
Early Schizophrenia and Bipolar Disorder Patients Display Reduced Neural Prepulse Inhibition

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Clinical Assessment
2.3. Prepulse Inhibition Test Session
2.4. Data Processing
2.4.1. Preprocessing
2.4.2. EMG and EEG Processing
2.5. Statistical Analysis
3. Results
3.1. Demographic and Clinical Data
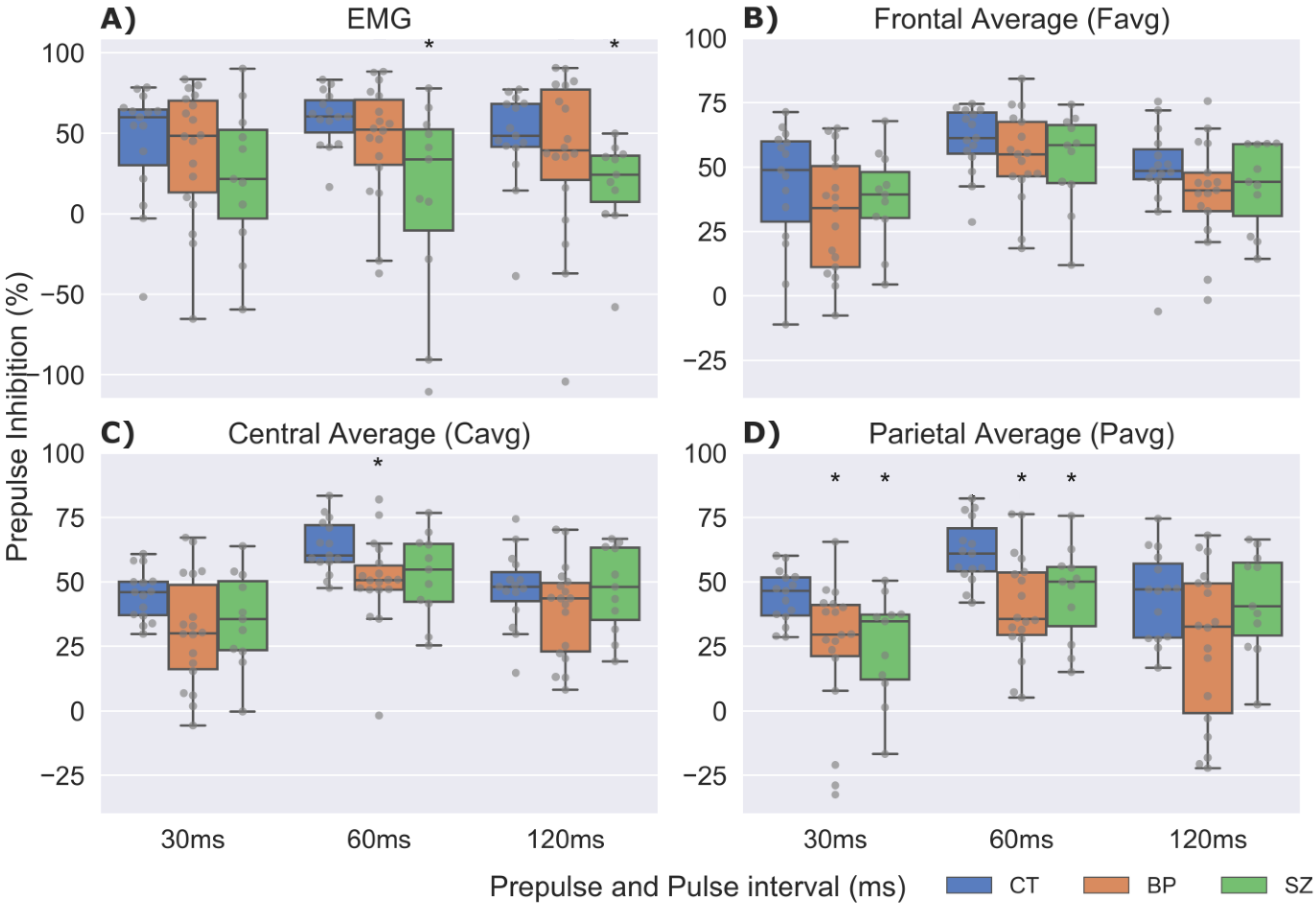
3.2. Prepulse Inhibition
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Van Os, J.; Kapur, S. Schizophrenia. Lancet 2009, 374, 635–645. [Google Scholar] [CrossRef]
- Yalincetin, B.; Bora, E.; Binbay, T.; Ulas, H.; Akdede, B.B.; Alptekin, K. Formal thought disorder in schizophrenia and bipolar disorder: A systematic review and meta-analysis. Schizophr. Res. 2017, 185, 2–8. [Google Scholar] [CrossRef]
- Craddock, N.; Owen, M.J. The beginning of the end for the Kraepelinian dichotomy. Br. J. Psychiatry 2005, 186, 364–366. [Google Scholar] [CrossRef] [Green Version]
- Dominguez, M.D.G.; Viechtbauer, W.; Simons, C.J.P.; van Os, J.; Krabbendam, L. Are psychotic psychopathology and neurocognition orthogonal? A systematic review of their associations. Psychol. Bull. 2009, 135, 157–171. [Google Scholar] [CrossRef] [PubMed]
- Rosen, C.; Marvin, R.; Reilly, J.L.; DeLeon, O.; Harris, M.S.; Keedy, S.K.; Solari, H.; Weiden, P.; Sweeney, J.A. Phenomenology of First-Episode Psychosis in Schizophrenia, Bipolar Disorder, and Unipolar Depression: A comparative analysis. Clin. Schizophr. Relat. Psychoses 2012, 6, 145A–151A. [Google Scholar] [CrossRef]
- Maier, W.; Zobel, A.; Wagner, M. Schizophrenia and bipolar disorder: Differences and overlaps. Curr. Opin. Psychiatry 2006, 19, 165–170. [Google Scholar] [CrossRef] [PubMed]
- Kraepelin, E. Dementia Praecox and Paraphrenia; Krieger Publishing Company: Huntington, NY, USA, 1971. [Google Scholar]
- Berrettini, W.H. Are schizophrenic and bipolar disorders related? A review of family and molecular studies. Biol. Psychiatry 2000, 48, 531–538. [Google Scholar] [CrossRef]
- Tohen, M.; Sanger, T.M.; McElroy, S.L.; Tollefson, G.D.; Chengappa, K.N.; Daniel, D.G.; Petty, F.; Centorrino, F.; Wang, R.; Grundy, S.L.; et al. Olanzapine versus placebo in the treatment of acute mania. Olanzapine HGEH Study Group. Am. J. Psychiatry 1999, 156, 702–709. [Google Scholar] [CrossRef]
- Sachs, G.S.; Grossman, F.; Ghaemi, S.N.; Okamoto, A.; Bowden, C.L. Combination of a Mood Stabilizer With Risperidone or Haloperidol for Treatment of Acute Mania: A Double-Blind, Placebo-Controlled Comparison of Efficacy and Safety. Am. J. Psychiatry 2002, 159, 1146–1154. [Google Scholar] [CrossRef]
- Lichtenstein, P.; Yip, B.H.; Björk, C.; Pawitan, Y.; Cannon, T.D.; Sullivan, P.F.; Hultman, C.M. Common genetic influences for schizophrenia and bipolar disorder: A population-based study of 2 million nuclear families. Lancet 2009, 373, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Craddock, N.; O’Donovan, M.C.; Owen, M.J. The genetics of schizophrenia and bipolar disorder: Dissecting psychosis. J. Med. Genet. 2005, 42, 193–204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bora, E.; Yucel, M.; Pantelis, C. Cognitive Impairment in Affective Psychoses: A Meta-analysis. Schizophr. Bull. 2009, 36, 112–125. [Google Scholar] [CrossRef] [Green Version]
- Hill, S.K.; Reilly, J.L.; Keefe, R.S.; Gold, J.M.; Bishop, J.R.; Gershon, E.S.; Tamminga, C.A.; Pearlson, G.D.; Keshavan, M.S.; Sweeney, J.A. Neuropsychological Impairments in Schizophrenia and Psychotic Bipolar Disorder: Findings from the Bipolar-Schizophrenia Network on Intermediate Phenotypes (B-SNIP) Study. Am. J. Psychiatry 2013, 170, 1275–1284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Demjaha, A.; MacCabe, J.H.; Murray, R. How Genes and Environmental Factors Determine the Different Neurodevelopmental Trajectories of Schizophrenia and Bipolar Disorder. Schizophr. Bull. 2011, 38, 209–214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trotta, A.; Murray, R.; MacCabe, J.H. Do premorbid and post-onset cognitive functioning differ between schizophrenia and bipolar disorder? A systematic review and meta-analysis. Psychol. Med. 2014, 45, 381–394. [Google Scholar] [CrossRef] [PubMed]
