
Benefits of Treadmill Training for Patients with Down Syndrome: A Systematic Review




Abstract
:1. Introduction
1.1. Health Complications Associated with Down Syndrome
1.2. Motor Development and Cognitive Function in Down Syndrome
1.3. Obesity and Alzheimer’s Disease in Down Syndrome
1.4. Treadmill Training as a Physical Therapy Method
1.5. Evaluating the Effectiveness of Treadmill Training for Down Syndrome
2. Materials and Methods
2.1. Research Question
2.2. Objectives of Systematic Review
- Determine various effects of treadmill training, alone or combined with physiotherapy among children and adults with Down syndrome;
- Assess the quality of the included RCTs using the Cochrane risk-of-bias tool for randomized trials;
- Analyze and compare the results of the selected studies.
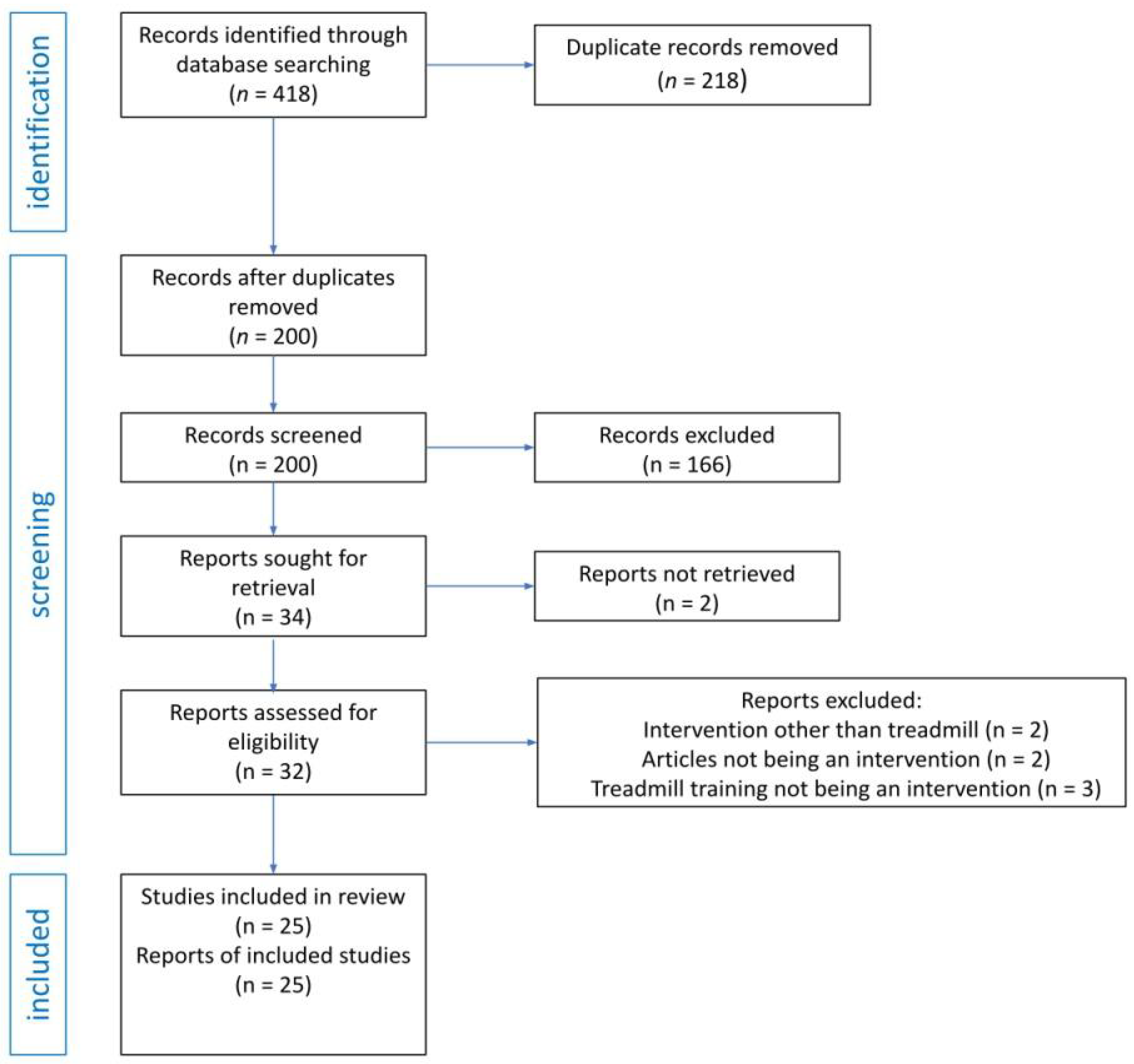
2.3. Search Strategy and Selection Process
2.4. Eligibility Criteria
- Types of studies: Randomized controlled, quasi-experimental, or clinical trial or pilot study published in English or Polish in peer-reviewed journals published from the inception of the database until 21st February 2023.
