

Alteration of Excitation/Inhibition Imbalance in the Hippocampus and Amygdala of Drug-Resistant Epilepsy Patients Treated with Acute Vagus Nerve Stimulation
 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
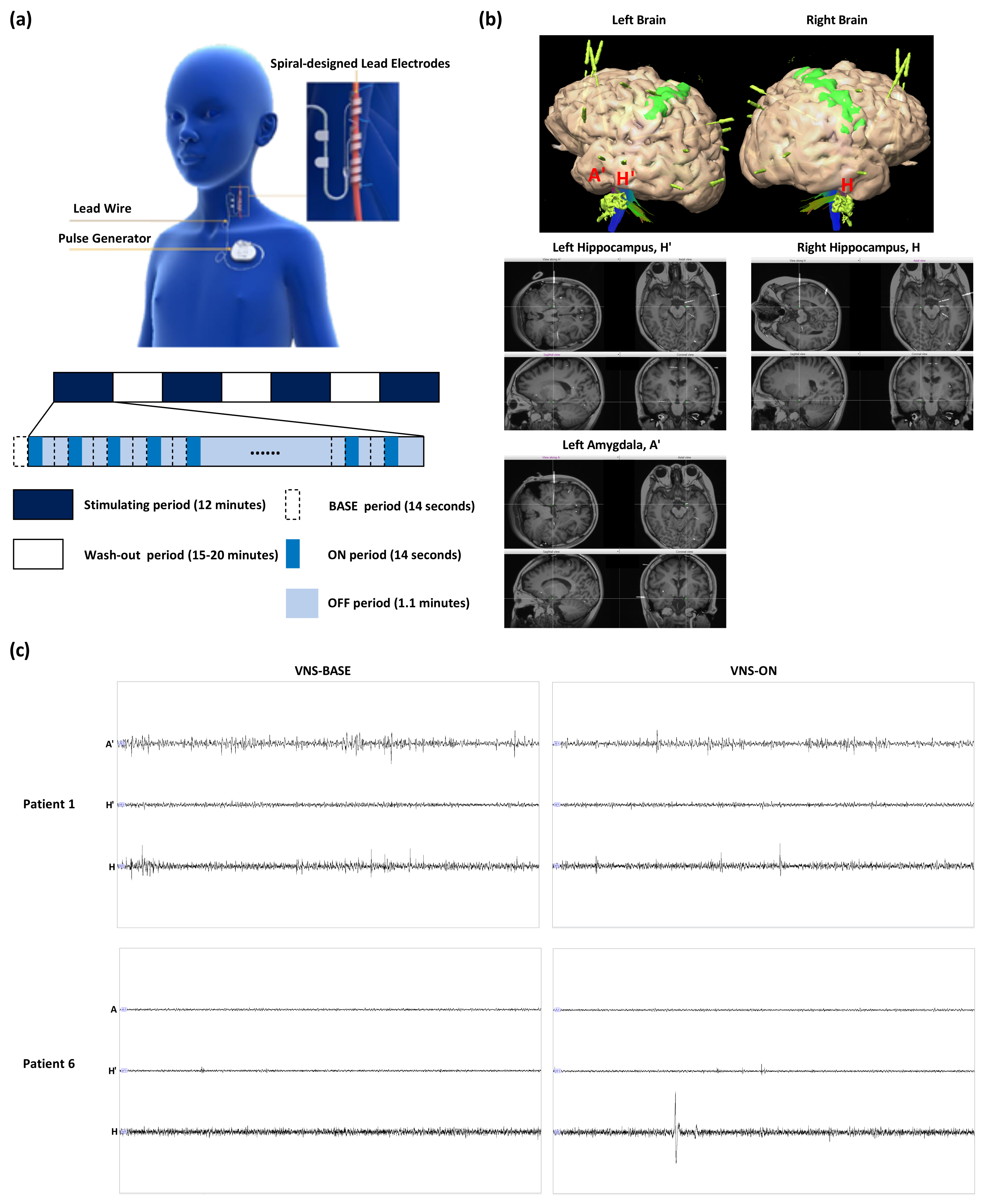
