
A Pilot Study on Plasma and Urine Neurotransmitter Levels in Children with Tic Disorders

Abstract
:1. Introduction
2. Materials and Methods
2.1. Chemicals and Reagents
2.2. Patients and Control Groups
2.3. Samples
2.4. Sample Preparation
2.5. UPLC–MS/MS and Quantification
2.6. Statistical Analysis
3. Results
3.1. Levels of Neurotransmitters from Plasma and Urine
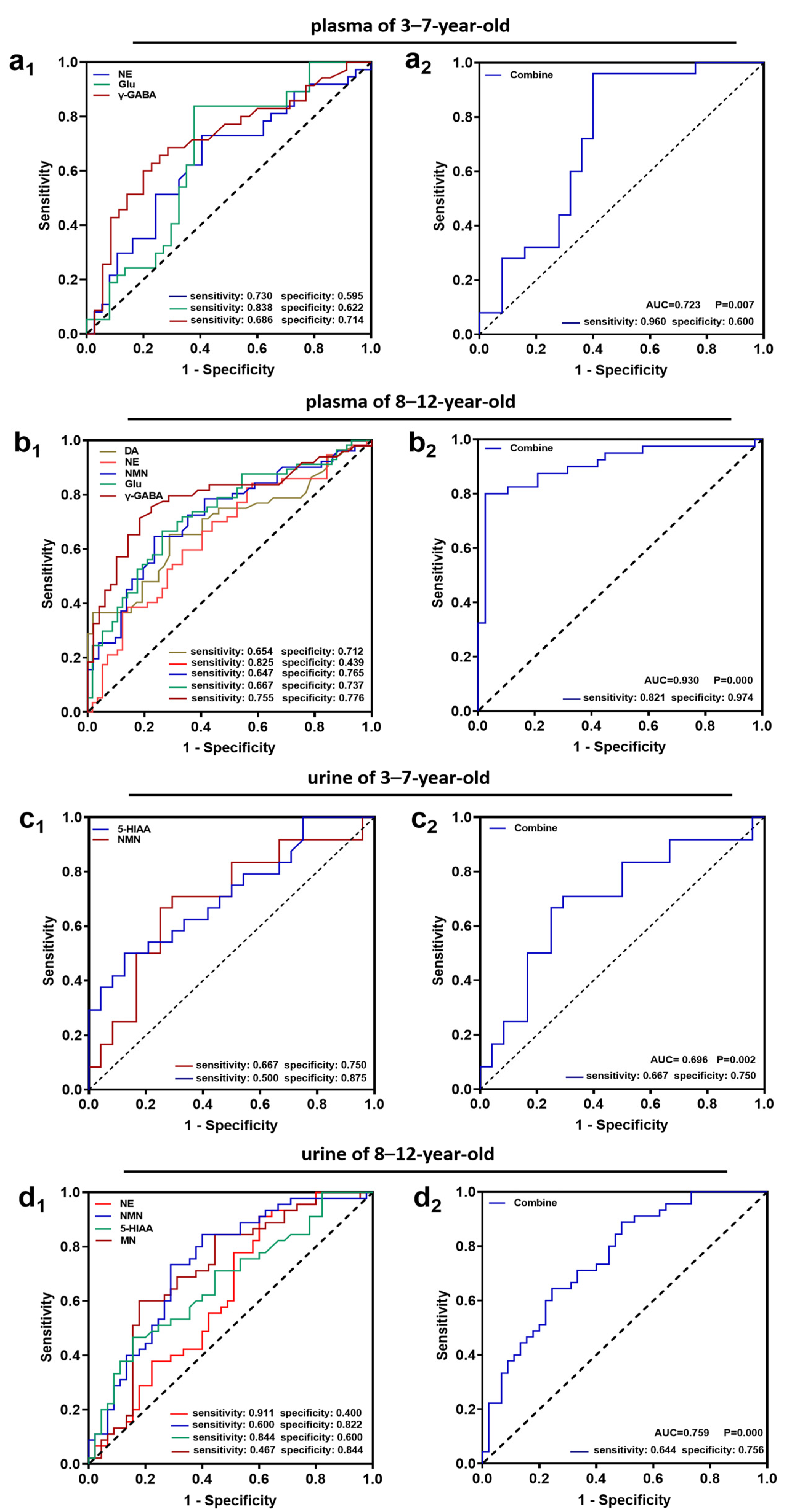
3.2. Assessing the Predictive Value of Neurotransmitters for Predicting TD
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Augustine, F.; Singer, H.S. Merging the pathophysiology and pharmacotherapy of tics. Tremor Other Hyperkinet Mov. 2019, 8, 595. [Google Scholar] [CrossRef]
- Li, F.; Cui, Y.; Li, Y.; Guo, L.; Ke, X.; Liu, J.; Luo, X.; Zheng, Y.; Leckman, J.F. Prevalence of mental disorders in school children and adolescents in China: Diagnostic data from detailed clinical assessments of 17,524 individuals. J. Child Psychol. Psychiatry 2022, 63, 34–46. [Google Scholar] [CrossRef]
- Knight, T.; Steeves, T.; Day, L.; Lowerison, M.; Jette, N.; Pringsheim, T. Prevalence of tic disorders: A systematic review and meta-analysis. Pediatr. Neurol. 2012, 47, 77–90. [Google Scholar] [CrossRef]
- Scharf, J.M.; Miller, L.L.; Gauvin, C.A.; Alabiso, J.; Mathews, C.A.; Ben-Shlomo, Y. Population prevalence of Tourette syndrome: A systematic review and meta-analysis. Mov. Disord. 2015, 30, 221–228. [Google Scholar] [CrossRef]
- Yang, J.; Hirsch, L.; Martino, D.; Jette, N.; Roberts, J.; Pringsheim, T. The prevalence of diagnosed tourette syndrome in Canada: A national population-based study. Mov. Disord. 2016, 31, 1658–1663. [Google Scholar] [CrossRef]
- Paschou, P.; Fernandez, T.V.; Sharp, F.; Heiman, G.A.; Hoekstra, P.J. Genetic susceptibility and neurotransmitters in Tourette syndrome. Int. Rev. Neurobiol. 2013, 112, 155–177. [Google Scholar]
- Lian-qing, H.; Hou-cheng, Z.; Yu-ze, H.; Yu-bin, W.; Wei-duan, Z.; Xuan, Z.; Shao-jun, Z. Determination and significance of serum dopamine in patients with tic disorder. J. Sun. Yat. Sen. Univ. Med. Sci. 2006, 27, 2. [Google Scholar]
- Guang-hua, X.; Min, W. The monoamine neurotransmitters changes and significances in tic disorder patients’ serom. Nerv. Dis. Ment. Health 2008, 8, 3. [Google Scholar]
- Janik, P.; Kalbarczyk, A.; Gutowicz, M.; Barańczyk-Kuźma, A.; Kwieciński, H. The analysis of selected neurotransmitter concentrations in serum of patients with Tourette syndrome. Neurol. Neurochir. Pol. 2010, 44, 251–259. [Google Scholar] [CrossRef]