- Johansson, V.; Hultman, C.M.; Kizling, I.; Martinsson, L.; Borg, J.; Hedman, A.; Cannon, T.D. The schizophrenia and bipolar twin study in Sweden (STAR). Schizophr. Res. 2019, 204, 183–192. [Google Scholar] [CrossRef]
- Domján, N.; Csifcsák, G.; Drótos, G.; Janka, Z.; Szendi, I. Different patterns of auditory information processing deficits in chronic schizophrenia and bipolar disorder with psychotic features. Schizophr. Res. 2012, 139, 253–259. [Google Scholar] [CrossRef]
- Geyer, M.A.; Krebs-Thomson, K.; Braff, D.L.; Swerdlow, N.R. Pharmacological studies of prepulse inhibition models of sensorimotor gating deficits in schizophrenia: A decade in review. Psychopharmacologia 2001, 156, 117–154. [Google Scholar] [CrossRef]
- Swerdlow, N.R.; Braff, D.L.; Geyer, M.A. Sensorimotor gating of the startle reflex: What we said 25 years ago, what has happened since then, and what comes next. J. Psychopharmacol. 2016, 30, 1072–1081. [Google Scholar] [CrossRef]
- Braff, D.L.; Geyer, M.A.; Swerdlow, N.R. Human studies of prepulse inhibition of startle: Normal subjects, patient groups, and pharmacological studies. Psychopharmacologia 2001, 156, 234–258. [Google Scholar] [CrossRef]
- Swerdlow, N.R.; Light, G.A.; Thomas, M.L.; Sprock, J.; Calkins, M.E.; Green, M.F.; Greenwood, T.A.; Gur, R.E.; Gur, R.C.; Lazzeroni, L.; et al. Deficient prepulse inhibition in schizophrenia in a multi-site cohort: Internal replication and extension. Schizophr. Res. 2018, 198, 6–15. [Google Scholar] [CrossRef] [Green Version]
- Turetsky, B.I.; Calkins, M.E.; Light, G.A.; Olincy, A.; Radant, A.D.; Swerdlow, N.R. Neurophysiological Endophenotypes of Schizophrenia: The Viability of Selected Candidate Measures. Schizophr. Bull. 2007, 33, 69–94. [Google Scholar] [CrossRef] [Green Version]
- Koch, M. The neurobiology of startle. Prog. Neurobiol. 1999, 59, 107–128. [Google Scholar] [CrossRef]
- Fendt, M.; Li, L.; Yeomans, J.S. Brain stem circuits mediating prepulse inhibition of the startle reflex. Psychopharmacology 2001, 156, 216–224. [Google Scholar] [CrossRef]
- Swerdlow, N.R.; Geyer, M.A.; Braff, D.L. Neural circuit regulation of prepulse inhibition of startle in the rat: Current knowledge and future challenges. Psychopharmacology 2001, 156, 194–215. [Google Scholar] [CrossRef]
- Swerdlow, N.R.; Light, G.A. Sensorimotor gating deficits in schizophrenia: Advancing our understanding of the phenotype, its neural circuitry and genetic substrates. Schizophr. Res. 2018, 198, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braff, D.L.; Geyer, M.A.; Light, G.A.; Sprock, J.; Perry, W.; Cadenhead, K.S.; Swerdlow, N.R. Impact of prepulse characteristics on the detection of sensorimotor gating deficits in schizophrenia. Schizophr. Res. 2001, 49, 171–178. [Google Scholar] [CrossRef]
- Hammer, T.B.; Oranje, B.; Fagerlund, B.; Bro, H.; Glenthøj, B.Y. Stability of prepulse inhibition and habituation of the startle reflex in schizophrenia: A 6-year follow-up study of initially antipsychotic-naive, first-episode schizophrenia patients. Int. J. Neuropsychopharmacol. 2011, 14, 913–925. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumari, V.; Fannon, D.; Geyer, M.A.; Premkumar, P.; Antonova, E.; Simmons, A.; Kuipers, E. Cortical grey matter volume and sensorimotor gating in schizophrenia. Cortex 2008, 44, 1206–1214. [Google Scholar] [CrossRef] [Green Version]
- Mackeprang, T.; Kristiansen, K.T.; Glenthoj, B.Y. Effects of antipsychotics on prepulse inhibition of the startle response in drug-naïve schizophrenic patients. Biol. Psychiatry 2002, 52, 863–873. [Google Scholar] [CrossRef]
- San-Martin, R.; Castro, L.A.; Menezes, P.R.; Fraga, F.; Simões, P.W.; Salum, C. Meta-Analysis of Sensorimotor Gating Deficits in Patients with Schizophrenia Evaluated by Prepulse Inhibition Test. Schizophr. Bull. 2020, 46, 1482–1497. [Google Scholar] [CrossRef]
