
Etomidate versus Propofol for Electroconvulsive Therapy in Patients with Major Depressive Disorders in Terms of Clinical Responses to Treatment: A Retrospective Analysis
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
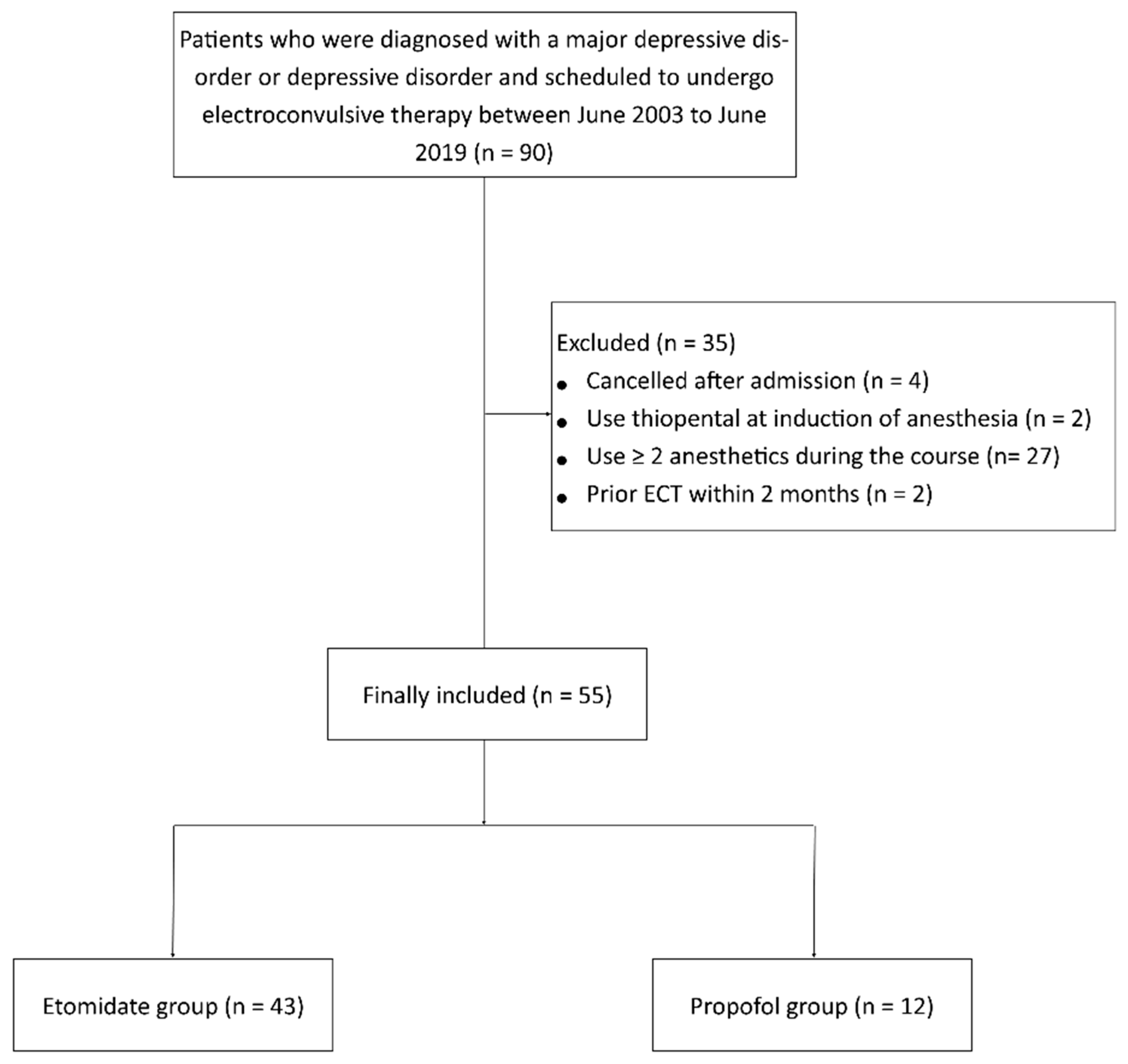
2.1. Study Design and Study Participants
2.2. Anesthesia for ECT
2.3. Outcomes
2.4. Statistical Analyses
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hoyer, C.; Kranaster, L.; Janke, C.; Sartorius, A. Impact of the anesthetic agents ketamine, etomidate, thiopental, and propofol on seizure parameters and seizure quality in electroconvulsive therapy: A retrospective study. Eur. Arch. Psychiatry Clin. Neurosci. 2014, 264, 255–261. [Google Scholar] [CrossRef] [PubMed]
- MacEwan, T. An audit of seizure duration in electroconvulsive therapy. Psychiatr. Bull. 2002, 26, 337–339. [Google Scholar] [CrossRef] [Green Version]
- McClintock, S.M.; Choi, J.; Deng, Z.D.; Appelbaum, L.G.; Krystal, A.D.; Lisanby, S.H. Multifactorial determinants of the neurocognitive effects of electroconvulsive therapy. J. ECT 2014, 30, 165–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdollahi, M.H.; Izadi, A.; Hajiesmaeili, M.R.; Ghanizadeh, A.; Dastjerdi, G.; Hosseini, H.A.; Ghiamat, M.M.; Abbasi, H.R. Effect of etomidate versus thiopental on major depressive disorder in electroconvulsive therapy, a randomized double-blind controlled clinical trial. J. ECT 2012, 28, 10–13. [Google Scholar] [CrossRef] [PubMed]
- Reddy, S.D.; Reddy, D.S. Midazolam as an anticonvulsant antidote for organophosphate intoxication--A pharmacotherapeutic appraisal. Epilepsia 2015, 56, 813–821. [Google Scholar] [CrossRef] [Green Version]
- Uppal, V.; Dourish, J.; Macfarlane, A. Anaesthesia for electroconvulsive therapy. Contin. Educ. Anaesth. Crit. Care Pain. 2010, 10, 192–196. [Google Scholar] [CrossRef] [Green Version]
- Singh, P.M.; Arora, S.; Borle, A.; Varma, P.; Trikha, A.; Goudra, B.G. Evaluation of etomidate for seizure duration in electroconvulsive therapy: A systematic review and meta-analysis. J. ECT 2015, 31, 213–225. [Google Scholar] [CrossRef]
- Coffey, C.E.; Lucke, J.; Weiner, R.D.; Krystal, A.D.; Aque, M. Seizure threshold in electroconvulsive therapy: I. Initial seizure threshold. Biol. Psychiatry 1995, 37, 713–720. [Google Scholar] [CrossRef]
- Busner, J.; Targum, S.D. The clinical global impressions scale: Applying a research tool in clinical practice. Psychiatry 2007, 4, 28–37. [Google Scholar]