- Wen-jing, Y.; Xue, B.; Wen, Z.; Li, W.; Xiao-wei, S.; Su-mei, W. Effects of Jianpi Zhidong Decoction on the neurotransmitters of tourette syndrome children. Chin. J. Tradit. Chin. Med. Pharm. 2015, 30, 5. [Google Scholar]
- Yu, S.; Yin, Y.; Li, Q.; Yu, J.; Liu, W.; Wang, D.; Cheng, Q.; Xie, S.; Cheng, X.; Qiu, L. Validation of an improved liquid chromatography tandem mass spectrometry method for rapid and simultaneous analysis of plasma catecholamine and their metabolites. J. Chromatogr. B Analyt. Technol. Biomed. Life Sci. 2019, 1129, 121805. [Google Scholar] [CrossRef]
- Bergmann, M.L.; Schmedes, A. Highly sensitive LC-MS/MS analysis of catecholamines in plasma. Clin. Biochem. 2020, 82, 51–57. [Google Scholar] [CrossRef]
- Cheuk, M.Y.; Lo, Y.C.; Poon, W.T. Determination of urine catecholamines and metanephrines by reversed-phase liquid chromatography-tandem mass spectrometry. Chin. J. Chromatogr. 2017, 35, 1042–1047. [Google Scholar] [CrossRef]
- Ayala-Lopez, N.; Watts, S.W. Physiology and pharmacology of neurotransmitter transporters. Compr. Physiol. 2021, 11, 2279–2295. [Google Scholar]
- Capetian, P.; Roessner, V.; Korte, C.; Walitza, S.; Riederer, F.; Taurines, R.; Gerlach, M.; Moser, A. Altered urinary tetrahydroisoquinoline derivatives in patients with Tourette syndrome: Reflection of dopaminergic hyperactivity? J. Neural. Transm. 2021, 128, 115–120. [Google Scholar] [CrossRef]
- Steeves, T.D.; Ko, J.H.; Kideckel, D.M.; Rusjan, P.; Houle, S.; Sandor, P.; Lang, A.E.; Strafella, A.P. Extrastriatal dopaminergic dysfunction in Tourette syndrome. Ann. Neurol. 2010, 67, 170–181. [Google Scholar] [CrossRef]
- Singer, H.S.; Szymanski, S.; Giuliano, J.; Yokoi, F.; Dogan, A.S.; Brasic, J.R.; Zhou, Y.; Grace, A.A.; Wong, D.F. Elevated intrasynaptic dopamine release in Tourette’s syndrome measured by PET. Am. J. Psychiatry. 2002, 159, 1329–1336. [Google Scholar] [CrossRef]
- Zhao, M.; Wang, X.; Deng, J.; Guan, Y.; Zhou, J.; Li, T.; Luan, G. Globus pallidus internus electric high-frequency stimulation modulates dopaminergic activity in the striatum of a rat model of Tourette syndrome. World Neurosurg. 2019, 127, e881–e887. [Google Scholar] [CrossRef]