- Matsuo, J.; Ota, M.; Hidese, S.; Teraishi, T.; Hori, H.; Ishida, I.; Hiraishi, M.; Kunugi, H. Sensorimotor Gating in Depressed and Euthymic Patients with Bipolar Disorder: Analysis on Prepulse Inhibition of Acoustic Startle Response Stratified by Gender and State. Front. Psychiatry 2018, 9, 123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sánchez-Morla, E.M.; Mateo, J.; Aparicio, A.; García-Jiménez, M.; Jiménez, E.; Santos, J.L. Prepulse inhibition in euthymic bipolar disorder patients in comparison with control subjects. Acta Psychiatr. Scand. 2016, 134, 350–359. [Google Scholar] [CrossRef] [PubMed]
- Perry, W.; Minassian, A.; Feifel, D.; Braff, D.L. Sensorimotor gating deficits in bipolar disorder patients with acute psychotic mania. Biol. Psychiatry 2001, 50, 418–424. [Google Scholar] [CrossRef]
- Mao, Z.; Bo, Q.; Li, W.; Wang, Z.; Ma, X.; Wang, C. Prepulse inhibition in patients with bipolar disorder: A systematic review and meta-analysis. BMC Psychiatry 2019, 19, 282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swerdlow, N.R.; Light, G.A.; Sprock, J.; Calkins, M.E.; Green, M.F.; Greenwood, T.; Gur, R.E.; Gur, R.C.; Lazzeroni, L.; Nuechterlein, K.H.; et al. Deficient prepulse inhibition in schizophrenia detected by the multi-site COGS. Schizophr. Res. 2014, 152, 503–512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quednow, B.B.; Wagner, M.; Westheide, J.; Beckmann, K.; Bliesener, N.; Maier, W.; Kühn, K.-U. Sensorimotor Gating and Habituation of the Startle Response in Schizophrenic Patients Randomly Treated with Amisulpride or Olanzapine. Biol. Psychiatry 2006, 59, 536–545. [Google Scholar] [CrossRef]
- Woznica, A.A.; Sacco, K.A.; George, T.P. Prepulse inhibition deficits in schizophrenia are modified by smoking status. Schizophr. Res. 2009, 112, 86–90. [Google Scholar] [CrossRef]
- Morales-Muñoz, I.; Jurado-Barba, R.; Fernández-Guinea, S.; Rodríguez-Jiménez, R.; Jiménez-Arriero, M.; Criado, J.R.; Rubio, G. Sensory Gating Deficits in First-Episode Psychosis. J. Nerv. Ment. Dis. 2016, 204, 877–884. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Gras, I.; Rubio, G.; del Manzano, B.A.; Rodríguez-Jiménez, R.; Garcia-Sanchez, F.; Bagney, A.; Leza, J.C.; Borrell, J. The relationship between prepulse inhibition and general psychopathology in patients with schizophrenia treated with long-acting risperidone. Schizophr. Res. 2009, 115, 215–221. [Google Scholar] [CrossRef]
- Earls, H.A.; Curran, T.; Mittal, V. A Meta-analytic Review of Auditory Event-Related Potential Components as Endophenotypes for Schizophrenia: Perspectives From First-Degree Relatives. Schizophr. Bull. 2016, 42, 1504–1516. [Google Scholar] [CrossRef] [PubMed]
- Bramon, E.; Rabe-Hesketh, S.; Sham, P.; Murray, R.M.; Frangou, S. Meta-analysis of the P300 and P50 waveforms in schizophrenia. Schizophr. Res. 2004, 70, 315–329. [Google Scholar] [CrossRef] [PubMed]
- De Wilde, O.; Bour, L.; Dingemans, P.; Koelman, J.; Linszen, D. A meta-analysis of P50 studies in patients with schizophrenia and relatives: Differences in methodology between research groups. Schizophr. Res. 2007, 97, 137–151. [Google Scholar] [CrossRef]
- Cheng, C.-H.; Chan, P.-Y.S.; Liu, C.-Y.; Hsu, S.-C. Auditory sensory gating in patients with bipolar disorders: A meta-analysis. J. Affect. Disord. 2016, 203, 199–203. [Google Scholar] [CrossRef] [PubMed]
- Erickson, M.A.; Ruffle, A.; Gold, J.M. A Meta-Analysis of Mismatch Negativity in Schizophrenia: From Clinical Risk to Disease Specificity and Progression. Biol. Psychiatry 2016, 79, 980–987. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Umbricht, D.; Krljes, S. Mismatch negativity in schizophrenia: A meta-analysis. Schizophr. Res. 2005, 76, 1–23. [Google Scholar] [CrossRef]
- Jeon, Y.-W.; Polich, J. Meta-analysis of P300 and schizophrenia: Patients, paradigms, and practical implications. Psychophysiology 2003, 40, 684–701. [Google Scholar] [CrossRef]
- Bestelmeyer, P.E.; Phillips, L.H.; Crombie, C.; Benson, P.; St. Clair, D. The P300 as a possible endophenotype for schizophrenia and bipolar disorder: Evidence from twin and patient studies. Psychiatry Res. 2009, 169, 212–219. [Google Scholar] [CrossRef]
- Hall, M.-H.; Schulze, K.; Rijsdijk, F.; Kalidindi, S.; McDonald, C.; Bramon, E.; Murray, R.; Sham, P. Are auditory P300 and duration MMN heritable and putative endophenotypes of psychotic bipolar disorder? A Maudsley Bipolar Twin and Family Study. Psychol. Med. 2009, 39, 1277–1287. [Google Scholar] [CrossRef]
