
Oxidative and Nitrosative Stress in Major Depressive Disorder: A Case Control Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting and Selection Criteria for Participants
2.2. Procedure
2.3. Separation of Neutrophils and Plasma
2.4. Assessment of ROS Generation
2.5. Estimation of Neutrophil and Plasma Nitrites
2.6. Estimation of Neutrophil nNOS Expression
2.7. Estimation of Neutrophil MPO Activity
2.8. Estimation of the Cortisol Level
2.9. Statistical Analysis
3. Results
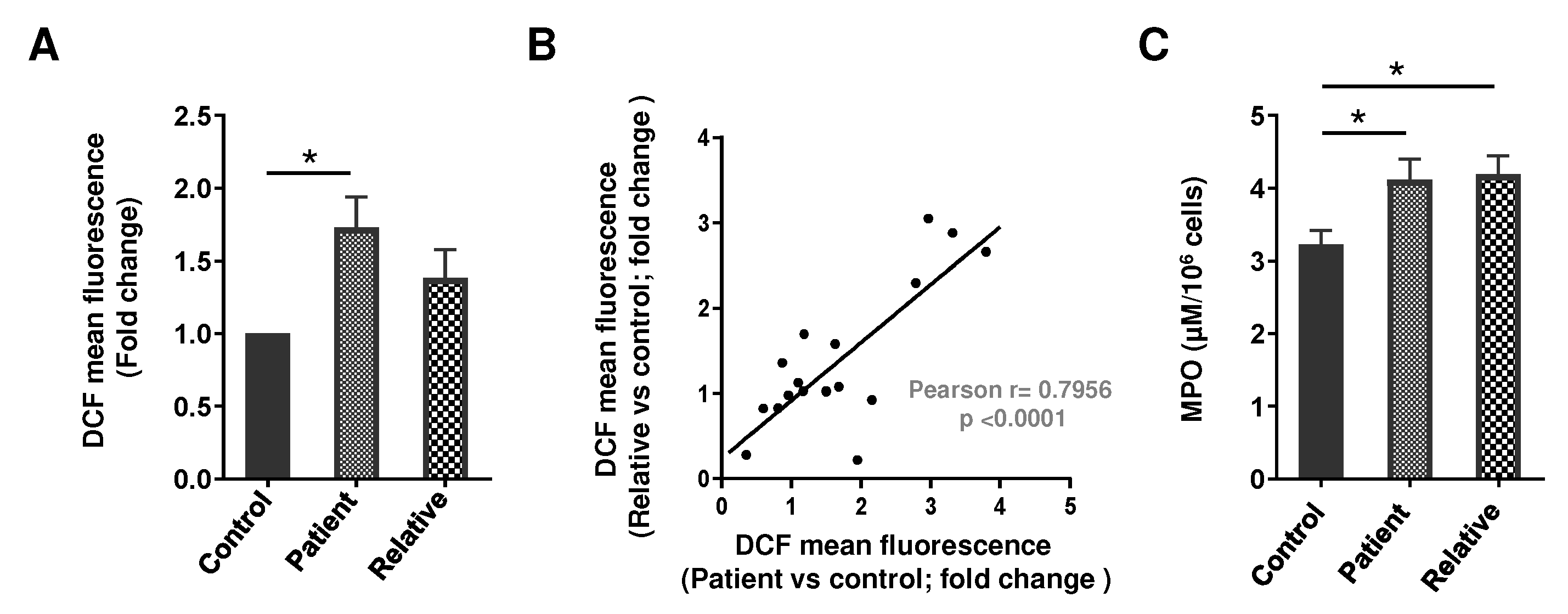
3.1. Oxidative Stress and MPO in the PMNs of Depression Patients and Their First-Degree Relatives
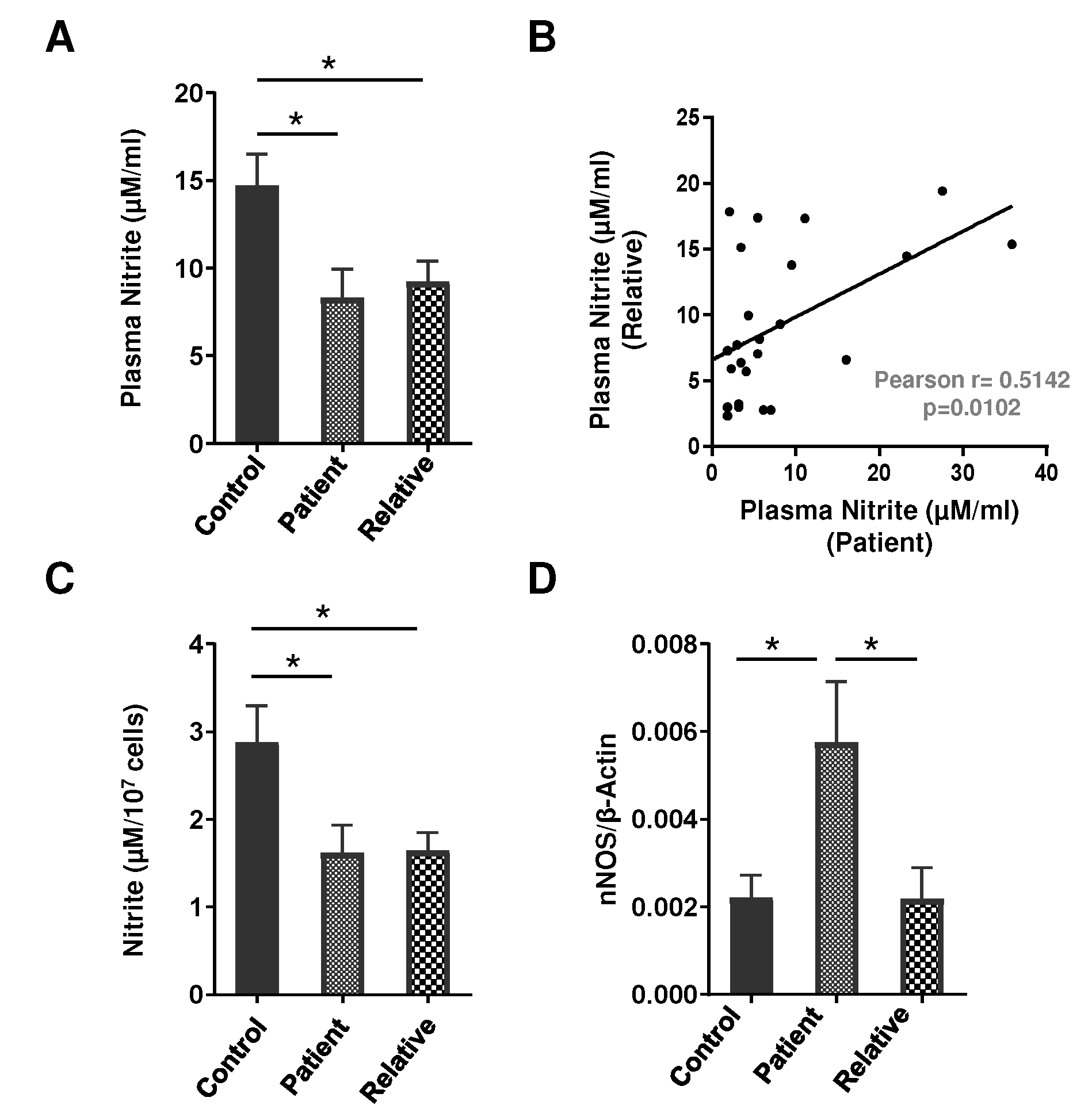
3.2. Nitrite Level and NOS Isoform Expression in the PMNs of Depression Patients and First-Degree Relatives
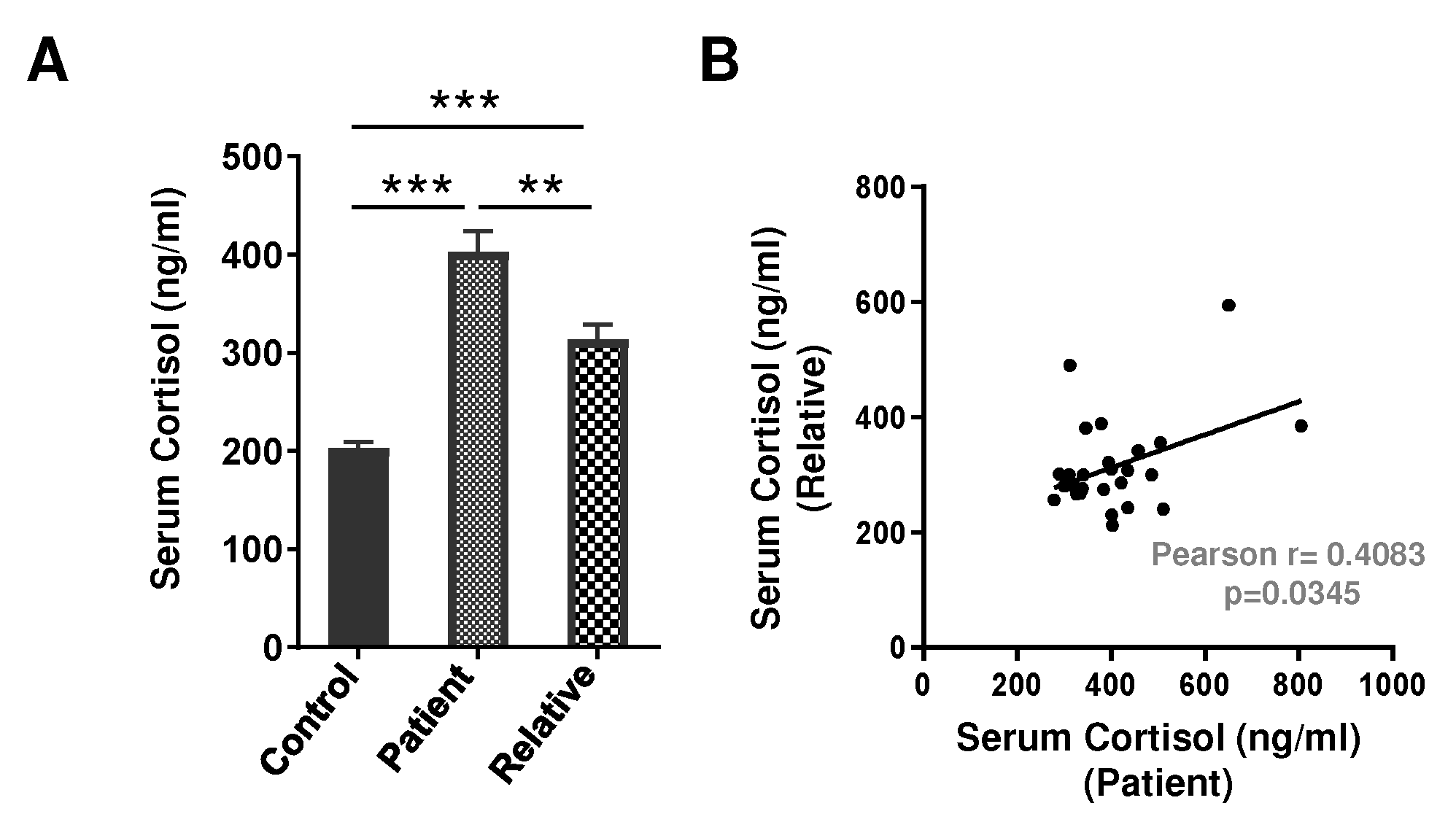
3.3. Serum Cortisol Level in Depression Patients and First-Degree Relatives
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Depression. 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/depression (accessed on 20 April 2021).
- Malhi, G.S.; Mann, J.J. Depression. Lancet 2018, 392, 2299–2312. [Google Scholar] [CrossRef]
- Sadock, B.; Sadock, V.; Ruiz, P. Depression and Bipolar Disorder. Kaplan & Sadock’s Synopsis of Psychiatry, 11th ed.; Wolters Kluwer: Philadelphia, PA, USA, 2015; pp. 752–830. [Google Scholar]
- Herken, H.; Gurel, A.; Selek, S.; Armutcu, F.; Ozen, M.E.; Bulut, M.; Kap, O.; Yumru, M.; Savas, H.A.; Akyol, O. Adenosine Deaminase, Nitric Oxide, Superoxide Dismutase, and Xanthine Oxidase in Patients with Major Depression: Impact of Antidepressant Treatment. Arch. Med. Res. 2007, 38, 247–252. [Google Scholar] [CrossRef]
- Maes, M.; Galecki, P.; Chang, Y.S.; Berk, M. A review on the oxidative and nitrosative stress (O&NS) pathways in major depression and their possible contribution to the (neuro)degenerative processes in that illness. Prog. Neuro Psychopharmacol. Biol. Psychiatry 2011, 35, 676–692. [Google Scholar] [CrossRef]
- Ozcan, M.E.; Gulec, M.; Ozerol, E.; Polat, R.; Akyol, O. Antioxidant enzyme activities and oxidative stress in affective disorders. Int. Clin. Psychopharmacol. 2004, 19, 89–95. [Google Scholar] [CrossRef]
- Srivastava, N.; Barthwal, M.K.; Dalal, P.K.; Agarwal, A.K.; Nag, D.; Seth, P.K.; Srimal, R.C.; Dikshit, M. A study on nitric oxide, beta-adrenergic receptors and antioxidant status in the polymorphonuclear leukocytes from the patients of depression. J. Affect. Disord. 2002, 72, 45–52. [Google Scholar] [CrossRef]