- Participants: Study participants with Down syndrome from all age groups.
- Intervention: Studies in which participants undergo treadmill training, alone or combined with physiotherapy.
- Comparison: Control groups formed only with patients with DS, who were offered only standard physiotherapy care or no therapeutic intervention.
- Outcome: In order to be included in the analysis, the study had to use a defined clinical outcome relating to mental or physical health in Down syndrome.
2.5. Risk of Bias Assessment
2.6. Data Extraction
2.7. Data Analysis
3. Results
3.1. Study Characteristics of Included Studies
3.1.1. Study Design
3.1.2. Setting
3.1.3. Participants
Characteristics
Number of Participants, Method of Recruitment, and Other Relevant Information
3.1.4. Interventions
Treadmill Training Interventions in Various Studies
Treadmill Training with Orthoses and Virtual Reality
Treadmill Training Duration and Intensity
Combining Treadmill Training with Other Physical Therapy Interventions
3.1.5. Outcome Assessment Tools
Walking Onset and Gait Patterns in Infants
Motor and Cardiovascular Function
Protein Oxidation and Plasma Leptin Levels
Executive Function, Cognitive Performance and Verbal Fluency
3.2. Outcomes
3.3. Ethical Issues Concerning Studies Involving Infants and Children
3.4. Risk of Bias
- Domain 1: Risk of bias arising from randomization process
- Domain 2: Risk of bias due to deviations from the intended interventions
- Domain 3: Risk of bias due to missing outcome data
- Domain 4: Risk of bias in measurement of the outcome
- Domain 5: Risk of bias in selection of the reported results

{kind=link}
| Randomized Controlled Trials | Domain 1 | Domain 2 | Domain 3 | Domain 4 | Domain 5 | Overall |
|---|---|---|---|---|---|---|
| Ulrich et al. (2001) [33] | Some concerns | Low risk | Low risk | Low risk | Low risk | Some concerns |
| Wu et al. (2007) [36] | Low risk | Some concerns | High risk | Low risk | Low risk | High risk |
| Looper et al. (2010) [42] | HIgh risk | High risk | High risk | Some concerns | Low risk | High risk |
| Lin et al. (2012) [47] | Low risk | Low risk | Low risk | Low risk | Low risk | Low risk |
| Ordonez et al. (2013) [46] | Some concerns | Low risk | Low risk | Low risk | Low risk | Some concerns |
| Ordonez et al. (2014) [48] | Low risk | Low risk | Low risk | Low risk | Low risk | Low risk |
| Chen et al. (2014) [50] | HIgh risk | Some concerns | Low risk | Low risk | Low risk | High risk |
| Chen et al. (2015) [52] | Some concerns | Some concerns | High risk | Low risk | Low risk | High risk |
| Alsakhawi et al. (2019) [8] | Low risk | Low risk | Low risk | Low risk | Low risk | Low risk |
| Randomized Trials with no Control | Domiain 1 | Domain 2 | Domain 3 | Domain 4 | Domain 5 | Overall |
| Wu et al. (2008) [37] | Some concerns | Low risk | Low risk | Low risk | Low risk | Some concerns |
| Ulrich et al. (2008) [38] | Some concerns | Some concerns | High risk | Low risk | Low risk | High risk |
| Angulo-Barroso et al. (2008) [39] | Some concerns | Some concerns | High risk | Low risk | Low risk | High risk |
| Angulo-Barroso, Wu et al. (2008) [40] | Low risk | Some concerns | Low risk | Low risk | Low risk | Some concerns |
