative Neuropsychological Tests for Assessing ADHD. Brain Sciences, 11(1), 36. https://doi.org/10.3390/brainsci11010036