- Sarandol, A.; Sarandol, E.; Eker, S.S.; Erdinc, S.; Vatansever, E.; Kirli, S. Major depressive disorder is accompanied with oxidative stress: Short-term antidepressant treatment does not alter oxidative–antioxidative systems. Hum. Psychopharmacol. Clin. Exp. 2007, 22, 67–73. [Google Scholar] [CrossRef]
- Herken, H.; Akyol, O.; Yilmaz, H.R.; Tutkun, H.; Savaş, H.A.; Ozen, M.E.; Kalenderoglu, A.; Gulec, M.; Yılmaz, H.R. Nitric oxide, adenosine deaminase, xanthine oxidase and superoxide dismutase in patients with panic disorder: Alterations by antidepressant treatment. Hum. Psychopharmacol. Clin. Exp. 2006, 21, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Cumurcu, B.E.; Ozyurt, H.; Etikan, I.; Demir, S.; Karlidag, R. Total antioxidant capacity and total oxidant status in patients with major depression: Impact of antidepressant treatment. Psychiatry Clin. Neurosci. 2009, 63, 639–645. [Google Scholar] [CrossRef] [PubMed]
- Kotan, V.O.; Sarandol, E.; Kirhan, E.; Ozkaya, G.; Kirli, S. Effects of long-term antidepressant treatment on oxidative status in major depressive disorder: A 24-week follow-up study. Prog. Neuro Psychopharmacol. Biol. Psychiatry 2011, 35, 1284–1290. [Google Scholar] [CrossRef] [PubMed]
- Yanik, M.; Erel, O.; Kati, M. The relationship between potency of oxidative stress and severity of depression. Acta Neuropsychiatr. 2004, 16, 200–203. [Google Scholar] [CrossRef] [PubMed]
- Behr, G.A.; Moreira, J.C.F.; Frey, B.N. Preclinical and Clinical Evidence of Antioxidant Effects of Antidepressant Agents: Implications for the Pathophysiology of Major Depressive Disorder. Oxidative Med. Cell. Longev. 2012, 2012, 609421. [Google Scholar] [CrossRef] [PubMed]
- Gawryluk, J.W.; Wang, J.-F.; Andreazza, A.C.; Shao, L.; Young, L.T. Decreased levels of glutathione, the major brain antioxidant, in post-mortem prefrontal cortex from patients with psychiatric disorders. Int. J. Neuropsychopharmacol. 2011, 14, 123–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seth, P.; Kumari, R.; Dikshit, M.; Srimal, R.C. Modulation of rat peripheral polymorphonuclear leukocyte response by nitric oxide and arginine. Blood 1994, 84, 2741–2748. [Google Scholar] [CrossRef] [Green Version]
- Sethi, S.; Singh, M.P.; Dikshit, M. Nitric oxide-mediated augmentation of polymorphonuclear free radical generation after hy-poxia-reoxygenation. Blood 1999, 93, 333–340. [Google Scholar] [CrossRef]
- Garthwaite, J. Glutamate, nitric oxide and cell-cell signalling in the nervous system. Trends Neurosci. 1991, 14, 60–67. [Google Scholar] [CrossRef]
- Dhir, A.; Kulkarni, S. Involvement of nitric oxide (NO) signaling pathway in the antidepressant action of bupropion, a dopamine reuptake inhibitor. Eur. J. Pharmacol. 2007, 568, 177–185. [Google Scholar] [CrossRef]
