
Cognitive and Affective Theory of Mind across Adulthood

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Neuropsychological Assessment
2.3. ToM Assessment
2.3.1. Affective Component of ToM
2.3.2. Cognitive Component of ToM
2.4. Procedure
2.5. Statistical Analysis
3. Results
3.1. Correlation Analyses of ToM Tasks among Age Groups
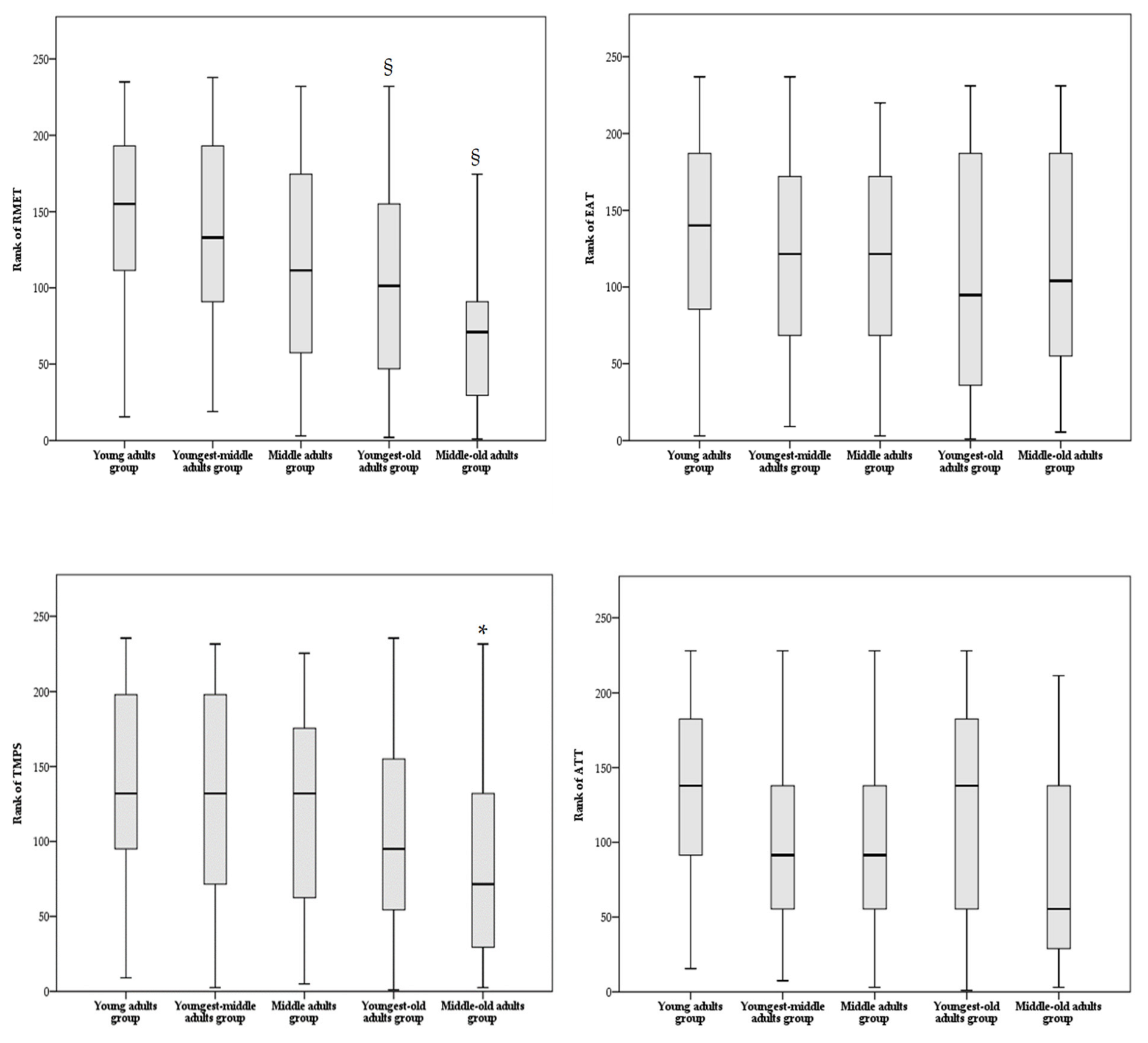
3.2. Comparison Analyses among Age Groups for ToM Tasks
3.3. Comparison Analyses among Age Groups for ToM Affective and Cognitive Outcomes
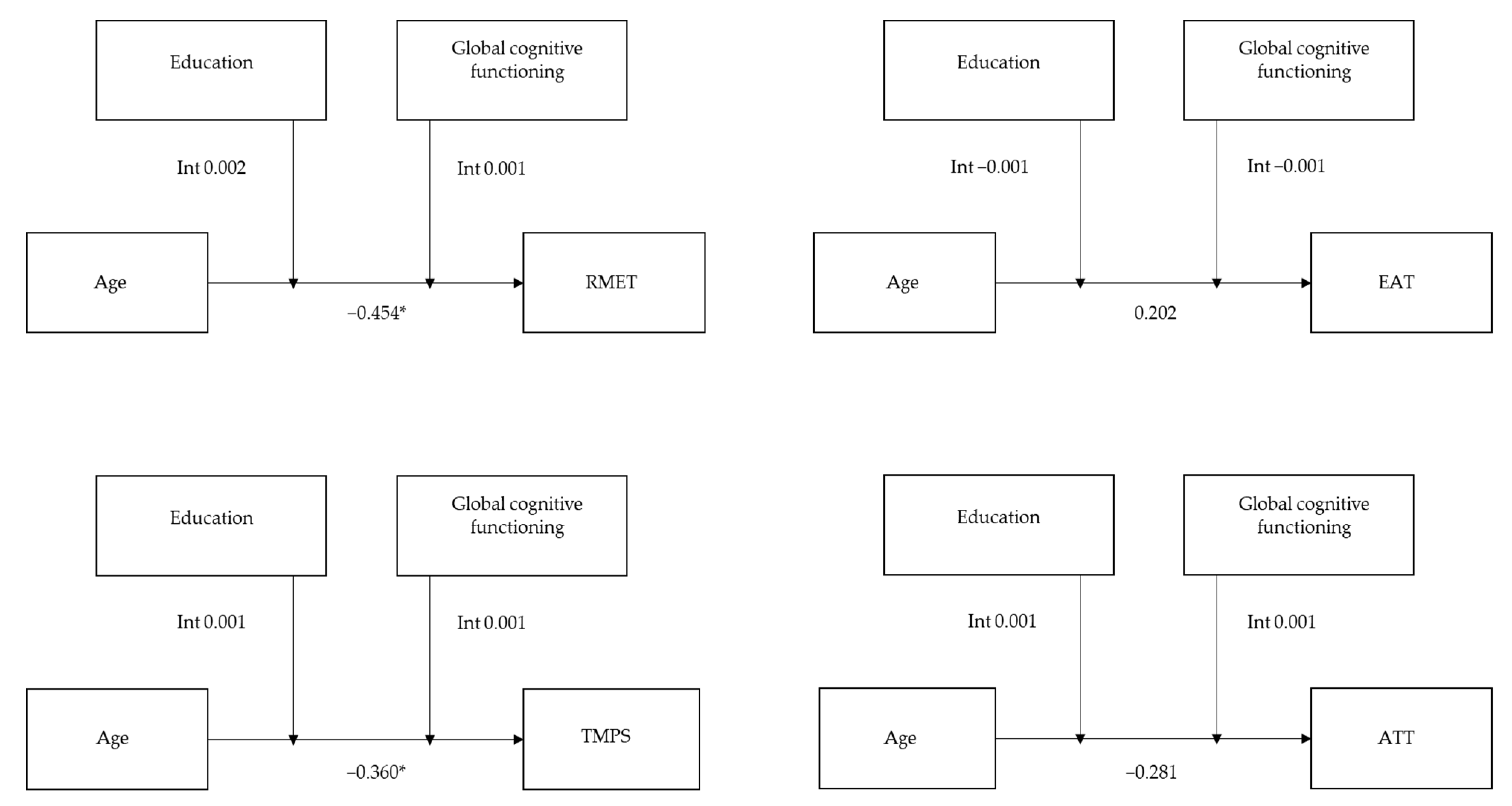
3.4. Moderation Role of Education and Global Cognitive Functioning in Relation to Aging and ToM Abilities
3.5. Summary of the Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Premack, D.; Woodruff, G. Does the chimpanzee have a theory of mind? Behav. Brain Sci. 1978, 1, 515–526. [Google Scholar] [CrossRef] [Green Version]
- Shamay-Tsoory, S.G.; Tomer, R.; Goldsher, D.; Berger, B.D.; AharonPeretz, J. Impairment in cognitive and affective empathy in patients with brain lesions: Anatomical and cognitive correlates. J. Clin. Exp. Neuropsychol. 2004, 26, 1113–1127. [Google Scholar] [CrossRef]
- Shamay-Tsoory, S.G.; Aharon-Peretz, J. Dissociable prefrontal networks for cognitive and affective theory of mind: A lesion study. Neuropsychologia 2007, 45, 3054–3067. [Google Scholar] [CrossRef] [PubMed]
- Hynes, C.A.; Baird, A.A.; Grafton, S.T. Differential role of the orbital frontal lobe in emotional versus cognitive perspective-taking. Neuropsychologia 2006, 44, 374–383. [Google Scholar] [CrossRef]
- Völlm, B.A.; Taylor, A.N.; Richardson, P.; Corcoran, R.; Stirling, J.; McKie, S.; Deakin, J.F.; Elliott, R. Neuronal correlates of theory of mind and empathy: A functional magnetic resonance imaging study in a nonverbal task. NeuroImage 2006, 29, 90–98. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, M.; Miner Weaver, J.M.; Nelson, J.A.; Calkins, S.D.; Leerkes, E.M.; Marcovitch, S. Longitudinal association between children‘s understanding of emotion and theory of mind. Cogn. Emot. 2011, 25, 1074–1086. [Google Scholar] [CrossRef] [Green Version]
- Wimmer, H.; Perner, J. Beliefs about beliefs: Representation and constraining function of wrong beliefs in young children’s understanding of deception. Cognition 1983, 13, 103–128. [Google Scholar] [CrossRef]
- Perner, J.; Wimmer, H. “John Thinks That Mary Thinks That…” attribution of second-order beliefs by 5- to 10- year-old children. J. Exp. Child Psychol. 1985, 39, 437–471. [Google Scholar] [CrossRef]
