One-Year Follow-Up Diagnostic Stability of Autism Spectrum Disorder Diagnosis in a Clinical Sample of Children and Toddlers

 , ,
, ,  ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Design and Procedure
2.2. Participants
- Group 1 (n = 8) Sub-Threshold Symptoms (STS): children with isolated symptoms or very mild symptoms, not fully consistent with the criteria for the disorder (ADOS severity score between 1 and 2).
- Group 2 (n = 68) Autism Spectrum Disorder (ASD): children that still met the DSM-5 criteria for ASD but with mild symptom severity (ADOS severity score between 3 and 4).
- Group 3 (n = 71) Autistic Disorder (AD): children with the highest symptom severity that fully met the DSM-5 criteria for ASD (ADOS severity score between 5 and 7).
2.3. Measures
Autism Severity
2.4. Statistical Approach
3. Results
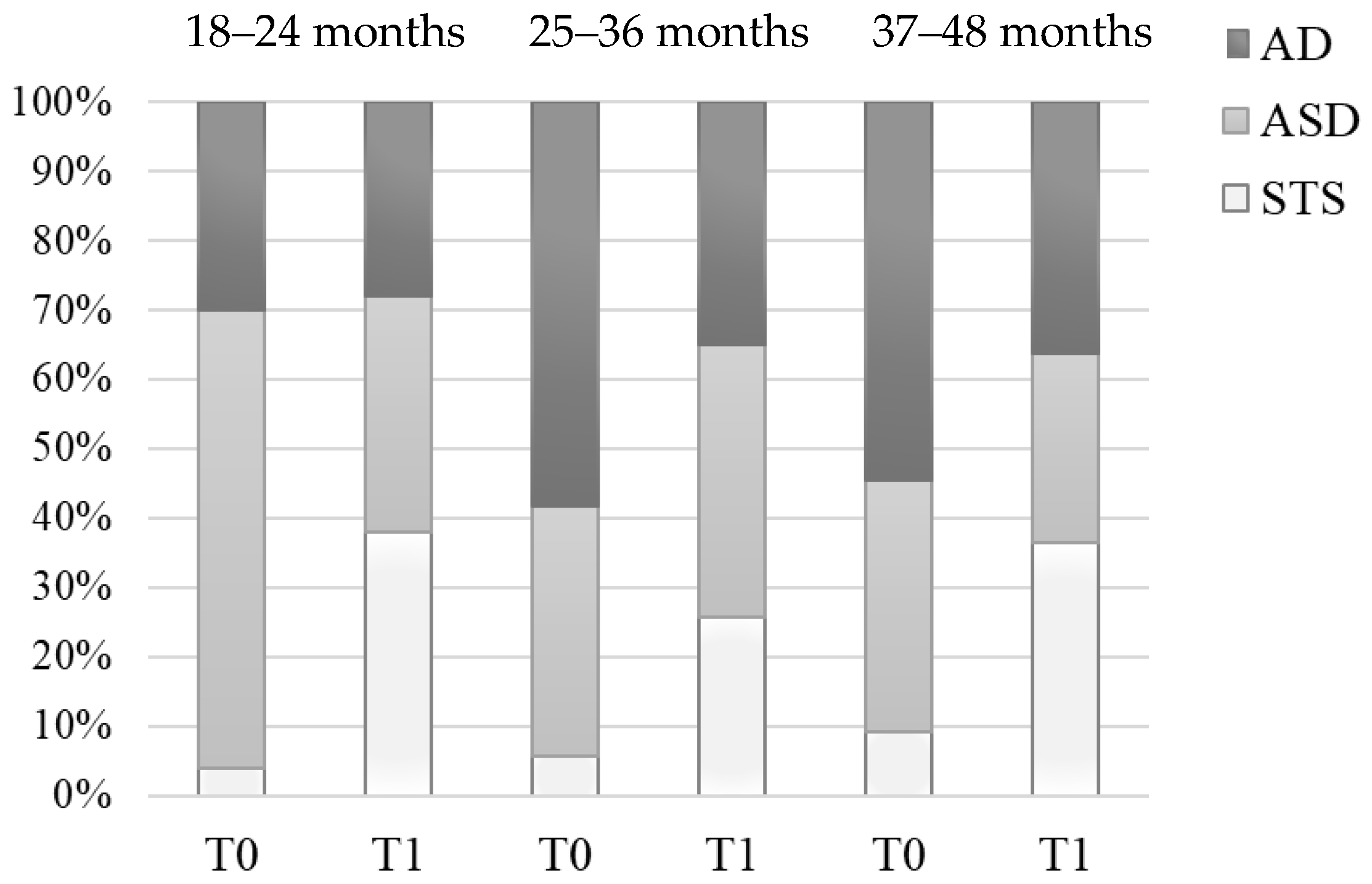
3.1. Severity Class Distribution at Baseline vs. Follow-Up (T0 vs. T1)
3.2. Stability and Diagnostic Parameters (T0 vs. T1)
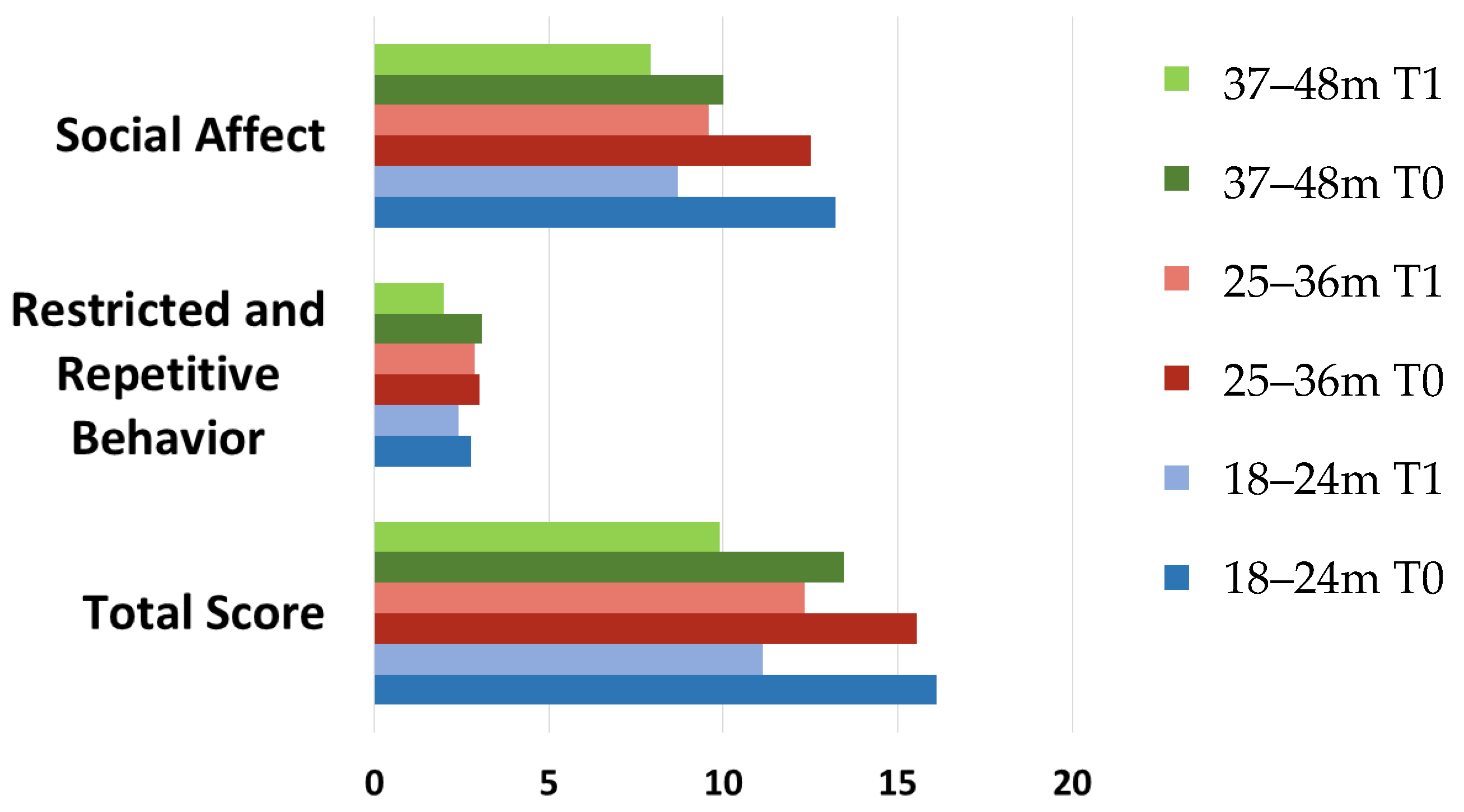
3.3. ADOS-2 Subscales at Baseline vs. Follow-Up (T0 vs. T1)
4. Discussion
4.1. Diagnostic Stability in Function of Different Age Classes Compared to Different Severity Levels
4.2. Diagnostic Reliability in Relation to Different Age Classes
4.3. Follow-Up Outcomes Assessed by the ADOS-2 Subscale Scores at Baseline and Follow-Up
5. Limitations and Future Directions
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lord, C.; Cook, E.H.; Leventhal, B.L.; Amaral, D.G. Autism spectrum disorders. Neuron 2000, 28, 355–363. [Google Scholar] [CrossRef] [Green Version]
- Honey, E.; Rodgers, J.; McConachie, H. Measurement of restricted and repetitive behaviour in children with autism spectrum disorder: Selecting a questionnaire or interview. Res. Autism Spectr. Disord. 2012, 6, 757–776. [Google Scholar] [CrossRef]
- Lai, M.-C.; Kassee, C.; Besney, R.; Bonato, S.; Hull, L.; Mandy, W.; Szatmari, P.; Ameis, S.H. Prevalence of co-occurring mental health diagnoses in the autism population: A systematic review and meta-analysis. Lancet Psychiatry 2019, 6, 819–829. [Google Scholar] [CrossRef]
- Vetri, L. Autism and Migraine: An Unexplored Association? Brain Sci. 2020, 10, 615. [Google Scholar] [CrossRef]
- Marotta, R.; Risoleo, M.C.; Messina, G.; Parisi, L.; Carotenuto, M.; Vetri, L.; Roccella, M. The Neurochemistry of Autism. Brain Sci. 2020, 10, 163. [Google Scholar] [CrossRef] [Green Version]
- Baio, J.; Wiggins, L.; Christensen, D.L.; Maenner, M.J.; Daniels, J.; Warren, Z.; Kurzius-Spencer, M.; Zahorodny, W.; Rosenberg, C.R.; White, T. Prevalence of autism spectrum disorder among children aged 8 years—Autism and developmental disabilities monitoring network, 11 sites, United States, 2014. MMWR Surveill. Summ. 2018, 67, 1. [Google Scholar] [CrossRef]
