

Multi-Frequency Electrocochleography and Electrode Scan to Identify Electrode Insertion Trauma during Cochlear Implantation


Abstract
:1. Introduction
2. Methods
3. Results
4. Discussion
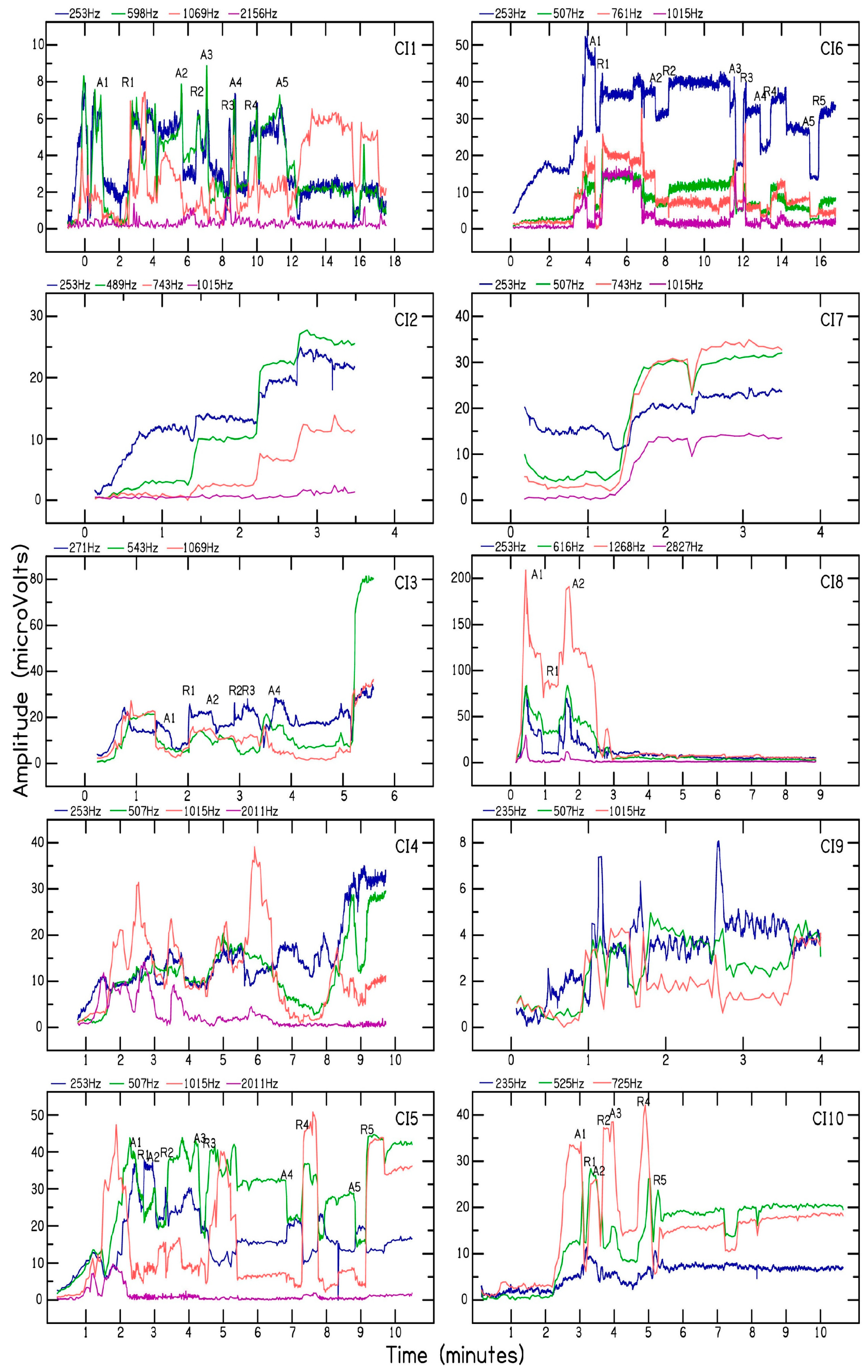
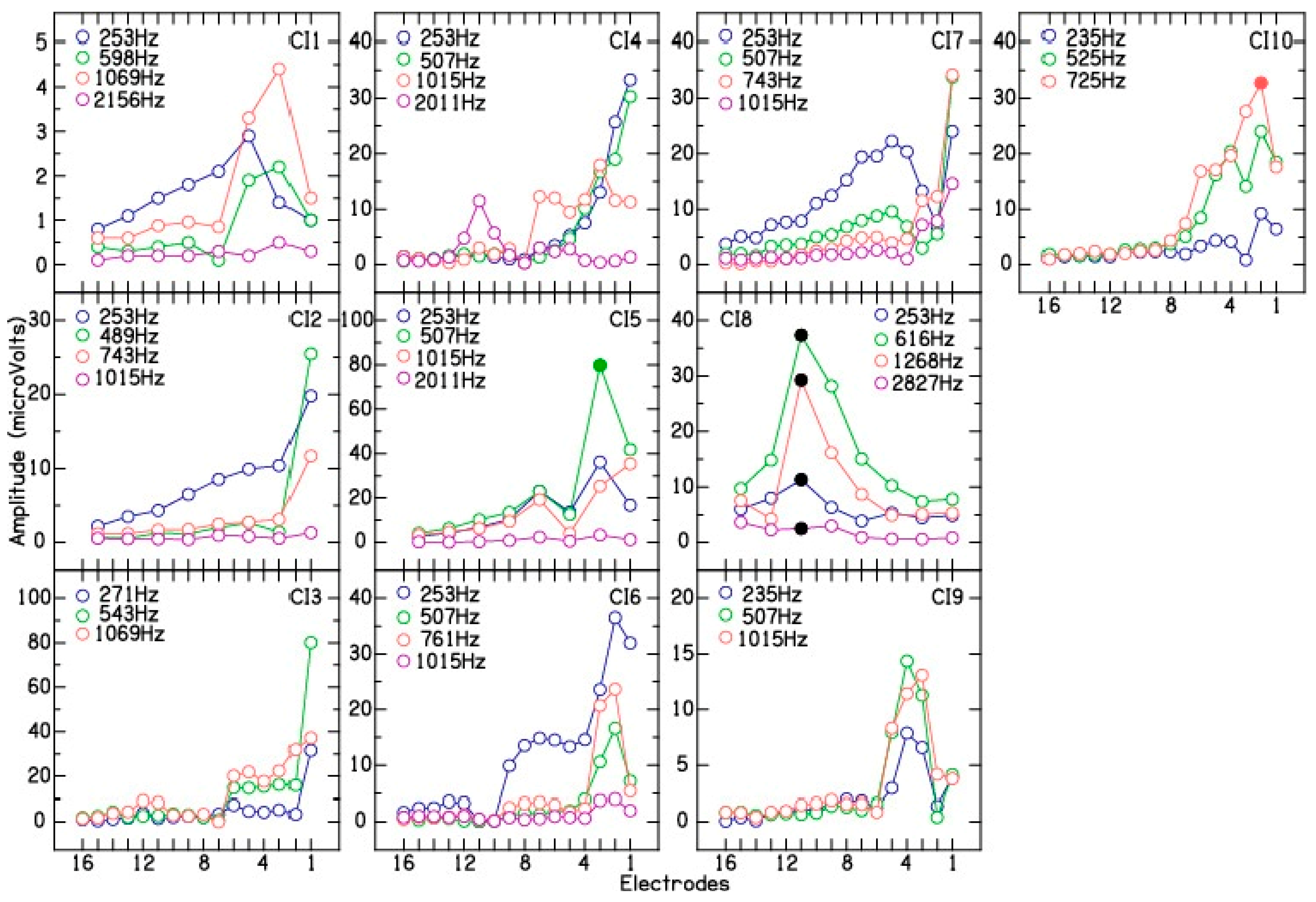
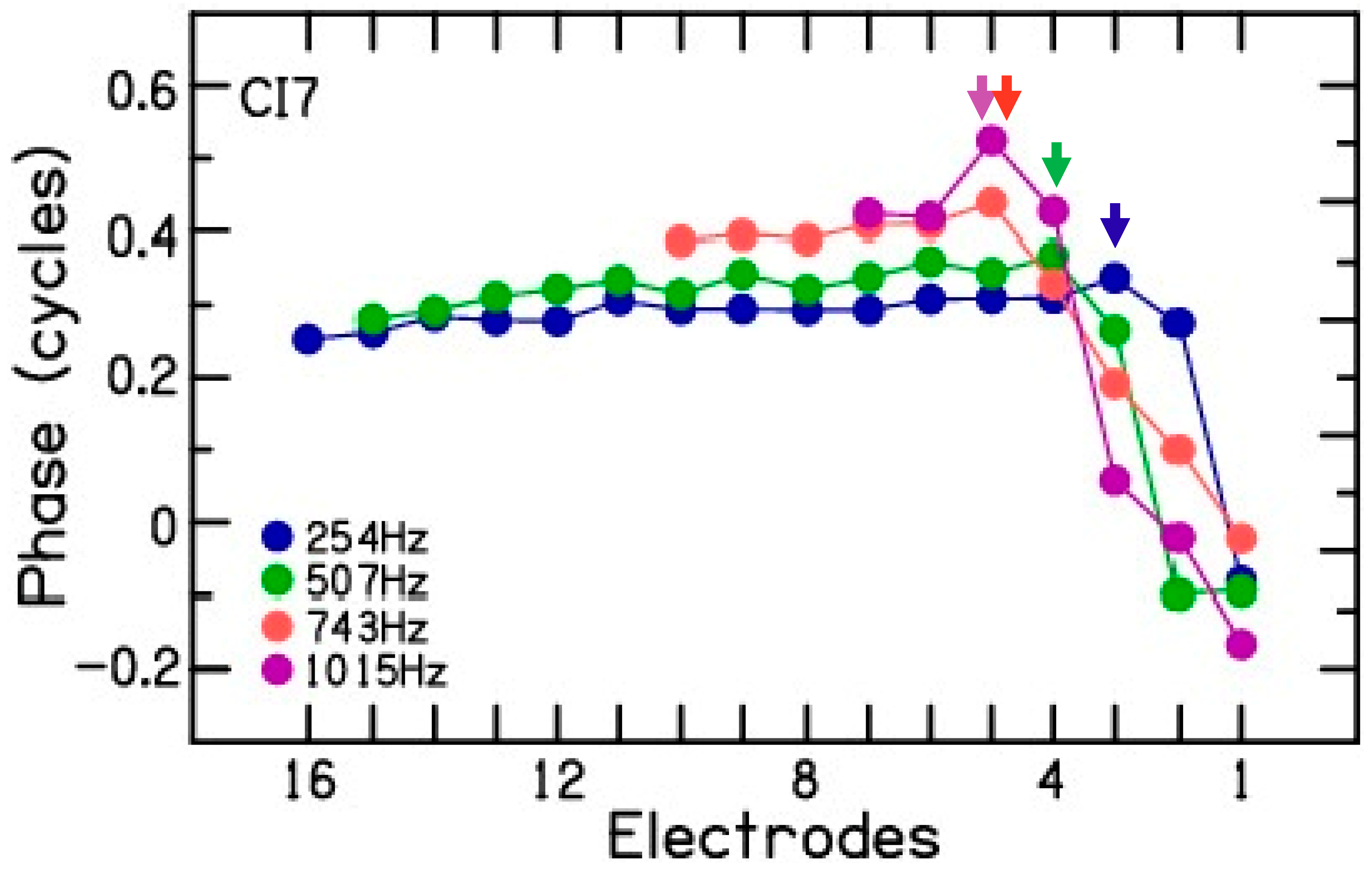
- The present study suggests that multi-frequency ECOG can be more reliable in detecting cochlear trauma as compared to the routinely used single-frequency ECOG measurements performed during CI electrode placement. Multi-frequency ECOG measurements are likely to show a simultaneous decrease in CM amplitude measured for the test frequencies during electrode insertion trauma, whereas a decrease in CM amplitude at one test frequency and a gradual increase in CM amplitude at other test frequencies are indicative of the advancement of the recording electrode beyond one of the multiple sites of CM generation or characteristic frequency along the basilar membrane [14].