- Dhir, A.; Kulkarni, S.K. Nitric oxide and major depression. Nitric Oxide 2011, 24, 125–131. [Google Scholar] [CrossRef]
- Harvey, B.H. Affective Disorders and Nitric Oxide: A Role in Pathways to Relapse and Refractoriness? Hum. Psychopharmacol. 1996, 11, 309–319. [Google Scholar] [CrossRef]
- Joca, S.R.; Guimarães, F.S. Inhibition of neuronal nitric oxide synthase in the rat hippocampus induces antidepressant-like effects. Psychopharmacology 2006, 185, 298–305. [Google Scholar] [CrossRef] [PubMed]
- van Amsterdam, J.G.; Opperhuizen, A. Nitric oxide and biopterin in depression and stress. Psychiatry Res. 1999, 85, 33–38. [Google Scholar] [CrossRef]
- Moncada, S.; Palmer, R.M.; Higgs, E. Biosynthesis of nitric oxide from l-arginine: A pathway for the regulation of cell function and communication. Biochem. Pharmacol. 1989, 38, 1709–1715. [Google Scholar] [CrossRef]
- Oliveira, R.M.; Guimarães, F.S.; Deakin, J. Expression of neuronal nitric oxide synthase in the hippocampal formation in affective disorders. Braz. J. Med. Biol. Res. 2008, 41, 333–341. [Google Scholar] [CrossRef] [Green Version]
- Srivastava, N.; Barthwal, M.K.; Dalal, P.K.; Agarwal, A.K.; Nag, D.; Srimal, R.C.; Seth, P.K.; Dikshit, M. Nitrite content and antioxidant enzyme levels in the blood of schizophrenia patients. Psychopharmacology 2001, 158, 140–145. [Google Scholar] [CrossRef]
- Sun, M.; Zhao, Y.; Gu, Y.; Xu, C. Inhibition of nNOS reduces ischemic cell death through down-regulating calpain and caspase-3 after experimental stroke. Neurochem. Int. 2009, 54, 339–346. [Google Scholar] [CrossRef] [PubMed]
- Finkel, M.S.; Laghrissi-Thode, F.; Pollock, B.G.; Rong, J. Paroxetine is a novel nitric oxide synthase inhibitor. Psychopharmacol. Bull. 1996, 32, 653–658. [Google Scholar]
- Harkin, A.; Connor, T.J.; Burns, M.P.; Kelly, J.P. Nitric oxide synthase inhibitors augment the effects of serotonin re-uptake inhibitors in the forced swimming test. Eur. Neuropsychopharmacol. 2004, 14, 274–281. [Google Scholar] [CrossRef] [PubMed]
- Umathe, S.N.; Bhutada, P.S.; Jain, N.S.; Mundhada, Y.R.; Borkar, S.S.; Dhumal, B. Role of nitric oxide in obsessive–compulsive behavior and its involvement in the anti-compulsive effect of paroxetine in mice. Nitric Oxide 2009, 21, 140–147. [Google Scholar] [CrossRef] [PubMed]
- Wallerath, T.; Gath, I.; Aulitzky, W.E.; Pollock, J.S.; Kleinert, H.; Förstermann, U. Identification of the NO synthase isoforms expressed in human neutrophil granulocytes, megakaryocytes and platelets. Thromb. Haemost. 1997, 77, 163–167. [Google Scholar] [CrossRef] [PubMed]