- Hansen, S.N.; Schendel, D.E.; Parner, E.T. Explaining the increase in the prevalence of autism spectrum disorders: The proportion attributable to changes in reporting practices. JAMA Pediatr. 2015, 169, 56–62. [Google Scholar] [CrossRef] [Green Version]
- Tordjman, S.; Somogyi, E.; Coulon, N.; Kermarrec, S.; Cohen, D.; Bronsard, G.; Bonnot, O.; Weismann-Arcache, C.; Botbol, M.; Lauth, B. Gene× Environment interactions in autism spectrum disorders: Role of epigenetic mechanisms. Front. Psychiatry 2014, 5, 53. [Google Scholar] [CrossRef] [Green Version]
- Buescher, A.V.S.; Cidav, Z.; Knapp, M.; Mandell, D.S. Costs of autism spectrum disorders in the United Kingdom and the United States. JAMA Pediatrics 2014, 168, 721–728. [Google Scholar] [CrossRef] [PubMed]
- Dawson, G.; Jones, E.J.H.; Merkle, K.; Venema, K.; Lowy, R.; Faja, S.; Kamara, D.; Murias, M.; Greenson, J.; Winter, J. Early behavioral intervention is associated with normalized brain activity in young children with autism. J. Am. Acad. Child Adolesc. Psychiatry 2012, 51, 1150–1159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dawson, G.; Rogers, S.; Munson, J.; Smith, M.; Winter, J.; Greenson, J.; Donaldson, A.; Varley, J. Randomized, controlled trial of an intervention for toddlers with autism: The Early Start Denver Model. Pediatrics 2010, 125, e17–e23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leaf, J.B.; Taubman, M.; Bloomfield, S.; Palos-Rafuse, L.; Leaf, R.; McEachin, J.; Oppenheim, M.L. Increasing social skills and pro-social behavior for three children diagnosed with autism through the use of a teaching package. Res. Autism Spectr. Disord. 2009, 3, 275–289. [Google Scholar] [CrossRef]
- McEachin, J.J.; Smith, T.; Ivar Lovaas, O. Long-term outcome for children with autism who received early intensive behavioral treatment. Am. J. Ment. Retard. 1993, 97, 359. [Google Scholar] [PubMed]
- Rogers, S.J.; Vismara, L.; Wagner, A.L.; McCormick, C.; Young, G.; Ozonoff, S. Autism treatment in the first year of life: A pilot study of infant start, a parent-implemented intervention for symptomatic infants. J. Autism Dev. Disord. 2014, 44, 2981–2995. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taubman, M.; Brierley, S.; Wishner, J.; Baker, D.; McEachin, J.; Leaf, R.B. The effectiveness of a group discrete trial instructional approach for preschoolers with developmental disabilities. Res. Dev. Disabil. 2001, 22, 205–219. [Google Scholar] [CrossRef]
- Wetherby, A.M.; Guthrie, W.; Woods, J.; Schatschneider, C.; Holland, R.D.; Morgan, L.; Lord, C. Parent-implemented social intervention for toddlers with autism: An RCT. Pediatrics 2014, 134, 1084–1093. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Granpeesheh, D.; Tarbox, J.; Dixon, D.R. Applied behavior analytic interventions for children with autism: A description and review of treatment research. Ann. Clin. Psychiatry 2009, 21, 162–173. [Google Scholar]