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gantz, B.J.; Turner, C.; Gfeller, K.E.; Lowder, M.W. Preservation of hearing in cochlear implant surgery: Advantages of combined electrical and acoustical speech processing. Laryngoscope 2005, 115, 796–802. [Google Scholar] [CrossRef] [Green Version]
- Gifford, R.H.; Dorman, M.F.; McKarns, S.A.; Spahr, A.J. Combined electric and contralateral acoustic hearing: Word and sentence recognition with bimodal hearing. J. Speech Lang. Hear. Res. 2007, 50, 835–843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Connell, B.P.; Holder, J.T.; Dwyer, R.T.; Gifford, R.H.; Noble, J.H.; Bennett, M.L.; Rivas, A.; Wanna, G.B.; Haynes, D.S.; Labadie, R.F. Intra- and Postoperative Electrocochleography May Be Predictive of Final Electrode Position and Postoperative Hearing Preservation. Front. Neurosci. 2017, 11, 291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harris, M.S.; Koka, K.; Riggs, W.J.; Saleh, S.; Holder, J.T.; Dwyer, R.T.; Prentiss, S.; Lefler, S.; Kozlowski, K.; Hiss, M.M.; et al. Can Electrocochleography Help Preserve Hearing after Cochlear Implantation with Full Electrode Insertion? Otol. Neurotol. 2022, 43, 789–796. [Google Scholar] [CrossRef] [PubMed]
- Harris, M.S.; Riggs, W.J.; Giardina, C.K.; O’Connell, B.P.; Holder, J.T.; Dwyer, R.T.; Koka, K.; Labadie, R.F.; Fitzpatrick, D.C.; Adunka, O.F. Patterns Seen During Electrode Insertion Using Intracochlear Electrocochleography Obtained Directly Through a Cochlear Implant. Otol. Neurotol. 2017, 38, 1415–1420. [Google Scholar] [CrossRef] [PubMed]
- Harris, M.S.; Riggs, W.J.; Koka, K.; Litvak, L.M.; Malhotra, P.; Moberly, A.C.; O’Connell, B.P.; Holder, J.; Di Lella, F.A.; Boccio, C.M.; et al. Real-Time Intracochlear Electrocochleography Obtained Directly Through a Cochlear Implant. Otol. Neurotol. 2017, 38, e107–e113. [Google Scholar] [CrossRef]
- Koka, K.; Riggs, W.J.; Dwyer, R.; Holder, J.T.; Noble, J.H.; Dawant, B.M.; Ortmann, A.; Valenzuela, C.V.; Mattingly, J.K.; Harris, M.M.; et al. Intra-Cochlear Electrocochleography During Cochear Implant Electrode Insertion Is Predictive of Final Scalar Location. Otol. Neurotol. 2018, 39, e654–e659. [Google Scholar] [CrossRef]
- Lenarz, T.; Buechner, A.; Gantz, B.; Hansen, M.; Tejani, V.D.; Labadie, R.; O’Connell, B.; Buchman, C.A.; Valenzuela, C.V.; Adunka, O.F.; et al. Relationship between Intraoperative Electrocochleography and Hearing Preservation. Otol. Neurotol. 2022, 43, e72–e78. [Google Scholar] [CrossRef]