- Galkina, S.I.; Golenkina, E.A.; Fedorova, N.V.; Ksenofontov, A.L.; Serebryakova, M.V.; Arifulin, E.A.; Stadnichuk, V.I.; Baratova, L.A.; Sud’Ina, G.F. Inhibition of Neutrophil Secretion Upon Adhesion as a Basis for the Anti-Inflammatory Effect of the Tricyclic Antidepressant Imipramine. Front. Pharmacol. 2021, 12, 709719. [Google Scholar] [CrossRef]
- Barthwal, M.K.; Srivastava, N.; Shukla, R.; Nag, D.; Seth, P.K.; Srirnal, R.C.; Dikshit, M. Polymorphonuclear leukocyte nitrite content and antioxidant enzymes in Parkinson’s disease patients. Acta Neurol. Scand. 1999, 100, 300–304. [Google Scholar] [CrossRef]
- Gatto, E.M.; Riobó, N.A.; Carreras, M.C.; Cherñavsky, A.; Rubio, A.; Satz, M.L.; Poderoso, J.J. Overexpression of neutrophil neuronal nitric oxide synthase in Parkinson’s disease. Nitric Oxide 2000, 4, 534–539. [Google Scholar] [CrossRef]
- Bryan, N.S. Nitrite in nitric oxide biology: Cause or consequence?: A systems-based review. Free Radic. Biol. Med. 2006, 41, 691–701. [Google Scholar] [CrossRef] [PubMed]
- Djordjević, V.V.; Stojanović, I.; Stanković-Ferlez, D.; Ristić, T.; Lazarević, D.; Cosić, V.; Djordjević, V.B. Plasma nitrite/nitrate concentrations in patients with schizophrenia. Clin. Chem. Lab. Med. 2010, 48, 89–94. [Google Scholar] [CrossRef] [Green Version]
- Gałecki, P.; Szemraj, J.; Bieńkiewicz, M.; Florkowski, A.; Gałecka, E. Lipid peroxidation and antioxidant protection in patients during acute depressive episodes and in remission after fluoxetine treatment. Pharmacol. Rep. 2009, 61, 436–447. [Google Scholar] [CrossRef]
- O’Connor, K.J.; Moncada, S. Glucocorticoids inhibit the induction of nitric oxide synthase and the related cell damage in ade-nocarcinoma cells. Biochim. Biophys. Acta 1991, 1097, 227–231. [Google Scholar] [CrossRef]
- Tonnessen, B.H.; Severson, S.R.; Hurt, R.D.; Miller, V.M. Modulation of nitric-oxide synthase by nicotine. J. Pharmacol. Exp. Ther. 2000, 295, 601–606. [Google Scholar]
- Vallance, P. Dietary nitrate: Poison or panacea? Gut 1997, 40, 288. [Google Scholar] [CrossRef] [Green Version]
- Raison, C.L.; Capuron, L.; Miller, A.H. Cytokines sing the blues: Inflammation and the pathogenesis of depression. Trends Immunol. 2006, 27, 24–31. [Google Scholar] [CrossRef] [Green Version]
- Vaccarino, V.; Brennan, M.-L.; Miller, A.H.; Bremner, J.D.; Ritchie, J.C.; Lindau, F.; Veledar, E.; Su, S.; Murrah, N.V.; Jones, L.; et al. Association of Major Depressive Disorder with Serum Myeloperoxidase and Other Markers of Inflammation: A Twin Study. Biol. Psychiatry 2008, 64, 476–483. [Google Scholar] [CrossRef] [Green Version]