- Pringsheim, T.; Okun, M.S.; Müller-Vahl, K.; Martino, D.; Jankovic, J.; Cavanna, A.E.; Woods, D.W.; Robinson, M.; Jarvie, E.; Roessner, V.; et al. Practice guideline recommendations summary: Treatment of tics in people with Tourette syndrome and chronic tic disorders. Neurology 2019, 92, 896–906. [Google Scholar] [CrossRef] [Green Version]
- Abi-Jaoude, E.; Segura, B.; Obeso, I.; Cho, S.S.; Houle, S.; Lang, A.E.; Rusjan, P.; Sandor, P.; Strafella, A.P. Similar striatal D2/D3 dopamine receptor availability in adults with Tourette syndrome compared with healthy controls: A [(11) C]-(+)-PHNO and [(11) C]raclopride positron emission tomography imaging study. Hum. Brain. Mapp. 2015, 36, 2592–2601. [Google Scholar] [CrossRef]
- Gobert, A.; Rivet, J.M.; Audinot, V.; Newman-Tancredi, A.; Cistarelli, L.; Millan, M.J. Simultaneous quantification of serotonin, dopamine and noradrenaline levels in single frontal cortex dialysates of freely-moving rats reveals a complex pattern of reciprocal auto- and heteroreceptor-mediated control of release. Neuroscience 1998, 84, 413–429. [Google Scholar] [CrossRef]
- Singer, H.S. Treatment of tics and tourette syndrome. Curr. Treat. Options Neurol. 2010, 12, 539–561. [Google Scholar] [CrossRef]
- Naaijen, J.; Forde, N.J.; Lythgoe, D.J.; Akkermans, S.E.; Openneer, T.J.; Dietrich, A.; Zwiers, M.P.; Hoekstra, P.J.; Buitelaar, J.K. Fronto-striatal glutamate in children with Tourette’s disorder and attention-deficit/hyperactivity disorder. Neuroimage Clin. 2016, 13, 16–23. [Google Scholar] [CrossRef] [Green Version]
- Kanaan, A.S.; Gerasch, S.; García-García, I.; Lampe, L.; Pampel, A.; Anwander, A.; Near, J.; Möller, H.E.; Müller-Vahl, K. Pathological glutamatergic neurotransmission in Gilles de la Tourette syndrome. Brain 2017, 140, 218–234. [Google Scholar] [CrossRef] [Green Version]
- Harris, A.D.; Singer, H.S.; Horska, A.; Kline, T.; Ryan, M.; Edden, R.A.; Mahone, E.M. GABA and glutamate in children with primary complex motor stereotypies: An 1H-MRS Study at 7T. Am. J. Neuroradiol. 2016, 37, 552–557. [Google Scholar] [CrossRef] [Green Version]
- Lerner, A.; Bagic, A.; Simmons, J.M.; Mari, Z.; Bonne, O.; Xu, B.; Kazuba, D.; Herscovitch, P.; Carson, R.E.; Murphy, D.L.; et al. Widespread abnormality of the γ-aminobutyric acid-ergic system in Tourette syndrome. Brain 2012, 135, 1926–1936. [Google Scholar] [CrossRef] [Green Version]
- McCairn, K.W.; Nagai, Y.; Hori, Y.; Ninomiya, T.; Kikuchi, E.; Lee, J.Y.; Suhara, T.; Iriki, A.; Minamimoto, T.; Takada, M.; et al. A primary role for nucleus accumbens and related limbic network in vocal tics. Neuron 2016, 89, 300–307. [Google Scholar] [CrossRef] [Green Version]