- O’Leary, S.; Briggs, R.; Gerard, J.M.; Iseli, C.; Wei, B.P.C.; Tari, S.; Rousset, A.; Bester, C. Intraoperative Observational Real-time Electrocochleography as a Predictor of Hearing Loss after Cochlear Implantation: 3 and 12 Month Outcomes. Otol. Neurotol. 2020, 41, 1222–1229. [Google Scholar] [CrossRef]
- Riggs, W.J.; Dwyer, R.T.; Holder, J.T.; Mattingly, J.K.; Ortmann, A.; Noble, J.H.; Dawant, B.M.; Valenzuela, C.V.; O’Connell, B.P.; Harris, M.S.; et al. Intracochlear Electrocochleography: Influence of Scalar Position of the Cochlear Implant Electrode on Postinsertion Results. Otol. Neurotol. 2019, 40, e503–e510. [Google Scholar] [CrossRef]
- Campbell, L.; Kaicer, A.; Sly, D.; Iseli, C.; Wei, B.; Briggs, R.; O’Leary, S. Intraoperative Real-time Cochlear Response Telemetry Predicts Hearing Preservation in Cochlear Implantation. Otol. Neurotol. 2016, 37, 332–338. [Google Scholar] [CrossRef] [PubMed]
- Dalbert, A.; Pfiffner, F.; Hoesli, M.; Koka, K.; Veraguth, D.; Roosli, C.; Huber, A. Assessment of Cochlear Function during Cochlear Implantation by Extra- and Intracochlear Electrocochleography. Front. Neurosci. 2018, 12, 18. [Google Scholar] [CrossRef]
- Saoji, A.A.; Graham, M.K.; Adkins, W.J.; Nassiri, A.M.; Neff, B.A.; Carlson, M.L.; Driscoll, C.L.W. Relationship Between Intraoperative Electrocochleography Responses and Immediate Postoperative Bone Conduction Thresholds in Cochlear Implantation. Otol. Neurotol. 2022, 43, e880–e887. [Google Scholar] [CrossRef] [PubMed]
- Saoji, A.A.; Patel, N.S.; Carlson, M.L.; Neff, B.A.; Koka, K.; Tarigoppula, V.S.A.; Driscoll, C.L.W. Multi-frequency Electrocochleography Measurements can be Used to Monitor and Optimize Electrode Placement during Cochlear Implant Surgery. Otol. Neurotol. 2019, 40, 1287–1291. [Google Scholar] [CrossRef] [PubMed]
- Buechner, A.; Bardt, M.; Haumann, S.; Geissler, G.; Salcher, R.; Lenarz, T. Clinical experiences with intraoperative electrocochleography in cochlear implant recipients and its potential to reduce insertion trauma and improve postoperative hearing preservation. PLoS ONE 2022, 17, e0266077. [Google Scholar] [CrossRef]
- Giardina, C.K.; Brown, K.D.; Adunka, O.F.; Buchman, C.A.; Hutson, K.A.; Pillsbury, H.C.; Fitzpatrick, D.C. Intracochlear Electrocochleography: Response Patterns During Cochlear Implantation and Hearing Preservation. Ear Hear. 2019, 40, 833–848. [Google Scholar] [CrossRef]