- Pinna, F.; Deriu, L.; Diana, E.; Perra, V.; Randaccio, R.P.; Sanna, L.; Tusconi, M.; Carpiniello, B.; Cagliari Recovery Study Group. Clinical Global impression-severity score as a reliable measure for routine evaluation of remission in schizophrenia and schizoaffective disorders. Ann. Gen. Psychiatry 2015, 14, 6. [Google Scholar] [CrossRef] [Green Version]
- Kolevzon, A.; Ventola, P.; Keary, C.J.; Heimer, G.; Neul, J.L.; Adera, M.; Jaeger, J. Development of an adapted Clinical Global impression scale for use in Angelman syndrome. J. Neurodev. Disord. 2021, 13, 3. [Google Scholar] [CrossRef]
- Forkmann, T.; Scherer, A.; Boecker, M.; Pawelzik, M.; Jostes, R.; Gauggel, S. The Clinical Global impression Scale and the influence of patient or staff perspective on outcome. BMC Psychiatry 2011, 11, 83. [Google Scholar] [CrossRef] [Green Version]
- Eranti, S.V.; Mogg, A.J.; Pluck, G.C.; Landau, S.; McLoughlin, D.M. Methohexitone, propofol and etomidate in electroconvulsive therapy for depression: A naturalistic comparison study. J. Affect. Disord. 2009, 113, 165–171. [Google Scholar] [CrossRef]
- Graveland, P.E.; Wierdsma, A.I.; van den Broek, W.W.; Birkenhäger, T.K. A retrospective comparison of the effects of propofol and etomidate on stimulus variables and efficacy of electroconvulsive therapy in depressed inpatients. Prog. Neuropsychopharmacol. Biol. Psychiatry 2013, 45, 230–235. [Google Scholar] [CrossRef]
- Spielmans, G.I.; McFall, J.P. A comparative meta-analysis of Clinical Global Impressions change in antidepressant trials. J. Nerv. Ment. Dis. 2006, 194, 845–852. [Google Scholar] [CrossRef]
- Khan, A.; Khan, S.R.; Shankles, E.B.; Polissar, N.L. Relative sensitivity of the Montgomery-Asberg Depression Rating Scale, the Hamilton Depression rating scale and the Clinical Global Impressions rating scale in antidepressant clinical trials. Int. Clin. Psychopharmacol. 2002, 17, 281–285. [Google Scholar] [CrossRef]
- Jindal, S.; Sidhu, G.K.; Kumari, S.; Kamboj, P.; Chauhan, R. Etomidate versus Propofol for Motor Seizure Duration during Modified Electroconvulsive Therapy. Anesth. Essays Res. 2020, 14, 62–67. [Google Scholar]
- Gurel, S.C.; Ozden, H.C.; Karahan, S.; Ayhan, Y. The superiority of ketofol and etomidate against propofol or thiopental anesthesia for ECT. Asian J Psychiatr. 2022, 72, 103090. [Google Scholar] [CrossRef]