- Astington, J.W.; Dack, L.A. Theory of Mind. In Encyclopedia of Infant and Early Childhood Development; Haith, M.M., Benson, J.B., Eds.; British Library Cataloguing; Elsevier Inc.: Amsterdam, The Netherlands, 2008; Volume 3, pp. 343–356. [Google Scholar]
- Vetter, N.C.; Altgassen, M.; Phillips, L.; Mahy, C.E.V.; Kliegel, M. Development of affective theory of mind across adolescence: Disentangling the role of executive functions. Dev. Neuropsychol. 2013, 38, 114–125. [Google Scholar] [CrossRef]
- Gabriel, E.T.; Oberger, R.; Schmoeger, M.; Deckert, M.; Vockh, S.; Auff, E.; Willinger, U. Cognitive and affective Theory of Mind in adolescence: Developmental aspects and associated neuropsychological variables. Psychol. Res. 2021, 85, 533–553. [Google Scholar] [CrossRef] [Green Version]
- MacDonald, P.M.; Kirkpatrick, S.W.; Sullivan, L.A. Production of facial expressions of emotion in preschool children. Percept. Mot. Skills 1996, 82, 76–78. [Google Scholar] [CrossRef] [PubMed]
- Ruffman, T.; Keenan, T.R. The belief-based emotion of suprise: The case for a lag in understanding relative to false belief. Dev. Psychol. 1996, 32, 40–49. [Google Scholar] [CrossRef]
- Pons, F.; Harris, P.L.; de Rosnay, M. Emotion comprehension between 3 and 11 years: Developmental periods and hierarchical organization. Eur. J. Dev. Psychol. 2004, 1, 127–152. [Google Scholar] [CrossRef]
- Phillips, L.H.; Bull, R.; Allen, R.; Insch, P.; Burr, K.; Ogg, W. Lifespan aging and belief reasoning: Influences of executive function and social cue decoding. Cognition 2011, 120, 236–247. [Google Scholar] [CrossRef]
- Sullivan, S.; Ruffman, T. Social understanding: How does it fare with advancing years? Br. J. Psychol. 2004, 95, 1–18. [Google Scholar] [CrossRef] [Green Version]
- Maylor, E.A.; Moulson, J.M.; Muncer, A.; Taylor, L.A. Does performance on theory of mind tasks decline in old age? Br. J. Psychol. 2002, 93, 465–485. [Google Scholar] [CrossRef]
- Charlton, R.A.; Barrick, T.R.; Markus, H.S.; Morris, R.G. Theory of mind associations with other cognitive functions and brain imaging in normal aging. Psychol. Aging 2009, 24, 338–348. [Google Scholar] [CrossRef] [PubMed]
- Saltzman, J.; Strauss, E.; Hunter, M.; Archibald, S. Theory of mind and executive functions in normal human aging and Parkinson’s disease. J. Int. Neuropsychol. Soc. 2000, 6, 781–788. [Google Scholar] [CrossRef]
- MacPherson, S.E.; Phillips, L.H.; Della Sala, S. Age, executive function, and social decision making: A dorsolateral prefrontal theory of cognitive aging. Psychol. Aging 2002, 17, 598–609. [Google Scholar] [CrossRef]