- O’Donnell, B.; Vohs, J.; Hetrick, W.; Carroll, C.; Shekhar, A. Auditory event-related potential abnormalities in bipolar disorder and schizophrenia. Int. J. Psychophysiol. 2004, 53, 45–55. [Google Scholar] [CrossRef]
- San-Martin, R.; Zimiani, M.I.; Noya, C.; Ávila, M.A.V.; Shuhama, R.; Del-Ben, C.M.; Menezes, P.R.; Fraga, F.; Salum, C. A Method for Simultaneous Evaluation of Muscular and Neural Prepulse Inhibition. Front. Neurosci. 2018, 12, 654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Z.-R.; Tan, Y.-L.; Yang, F.-D.; Zhang, W.-F.; Zou, Y.-Z.; Tan, S.-P.; Song, C.-S.; Li, Y.-L.; Zhang, W.-H.; Zhou, D.-F. Impaired prepulse inhibition of acoustic startle in Chinese patients with first-episode, medication-naïve schizophrenia. Chin. Med. J. 2013, 126, 526–531. [Google Scholar]
- Xue, Y.-Y.; Wang, H.-N.; Xue, F.; Tan, Q.-R. Atypical Antipsychotics Do Not Reverse Prepulse Inhibition Deficits in Acutely Psychotic Schizophrenia. J. Int. Med. Res. 2012, 40, 1467–1475. [Google Scholar] [CrossRef] [Green Version]
- Light, G.A.; Swerdlow, N.R.; Rissling, A.J.; Radant, A.; Sugar, C.A.; Sprock, J.; Pela, M.; Geyer, M.A.; Braff, D.L. Characterization of Neurophysiologic and Neurocognitive Biomarkers for Use in Genomic and Clinical Outcome Studies of Schizophrenia. PLoS ONE 2012, 7, e39434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meincke, U.; Mörth, D.; Voß, T.; Thelen, B.; Geyer, M.A.; Gouzoulis-Mayfrank, E.; Voss, T. Prepulse inhibition of the acoustically evoked startle reflex in patients with an acute schizophrenic psychosis—A longitudinal study. Eur. Arch. Psychiatry Clin. Neurosci. 2004, 254, 415–421. [Google Scholar] [CrossRef]
- Carroll, C.A.; Vohs, J.L.; O’Donnell, B.F.; Shekhar, A.; Hetrick, W.P. Sensorimotor gating in manic and mixed episode bipolar disorder. Bipolar Disord. 2007, 9, 221–229. [Google Scholar] [CrossRef]
- Kedzior, K.K.; Koch, M.; Basar-Eroglu, C. Auditory-evoked EEG oscillations associated with prepulse inhibition (PPI) of auditory startle reflex in healthy humans. Brain Res. 2007, 1163, 111–118. [Google Scholar] [CrossRef] [PubMed]
- Koch, M.; Schmiedt-Fehr, C.; Mathes, B. Neuropharmacology of altered brain oscillations in schizophrenia. Int. J. Psychophysiol. 2016, 103, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Jongsma, H.; Gayer-Anderson, C.; Lasalvia, A.; Quattrone, D.; Mulè, A.; Szoke, A.; Selten, J.-P.; Turner, C.; Arango, C.; Tarricone, I.; et al. Treated Incidence of Psychotic Disorders in the Multinational EU-GEI Study. JAMA Psychiatry 2018, 75, 36–46. [Google Scholar] [CrossRef]
- Di Forti, M.; Quattrone, D.; Freeman, T.P.; Tripoli, G.; Gayer-Anderson, C.; Quigley, H.; Rodriguez, V.; Jongsma, H.E.; Ferraro, L.; La Cascia, C.; et al. The contribution of cannabis use to variation in the incidence of psychotic disorder across Europe (EU-GEI): A multicentre case-control study. Lancet Psychiatry 2019, 6, 427–436. [Google Scholar] [CrossRef] [Green Version]
- Del-Ben, C.M.; Shuhama, R.; Loureiro, C.M.; Ragazzi, T.C.C.; Zanatta, D.P.; Tenan, S.H.G.; Santos, J.L.F.; Louzada-Junior, P.; Dos Santos, A.C.; Morgan, C.; et al. Urbanicity and risk of first-episode psychosis: Incidence study in Brazil. Br. J. Psychiatry 2019, 215, 726–729. [Google Scholar] [CrossRef]
- Overall, J.E.; Gorham, D.R. The brief psychiatric rating scale. Psychol. Rep. 1962, 10, 799–812. [Google Scholar] [CrossRef]
- Hamilton, M. A rating scale for depression. J. Neurol. Neurosurg. Psychiatry 1960, 23, 56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Young, R.C.; Biggs, J.T.; Ziegler, V.E.; Meyer, D.A. A Rating Scale for Mania: Reliability, Validity and Sensitivity. Br. J. Psychiatry 1978, 133, 429–435. [Google Scholar] [CrossRef] [PubMed]
- Vilela, J.; Crippa, J.; Del-Ben, C.M.; Loureiro, S. Reliability and validity of a Portuguese version of the Young Mania Rating Scale. Braz. J. Med Biol. Res. 2005, 38, 1429–1439. [Google Scholar] [CrossRef]
- Oldfield, R.C. The assessment and analysis of handedness: The Edinburgh inventory. Neuropsychologia 1971, 9, 97–113. [Google Scholar] [CrossRef]