- Johnson, C.P.; Myers, S.M. Identification and evaluation of children with autism spectrum disorders. Pediatrics 2007, 120, 1183–1215. [Google Scholar] [CrossRef] [Green Version]
- Vismara, L.A.; Rogers, S.J. Behavioral treatments in autism spectrum disorder: What do we know? Annu. Rev. Clin. Psychol. 2010, 6, 447–468. [Google Scholar] [CrossRef] [Green Version]
- Warren, Z.; McPheeters, M.L.; Sathe, N.; Foss-Feig, J.H.; Glasser, A.; Veenstra-VanderWeele, J. A systematic review of early intensive intervention for autism spectrum disorders. Pediatrics 2011, 127, e1303–e1311. [Google Scholar] [CrossRef]
- Zwaigenbaum, L.; Bauman, M.L.; Choueiri, R.; Fein, D.; Kasari, C.; Pierce, K.; Stone, W.L.; Yirmiya, N.; Estes, A.; Hansen, R.L. Early identification and interventions for autism spectrum disorder: Executive summary. Pediatrics 2015, 136, S1–S9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zwaigenbaum, L.; Bryson, S.; Garon, N. Early identification of autism spectrum disorders. Behav. Brain Res. 2013, 251, 133–146. [Google Scholar] [CrossRef] [PubMed]
- Chasson, G.S.; Harris, G.E.; Neely, W.J. Cost comparison of early intensive behavioral intervention and special education for children with autism. J. Child Fam. Stud. 2007, 16, 401–413. [Google Scholar] [CrossRef]
- Howlin, P.; Magiati, I.; Charman, T. Systematic review of early intensive behavioral interventions for children with autism. Am. J. Intellect. Dev. Disabil. 2009, 114, 23–41. [Google Scholar] [CrossRef] [PubMed]
- Smith, T.; Klorman, R.; Mruzek, D.W. Predicting outcome of community-based early intensive behavioral intervention for children with autism. J. Abnorm. Child Psychol. 2015, 43, 1271–1282. [Google Scholar] [CrossRef] [PubMed]
- Hayward, D.; Eikeseth, S.; Gale, C.; Morgan, S. Assessing progress during treatment for young children with autism receiving intensive behavioural interventions. Autism 2009, 13, 613–633. [Google Scholar] [CrossRef]
- Sallows, G.O.; Graupner, T.D. Intensive behavioral treatment for children with autism: Four-year outcome and predictors. Am. J. Ment. Retard. 2005, 110, 417–438. [Google Scholar] [CrossRef]
- Reichow, B.; Barton, E.E.; Boyd, B.A.; Hume, K. Early intensive behavioral intervention (EIBI) for young children with autism spectrum disorders (ASD). Cochrane Database Syst. Rev. 2012. [Google Scholar] [CrossRef]
- Steiner, A.M.; Goldsmith, T.R.; Snow, A.V.; Chawarska, K. Practitioner’s guide to assessment of autism spectrum disorders in infants and toddlers. J. Autism Dev. Disord. 2012, 42, 1183–1196. [Google Scholar] [CrossRef] [Green Version]