- Bester, C.W.; Campbell, L.; Dragovic, A.; Collins, A.; O’Leary, S.J. Characterizing Electrocochleography in Cochlear Implant Recipients with Residual Low-Frequency Hearing. Front. Neurosci. 2017, 11, 141. [Google Scholar] [CrossRef] [Green Version]
- Sijgers, L.; Pfiffner, F.; Grosse, J.; Dillier, N.; Koka, K.; Roosli, C.; Huber, A.; Dalbert, A. Simultaneous Intra- and Extracochlear Electrocochleography During Cochlear Implantation to Enhance Response Interpretation. Trends Hear. 2021, 25, 1–13. [Google Scholar] [CrossRef]
- Koka, K.; Saoji, A.A.; Litvak, L.M. Electrocochleography in Cochlear Implant Recipients With Residual Hearing: Comparison With Audiometric Thresholds. Ear Hear. 2017, 38, e161–e167. [Google Scholar] [CrossRef]
- Fontenot, T.E.; Giardina, C.K.; Dillon, M.T.; Rooth, M.A.; Teagle, H.F.; Park, L.R.; Brown, K.D.; Adunka, O.F.; Buchman, C.A.; Pillsbury, H.C.; et al. Residual Cochlear Function in Adults and Children Receiving Cochlear Implants: Correlations with Speech Perception Outcomes. Ear Hear. 2019, 40, 577–591. [Google Scholar] [CrossRef]
- Choudhury, B.; Fitzpatrick, D.C.; Buchman, C.A.; Wei, B.P.; Dillon, M.T.; He, S.; Adunka, O.F. Intraoperative round window recordings to acoustic stimuli from cochlear implant patients. Otol. Neurotol. 2012, 33, 1507–1515. [Google Scholar] [CrossRef] [PubMed]
- Radeloff, A.; Shehata-Dieler, W.; Scherzed, A.; Rak, K.; Harnisch, W.; Hagen, R.; Mlynski, R. Intraoperative monitoring using cochlear microphonics in cochlear implant patients with residual hearing. Otol. Neurotol. 2012, 33, 348–354. [Google Scholar] [CrossRef] [PubMed]
- van Gendt, M.J.; Koka, K.; Kalkman, R.K.; Stronks, H.C.; Briaire, J.J.; Litvak, L.; Frijns, J.H.M. Simulating intracochlear electrocochleography with a combined model of acoustic hearing and electric current spread in the cochlea. J. Acoust. Soc. Am. 2020, 147, 2049. [Google Scholar] [CrossRef] [PubMed]
- Downing, M. Electrode Designs for Protection of the Delicate Cochlear Structures. J. Int. Adv. Otol. 2018, 14, 401–403. [Google Scholar] [CrossRef] [PubMed]
- Campbell, L.; Bester, C.; Iseli, C.; Sly, D.; Dragovic, A.; Gummer, A.W.; O’Leary, S. Electrophysiological Evidence of the Basilar-Membrane Travelling Wave and Frequency Place Coding of Sound in Cochlear Implant Recipients. Audiol. Neurotol. 2017, 22, 180–189. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
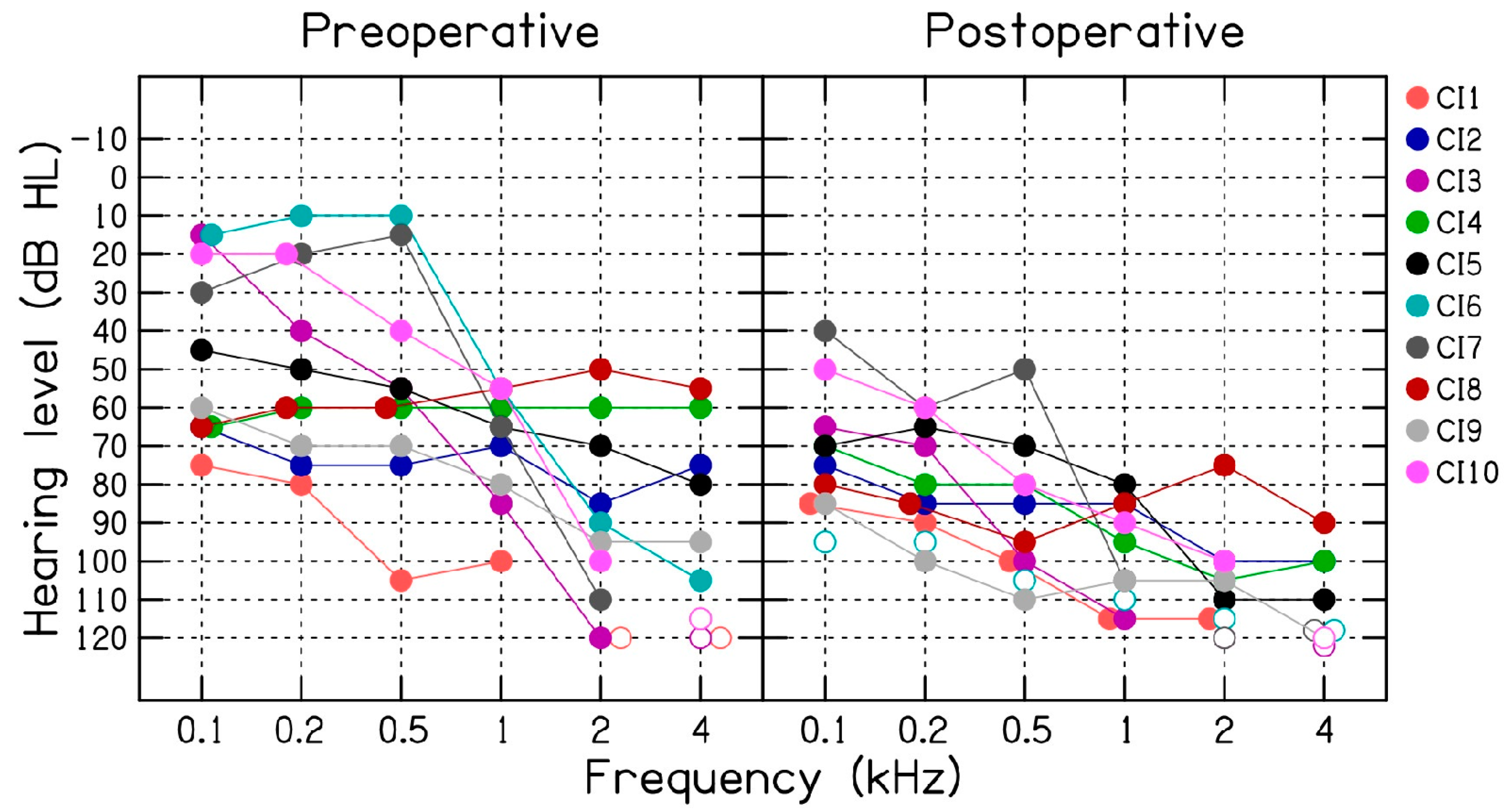
| Subjects | Age/Gender | Frequencies (Hz) | Decrease in CM (µV) | Preoperative Thresholds (dB HL) | Postoperative Thresholds (dB HL) |