| Wu et al. (2010) [43] | Low risk | Some concerns | Some concerns | Low risk | Low risk | Some concerns |
| EL-Meniawy et al. (2012) [45] | Some concerns | Low risk | Low risk | Low risk | Low risk | Some concerns |
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lukowski, A.F.; Milojevich, H.M.; Eales, L. Chapter Eight—Cognitive Functioning in Children with Down Syndrome: Current Knowledge and Future Directions. In Advances in Child Development and Behavior; Benson, J.B., Ed.; JAI: Stamford, CT, USA, 2019; Volume 56, pp. 257–289. [Google Scholar]
- Diamandopoulos, K.; Green, J. Down syndrome: An integrative review. J. Neonatal Nurs. 2018, 24, 235–241. [Google Scholar] [CrossRef]
- Asim, A.; Kumar, A.; Muthuswamy, S.; Jain, S.; Agarwal, S. “Down syndrome: An insight of the disease”. J. Biomed. Sci. 2015, 22, 41. [Google Scholar] [CrossRef]
- Antonarakis, S.E.; Skotko, B.G.; Rafii, M.S.; Strydom, A.; Pape, S.E.; Bianchi, D.W.; Sherman, S.L.; Reeves, R.H. Down syndrome. Nat. Rev. Dis. Prim. 2020, 6, 9. [Google Scholar] [CrossRef]
- Bayley, N. Manual for the Bayley Scales of Infant Development (No Title). 1969. Available online: https://cir.nii.ac.jp/crid/1130000795357934080 (accessed on 21 April 2023).
- Henderson, S. Some aspects of the development of motor control in Down’s syndrome. Themes Mot. Dev. 1986, 69–92. [Google Scholar]
- Pitetti, K.H.; Climstein, M.; Mays, M.J.; Barrett, P.J. Isokinetic arm and leg strength of adults with Down syndrome: A comparative study. Arch. Phys. Med. Rehabil. 1992, 73, 847–850. [Google Scholar]
- Alsakhawi, R.S.; Elshafey, M.A. Effect of Core Stability Exercises and Treadmill Training on Balance in Children with Down Syndrome: Randomized Controlled Trial. Adv. Ther. 2019, 36, 2364–2373. [Google Scholar] [CrossRef]
- Gustafson, G.E. Effects of the ability to locomote on infants’ social and exploratory behaviors: An experimental study. Dev. Psychol. 1984, 20, 397. [Google Scholar] [CrossRef]
- Inadera, H. The usefulness of circulating adipokine levels for the assessment of obesity-related health problems. Int. J. Med. Sci. 2008, 5, 248. [Google Scholar] [CrossRef]
- Malamud, N. Neuropathology of Organic Brain Syndromes Associated with Aging. In Aging and the Brain: The Proceedings of the Fifth Annual Symposium Held at the Texas Research Institute of Mental Sciences in Houston, October 1971; Springer: Berlin/Heidelberg, Germany, 1995; pp. 63–87. [Google Scholar]
- Leverenz, J.B.; Raskind, M.A. Early amyloid deposition in the medial temporal lobe of young Down syndrome patients: A regional quantitative analysis. Exp. Neurol. 1998, 150, 296–304. [Google Scholar] [CrossRef]
- Adams, D.; Oliver, C. The relationship between acquired impairments of executive function and behaviour change in adults with Down syndrome. J. Intellect. Disabil. Res. 2010, 54, 393–405. [Google Scholar] [CrossRef]
- Daunhauer, L.A.; Fidler, D.J.; Will, E. School function in students with Down syndrome. Am. J. Occup. Ther. 2014, 68, 167–176. [Google Scholar] [CrossRef]
- Nash, H.M.; Snowling, M.J. Semantic and phonological fluency in children with Down syndrome: Atypical organization of language or less efficient retrieval strategies? Cogn. Neuropsychol. 2008, 25, 690–703. [Google Scholar] [CrossRef]