- Gałecki, P.; Gałecka, E.; Maes, M.; Chamielec, M.; Orzechowska, A.; Bobińska, K.; Lewiński, A.; Szemraj, J. The expression of genes encoding for COX-2, MPO, iNOS, and sPLA2-IIA in patients with recurrent depressive disorder. J. Affect. Disord. 2012, 138, 360–366. [Google Scholar] [CrossRef]
- American Psychiatric Association. Mood disorders. In Diagnostic and Statistical Manual of Mental Disorders (DSM-IV-TR), 4th ed.; American Psychiatric Association: Washington, DC, USA, 2000; pp. 345–428. [Google Scholar]
- Goldberg, D.; Williams, P. A User’s Guide to the General Health Questionnaire; NFER-Nelson: Windsor, UK, 1988. [Google Scholar]
- Hamilton, M. A rating scale for depression. J. Neurol. Neurosurg. Psychiatry 1960, 23, 56–62. [Google Scholar] [CrossRef] [Green Version]
- American Psychiatric Association. Global assessment of functioning scale. In Diagnostic and Statistical Manual of Mental Disorders (DSM-IV-TR), 4th ed.; American Psychiatric Association: Washington, DC, USA, 2000; pp. 34–35. [Google Scholar]
- Singh, A.K.; Awasthi, D.; Dubey, M.; Nagarkoti, S.; Chandra, T.; Barthwal, M.K.; Tripathi, A.K.; Dikshit, M. Expression of inducible NOS is indispensable for the antiproliferative and proapoptotic effect of imatinib in BCR–ABL positive cells. J. Leukoc. Biol. 2021, 110, 853–866. [Google Scholar] [CrossRef]
- Jyoti, A.; Singh, A.; Dubey, M.; Kumar, S.; Saluja, R.; Keshari, R.S.; Verma, A.; Chandra, T.; Kumar, A.; Bajpai, V.K.; et al. Interaction of Inducible Nitric Oxide Synthase with Rac2 Regulates Reactive Oxygen and Nitrogen Species Generation in the Human Neutrophil Phagosomes: Implication in Microbial Killing. Antioxid. Redox Signal. 2014, 20, 417–431. [Google Scholar] [CrossRef]
- Jones, M.N. Nitrate reduction by shaking with cadmium: Alternative to cadmium columns. Water Res. 1984, 18, 643–646. [Google Scholar] [CrossRef]
- Singh, A.K.; Awasthi, D.; Dubey, M.; Nagarkoti, S.; Kumar, A.; Chandra, T.; Barthwal, M.K.; Tripathi, A.K.; Dikshit, M. High oxidative stress adversely affects NFκB mediated induction of inducible nitric oxide synthase in human neutrophils: Implications in chronic myeloid leukemia. Nitric Oxide 2016, 58, 28–41. [Google Scholar] [CrossRef]
- Nomura, Y.; Wickramaratne, P.J.; Warner, V.; Mufson, L.; Weissman, M.M. Family discord, parental depression, and psycho-pathology in offspring: Ten-year follow-up. J. Am. Acad. Child Adolesc. Psychiatry 2002, 41, 402–409. [Google Scholar] [CrossRef] [PubMed]
- Zalar, B.; Blatnik, A.; Maver, A.; Klemenc-Ketiš, Z.; Peterlin, B. Family history as an important factor for stratifying participants in genetic studies of major depression. Balk. J. Med. Genet. 2018, 21, 5–12. [Google Scholar] [CrossRef] [Green Version]