|---|---|---|---|---|---|
| CI1 | 74/F | 253, 598, 1069, 2156 | 82, 91, 71, 90% | 75, 80, 105, 100, NR, NR | 85, 90, 100, 115, 115, NR |
| CI2 | 76/M | 253, 489, 743, 1015 | 13, 8, 17, 45% | 65, 75, 75, 70, 85, 75 | 75, 85, 85, 85, 100, 100 |
| CI3 | 87/M | 271, 543, 1069 | 4, 1, 0% | 15, 40, 55, 85, 120, NR | 65, 70, 100, 115, NR, NR |
| CI4 | 54/M | 253, 507, 1015, 2011 | 6, 0, 71, 95% | 65, 60, 60, 60, 60, 60 | 70, 80, 80, 95, 105, 100 |
| CI5 | 88/M | 253, 507, 1015, 2011 | 56, 6, 29, 81% | 45, 50, 55, 65, 70, 80 | 70, 65, 70, 80, 110, 110 |
| CI6 | 73/F | 253, 507, 761, 1015 | 38, 63, 83, 89% | 15, 10, 10, 55, 90, 105 | NR, NR, NR, NR, NR, NR |
| CI7 | 76/M | 253, 507, 743, 1015 | 3, 0, 6, 6% | 30, 20, 15, 65, 110, NR | 40, 60, 50, 105, NR, NR |
| CI8 | 60/F | 253, 616, 1268, 2827 | 94, 97, 98, 96% | 65, 60, 60, 55, 50, 55 | 80, 85, 95, 85, 75, 90 |
| CI9 | 72/F | 235, 507, 1015 | 52, 38, 5% | 60, 70, 70, 80, 95, 95 | 85, 100, 110, 105, 105, 120 |
| CI10 | 71/M | 253, 525, 725 | 39, 32, 57% | 20, 20, 40, 55, 100, NR | 50, 60, 80, 90, 100, NR |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saoji, A.A.; Graham, M.K.; Adkins, W.J.; Koka, K.; Carlson, M.L.; Neff, B.A.; Driscoll, C.L.W.; Fitzpatrick, D.C. Multi-Frequency Electrocochleography and Electrode Scan to Identify Electrode Insertion Trauma during Cochlear Implantation. Brain Sci. 2023, 13, 330. https://doi.org/10.3390/brainsci13020330
Saoji AA, Graham MK, Adkins WJ, Koka K, Carlson ML, Neff BA, Driscoll CLW, Fitzpatrick DC. Multi-Frequency Electrocochleography and Electrode Scan to Identify Electrode Insertion Trauma during Cochlear Implantation. Brain Sciences. 2023; 13(2):330. https://doi.org/10.3390/brainsci13020330
Chicago/Turabian StyleSaoji, Aniket A., Madison K. Graham, Weston J. Adkins, Kanthaiah Koka, Matthew L. Carlson, Brian A. Neff, Colin L. W. Driscoll, and Douglas C. Fitzpatrick. 2023. "Multi-Frequency Electrocochleography and Electrode Scan to Identify Electrode Insertion Trauma during Cochlear Implantation" Brain Sciences 13, no. 2: 330. https://doi.org/10.3390/brainsci13020330
APA StyleSaoji, A. A., Graham, M. K., Adkins, W. J., Koka, K., Carlson, M. L., Neff, B. A., Driscoll, C. L. W., & Fitzpatrick, D. C. (2023). Multi-Frequency Electrocochleography and Electrode Scan to Identify Electrode Insertion Trauma during Cochlear Implantation. Brain Sciences, 13(2), 330. https://doi.org/10.3390/brainsci13020330