- Braff, D.L.; Light, G.A.; Ellwanger, J.; Sprock, J.; Swerdlow, N.R. Female schizophrenia patients have prepulse inhibition deficits. Biol. Psychiatry 2005, 57, 817–820. [Google Scholar] [CrossRef] [PubMed]
- Oranje, B.; Glenthøj, B. Clonidine Normalizes Sensorimotor Gating Deficits in Patients with Schizophrenia on Stable Medication. Schizophr. Bull. 2012, 39, 684–691. [Google Scholar] [CrossRef] [Green Version]
- Fraga, F.J.; Noya, C.V.; Zimiani, M.I.; Avila, M.A.; Shuhama, R.; Del-Ben, C.M.; Menezes, P.R.; Martin, R.S.; Salum, C. Simultaneous evaluation of prepulse inhibition with EMG and EEG using advanced artifact removal techniques. In Proceedings of the 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Orlando, FL, USA, 16–20 August 2016; pp. 5262–5265. [Google Scholar] [CrossRef]
- Delorme, A.; Makeig, S. EEGLAB: An Open Source Toolbox for Analysis of Single-Trial EEG Dynamics Including Independent Component Analysis. J. Neurosci. Methods 2004, 134, 9–21. [Google Scholar] [CrossRef] [Green Version]
- Chaumon, M.; Bishop, D.V.; Busch, N.A. A practical guide to the selection of independent components of the electroencephalogram for artifact correction. J. Neurosci. Methods 2015, 250, 47–63. [Google Scholar] [CrossRef]
- Blumenthal, T.D.; Cuthbert, B.N.; Filion, D.L.; Hackley, S.; Lipp, O.; van Boxtel, A. Committee report: Guidelines for human startle eyeblink electromyographic studies. Psychophysiology 2005, 42, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Boxtel, A.; Boelhouwer, A.; Bos, A. Optimal EMG signal bandwidth and interelectrode distance for the recording of acoustic, electrocutaneous, and photic blink reflexes. Psychophysiology 1998, 35, 690–697. [Google Scholar] [CrossRef]
- Delorme, A.; Sejnowski, T.; Makeig, S. Enhanced detection of artifacts in EEG data using higher-order statistics and independent component analysis. NeuroImage 2006, 34, 1443–1449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kedzior, K.K.; Martin-Iverson, M.T. Attention-dependent reduction in prepulse inhibition of the startle reflex in cannabis users and schizophrenia patients—A pilot study. Eur. J. Pharmacol. 2007, 560, 176–182. [Google Scholar] [CrossRef]
- Abduljawad, K.A.J.; Langley, R.W.; Bradshaw, C.M.; Szabadi, E. Effects of clonidine and diazepan on ppi N1/P2. J. Psychopharmacol. 2001, 14, 258–265. [Google Scholar]
- Sommer, K.; Van Der Molen, M.W.; De Pascalis, V. BIS/BAS sensitivity and emotional modulation in a prepulse-inhibition paradigm: A brain potential study. Physiol. Behav. 2016, 154, 100–113. [Google Scholar] [CrossRef]
- Ziermans, T.B.; Schothorst, P.F.; Sprong, M.; Magnée, M.J.; van Engeland, H.; Kemner, C. Reduced prepulse inhibition as an early vulnerability marker of the psychosis prodrome in adolescence. Schizophr. Res. 2012, 134, 10–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2013. [Google Scholar]
- Ludewig, K.; Geyer, M.A.; Etzensberger, M.; Vollenweider, F.X. Stability of the acoustic startle reflex, prepulse inhibition, and habituation in schizophrenia. Schizophr. Res. 2002, 55, 129–137. [Google Scholar] [CrossRef]
- Shi, J.; Wang, Z.; Tan, Y.; Fan, H.; An, H.; Zuo, L.; Yang, F.; Tan, S.; Li, J.; Zhang, X.; et al. CHRNA4was associated with prepulse inhibition of schizophrenia in Chinese: A pilot study. Cogn. Neuropsychiatry 2016, 21, 156–167. [Google Scholar] [CrossRef]
- Kunugi, H.; Tanaka, M.; Hori, H.; Hashimoto, R.; Saitoh, O.; Hironaka, N. Prepulse inhibition of acoustic startle in Japanese patients with chronic schizophrenia. Neurosci. Res. 2007, 59, 23–28. [Google Scholar] [CrossRef]
- Perry, W.; Minassian, A.; Feifel, D. Prepulse inhibition in patients with non-psychotic major depressive disorder. J. Affect. Disord. 2004, 81, 179–184. [Google Scholar] [CrossRef]
- Rubio, G.; López-Muñoz, F.; Barba, R.J.; Martínez-Gras, I.; Rodríguez-Jiménez, R.; Espinosa, R.; Nieto, M.P.; Moratti, S.; Jiménez-Arriero, M.; Leza, J.C. Stress induced by the socially evaluated cold-pressor test cause equivalent deficiencies of sensory gating in male subjects with schizophrenia and healthy controls. Psychiatry Res. 2015, 228, 283–288. [Google Scholar] [CrossRef]