- Frank, M.G.; Hendricks, S.E.; Bessette, D.; Johnson, D.R.; Frank, J.L.W.; Burke, W.J. Levels of monocyte reactive oxygen species are associated with reduced natural killer cell activity in major depressive disorder. Neuropsychobiology 2001, 44, 1–6. [Google Scholar] [CrossRef]
- Talarowska, M.; Szemraj, J.; Gałecki, P. Myeloperoxidase gene expression and cognitive functions in depression. Adv. Med. Sci. 2015, 60, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, B.S.; Dean, O.M.; Dodd, S.; Malhi, G.S.; Berk, M. N-acetylcysteine in depressive symptoms and functionality: A systematic review and meta-analysis. J. Clin. Psychiatry 2016, 77, e457–e466. [Google Scholar] [CrossRef]
- Ooi, S.L.; Green, R.; Pak, S.C. N-Acetylcysteine for the Treatment of Psychiatric Disorders: A Review of Current Evidence. BioMed Res. Int. 2018, 2469486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ribaudo, G.; Bortoli, M.; Pavan, C.; Zagotto, G.; Orian, L. Antioxidant Potential of Psychotropic Drugs: From Clinical Evidence to In Vitro and In Vivo Assessment and toward a New Challenge for in Silico Molecular Design. Antioxidants 2020, 9, 714. [Google Scholar] [CrossRef] [PubMed]
- Farhadnejad, H.; Tehrani, A.N.; Salehpour, A.; Hekmatdoost, A. Antioxidant vitamin intakes and risk of depression, anxiety and stress among female adolescents. Clin. Nutr. ESPEN 2020, 40, 257–262. [Google Scholar] [CrossRef]
- Gautam, M.; Agrawal, M.; Gautam, M.; Sharma, P.; Gautam, A.S.; Gautam, S. Role of antioxidants in generalised anxiety disorder and depression. Indian J. Psychiatry 2012, 54, 244–247. [Google Scholar] [CrossRef]
- Huang, Q.; Liu, H.; Suzuki, K.; Ma, S.; Liu, C. Linking What We Eat to Our Mood: A Review of Diet, Dietary Antioxidants, and Depression. Antioxidants 2019, 8, 376. [Google Scholar] [CrossRef] [Green Version]
- Scapagnini, G.; Davinelli, S.; Drago, F.; De Lorenzo, A.; Oriani, G. Antioxidants as antidepressants: Fact or fiction? CNS Drugs 2012, 26, 477–490. [Google Scholar] [CrossRef]
- Caruso, G.; Grasso, M.; Fidilio, A.; Torrisi, S.A.; Musso, N.; Geraci, F.; Tropea, M.R.; Privitera, A.; Tascedda, F.; Puzzo, D.; et al. Antioxidant Activity of Fluoxetine and Vortioxetine in a Non-Transgenic Animal Model of Alzheimer’s Disease. Front. Pharmacol. 2021, 12, 809541. [Google Scholar] [CrossRef]
- Ali-Sisto, T.; Tolmunen, T.; Viinamäki, H.; Mäntyselkä, P.; Valkonen-Korhonen, M.; Koivumaa-Honkanen, H.; Honkalampi, K.; Ruusunen, A.; Nandania, J.; Velagapudi, V.; et al. Global arginine bioavailability ratio is decreased in patients with major depressive disorder. J. Affect. Disord. 2018, 229, 145–151. [Google Scholar] [CrossRef] [Green Version]