- Mahy, C.E.V.; Vetter, N.; Kühn-Popp, N.; Löcher, C.; Krautschuk, S.; Kliegel, M. The influence of inhibitory processes on affective theory of mind in young and old adults. Neuropsychol. Dev. Cogn. 2014, 21, 129–145. [Google Scholar] [CrossRef]
- Grainger, S.A.; Henry, J.D.; Phillips, L.H.; Vanman, E.J.; Allen, R. Age deficits in facial affect recognition: The influence of dynamic cues. J. Gerontol. B Psychol. Sci. Soc. Sci. 2017, 72, 622–632. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castelli, I.; Baglio, F.; Blasi, V.; Alberoni, M.; Falini, A.; Liverta-Sempio, O.; Nemni, R.; Marchetti, A. Effects of aging on mindreading ability through the eyes: An fMRI study. Neuropsychologia 2010, 48, 2586–2594. [Google Scholar] [CrossRef] [PubMed]
- Duval, C.; Piolino, P.; Bejanin, A.; Eustache, F.; Desgranges, B. Age effects on different components of theory of mind. Conscious. Cogn. 2011, S20, 627–642. [Google Scholar] [CrossRef]
- Li, X.; Wang, K.; Wang, F.; Tao, Q.; Xie, Y.; Cheng, Q. Aging of theory of mind: The influence of educational level and cognitive processing. Int. J. Psychol. 2013, 48, 715–727. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Su, Y. Age-related differences in the performance of theory of mind in older adults: A dissociation of cognitive and affective components. Psychol. Aging 2013, 28, 284–291. [Google Scholar] [CrossRef]
- Fischer, A.L.; O’Rourke, N.; Loken Thornton, W. Age Differences in Cognitive and Affective Theory of Mind: Concurrent Contributions of Neurocognitive Performance, Sex, and Pulse Pressure. J. Gerontol. B. Psychol. Sci. Soc. Sci. 2017, 72, 71–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bottiroli, S.; Cavallini, E.; Ceccato, I.; Vecchi, T.; Lecce, S. Theory of Mind in aging: Comparing cognitive and affective components in the faux pas test. Arch. Gerontol. Geriatr. 2016, 62, 152–162. [Google Scholar] [CrossRef]
- Stone, V.E.; Baron-Cohen, S.; Knight, R.T. Frontal lobe contributions to theory of mind. J. Cogn. Neurosci. 1998, 10, 640–656. [Google Scholar] [CrossRef]
- Baksh, R.A.; Abrahams, S.; Auyeung, B.; MacPherson, S.E. The Edinburgh Social Cognition Test (ESCoT): Examining the effects of age on a new measure of theory of mind and social norm understanding. PLoS ONE 2018, 13, e0195818. [Google Scholar] [CrossRef]
- Slessor, G.; Phillips, L.H.; Bull, R. Exploring the specificity of age-related differences in theory of mind tasks. Psychol. Aging 2007, 22, 639–643. [Google Scholar] [CrossRef] [Green Version]