- Fargotstein, M.; Hasenkamp, W.; Gross, R.; Cuthbert, B.; Green, A.; Swails, L.; Lewison, B.; Boshoven, W.; Keyes, M.; Duncan, E. The effect of antipsychotic medications on acoustic startle latency in schizophrenia. Schizophr. Res. 2018, 198, 28–35. [Google Scholar] [CrossRef]
- Bertelsen, B.; Oranje, B.; Melchior, L.; Fagerlund, B.; Werge, T.M.; Mikkelsen, J.D.; Tümer, Z.; Glenthøj, B. Association Study of CHRNA7 Promoter Variants with Sensory and Sensorimotor Gating in Schizophrenia Patients and Healthy Controls: A Danish Case–Control Study. NeuroMolecular Med. 2015, 17, 423–430. [Google Scholar] [CrossRef]
- Huotilainen, M.; Winkler, I.; Alho, K.; Escera, C.; Virtanen, J.; Ilmoniemi, R.; Jääskeläinen, I.P.; Pekkonen, E.; Näätänen, R. Combined mapping of human auditory EEG and MEG responses. Electroencephalogr. Clin. Neurophysiol. Potentials Sect. 1998, 108, 370–379. [Google Scholar] [CrossRef]
- Joos, K.; Gilles, A.; Van de Heyning, P.; De Ridder, D.; Vanneste, S. From sensation to percept: The neural signature of auditory event-related potentials. Neurosci. Biobehav. Rev. 2014, 42, 148–156. [Google Scholar] [CrossRef] [PubMed]
- Inui, K.; Nakagawa, K.; Nishihara, M.; Motomura, E.; Kakigi, R. Inhibition in the Human Auditory Cortex. PLoS ONE 2016, 11, e0155972. [Google Scholar] [CrossRef] [PubMed]
- Inui, K.; Tsuruhara, A.; Nakagawa, K.; Nishihara, M.; Kodaira, M.; Motomura, E.; Kakigi, R. Prepulse inhibition of change-related P50m no correlation with P50m gating. SpringerPlus 2013, 2, 588. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Pascalis, V.; Russo, E. Hypnotizability, Hypnosis and Prepulse Inhibition of the Startle Reflex in Healthy Women: An ERP Analysis. PLoS ONE 2013, 8, e79605. [Google Scholar] [CrossRef] [Green Version]
- Pascual-Marqui, R.D.; Michel, C.; Lehmann, D. Low resolution electromagnetic tomography: A new method for localizing electrical activity in the brain. Int. J. Psychophysiol. 1994, 18, 49–65. [Google Scholar] [CrossRef]
- Storozheva, Z.I.; Kirenskaya, A.; Novototsky-Vlasov, V.Y.; Telesheva, K.Y.; Pletnikov, M. Startle Modification and P50 Gating in Schizophrenia Patients and Controls: Russian Population. Span. J. Psychol. 2016, 19, E8. [Google Scholar] [CrossRef]
- Swerdlow, N.R.; Weber, M.; Qu, Y.; Light, G.A.; Braff, D.L. Realistic Expectations of Prepulse Inhibition in Translational Models for Schizophrenia Research. Psychopharmacology 2008, 199, 331–388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cassani, R.; Estarellas, M.; San-Martin, R.; Fraga, F.J.; Falk, T.H. Systematic Review on Resting-State EEG for Alzheimer’s Disease Diagnosis and Progression Assessment. Dis. Markers 2018, 2018, 5147815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ianof, J.N.; Fraga, F.J.; Ferreira, L.A.; Ramos, R.T.; Demario, J.L.C.; Baratho, R.; Basile, L.F.H.; Nitrini, R.; Anghinah, R. Comparative analysis of the electroencephalogram in patients with Alzheimer’s disease, diffuse axonal injury patients and healthy controls using LORETA analysis. Dement. Neuropsychol. 2017, 11, 176–185. [Google Scholar] [CrossRef]
- Hejl, A.-M.; Glenthøj, B.; Mackeprang, T.; Hemmingsen, R.; Waldemar, G. Prepulse inhibition in patients with Alzheimer’s disease. Neurobiol. Aging 2004, 25, 1045–1050. [Google Scholar] [CrossRef]
- Giakoumaki, S.G.; Roussos, P.; Rogdaki, M.; Karli, C.; Bitsios, P.; Frangou, S. Evidence of Disrupted Prepulse Inhibition in Unaffected Siblings of Bipolar Disorder Patients. Biol. Psychiatry 2007, 62, 1418–1422. [Google Scholar] [CrossRef]
- Aggernaes, B.; Glenthoj, B.Y.; Ebdrup, B.H.; Rasmussen, H.; Lublin, H.; Oranje, B. Sensorimotor gating and habituation in antipsychotic-naive, first-episode schizophrenia patients before and after 6 months’ treatment with quetiapine. Int. J. Neuropsychopharmacol. 2010, 13, 1383–1395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Storozheva, Z.I.; Kirenskaya, A.V.; Lazarev, I.E.; Novototskii-Vlasov, V.Y.; Samylkin, D.V.; Fastovtsov, G.A. Prepulse Modification of the Acoustic Startle Reaction in Healthy Subjects and Patients with Schizophrenia. Neurosci. Behav. Physiol. 2012, 42, 128–132. [Google Scholar] [CrossRef]