- Mehrholz, J.; Kugler, J.; Storch, A.; Pohl, M.; Hirsch, K.; Elsner, B. Treadmill training for patients with Parkinson Disease. An abridged version of a Cochrane Review. Eur. J. Phys. Rehabil. Med. 2016, 52, 704–713. [Google Scholar]
- Tally, Z.; Boetefuer, L.; Kauk, C.; Perez, G.; Schrand, L.; Hoder, J. The efficacy of treadmill training on balance dysfunction in individuals with chronic stroke: A systematic review. Top. Stroke Rehabil. 2017, 24, 539–546. [Google Scholar] [CrossRef]
- Han, Y.-G.; Yun, C.-K. Effectiveness of treadmill training on gait function in children with cerebral palsy: Meta-analysis. J. Exerc. Rehabil. 2020, 16, 10. [Google Scholar] [CrossRef]
- Kleim, J.A.; Jones, T.A. Principles of experience-dependent neural plasticity: Implications for rehabilitation after brain damage. J. Speech Lang. Hear. Res. 2008, 51, S225–S239. [Google Scholar] [CrossRef]
- Ringenbach, S.D.; Albert, A.R.; Chen, C.-C.; Alberts, J.L. Acute bouts of assisted cycling improves cognitive and upper extremity movement functions in adolescents with Down syndrome. Ment. Retard. 2014, 52, 124–135. [Google Scholar] [CrossRef]
- Damiano, D.L.; DeJong, S.L. A systematic review of the effectiveness of treadmill training and body weight support in pediatric rehabilitation. J. Neurol. Phys. Ther. 2009, 33, 27–44. [Google Scholar] [CrossRef]
- Valentín-Gudiol, M.; Mattern-Baxter, K.; Girabent-Farrés, M.; Bagur-Calafat, C.; Hadders-Algra, M.; Angulo-Barroso, R.M. Treadmill interventions in children under six years of age at risk of neuromotor delay. Cochrane Database Syst. Rev. 2017, 2017, CD009242. [Google Scholar] [CrossRef]
- Paleg, G.; Romness, M.; Livingstone, R. Interventions to improve sensory and motor outcomes for young children with central hypotonia: A systematic review. J. Pediatr. Rehabil. Med. 2018, 11, 57–70. [Google Scholar] [CrossRef]
- Valentin-Gudiol, M.; Bagur-Calafat, C.; Girabent-Farrés, M.; Hadders-Algra, M.; Mattern-Baxter, K.; Angulo-Barroso, R. Treadmill interventions with partial body weight support in children under six years of age at risk of neuromotor delay: A report of a Cochrane systematic review and meta-analysis. Eur. J. Phys. Rehabil. Med. 2013, 49, 67–91. [Google Scholar]
- Pino-Ramos, G.-D.; Romero-Galisteo, R.P.; Pinero-Pinto, E.; Lirio-Romero, C.; Palomo-Carrión, R. Eficacia de la marcha en cinta rodante sobre el desarrollo motor de niños con parálisis cerebral y síndrome de down. Medicina 2021, 81, 367–374. [Google Scholar]
- Andriolo, R.B.; El Dib, R.; Ramos, L.; Atallah, Á.N.; da Silva, E.M. Aerobic exercise training programmes for improving physical and psychosocial health in adults with Down syndrome. Cochrane Database Syst. Rev. 2005. [Google Scholar]
- Zwicker, J.G.; Mayson, T.A. Effectiveness of treadmill training in children with motor impairments: An overview of systematic reviews. Pediatr. Phys. Ther. 2010, 22, 361–377. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef]
- Sterne, J.A.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2019. [Google Scholar]
- Ulrich, B.D.; Ulrich, D.A.; Collier, D.H. Alternating stepping patterns: Hidden abilities of 11-month-old infants with Down syndrome. Dev. Med. Child Neurol. 1992, 34, 233–239. [Google Scholar] [CrossRef]