- Chrapko, W.E.; Jurasz, P.; Radomski, M.W.; Lara, N.; Archer, S.L.; Le Mellédo, J.M. Decreased platelet nitric oxide synthase activity and plasma nitric oxide metabolites in major depressive disorder. Biol. Psychiatry 2004, 56, 129–134. [Google Scholar] [CrossRef] [PubMed]
- García, R.G.; Zarruk, J.G.; Barrera, C.; Pinzón, A.; Trillos, E.; Arenas, W.D.; Luengas, C.; Tomaz, C.; López-Jaramillo, P. Plasma Nitrate Levels and Flow-Mediated Vasodilation in Untreated Major Depression. Psychosom. Med. 2011, 73, 344–349. [Google Scholar] [CrossRef]
- Loeb, E.; El Asmar, K.; Trabado, S.; Gressier, F.; Colle, R.; Rigal, A.; Martin, S.; Verstuyft, C.; Fève, B.; Chanson, P.; et al. Nitric Oxide Synthase activity in major depressive episodes before and after antidepressant treatment: Results of a large case-control treatment study. Psychol. Med. 2020, 52, 80–89. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, E.; Yagi, G.; Nakaki, T.; Kanba, S.; Asai, M. Elevated plasma nitrate levels in depressive states. J. Affect. Disord. 2001, 63, 221–224. [Google Scholar] [CrossRef]
- Bernstein, H.-G.; Stanarius, A.; Baumann, B.; Henning, H.; Krell, D.; Danos, P.; Falkai, P.; Bogerts, B. Nitric oxide synthase-containing neurons in the human hypothalamus: Reduced number of immunoreactive cells in the paraventricular nucleus of depressive patients and schizophrenics. Neuroscience 1998, 83, 867–875. [Google Scholar] [CrossRef]
- Karolewicz, B.; Szebeni, K.; Stockmeier, C.A.; Konick, L.; Overholser, J.C.; Jurjus, G.; Roth, B.L.; Ordway, G.A. Low nNOS protein in the locus coeruleus in major depression. J. Neurochem. 2004, 91, 1057–1066. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gałecki, P.; Maes, M.; Florkowski, A.; Lewiński, A.; Gałecka, E.; Bieńkiewicz, M.; Szemraj, J. Association between inducible and neuronal nitric oxide synthase polymorphisms and recurrent depressive disorder. J. Affect. Disord. 2011, 129, 175–182. [Google Scholar] [CrossRef]
- Zunszain, P.A.; Anacker, C.; Cattaneo, A.; Carvalho, L.A.; Pariante, C.M. Glucocorticoids, cytokines and brain abnormalities in depression. Prog. Neuropsychopharmacol. Biol. Psychiatry 2011, 35, 722–729. [Google Scholar] [CrossRef] [Green Version]
- Di Rosa, M.; Radomski, M.; Carnuccio, R.; Moncada, S. Glucocorticoids inhibit the induction of nitric oxide synthase in macro-phages. Biochem. Biophys. Res. Commun. 1990, 172, 1246–1252. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Control | Patient | Relative | |