- Takahashi, H.; Iwase, M.; Ishii, R.; Ohi, K.; Fukumoto, M.; Azechi, M.; Ikezawa, K.; Kurimoto, R.; Canuet, L.; Nakahachi, T.; et al. Impaired prepulse inhibition and habituation of acoustic startle response in Japanese patients with schizophrenia. Neurosci. Res. 2008, 62, 187–194. [Google Scholar] [CrossRef]
- Swerdlow, N.R.; Light, G.A.; Cadenhead, K.S.; Sprock, J.; Hsieh, M.H.; Braff, D.L. Startle Gating Deficits in a Large Cohort of Patients with Schizophrenia. Arch. Gen. Psychiatry 2006, 63, 1325–1335. [Google Scholar] [CrossRef] [Green Version]
- Perry, W.; Feifel, D.; Minassian, A.; Bhattacharjie, I.; Braff, D.L. Information processing deficits in acutely psychotic schizophrenia patients medicated and unmedicated at the time of admission. Am. J. Psychiatry 2002, 159, 1375–1381. [Google Scholar] [CrossRef]
- Braff, D.L.; Swerdlow, N.R.; Geyer, M.A. Symptom correlates of prepulse inhibition deficits in male schizophrenic patients. Am. J. Psychiatry 1999, 156, 596–602. [Google Scholar] [CrossRef] [PubMed]
- Matsuo, J.; Ota, M.; Hori, H.; Hidese, S.; Teraishi, T.; Ishida, I.; Hiraishi, M.; Kunugi, H. A large single ethnicity study of prepulse inhibition in schizophrenia: Separate analysis by sex focusing on effect of symptoms. J. Psychiatr. Res. 2016, 82, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Cadenhead, K.S.; Light, G.A.; Geyer, M.A.; Braff, D.L. Sensory Gating Deficits Assessed by the P50 Event-Related Potential in Subjects with Schizotypal Personality Disorder. Am. J. Psychiatry 2000, 157, 55–59. [Google Scholar] [CrossRef] [PubMed]
- Boutros, N.N.; Korzyukov, O.; Jansen, B.; Feingold, A.; Bell, M. Sensory gating deficits during the mid-latency phase of information processing in medicated schizophrenia patients. Psychiatry Res. 2004, 126, 203–215. [Google Scholar] [CrossRef]
- Schächinger, H.; Müller, B.U.; Strobel, W.; Langewitz, W.; Ritz, R. Midazolam effects on prepulse inhibition of the acoustic blink reflex. Br. J. Clin. Pharmacol. 1999, 47, 421–426. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schizophrenia, F.-E.; Ludewig, K.; Geyer, M.A.; Vollenweider, F.X. Deficits in prepulse inhibition and habituation in never-medicated, first-episode schizophrenia. Biol. Psychiatry 2003, 54, 121–128. [Google Scholar] [CrossRef]
- Hammer, T.B.; Oranje, B.; Skimminge, A.; Aggernæs, B.; Ebdrup, B.H.; Glenthøj, B.; Baaré, W. Structural brain correlates of sensorimotor gating in antipsychotic-naive men with first-episode schizophrenia. J. Psychiatry Neurosci. 2013, 38, 34–42. [Google Scholar] [CrossRef] [Green Version]
- Kumari, V.; Aasen, I.; Sharma, T. Sex differences in prepulse inhibition deficits in chronic schizophrenia. Schizophr. Res. 2003, 69, 219–235. [Google Scholar] [CrossRef]
- Kumari, V.; Soni, W.; Sharma, T. Prepulse inhibition of the startle response in risperidone-treated patients: Comparison with typical antipsychotics. Schizophr. Res. 2002, 55, 139–146. [Google Scholar] [CrossRef]
- Greenwood, T.A.; Light, G.A.; Swerdlow, N.R.; Calkins, M.E.; Green, M.F.; Gur, R.E.; Gur, R.C.; Lazzeroni, L.C.; Nuechterlein, K.H.; Olincy, A.; et al. Gating Deficit Heritability and Correlation with Increased Clinical Severity in Schizophrenia Patients with Positive Family History. Am. J. Psychiatry 2016, 173, 385–391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Pascalis, V.; Cozzuto, G.; Russo, E. Effects of personality trait emotionality on acoustic startle response and prepulse inhibition including N100 and P200 event-related potential. Clin. Neurophysiol. 2013, 124, 292–305. [Google Scholar] [CrossRef]
- Moran, L.V.; Hong, L.E. High vs Low Frequency Neural Oscillations in Schizophrenia. Schizophr. Bull. 2011, 37, 659–663. [Google Scholar] [CrossRef] [PubMed]
- Oranje, B.; Geyer, M.A.; Bocker, K.B.; Kenemans, J.L.; Verbaten, M.N. Prepulse inhibition and P50 suppression: Commonalities and dissociations. Psychiatry Res. 2006, 143, 147–158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Erin, A.H.; Hazlett, E.A.; Buchsbaum, M.S. Sensorimotor gating deficits and hypofrontality in schizophrenia. Front. Biosci. 2001, 6, d1069–d1072. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Control (n = 15) | Bipolar (n = 18) | Schizophrenia (n = 11) | Test Types | Omnibus Statistic and Significance Pairwise Comparisons |