- Ulrich, B.D.; Ulrich, D.A.; Collier, D.H.; Cole, E.L. Developmental shifts in the ability of infants with Down syndrome to produce treadmill steps. Phys. Ther. 1995, 75, 14–23. [Google Scholar] [CrossRef]
- Ulrich, D.A.; Ulrich, B.D.; Angulo-Kinzler, R.M.; Yun, J. Treadmill training of infants with Down syndrome: Evidence-based developmental outcomes. Pediatrics 2001, 108, E84. [Google Scholar] [CrossRef]
- Carmeli, E.; Kessel, S.; Coleman, R.; Ayalon, M. Effects of a treadmill walking program on muscle strength and balance in elderly people with Down syndrome. J. Gerontol. A Biol. Sci. Med. Sci. 2002, 57, M106–M110. [Google Scholar] [CrossRef]
- Carmeli, E.; Barchad, S.; Masharawi, Y.; Coleman, R. Impact of a walking program in people with down syndrome. J. Strength Cond. Res. 2004, 18, 180–184. [Google Scholar]
- Wu, J.; Looper, J.; Ulrich, B.D.; Ulrich, D.A.; Angulo-Barroso, R.M. Exploring effects of different treadmill interventions on walking onset and gait patterns in infants with Down syndrome. Dev. Med. Child Neurol. 2007, 49, 839–845. [Google Scholar] [CrossRef]
- Wu, J.; Ulrich, D.A.; Looper, J.; Tiernan, C.W.; Angulo-Barroso, R.M. Strategy adoption and locomotor adjustment in obstacle clearance of newly walking toddlers with Down syndrome after different treadmill interventions. Exp. Brain Res. 2008, 186, 261–272. [Google Scholar] [CrossRef]
- Ulrich, D.A.; Lloyd, M.C.; Tiernan, C.W.; Looper, J.E.; Angulo-Barroso, R.M. Effects of intensity of treadmill training on developmental outcomes and stepping in infants with Down syndrome: A randomized trial. Phys. Ther. 2008, 88, 114–122. [Google Scholar] [CrossRef]
- Angulo-Barroso, R.; Burghardt, A.R.; Lloyd, M.; Ulrich, D.A. Physical activity in infants with Down syndrome receiving a treadmill intervention. Infant Behav. Dev. 2008, 31, 255–269. [Google Scholar] [CrossRef]
- Angulo-Barroso, R.M.; Wu, J.; Ulrich, D.A. Long-term effect of different treadmill interventions on gait development in new walkers with Down syndrome. Gait Posture 2008, 27, 231–238. [Google Scholar] [CrossRef]
- Mendonca, G.V.; Pereira, F.D. Influence of long-term exercise training on submaximal and peak aerobic capacity and locomotor economy in adult males with Down’s syndrome. Med. Sci. Monit. 2009, 15, Cr33–Cr39. [Google Scholar]
- Looper, J.; Ulrich, D.A. Effect of treadmill training and supramalleolar orthosis use on motor skill development in infants with Down syndrome: A randomized clinical trial. Phys. Ther. 2010, 90, 382–390. [Google Scholar] [CrossRef]
- Wu, J.; Looper, J.; Ulrich, D.A.; Angulo-Barroso, R.M. Effects of various treadmill interventions on the development of joint kinematics in infants with Down syndrome. Phys. Ther. 2010, 90, 1265–1276. [Google Scholar] [CrossRef]
- Ordonez, F.J.; Rosety, I.; Rosety, M.A.; Camacho-Molina, A.; Fornieles, G.; Rosety, M.; Rosety-Rodriguez, M. Aerobic training at moderate intensity reduced protein oxidation in adolescents with Down syndrome. Scand. J. Med. Sci. Sports 2012, 22, 91–94. [Google Scholar] [CrossRef]
- El-Meniawy, G.H.; Kamal, H.M.; Elshemy, S.A. Role of treadmill training versus suspension therapy on balance in children with Down syndrome. Egypt. J. Med. Hum. Genet. 2012, 13, 37–43. [Google Scholar] [CrossRef]