- Kadiyala, P.K.; Kadiyala, L.D. Anaesthesia for electroconvulsive therapy: An overview with an update on its role in potentiating electroconvulsive therapy. Indian J. Anaesth. 2017, 61, 373–380. [Google Scholar] [CrossRef]
- Voss, L.J.; Sleigh, J.W.; Barnard, J.P.M.; Kirsch, H.E. The howling cortex: Seizures and general anesthetic drugs. Anesth. Analg. 2008, 107, 1689–1703. [Google Scholar] [CrossRef] [Green Version]
- Baker, M.T. The anticonvulsant effects of propofol and a propofol analog, 2,6-diisopropyl-4-(1-hydroxy-2,2,2-trifluoroethyl) phenol, in a 6-Hz partial seizure model. Anesth. Analg. 2011, 112, 340–344. [Google Scholar] [CrossRef] [PubMed]
- Erdil, F.; Demirbilek, S.; Begec, Z.; Ozturk, E.; Ersoy, M.O. Effects of propofol or etomidate on QT interval during electroconvulsive therapy. J. ECT 2009, 25, 174–177. [Google Scholar] [CrossRef] [PubMed]
- Gazdag, G.; Kocsis, N.; Tolna, J.; Iványi, Z. Etomidate versus propofol for electroconvulsive therapy in patients with schizophrenia. J. ECT 2004, 20, 225–229. [Google Scholar] [CrossRef] [PubMed]
- Mehta, D.; Palta, S.; Gupta, N.; Saroa, R. Comparison of effect of etomidate with propofol on hemodynamics during modified electroconvulsive therapy. J. Anaesthesiol. Clin. Pharmacol. 2022, 38, 104–110. [Google Scholar]
- Ding, Z.; White, P.F. Anesthesia for electroconvulsive therapy. Anesth. Analg. 2002, 94, 1351–1364. [Google Scholar] [CrossRef]
- Su, P.; Pan, J.Z. Anesthesia for Electroconvulsive Therapy. In Anesthesiology: A Practical Approach; Goudra, B.G., Ed.; Springer International Publishing: Cham/Geneva, Switzerland, 2018; pp. 229–238. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | Etomidate (n = 43) | Propofol (n = 12) | p Value |
|---|---|---|---|
| Age, years | 66.2 ± 11.5 | 63.8 ± 10.4 | 0.516 |
| Female sex, n (%) | 32 (74.4%) | 10 (83.3%) | 0.709 |
| BMI, kg/m2 | 23.4 ± 3.6 | 21.7 ± 2.3 | 0.063 |
| Drug treatment | |||
| SSRI, n (%) | 22 (51.2%) | 11 (91.7%) | 0.018 * |
| SNRI, n (%) | 17 (39.5%) | 5 (41.7%) | 0.894 |
| TCA, n (%) | 15 (34.9%) | 6 (50.0%) | 0.341 |
| NDRI, n (%) | 6 (14.0%) | 1 (8.3%) | 1.000 |
| BDZ, n (%) | 34 (79.1%) | 11 (91.7%) | 0.430 |
| Antipsychotics, n (%) | 31 (72.1%) | 10 (83.3 %) | 0.709 |
| Baseline hemodynamic parameter | |||
| Heart rate, /min | 90.4 ± 10.4 | 93.7 ± 10.2 | 0.325 |
| Systolic blood pressure, mmHg | 136.7 ± 12.8 | 138.0 ± 12.2 | 0.863 |