- Bernstein, D.M.; Thornton, W.L.; Sommerville, J.A. Theory of mind through the ages: Older and middle-aged adults exhibit more errors than do younger adults on a continuous false belief task. Exp. Aging Res. 2011, 37, 481–502. [Google Scholar] [CrossRef] [PubMed]
- Kelley, W.M.; Miezin, F.M.; McDermott, K.B.; Buckner, R.L.; Raichle, M.E.; Cohen, N.J.; Ollinger, J.M.; Akbudak, E.; Conturo, T.E.; Snyder, A.Z.; et al. Hemispheric specialization in human dorsal frontal cortex and medial temporal lobe for verbal and nonverbal memory encoding. Neuron 1998, 20, 927–936. [Google Scholar] [CrossRef] [Green Version]
- Thompson-Schill, S.L.; D’Esposito, M.; Aguirre, G.K.; Farah, M.J. Role of left inferior prefrontal cortex in retrieval of semantic knowledge: A reevaluation. Proc. Natl. Acad. Sci. USA 1997, 94, 14792–14797. [Google Scholar] [CrossRef] [Green Version]
- Moran, J.M.; Jolly, E.; Mitchell, J.P. Social-cognitive deficits in normal aging. J. Neurosci. 2012, 32, 5553–5561. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castelli, F.; Happé, F.; Frith, U.; Frith, C. Movement and mind: A functional imaging study of perception and interpretation of complex intentional movement patterns. Neuroimage 2000, 12, 314–325. [Google Scholar] [CrossRef] [PubMed]
- Raimo, S.; Di Vita, A.; Boccia, M.; Iona, T.; Cropano, M.; Gaita, M.; Guariglia, C.; Grossi, D.; Palermo, L. The Body across the Lifespan: On the Relation between Interoceptive Sensibility and High-Order Body Representations. Brain Sci. 2021, 11, 493. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.B.; Oh, J.H.; Park, J.H.; Choi, S.P.; Wee, J.H. Differences in youngest-old, middle-old, and oldest-old patients who visit the emergency department. Clin. Exp. Emerg. Med. 2018, 5, 249–255. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Santangelo, G.; Siciliano, M.; Pedone, R.; Vitale, C.; Falco, F.; Bisogno, R.; Siano, P.; Barone, P.; Grossi, D.; Santangelo, F.; et al. Normative data for the Montreal Cognitive Assessment in an Italian population sample. Neurol. Sci. 2015, 36, 585–591. [Google Scholar] [CrossRef] [Green Version]
- Raven, J.C. Progressive Matrices 1947; Series A, AB; B.H.K. Levis & Co., Ltd.: London, UK, 1947. [Google Scholar]
- Spinnler, H.; Tognoni, G. Standardizzazione e taratura italiana di test neuropsicologici. Ital. J. Neurol. Sci. 1987, 6, 47–50. [Google Scholar]