- Ordoñez, F.J.; Fornieles-Gonzalez, G.; Camacho, A.; Rosety, M.A.; Rosety, I.; Diaz, A.J.; Rosety-Rodriguez, M. Anti-inflammatory effect of exercise, via reduced leptin levels, in obese women with Down syndrome. Int. J. Sport Nutr. Exerc. Metab. 2013, 23, 239–244. [Google Scholar] [CrossRef]
- Lin, H.C.; Wuang, Y.P. Strength and agility training in adolescents with Down syndrome: A randomized controlled trial. Res. Dev. Disabil. 2012, 33, 2236–2244. [Google Scholar] [CrossRef]
- Ordonez, F.J.; Rosety, M.A.; Camacho, A.; Rosety, I.; Diaz, A.J.; Fornieles, G.; Garcia, N.; Rosety-Rodriguez, M. Aerobic training improved low-grade inflammation in obese women with intellectual disability. J. Intellect. Disabil. Res. 2014, 58, 583–590. [Google Scholar] [CrossRef]
- Rodenbusch, T.L.; Ribeiro, T.S.; Simão, C.R.; Britto, H.M.; Tudella, E.; Lindquist, A.R. Effects of treadmill inclination on the gait of children with Down syndrome. Res. Dev. Disabil. 2013, 34, 2185–2190. [Google Scholar] [CrossRef]
- Chen, C.C.; Ringenbach, D.R.; Snow, M. Treadmill walking effects on grip strength in young men with Down syndrome. Res. Dev. Disabil. 2014, 35, 288–293. [Google Scholar] [CrossRef]
- Rosety-Rodriguez, M.; Diaz, A.J.; Rosety, I.; Rosety, M.A.; Camacho, A.; Fornieles, G.; Rosety, M.; Ordonez, F.J. Exercise reduced inflammation: But for how long after training? J. Intellect. Disabil. Res. 2014, 58, 874–879. [Google Scholar] [CrossRef]
- Chen, C.C.; Ringenbach, S.D.; Crews, D.; Kulinna, P.H.; Amazeen, E.L. The association between a single bout of moderate physical activity and executive function in young adults with Down syndrome: A preliminary study. J. Intellect. Disabil. Res. 2015, 59, 589–598. [Google Scholar] [CrossRef]
- Chen, C.C.; Ringenbach, S.D. Dose-response relationship between intensity of exercise and cognitive performance in individuals with Down syndrome: A preliminary study. J. Intellect. Disabil. Res. 2016, 60, 606–614. [Google Scholar] [CrossRef]
- Chen, C.J.J.; Ringenbach, S.D.R. The effect of acute exercise on the performance of verbal fluency in adolescents and young adults with Down syndrome: A pilot study. J. Intellect. Disabil. Res. 2019, 63, 614–623. [Google Scholar] [CrossRef]
- Paul, Y.; Ellapen, T.J.; Barnard, M.; Hammill, H.V.; Swanepoel, M. The health benefits of exercise therapy for patients with Down syndrome: A systematic review. Afr. J. Disabil. 2019, 8, 576. [Google Scholar] [CrossRef]
- Naczk, A.; Gajewska, E.; Naczk, M. Effectiveness of Swimming Program in Adolescents with Down Syndrome. Int. J. Environ. Res. Public Health 2021, 18, 7441. [Google Scholar] [CrossRef]
- Ringenbach, S.D.; Holzapfel, S.D.; Mulvey, G.M.; Jimenez, A.; Benson, A.; Richter, M. The effects of assisted cycling therapy (ACT) and voluntary cycling on reaction time and measures of executive function in adolescents with Down syndrome. J. Intellect. Disabil. Res. 2016, 60, 1073–1085. [Google Scholar] [CrossRef]

| No. | Study | Duration | Design | Intervention | Age | Co-Morbidities |
|---|---|---|---|---|---|---|
| 1 | Ulrich et al. (1992) [31] | 11 months | Single group design | Supported treadmill stepping for infants with DS | 7 months | Congenital heart defects (n = 5) |