- Luyster, R.; Gotham, K.; Guthrie, W.; Coffing, M.; Petrak, R.; Pierce, K.; Bishop, S.; Esler, A.; Hus, V.; Oti, R. The Autism Diagnostic Observation Schedule—Toddler Module: A new module of a standardized diagnostic measure for autism spectrum disorders. J. Autism Dev. Disord. 2009, 39, 1305–1320. [Google Scholar] [CrossRef] [Green Version]
- Bishop, S.L.; Luyster, R.; Richler, J.; Lord, C. Diagnostic assessment. In Autism Spectrum Disorders in Infants and Toddlers: Diagnosis, Assessment, and Treatment; Chawarska, K., Klin, A., Volkmar, F.R., Eds.; Guilford Press: New York, NY, USA, 2008; pp. 207–242. [Google Scholar]
- Baron-Cohen, S.; Cox, A.; Baird, G.; Swettenham, J.; Drew, A.; Nightingale, N.; Morgan, K.; Charman, T. Psychological markers ofautism at 18 months of age in a large population. Br. J. Psychiatry 1996, 168, 158–163. [Google Scholar] [CrossRef] [PubMed]
- Charman, T.; Taylor, E.; Drew, A.; Cockerill, H.; Brown, J.A.; Baird, G. Outcome at 7 years of children diagnosed with autism at age 2: Predictive validity of assessments conducted at 2 and 3 years of age and pattern of symptom change over time. J. Child Psychol. Psychiatry 2005, 46, 500–513. [Google Scholar] [CrossRef] [PubMed]
- Moore, V.; Goodson, S. How well does early diagnosis of autism stand the test of time? Follow-up study of children assessed for autism at age 2 and development of an early diagnostic service. Autism 2003, 7, 47–63. [Google Scholar] [CrossRef] [PubMed]
- Lord, C. Follow-up of two-year-olds referred for possible autism. J. Child Psychol. Psychiatry 1995, 36, 1365–1382. [Google Scholar] [CrossRef]
- Stone, W.L.; Lee, E.B.; Ashford, L.; Brissie, J.; Hepburn, S.L.; Coonrod, E.E.; Weiss, B.H. Can autism be diagnosed accurately in children under 3 years? J. Child Psychol. Psychiatry 1999, 40, 219–226. [Google Scholar] [CrossRef]
- Siu, A.L.; Bibbins-Domingo, K.; Grossman, D.C.; Baumann, L.C.; Davidson, K.W.; Ebell, M.; García, F.A.R.; Gillman, M.; Herzstein, J.; Kemper, A.R. Screening for autism spectrum disorder in young children: US Preventive Services Task Force recommendation statement. JAMA 2016, 315, 691–696. [Google Scholar] [CrossRef] [Green Version]
- Mundy, P. A review of joint attention and social-cognitive brain systems in typical development and autism spectrum disorder. Eur. J. Neurosci. 2018, 47, 497–514. [Google Scholar] [CrossRef]
- Perin, C.; Valagussa, G.; Mazzucchelli, M.; Gariboldi, V.; Cerri, C.G.; Meroni, R.; Grossi, E.; Cornaggia, C.M.; Menant, J.; Piscitelli, D. Physiological Profile Assessment of Posture in Children and Adolescents with Autism Spectrum Disorder and Typically Developing Peers. Brain Sci. 2020, 10, 681. [Google Scholar] [CrossRef] [PubMed]
- Baio, J. Prevalence of autism spectrum disorder among children aged 8 years-autism and developmental disabilities monitoring network, 11 sites, United States, 2010. Mmwr Surveill. Summ. Morb. Mortal. Wkly. Rep. Surveill. Summ. 2014, 63, 1–21. [Google Scholar]