- Niens, J.; Reh, F.; Çoban, B.; Cichewicz, K.; Eckardt, J.; Liu, Y.T.; Hirsh, J.; Riemensperger, T.D. Dopamine modulates serotonin innervation in the drosophila brain. Front. Syst. Neurosci. 2017, 11, 76. [Google Scholar] [CrossRef] [Green Version]
- Hildonen, M.; Levy, A.M.; Dahl, C.; Bjerregaard, V.A.; Birk Møller, L.; Guldberg, P.; Debes, N.M.; Tümer, Z. Elevated expression of SLC6A4 encoding the serotonin transporter (SERT) in Gilles de la Tourette syndrome. Genes 2021, 12, 86. [Google Scholar] [CrossRef]
- Müller-Vahl, K.R.; Bindila, L.; Lutz, B.; Musshoff, F.; Skripuletz, T.; Baumgaertel, C.; Sühs, K.W. Cerebrospinal fluid endocannabinoid levels in Gilles de la Tourette syndrome. Neuropsychopharmacology 2020, 45, 1323–1329. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Number of Plasma Samples | Number of Urine Samples | |||
|---|---|---|---|---|
| 3–7-Year-Old | 8–12-Year-Old | 3–7-Year-Old | 8–12-Year-Old | |
| TD | 37 | 57 | 24 | 45 |
| Control | 37 | 57 | 24 | 45 |
| Variable (nmol/L) | 3–7-Year-Old | 8–12-Year-Old | ||||
|---|---|---|---|---|---|---|
| TD | Control | p | TD | Control | p | |
| Dopamine (DA) | 0.089 (0.056–0.225) | 0.090 (0.029–1.417) | 0.844 | 0.098 (0.061–0.250) | 0.079 (0.038–0.127) | 0.001 |
| Epinephrine (E) | 0.412 (0.107–2.106) | 0.438 (0.114–1.323) | 0.991 | 0.508 (0.105–1.762) | 0.518 (0.139–1.032) | 0.650 |
| Norepinephrine (NE) | 2.359 (0.515–6.164) | 1.466 (0.536–4.824) | 0.035 | 2.115 (0.593–9.338) | 1.279 (0.527–8.947) | 0.005 |
| Normetanephrine (NMN) | 0.203 (0.070–0.503) | 0.151 (0.055–0.357) | 0.184 | 0.249 (0.062–0.858) | 0.138 (0.055–0.542) | 0.000 |
| 5-hydroxytryptamine (5-HT) | 323.000 (67.500–830.560) | 320.000 (64.600–2564.840) | 0.339 | 283.000 (26.400–1436.600) | 262.000 (61.400–2041.600) | 0.661 |
| Glutamic Acid (Glu) (×104) | 5.483 (2.138–15.442) | 3.603 (1.007–13.879) | 0.017 | 6.053 (2.014–14.478) | 3.541 (1.251–8.440) | 0.000 |
| Tyrosine (Tyr) (×104) | 6.938 (3.774–16.358) | 6.515 (3.463–14.069) | 0.440 | 6.840 (3.580–13.909) | 7.813 (4.229–12.455) | 0.080 |
| Tryptophan (Trp) (×104) | 4.737 (2.830–7.570) | 4.709 (2.304–8.087) | 0.677 | 4.383 (2.099–7.417) | 5.708 (3.080–11.129) | 0.000 |
| γ-aminobutyric acid (γ-GABA) | 109.000 (35.400–840.100) | 65.000 (16.850–442.226) | 0.002 | 90.000 (21.600–785.000) | 52.000 (13.400–145.800) | 0.000 |