| 2 | Ulrich et al. (1995) [32] | 4–21 months | Single group design | Longitudinal supported treadmill stepping for infants with DS | 8–11 months | Congenital heart defects (n = 5) |
| 3 | Ulrich et al. (2001) [33] | Until independent walking | Randomized controlled trial | Treadmill stepping practice for infants with DS | 307.4 days | Congenital heart disease requiring surgery (SG: n = 7, CG: n = 2) |
| 4 | Carmeli et al. (2002) [34] | 6 months | Parallel group design | Treadmill walking program for adults with DS | 63 years | SG: Cardiac disease (n = 2) |
| 5 | Carmeli et al. (2004) [35] | 15 weeks | Parallel group design | Treadmill walking program for ID adults with arterial occlusive disease | SG: 65.5 years, CG: 62 years | Arterial occlusive disease |
| 6 | Wu et al. (2007) [36] | Until 3 independent steps + 1 and 3-month follow-up | Randomized controlled trial | Different treadmill interventions for infants with DS | SG: LG—21.4 months, HI—19.2 months, CG: 23.9 months | Not reported |
| 7 | Wu et al. (2008 [37]) | LG group—11 months, HI group—9.6 months + 1-year follow-up | Randomized trial (no control) | Treadmill interventions for newly walking toddlers with DS | HI group: 9.65 months, LG group: 10.40 months | Not reported |
| 8 | Ulrich et al. (2008) [38] | Until 3 independent steps | Randomized trial (no control) | Individualized, progressively intense treadmill training for infants with DS | HI group: 9.65 months, LG group: 10.40 months | Congenital heart defects (HI: n = 8, LG: n = 6) |
| 9 | Angulo-Barroso et al. (2008) [39] | 15 months + 1-year follow-up | Randomized trial (no control) | Higher intensity, individualized TMT protocol for infants with DS | HI group: 9.65 months, LG group: 10.40 months | Not reported |
| 10 | Angulo-Barroso, Wu et al. (2008) [40] | 15 months + 1-year follow-up | Randomized trial (no control) | Long-term effect of different treadmill interventions on gait patterns in infants with DS | HI group: 9.7 months, LG group: 10.40 months | Not reported |
| 11 | Mendonca et al. (2009) [41] | 12 + 28 weeks | Single group design | 28-week training program for DS males to improve aerobic capacity and locomotor economy | 34.5 years | Not reported |
| 12 | Looper et al. (2010) [42] | Until 3 independent steps + 1-month follow-up | Randomized controlled trial | Early orthosis use combined with treadmill training in infants with DS vs. treadmill training alone | SG: 578 days, CG: 642 days | Not reported |
| 13 | Wu et al. (2010) [43] | Until 3 independent steps + 1-year gait follow-up | Randomized trial (no control) | Different treadmill interventions on joint kinematic patterns in infants with DS | LG: 35.7 months, HI: 75 months | Not reported |
| 14 | Ordonez et al. (2010) [44] | 12-week training | Parallel group design with matched control | Aerobic training for reducing protein oxidation | 16.3 years | Not reported |
| 15 | El- Meniawy et al. (2012) [45] | 3 months intervention + 3-month follow-up | Randomized trial (no control) | Treadmill training vs. suspension therapy on balance in children with DS | 9.34 years | Not reported |