| Diastolic blood pressure, mmHg | 81.4 ± 9.7 | 79.7 ± 7.1 | 0.580 |
| Mean blood pressure, mmHg | 96.2 ± 9.6 | 97.2 ± 8.3 | 0.740 |
| Etomidate (n = 43) | Propofol (n = 12) | p Value | |
|---|---|---|---|
| Mood | 0.530 | ||
| Euthymic | 28 (65.1%) | 10 (83.3%) | |
| Mild depressive | 12 (27.9%) | 2 (16.7%) | |
| Moderate depressive | 3 (7.0%) | 0 | |
| Remission | 0.199 | ||
| Full remission | 6 (14.0%) | 4 (33.3%) | |
| Partial remission | 37 (86.0%) | 8 (66.7%) | |
| Length of hospital stay | 30 [24, 39] | 37 [23.5, 50.5] | 0.380 |
| Side effect | |||
| Amnesia | 13 (30.2%) | 4 (33.3%) | 1.000 |
| Headache | 1 (2.3%) | 1 (8.3%) | 0.392 |
| Anxiety | 0 | 2 (16.7%) | 0.044 * |
| Insomnia | 0 | 1 (8.3%) | 0.218 |
| Variables | Etomidate (n = 43) | Propofol (n = 12) | p Value |
|---|---|---|---|
| Number of ECT | 7.6 ± 2.2 | 10.0 ± 3.2 | 0.004 * |
| Mean motor seizure (s) | 42.0 [36.8, 51.4] | 23.65 [22.65, 28.5] | <0.001 * |
| Mean EEG seizure (s) | 51.8 [44.15, 56.2] | 33.5 [31.3, 37.825] | <0.001 * |
| Mean stimulus charge (mC) | 211.2 [165.4, 286.65] | 394.75 [293.5, 660.8] | 0.001 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoon, I.-Y.; Ryu, J.-H.; Do, S.-H.; Min, B.; Koo, C.-H. Etomidate versus Propofol for Electroconvulsive Therapy in Patients with Major Depressive Disorders in Terms of Clinical Responses to Treatment: A Retrospective Analysis. Brain Sci. 2023, 13, 1023. https://doi.org/10.3390/brainsci13071023
Yoon I-Y, Ryu J-H, Do S-H, Min B, Koo C-H. Etomidate versus Propofol for Electroconvulsive Therapy in Patients with Major Depressive Disorders in Terms of Clinical Responses to Treatment: A Retrospective Analysis. Brain Sciences. 2023; 13(7):1023. https://doi.org/10.3390/brainsci13071023
Chicago/Turabian StyleYoon, In-Young, Jung-Hee Ryu, Sang-Hwan Do, Beomjun Min, and Chang-Hoon Koo. 2023. "Etomidate versus Propofol for Electroconvulsive Therapy in Patients with Major Depressive Disorders in Terms of Clinical Responses to Treatment: A Retrospective Analysis" Brain Sciences 13, no. 7: 1023. https://doi.org/10.3390/brainsci13071023
APA StyleYoon, I. -Y., Ryu, J. -H., Do, S. -H., Min, B., & Koo, C. -H. (2023). Etomidate versus Propofol for Electroconvulsive Therapy in Patients with Major Depressive Disorders in Terms of Clinical Responses to Treatment: A Retrospective Analysis. Brain Sciences, 13(7), 1023. https://doi.org/10.3390/brainsci13071023