- Baron-Cohen, S.; Jolliffe, T.; Mortimore, C.; Robertson, M. Another advanced test of theory of mind: Evidence from very high functioning adults with autism or asperger syndrome. J. Child. Psychol. Psychiatry 1997, 38, 813–822. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vellante, M.; Baron-Cohen, S.; Melis, M.; Marrone, M.; Petretto, D.R.; Masala, C.; Preti, A. The “Reading the Mind in the Eyes” test: Systematic review of psychometric properties and a validation study in Italy. Cogn. Neuropsychiatry 2013, 18, 326–354. [Google Scholar] [CrossRef] [PubMed]
- Blair, R.J.; Cipolotti, L. Impaired social response reversal. A case of ‘acquired sociopathy’. Brain 2000, 123, 1122–1141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brüne, M. Theory of mind and the role of IQ in chronic disorganized schizophrenia. Schizophr. Res. 2003, 60, 57–64. [Google Scholar] [CrossRef]
- Prior, M.; Marchi, S.; Sartori, G. Social Cognition and Behavior. A Tool for Assessment. Cognizione Sociale e Comportamento. Uno Strumento per la Misurazione, ED; Upsel Domenighini Editore: Padova, Italy, 2003. [Google Scholar]
- Lissek, S.; Peters, S.; Fuchs, N.; Witthaus, H.; Nicolas, V.; Tegenthoff, M.; Juckel, G.; Brüne, M. Cooperation and deception recruit different subsets of the theory-of-mind network. PLoS ONE 2008, 3, e2023. [Google Scholar] [CrossRef] [Green Version]
- Quade, D. Rank analysis of covariance. J. Am. Stat. Assoc. 1967, 62, 1187–1200. [Google Scholar] [CrossRef]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; Guildford Press: New York, NY, USA, 2013. [Google Scholar]
- Keightley, M.L.; Winocur, G.; Burianova, H.; Hongwanishkul, D.; Grady, C.L. Age effects on social cognition: Faces tell a different story. Psychol. Aging 2006, 21, 558–572. [Google Scholar] [CrossRef]
- Schurz, M.; Radua, J.; Aichhorn, M.; Richlan, F.; Perner, J. Fractionating theory of mind: A meta-analysis of functional brain imaging studies. Neurosci. Biobehav. Rev. 2014, 42, 9–34. [Google Scholar] [CrossRef] [Green Version]
- Poletti, M.; Enrici, I.; Adenzato, M. Cognitive and affective Theory of Mind in neurodegenerative diseases: Neuropsychological, neuroanatomical and neurochemical levels. Neurosci. Biobehav. Rev. 2012, 36, 2147–2164. [Google Scholar] [CrossRef]
- Belfort, T.; Simões, J.P.; Santos, R.L.; Lacerda, I.; Dourado, M.C.N. Social cognition: Patterns of impairments in mild and moderate Alzheimer’s disease. Int. J. Geriatr. Psychiatry 2020, 35, 1385–1392. [Google Scholar] [CrossRef]