| 16 | Ordonez et al. (2013) [46] | 10-week aerobic training program | Randomized controlled trial | Aerobic training on plasma adipokines in obese women with DS | EG: 24.7 years, CG: 25.1 years | Obesity, mild ID |
| 17 | Lin et al. (2012) [47] | 6-week program + 6-week follow-up | Randomized controlled trial | Strength and agility training for adolescents with DS | SG: 10.6 years, CG: 11.2 years | Not reported |
| 18 | Ordonez et al. (2014) [48] | 10-week aerobic training program | Randomized controlled trial | Aerobic training on pro-inflammatory cytokines and acute phase proteins in women with DS | EG: 24.7 years, CG: 25.1 years | Obesity |
| 19 | Rodenbusch et al. (2013) [49] | Only intervention | Single group design | Effects of upward treadmill inclination on gait of children with DS | 8.43 years | Not reported |
| 20 | Chen et al. (2014) [50] | ~20 min (only intervention) | Randomized controlled trial | Relation between grip strength, anthropometric factors, and aerobic exercise impact on grip strength in young men with DS | EG: 21.76 years, CG: 17.77 years | Not reporte |
| 21 | Rosety-Rodriguez et al. (2014) [51] | 10-week aerobic training program + 6-month follow-up | Parallel group design with matched control | Reduced inflammation effects maintenance after aerobic program completion | EG: 24.7 years, CG: 25.1 years | Obesity, mild ID |
| 22 | Chen et al. (2015) [52] | ~20 min (only intervention) | Randomized controlled trial | Impact of single exercise intervention on executive function in young adults with DS | EG: 23.45 years, CG: 20.58 years | Not reported |
| 23 | Chen et al. (2016) [53] | ~20 min (only intervention) | Parallel group design with matched control | Dose-response relationship between acute exercise intensity and cognitive performance | MI: 23.7 years, HI: 22.10 years, CG: 19.11 years | Not reported |
| 24 | Chen et al. (2019) [54] | ~20 min intervention + 5–10 min rest + ~1.5 h verbal tests | Parallel group design with matched control | Relationship between acute exercise and verbal fluency | MI: 21.42 years, HI: 22.70 years, CG: 20.58 years | Not reported |
| 25 | Alsakhawi et al. (2019) [8] | 4 months | Randomized controlled trial | Core stability training vs. treadmill exercises on balance in children with DS | 4.59 years | Not reported |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kamińska, K.; Ciołek, M.; Krysta, K.; Krzystanek, M. Benefits of Treadmill Training for Patients with Down Syndrome: A Systematic Review. Brain Sci. 2023, 13, 808. https://doi.org/10.3390/brainsci13050808
Kamińska K, Ciołek M, Krysta K, Krzystanek M. Benefits of Treadmill Training for Patients with Down Syndrome: A Systematic Review. Brain Sciences. 2023; 13(5):808. https://doi.org/10.3390/brainsci13050808
Chicago/Turabian StyleKamińska, Karolina, Michał Ciołek, Krzysztof Krysta, and Marek Krzystanek. 2023. "Benefits of Treadmill Training for Patients with Down Syndrome: A Systematic Review" Brain Sciences 13, no. 5: 808. https://doi.org/10.3390/brainsci13050808
APA StyleKamińska, K., Ciołek, M., Krysta, K., & Krzystanek, M. (2023). Benefits of Treadmill Training for Patients with Down Syndrome: A Systematic Review. Brain Sciences, 13(5), 808. https://doi.org/10.3390/brainsci13050808