|---|---|---|---|---|---|
| Age at STREAM (years) | 26.8 ± 7.42 | 25.55 ± 6.87 | 27.36 ± 8.93 | a | F(2,41) = 0.22, n.s. |
| Education (years) | 12.5 ± 2.69 | 10.79 ± 2.48 | 10.02 ± 2.37 | a, t | F(2,41) = 3.39, p = 0.02; θ |
| Sex (m/f) | 9/6 | 10/8 | 8/3 | c | χ2(2, 41) = 0.87, n.s. |
| Age of onset (years) | - | 24.47 ± 6.84 | 25.65 ± 8.96 | b | t(17.10) = 0.38, n.s. |
| PPI test—treat. start (years) | - | 1.57 ± 0.8 | 1.84 ± 0.92 | b | t(19.01) = 0.81, n.s. |
| Edinburgh (score) | 17.26 ± 3.15 | 17.94 ± 2.33 | 17.54 ± 2.38 | d | k2(2) = 0.50, n.s. |
| BPRS STREAM (score) | 0.93 ± 2.84 | 9 ± 5.58 | 12.81 ± 6.86 | k, w | k2(2) = 24.61, p < 0.00001; θ, δ |
| BPRS at PPI test (score) | 1.93 ± 2.65 | 3.77 ± 7.05 | 7.45 ± 8.06 | k | k2(2) = 4.05, n.s. |
| Hamilton D at STREAM (score) | 1.86 ± 5.16 | 5.27 ± 6.02 | 9.18 ± 5.84 | k, w | k2(2) = 15.67, p < 0.001; θ, δ |
| Hamilton D at PPI test (score) | 1.93 ± 3.03 | 2.5 ± 3.09 | 6.27 ± 6.73 | k | k2(2) = 5.45, n.s. |
| YMRS at STREAM (score) | 0.53 ± 1.18 | 13.5 ± 10.18 | 5.18 ± 4.91 | k, w | k2(2) = 22.35, p < 0.001; θ, δ |
| YMRS at PPI test (score) | 0.53 ± 0.83 | 3.05 ± 5.77 | 2.9 ± 3.83 | k | k2(2) = 2.75, n.s. |
| Atypical antipsychotic (%) | - | 39% | 82% | c | χ2(1, 29) = 5.09, p = 0.05; β |
| Typical antipsychotic (%) | - | 6% | 18% | c | χ2(1, 29) = 1.17, n.s. |
| Humor stabilizer (%) | - | 61% | - | c | χ2(1, 29) = 10.83, p < 0.01; β |
| Benzodiazepines (%) | - | 22% | 45% | c | χ2(1, 29) = 1.72, n.s. |
| Electrode | Response | Control (n = 15) | Bipolar (n = 18) | Schizophrenia (n = 11) | Omnibus Statistic |
|---|---|---|---|---|---|
| EMG | P Amp (µV) | 2.23 | 1.87 | 3.04 | χ2(2) = 0.62, n.s. |
| %PPI30 | 60.05 | 48.49 | 21.61 | χ2(2) = 1.9, n.s. | |
| %PPI60 | 60.52 | 52.25 | 33.81 | χ2(2) = 6.71, p = 0.03 | |
| %PPI120 | 48.51 | 39.29 | 24.26 | χ2(2) = 6.81, p = 0.03 | |
| Favg | P Amp (μV) | 21.89 | 16.90 | 13.95 | χ2(2) = 2.94, n.s. |
| %PPI 30 | 48.89 | 34.14 | 39.36 | χ2(2) = 2.6, n.s. | |
| %PPI 60 | 61.36 | 54.90 | 58.55 | χ2(2) = 1.95, n.s. | |
| %PPI 120 | 48.52 | 41.01 | 44.28 | χ2(2) = 2.86, n.s. | |
| Cavg | P Amp (µV) | 25.26 | 20.97 | 19.47 | χ2(2) = 3.68, n.s. |
| %PPI 30 | 45.96 | 30.12 | 35.50 | χ2(2) = 5.11, n.s. | |
| %PPI 60 | 60.29 | 50.72 | 54.72 | χ2(2) = 7.46, p = 0.02 | |
| %PPI 120 | 48.14 | 43.58 | 48.06 | χ2(2) = 2.28, n.s. | |
| Pavg | P Amp (µV) | 19.70 | 14.79 | 13.65 | χ2(2) = 5.26, n.s. |
| %PPI 30 | 46.52 | 29.62 | 34.65 | χ2(2) = 9.45, p < 0.01 | |
| %PPI 60 | 61.00 | 35.55 | 50.15 | χ2(2) = 10.45, p < 0.01 | |
| %PPI 120 | 47.09 | 32.62 | 40.59 | χ2(2) = 3.29, n.s. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
San-Martin, R.; Zimiani, M.I.; de Ávila, M.A.V.; Shuhama, R.; Del-Ben, C.M.; Menezes, P.R.; Fraga, F.J.; Salum, C. Early Schizophrenia and Bipolar Disorder Patients Display Reduced Neural Prepulse Inhibition. Brain Sci. 2022, 12, 93. https://doi.org/10.3390/brainsci12010093
San-Martin R, Zimiani MI, de Ávila MAV, Shuhama R, Del-Ben CM, Menezes PR, Fraga FJ, Salum C. Early Schizophrenia and Bipolar Disorder Patients Display Reduced Neural Prepulse Inhibition. Brain Sciences. 2022; 12(1):93. https://doi.org/10.3390/brainsci12010093
Chicago/Turabian StyleSan-Martin, Rodrigo, Maria Inês Zimiani, Milton Augusto Vendramini de Ávila, Rosana Shuhama, Cristina Marta Del-Ben, Paulo Rossi Menezes, Francisco José Fraga, and Cristiane Salum. 2022. "Early Schizophrenia and Bipolar Disorder Patients Display Reduced Neural Prepulse Inhibition" Brain Sciences 12, no. 1: 93. https://doi.org/10.3390/brainsci12010093
APA StyleSan-Martin, R., Zimiani, M. I., de Ávila, M. A. V., Shuhama, R., Del-Ben, C. M., Menezes, P. R., Fraga, F. J., & Salum, C. (2022). Early Schizophrenia and Bipolar Disorder Patients Display Reduced Neural Prepulse Inhibition. Brain Sciences, 12(1), 93. https://doi.org/10.3390/brainsci12010093