- Christensen, D.L.; Braun, K.V.N.; Baio, J.; Bilder, D.; Charles, J.; Constantino, J.N.; Daniels, J.; Durkin, M.S.; Fitzgerald, R.T.; Kurzius-Spencer, M. Prevalence and characteristics of autism spectrum disorder among children aged 8 years—Autism and developmental disabilities monitoring network, 11 sites, United States, 2012. Mmwr Surveill. Summ. 2018, 65, 1. [Google Scholar] [CrossRef]
- Rondeau, E.; Klein, L.S.; Masse, A.; Bodeau, N.; Cohen, D.; Guilé, J.-M. Is pervasive developmental disorder not otherwise specified less stable than autistic disorder? A meta-analysis. J. Autism Dev. Disord. 2011, 41, 1267–1276. [Google Scholar] [CrossRef] [PubMed]
- Woolfenden, S.; Sarkozy, V.; Ridley, G.; Williams, K. A systematic review of the diagnostic stability of autism spectrum disorder. Res. Autism Spectr. Disord. 2012, 6, 345–354. [Google Scholar] [CrossRef]
- Kantzer, A.K.; Fernell, E.; Westerlund, J.; Hagberg, B.; Gillberg, C.; Miniscalco, C. Young children who screen positive for autism: Stability, change and “comorbidity” over two years. Res. Dev. Disabil. 2018, 72, 297–307. [Google Scholar] [CrossRef] [PubMed]
- Maenner, M.J.; Rice, C.E.; Arneson, C.L.; Cunniff, C.; Schieve, L.A.; Carpenter, L.A.; Braun, K.V.N.; Kirby, R.S.; Bakian, A.V.; Durkin, M.S. Potential impact of DSM-5 criteria on autism spectrum disorder prevalence estimates. JAMA Psychiatry 2014, 71, 292–300. [Google Scholar] [CrossRef] [Green Version]
- Anderson, D.K.; Liang, J.W.; Lord, C. Predicting young adult outcome among more and less cognitively able individuals with autism spectrum disorders. J. Child Psychol. Psychiatry 2014, 55, 485–494. [Google Scholar] [CrossRef]
- Troyb, E.; Orinstein, A.; Tyson, K.; Eigsti, I.-M.; Naigles, L.; Fein, D. Restricted and repetitive behaviors in individuals with a history of ASDs who have achieved optimal outcomes. J. Autism Dev. Disord. 2014, 44, 3168–3184. [Google Scholar] [CrossRef] [Green Version]
- Ozonoff, S.; Young, G.S.; Landa, R.J.; Brian, J.; Bryson, S.; Charman, T.; Chawarska, K.; Macari, S.L.; Messinger, D.; Stone, W.L. Diagnostic stability in young children at risk for autism spectrum disorder: A baby siblings research consortium study. J. Child Psychol. Psychiatry 2015, 56, 988–998. [Google Scholar] [CrossRef] [Green Version]
- Robins, D.L.; Casagrande, K.; Barton, M.; Chen, C.-M.A.; Dumont-Mathieu, T.; Fein, D. Validation of the modified checklist for autism in toddlers, revised with follow-up (M-CHAT-R/F). Pediatrics 2014, 133, 37–45. [Google Scholar] [CrossRef] [Green Version]
- Lord, C.; Rutter, M.; DiLavore, P.; Risi, S.; Gotham, K.; Bishop, S. Autism Diagnostic Observation Schedule–Second Edition (ADOS-2); Western Psychological Services: Los Angeles, CA, USA, 2012. [Google Scholar]