|---|---|---|---|
| Number of patients | 27 | 29 | 27 |
| Age, Years (mean ± SEM) | 29.25 ± 0.90 | 30.24 ± 1.84 | 31.11 ± 1.85 |
| Gender (M/F), n (%) | 18 (66.67%)/9 (33.33%) | 13 (44.82%)/16 (55.17%) | 15 (55.56%)/12 (44.44%) |
| FBS, mg/dL (mean ± SEM) | 77.25 ± 2.1 | 81.07 ± 1.77 | 76.74 ± 2.0 |
| Cholesterol, mg/dL (mean ± SEM) | 109.4. ± 2.4 | 116.9 ± 3.0 | 117.7 ± 4.5 |
| Total Bilirubin, mg/dL (mean ± SEM) | 0.5700 ± 0.024 | 0.5169 ± 0.0178 | 0.5833 ± 0.0212 |
| ALP, U/L (mean ± SEM) | 120.9 ± 7.7 | 129 ± 9.2 | 114.5 ± 9.6 |
| SGPT, U/L (mean ± SEM) | 30.25 ± 1.58 | 29.24 ± 1.92 | 33.67 ± 1.93 |
| TLC (mean ± SEM) | 6554 ± 210.8 | 6721 ± 209.6 | 6670 ± 221.5 |
| Variable | |
|---|---|
| Diagnosis | |
| Major depressive disorder (1st episode), n (%) | 25 (86.21%) |
| Major depressive disorder, recurrent, n (%) | 04 (13.79%) |
| Duration of current episode, (mean ± SEM) | 3.94 ± 0.5838 months |
| Family of mood disorder present, n (%) | 05 (17.24%) |
| Severity of depression, score on HAM-D, (mean ± SEM) | 19.86 ± 0.7636 |
| Functioning, score on GAF, (mean ± SEM) | 34.10 ± 1.905 |
| PMNs ROS | Plasma Nitrite | PMNs Nitrite | nNOS mRNA Expression | PMNs MPO | Cortisol | |
|---|---|---|---|---|---|---|
| r | 0.7956 | 0.5142 | 0.6762 | 0.2604 | 0.01353 | 0.4083 |
| p | 0.0001* | 0.0102 * | 0.0021 ** | 0.2542 | 0.9603 | 0.0345 * |
| n | 18 | 24 | 18 | 21 | 16 | 27 |
| 95% CI | 0.5230 to 0.9205 | 0.1398 to 0.7600 | 0.3060 to 0.8688 | −0.1929 to 0.6222 | −0.4854 to 0.5058 | 0.03354 to 0.6825 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Somani, A.; Singh, A.K.; Gupta, B.; Nagarkoti, S.; Dalal, P.K.; Dikshit, M. Oxidative and Nitrosative Stress in Major Depressive Disorder: A Case Control Study. Brain Sci. 2022, 12, 144. https://doi.org/10.3390/brainsci12020144
Somani A, Singh AK, Gupta B, Nagarkoti S, Dalal PK, Dikshit M. Oxidative and Nitrosative Stress in Major Depressive Disorder: A Case Control Study. Brain Sciences. 2022; 12(2):144. https://doi.org/10.3390/brainsci12020144
Chicago/Turabian StyleSomani, Aditya, Abhishek Kumar Singh, Bandna Gupta, Sheela Nagarkoti, Pronob Kumar Dalal, and Madhu Dikshit. 2022. "Oxidative and Nitrosative Stress in Major Depressive Disorder: A Case Control Study" Brain Sciences 12, no. 2: 144. https://doi.org/10.3390/brainsci12020144
APA StyleSomani, A., Singh, A. K., Gupta, B., Nagarkoti, S., Dalal, P. K., & Dikshit, M. (2022). Oxidative and Nitrosative Stress in Major Depressive Disorder: A Case Control Study. Brain Sciences, 12(2), 144. https://doi.org/10.3390/brainsci12020144