- Moran, J.M. Lifespan development: The effects of typical aging on theory of mind. Behav. Brain Res. 2013, 237, 32–40. [Google Scholar] [CrossRef] [PubMed]
- Kynast, J.; Quinque, E.M.; Polyakova, M.; Luck, T.; Riedel-Heller, S.G.; Baron-Cohen, S.; Hinz, A.; Witte, A.V.; Sacher, J.; Villringer, A.; et al. Mindreading From the Eyes Declines With Aging—Evidence from 1603 Subjects. Front. Aging Neurosci. 2020, 12, 550416. [Google Scholar] [CrossRef] [PubMed]
- Amodio, D.M.; Frith, C.D. Meeting of minds: The medial frontal cortex and social cognition. Nature reviews. Neuroscience 2006, 7, 268–277. [Google Scholar] [CrossRef] [PubMed]
- German, T.P.; Hehman, J.A. Representational and executive selection resources in ‘theory of mind’: Evidence from compromised belief-desire reasoning in old age. Cognition 2006, 101, 129–152. [Google Scholar] [CrossRef]
- Bailey, P.E.; Henry, J.D. Growing less empathic with age: Disinhibition of the self-perspective. J. Gerontol. B Psychol. Sci. Soc. Sci. 2008, 63, 219–226. [Google Scholar] [CrossRef] [Green Version]
- Cavallini, E.; Lecce, S.; Bottiroli, S.; Palladino, P.; Pagnin, A. Beyond false belief: Theory of mind in young, young-old, and old-old adults. Int. J. Aging Hum. Dev. 2013, 76, 181–198. [Google Scholar] [CrossRef]
- Obisesan, T.O.; Gillum, R.F. Cognitive function, social integration and mortality in a U.S. national cohort study of older adults. BMC Geriatr. 2009, 9, 33. [Google Scholar] [CrossRef] [Green Version]
- James, B.D.; Boyle, P.A.; Bennett, D.A. Correlates of susceptibility to scams in older adults without dementia. J. Elder. Abuse. Negl. 2014, 26, 107–122. [Google Scholar] [CrossRef]
- Kalbe, E.; Schlegel, M.; Sack, A.T.; Nowak, D.A.; Dafotakis, M.; Bangard, C.; Brand, M.; Shamay-Tsoory, S.; Onur, O.A.; Kessler, J. Dissociating cognitive from affective theory of mind: A TMS study. Cortex 2010, 46, 769–780. [Google Scholar] [CrossRef]
- Quesque, F.; Rossetti, Y. What do theory-of-mind tasks actually measure? Theory and practice. Perspect. Psychol. Sci. 2002, 15, 384–396. [Google Scholar] [CrossRef]
- Altschuler, M.R.; Trevisan, D.A.; Wolf, J.M.; Naples, A.J.; Foss-Feig, J.H.; Srihari, V.H.; McPartland, J.C. Face perception predicts affective theory of mind in autism spectrum disorder but not schizophrenia or typical development. J. Abnorm. Psychol. 2021, 130, 413–422. [Google Scholar] [CrossRef] [PubMed]