- Pierce, K.; Gazestani, V.H.; Bacon, E.; Barnes, C.C.; Cha, D.; Nalabolu, S.; Lopez, L.; Moore, A.; Pence-Stophaeros, S.; Courchesne, E. Evaluation of the Diagnostic Stability of the Early Autism Spectrum Disorder Phenotype in the General Population Starting at 12 Months. JAMA Pediatr. 2019, 173, 578–587. [Google Scholar] [CrossRef]
- Towle, P.O.; Patrick, P.A.; Ridgard, T.; Pham, S.; Marrus, J. Is Earlier Better? The Relationship between Age When Starting Early Intervention and Outcomes for Children with Autism Spectrum Disorder: A Selective Review. Autism. Res. Treat. 2020, 2020, 7605876. [Google Scholar] [CrossRef]
- Oliver, C.; Petty, J.; Ruddick, L.; Bacarese-Hamilton, M. The association between repetitive, self-injurious and aggressive behavior in children with severe intellectual disability. J. Autism Dev. Disord. 2012, 42, 910–919. [Google Scholar] [CrossRef] [PubMed]
- Hinnebusch, A.J.; Miller, L.E.; Fein, D.A. Autism spectrum disorders and low mental age: Diagnostic stability and developmental outcomes in early childhood. J. Autism Dev. Disord. 2017, 47, 3967–3982. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simms, M.D. When autistic behavior suggests a disease other than classic autism. Pediatric Clin. 2017, 64, 127–138. [Google Scholar] [CrossRef] [PubMed]
- Blumberg, S.J.; Zablotsky, B.; Avila, R.M.; Colpe, L.J.; Pringle, B.A.; Kogan, M.D. Diagnosis lost: Differences between children who had and who currently have an autism spectrum disorder diagnosis. Autism 2016, 20, 783–795. [Google Scholar] [CrossRef] [Green Version]
- Wiggins, L.D.; Baio, J.; Schieve, L.; Lee, L.-C.; Nicholas, J.; Rice, C.E. Retention of autism spectrum diagnoses by community professionals: Findings from the autism and developmental disabilities monitoring network, 2000 and 2006. J. Dev. Behav. Pediatr. JDBP 2012, 33, 387. [Google Scholar] [CrossRef] [Green Version]
- Luyster, R.; Qiu, S.; Lopez, K.; Lord, C. Predicting outcomes of children referred for autism using the MacArthur–Bates Communicative Development Inventory. J. Speechlanguageand Hear. Res. 2007. [Google Scholar] [CrossRef]
- Fein, D.; Barton, M.; Eigsti, I.M.; Kelley, E.; Naigles, L.; Schultz, R.T.; Stevens, M.; Helt, M.; Orinstein, A.; Rosenthal, M. Optimal outcome in individuals with a history of autism. J. Child Psychol. Psychiatry 2013, 54, 195–205. [Google Scholar] [CrossRef] [Green Version]
- Rogers, S.J. Developmental regression in autism spectrum disorders. Ment. Retard. Dev. Disabil. Res. Rev. 2004, 10, 139–143. [Google Scholar] [CrossRef]
- Bieleninik, Ł.; Posserud, M.-B.; Geretsegger, M.; Thompson, G.; Elefant, C.; Gold, C. Tracing the temporal stability of autism spectrum diagnosis and severity as measured by the Autism Diagnostic Observation Schedule: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0183160. [Google Scholar] [CrossRef] [Green Version]