| Variable (µg/g crt) | 3–7-Year-Old | 8–12-Year-Old | ||||
|---|---|---|---|---|---|---|
| TD | Control | p | TD | Control | p | |
| Dopamine (DA) | 465.095 (165.969–1131.521) | 497.020 (174.262–1074.702) | 0.967 | 388.200 (227.438–920.541) | 403.610 (140.032–964.183) | 0.768 |
| Epinephrine (E) | 35.860 (12.656–133.923) | 60.375 (11.265–103.146) | 0.918 | 20.580 (5.271–109.440) | 48.930 (7.539–100.839) | 0.025 |
| Norepinephrine (NE) | 47.180 (28.110–187.927) | 42.320 (9.178–108.930) | 0.322 | 44.260 (21.334–118.078) | 37.470 (11.023–115.271) | 0.045 |
| Metanephrine (MN) | 34.265 (11.174–159.292) | 36.400 (5.761–135.284) | 0.446 | 38.730 (12.427–106.105) | 22.620 (7.600–112.756) | 0.000 |
| Normetanephrine (NMN) | 200.635 (17.185–450.106) | 91.355 (17.265–349.413) | 0.020 | 92.820 (30.022–573.435) | 51.560 (15.331–304.060) | 0.000 |
| Vanillylmandelic Acid (VMA) (×103) | 1.715 (0.418–8.883) | 1.300 (0.279–5.483) | 0.132 | 1.000 (0.314–13.543) | 1.600 (0.187–9.141) | 0.379 |
| Homovanillic acid (HVA) (×103) | 5.010 (1.403–51.593) | 4.226 (1.219–10.603) | 0.279 | 2.540 (0.177–11.100) | 3.470 (0.676–10.136) | 0.019 |
| 5-Hydroxyindoleacetic acid (5-HIAA) (×103) | 5.810 (1.246–133.066) | 2.220 (0.365–9.978) | 0.010 | 2.960 (0.422–13.360) | 1.750 (0.113–9.695) | 0.006 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qian, Q.-Q.; Tan, Q.-Q.; Sun, D.; Lu, Q.; Xin, Y.-Y.; Wu, Q.; Zhou, Y.; Liu, Y.-X.; Tian, P.-C.; Liu, Z.-S. A Pilot Study on Plasma and Urine Neurotransmitter Levels in Children with Tic Disorders. Brain Sci. 2022, 12, 880. https://doi.org/10.3390/brainsci12070880
Qian Q-Q, Tan Q-Q, Sun D, Lu Q, Xin Y-Y, Wu Q, Zhou Y, Liu Y-X, Tian P-C, Liu Z-S. A Pilot Study on Plasma and Urine Neurotransmitter Levels in Children with Tic Disorders. Brain Sciences. 2022; 12(7):880. https://doi.org/10.3390/brainsci12070880
Chicago/Turabian StyleQian, Qiao-Qiao, Qian-Qian Tan, Dan Sun, Qing Lu, Ying-Ying Xin, Qian Wu, Yong Zhou, Yang-Xi Liu, Pei-Chao Tian, and Zhi-Sheng Liu. 2022. "A Pilot Study on Plasma and Urine Neurotransmitter Levels in Children with Tic Disorders" Brain Sciences 12, no. 7: 880. https://doi.org/10.3390/brainsci12070880
APA StyleQian, Q. -Q., Tan, Q. -Q., Sun, D., Lu, Q., Xin, Y. -Y., Wu, Q., Zhou, Y., Liu, Y. -X., Tian, P. -C., & Liu, Z. -S. (2022). A Pilot Study on Plasma and Urine Neurotransmitter Levels in Children with Tic Disorders. Brain Sciences, 12(7), 880. https://doi.org/10.3390/brainsci12070880