- Schaafsma, S.M.; Pfaff, D.W.; Spunt, R.P.; Adolphs, R. Deconstructing and reconstructing theory of mind. Trends Cogn. Sci. 2015, 19, 65–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hall, J.A.; Andrzejewski, S.A.; Yopchick, J.E. Psychosocial correlates of interpersonal sensitivity: A meta-analysis. J. Nonverbal Behav. 2009, 33, 149–180. [Google Scholar] [CrossRef]
- Cavallini, E.; Ceccato, I.; Bertoglio, S.; Francescani, A.; Vigato, F.; Ianes, A.B.; Lecce, S. Can theory of mind of healthy older adults living in a nursing home be improved? A randomized controlled trial. Aging Clin. Exp. Res. 2021, 33, 3029–3037. [Google Scholar] [CrossRef]
- Lecce, S.; Bottiroli, S.; Bianco, F.; Rosi, A.; Cavallini, E. Training older adults on Theory of Mind (ToM): Transfer on metamemory. Arch. Gerontol. Geriatr. 2015, 60, 217–226. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Young Adult Group (N = 50) | Youngest-Middle Adult Group (N = 50) | Middle Adult Group (N = 50) | Youngest-Old Adult Group (N = 50) | Middle-Old Adult Group (N = 38) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | Range | Mean ± SD | Range | Mean ± SD | Range | Mean ± SD | Range | Mean ± SD | Range | |
| Age | 28.84 ± 6.11 | 18–40 | 46.10 ± 2.98 | 41–50 | 55.36 ± 2.55 | 51–60 | 64.44 ± 2.94 | 61–70 | 73.76 ± 2.36 | 71–80 |
| Sex (F/M) | 25/25 | 25/25 | 25/25 | 25/25 | 18/20 | |||||
| Education ° | 14.72 ± 2.51 | 8–18 | 12.82 ± 3.81 | 8–18 | 11.86 ± 3.47 | 5–18 | 12.30 ± 4.14 | 5–18 | 9.57 ± 3.83 | 5–18 |
| MoCA | 27.56 ± 1.82 | 23–30 | 26.41 ± 2.12 | 20–30 | 25.58 ± 2.24 | 21–30 | 23.48 ± 3.69 | 14–29 | 22.07 ± 3.24 | 12–27 |
| RCPM | 34.26 ± 2.30 | 26–36 | 31.67 ± 3.68 | 18–36 | 30.94 ± 3.97 | 21–36 | 28.87 ± 5.17 | 14–36 | 26.76 ± 6.64 | 13–36 |
| MoCA * | 25.15 ± 1.88 | 20.59–28.85 | 25.07 ± 2.02 | 21.15–28.65 | 25.47 ± 2.28 | 21.51–30 | 24.03 ± 2.81 | 16.11–27.98 | 24.11 ± 3.21 | 16.40–27.72 |
| RCPM * | 29.34 ± 2.43 | 21.20–35.90 | 28.64 ± 3.24 | 17.30–34.30 | 29.62 ± 3.68 | 19.30–36 | 29.20 ± 3.55 | 17.90–35.90 | 28.57 ± 5.83 | 12.10–36 |
| Young Adult Group | |||||
| RMET | EAT | TMPS | ATT | ||
| RMET | rrho | 1 | 0.145 | 0.285 | 0.236 |
| p | 0.316 | 0.047 | 0.114 | ||
| EAT | rrho | - | 1 | 0.372 | 0.327 |
| p | 0.008 | 0.027 | |||
| TMPS | rrho | - | - | 1 | 0.308 |
| p | 0.039 | ||||
| ATT | rrho | - | - | - | 1 |
| p | |||||
| Youngest-Middle Adult Group | |||||
| RMET | EAT | TMPS | ATT | ||
| RMET | rrho | 1 | 0.318 | 0.267 | 0.329 |
| p | 0.025 | 0.061 | 0.019 | ||
| EAT | rrho | - | 1 | 0.372 | 0.464 * |
| p | 0.008 | 0.001 | |||
| TMPS | rrho | - | - | 1 | 0.134 |
| p | 0.352 | ||||
| ATT | rrho | - | - | - | 1 |
| p | |||||
| Middle Adult Group | |||||