- Morrier, M.J.; McGee, G.G.; Daly, T. Effects of toy selection and arrangement on the social behaviors of an inclusive group of preschool-aged children. Early Child. Serv. Interdiscip. J. Eff. 2009, 3, 157–177. [Google Scholar]
- Rogers, S.J.; Estes, A.; Lord, C.; Vismara, L.; Winter, J.; Fitzpatrick, A.; Guo, M.; Dawson, G. Effects of a brief Early Start Denver Model (ESDM)–based parent intervention on toddlers at risk for autism spectrum disorders: A randomized controlled trial. J. Am. Acad. Child Adolesc. Psychiatry 2012, 51, 1052–1065. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| a. (T0) | Age Classes | Total | ||||
|---|---|---|---|---|---|---|
| 18–24 Months | 25–36 Months | 37–48 Months | ||||
| Baseline Diagnosis | STS | Counting | 2 | 5 | 1 | 8 |
| T0-diagnosis % | 25.0% | 62.5% | 12.5% | 100.0% | ||
| Age classes % | 4.0% | 5.8% | 9.1% | 5.4% | ||
| Total % | 1.4% | 3.4% | 0.7% | 5.4% | ||
| ASD | Counting | 33 | 31 | 4 | 68 | |
| T0-diagnosis % | 48.5% | 45.6% | 5.9% | 100.0% | ||
| Age classes % | 66.0% | 36.0% | 36.4% | 46.3% | ||
| Total % | 22.4% | 21.1% | 2.7% | 46.3% | ||
| AD | Counting | 15 | 50 | 6 | 71 | |
| T0-diagnosis % | 21.1% | 70.4% | 8.5% | 100.0% | ||
| Age classes % | 30.0% | 58.1% | 54.5% | 48.3% | ||
| Total % | 10.2% | 34.0% | 4.1% | 48.3% | ||
| b. (T1) | ||||||
| Follow up Diagnosis | STS | Counting | 19 | 22 | 4 | 45 |
| T1-diagnosis % | 42.2% | 48.9% | 8.9% | 100.0% | ||
| Age classes % | 38.0% | 25.6% | 36.4% | 30.6% | ||
| Total % | 12.9% | 15.0% | 2.7% | 30.6% | ||
| ASD | Counting | 17 | 34 | 3 | 54 | |
| T1-diagnosis % | 31.5% | 63.0% | 5.6% | 100.0% | ||
| Age classes % | 34.0% | 39.5% | 27.3% | 36.7% | ||
| Total % | 11.6% | 23.1% | 2.0% | 36.7% | ||
| AD | Counting | 14 | 30 | 4 | 48 | |
| T1-diagnosis % | 29.2% | 62.5% | 8.3% | 100.0% | ||
| Age classes % | 28.0% | 34.9% | 36.4% | 32.7% | ||
| Total % | 9.5% | 20.4% | 2.7% | 32.7% | ||
| Total | Counting | 50 | 86 | 11 | 147 | |
| Age classes % | 100.0% | 100.0% | 100.0% | 100.0% | ||
| Total % | 34.0% | 58.5% | 7.5% | 100.0% | ||
| T0 | T1 | |||
|---|---|---|---|---|
| AD | ASD | STS | ||
| AD | 71 | 32 | ||
| 28 | ||||
| 11 | ||||
| ASD | 68 | 15 | ||
| 23 | ||||
| 30 | ||||
| STS | 8 | 1 | ||
| 3 | ||||
| 4 | ||||
| Total | 147 | 48 | 54 | 45 |
| T0 | T1 | Total | Classification |
|---|---|---|---|
| A | A | 98 (66.7%) | True positives |
| A | STS | 41(27.9%) | False positives |
| STS | A | 4 (2.7%) | False negatives |
| STS | STS | 4 (2.7%) | True negatives |
| Total | 147 |
| Diagnostic Parameters | |
|---|---|
| Sensitivity | 96.08% |
| Specificity | 8.89% |
| Positive Predictive Value | 70.50% |
| Negative Predictive Value | 50% |
| True Positive (n = 98) | False Positive (n = 41) | False Negative (n = 4) | True Negative (n = 4) | Sensitivity | Specificity | Positive Predicted Value | Negative Predicted Value | |
|---|---|---|---|---|---|---|---|---|
| 18–24 months (n = 50) | 30 | 18 | 1 | 1 | 96.77% | 5.26% | 62.50% | 50% |
| 25–35 months (n = 86) | 61 | 20 | 3 | 2 | 95.31% | 9.09% | 75.30% | 40% |
| 36–48 months (n = 11) | 7 | 3 | 0 | 1 | -- | -- | -- | -- |
| ADOS-2 Scales | T0 | T1 | ||
|---|---|---|---|---|
| 18–24 Months (n = 50) | ||||
| M | SD | M | SD | |
| Social Affect | 13.22 | 3.65 | 8.68 | 5.20 |
| Restricted and Repetitive Behavior | 2.76 | 1.70 | 2.42 | 1.80 |
| Total Score | 16.10 | 4.51 | 11.14 | 6.16 |
| 25–36 Months (n = 86) | ||||
| Social Affect | 12.52 | 4.57 | 9.57 | 5.37 |
| Restricted and Repetitive Behavior | 3.02 | 1.75 | 2.87 | 2.03 |
| Total Score | 15.53 | 5.50 | 12.33 | 6.37 |
| 37–48 Months (n = 11) | ||||
| Social Affect | 10.00 | 4.49 | 7.91 | 4.11 |
| Restricted and Repetitive Behavior | 3.09 | 1.58 | 2.00 | 1.41 |
| Total Score | 13.45 | 5.47 | 9.91 | 5.32 |
| 18–24 Months | ADOS-2–SA T1–T0 | ADOS-2–RRB T1–T0 |
|---|---|---|
| Z | −4.384 a | −0.783 a |
| p (2-tailed) | < 0.001 | 0.646 |
| 25–36 months | ||
| Z | −5.624 a | −0.631 a |
| p (2-tailed) | <0.001 | 0.528 |
| 37–48 months | ||
| Z | −1.637 a | −2.154 a |
| p (2-tailed) | 0.102 | 0.031 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Benedetto, L.; Cucinotta, F.; Maggio, R.; Germanò, E.; De Raco, R.; Alquino, A.; Impallomeni, C.; Siracusano, R.; Vetri, L.; Roccella, M.; et al. One-Year Follow-Up Diagnostic Stability of Autism Spectrum Disorder Diagnosis in a Clinical Sample of Children and Toddlers. Brain Sci. 2021, 11, 37. https://doi.org/10.3390/brainsci11010037
Benedetto L, Cucinotta F, Maggio R, Germanò E, De Raco R, Alquino A, Impallomeni C, Siracusano R, Vetri L, Roccella M, et al. One-Year Follow-Up Diagnostic Stability of Autism Spectrum Disorder Diagnosis in a Clinical Sample of Children and Toddlers. Brain Sciences. 2021; 11(1):37. https://doi.org/10.3390/brainsci11010037
Chicago/Turabian StyleBenedetto, Loredana, Francesca Cucinotta, Roberta Maggio, Eva Germanò, Roberta De Raco, Ausilia Alquino, Caterina Impallomeni, Rosamaria Siracusano, Luigi Vetri, Michele Roccella, and et al. 2021. "One-Year Follow-Up Diagnostic Stability of Autism Spectrum Disorder Diagnosis in a Clinical Sample of Children and Toddlers" Brain Sciences 11, no. 1: 37. https://doi.org/10.3390/brainsci11010037
APA StyleBenedetto, L., Cucinotta, F., Maggio, R., Germanò, E., De Raco, R., Alquino, A., Impallomeni, C., Siracusano, R., Vetri, L., Roccella, M., Ingrassia, M., & Gagliano, A. (2021). One-Year Follow-Up Diagnostic Stability of Autism Spectrum Disorder Diagnosis in a Clinical Sample of Children and Toddlers. Brain Sciences, 11(1), 37. https://doi.org/10.3390/brainsci11010037