| RMET | EAT | TMPS | ATT | ||
| RMET | rrho | 1 | 0.156 | 0.293 | 0.032 |
| p | 0.278 | 0.039 | 0.824 | ||
| EAT | rrho | - | 1 | 0.334 | 0.453 * |
| p | 0.018 | 0.001 | |||
| TMPS | rrho | - | - | 1 | 0.320 |
| p | 0.024 | ||||
| ATT | rrho | - | - | - | 1 |
| p | |||||
| Youngest-Old Adult Group | |||||
| RMET | EAT | TMPS | ATT | ||
| RMET | rrho | 1 | −0.082 | 0.524 * | 0.192 |
| p | 0.571 | <0.001 | 0.181 | ||
| EAT | rrho | - | 1 | 0.197 | 0.362 |
| p | 0.169 | 0.010 | |||
| TMPS | rrho | - | - | 1 | 0.046 |
| p | 0.752 | ||||
| ATT | rrho | - | - | - | 1 |
| p | |||||
| Middle-Old Adult Group | |||||
| RMET | EAT | TMPS | ATT | ||
| RMET | rrho | 1 | 0.429 | 0.293 | 0.489 * |
| p | 0.007 | 0.078 | 0.003 | ||
| EAT | rrho | - | 1 | 0.213 | 0.580 * |
| p | 0.206 | <0.001 | |||
| TMPS | rrho | - | - | 1 | 0.141 |
| p | 0.426 | ||||
| ATT | rrho | - | - | - | 1 |
| p | |||||
| Young Adult Group | Youngest-Middle Adult Group | Middle Adult Group | Youngest-Old Adult Group | Middle-Old Adult Group | Age Group | |||
|---|---|---|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | F | p | η2 | |
| RMET | 26.74 ± 4.07 | 26.34 ± 3.76 | 24.56 ± 4.68 | 23.82 ± 5.42 *§ | 22 ± 5.29 *§ | 6.061 | <0.001 | 0.127 |
| EAT | 26.44 ± 4.82 | 25.50 ± 4.73 | 25.62 ± 4.30 | 24.34 ± 6.23 | 25.47 ± 4.88 | 0.355 | 0.841 | 0.008 |
| TMPS | 51.91 ± 4.21 | 50.62 ± 5.64 | 49.62 ± 6.05 | 49.14 ± 5.73 | 47.48 ± 6.05 * | 2.911 | 0.023 | 0.066 |
| ATT | 10.19 ± 1.62 | 9.22 ± 1.90 | 9.24 ± 1.93 | 9.34 ± 2.17 | 8.62 ± 2.01 | 2.091 | 0.084 | 0.049 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Raimo, S.; Cropano, M.; Roldán-Tapia, M.D.; Ammendola, L.; Malangone, D.; Santangelo, G. Cognitive and Affective Theory of Mind across Adulthood. Brain Sci. 2022, 12, 899. https://doi.org/10.3390/brainsci12070899
Raimo S, Cropano M, Roldán-Tapia MD, Ammendola L, Malangone D, Santangelo G. Cognitive and Affective Theory of Mind across Adulthood. Brain Sciences. 2022; 12(7):899. https://doi.org/10.3390/brainsci12070899
Chicago/Turabian StyleRaimo, Simona, Maria Cropano, María Dolores Roldán-Tapia, Lidia Ammendola, Daniela Malangone, and Gabriella Santangelo. 2022. "Cognitive and Affective Theory of Mind across Adulthood" Brain Sciences 12, no. 7: 899. https://doi.org/10.3390/brainsci12070899
APA StyleRaimo, S., Cropano, M., Roldán-Tapia, M. D., Ammendola, L., Malangone, D., & Santangelo, G. (2022). Cognitive and Affective Theory of Mind across Adulthood. Brain Sciences, 12(7), 899. https://doi.org/10.3390/brainsci12070899