2.2. Vagus Nerve Stimulation
2.3. SEEG Electrode Implantation and Data Acquisition
2.4. 1/f Power Slope Estimation
2.5. Statistical Analysis
3. Results
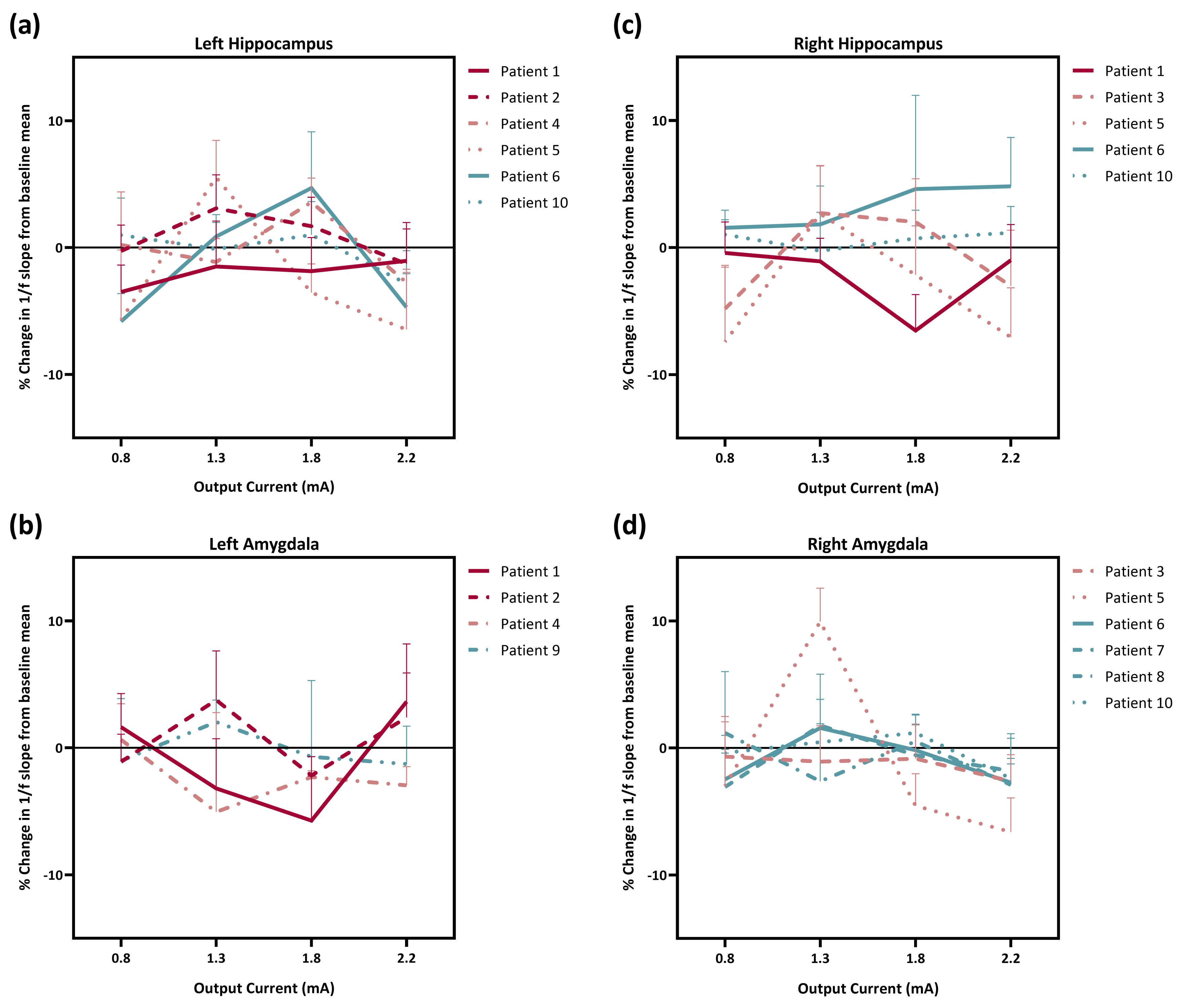
3.1. Effect of Different Stimulation Amplitudes on the Regulation of E/I Imbalance
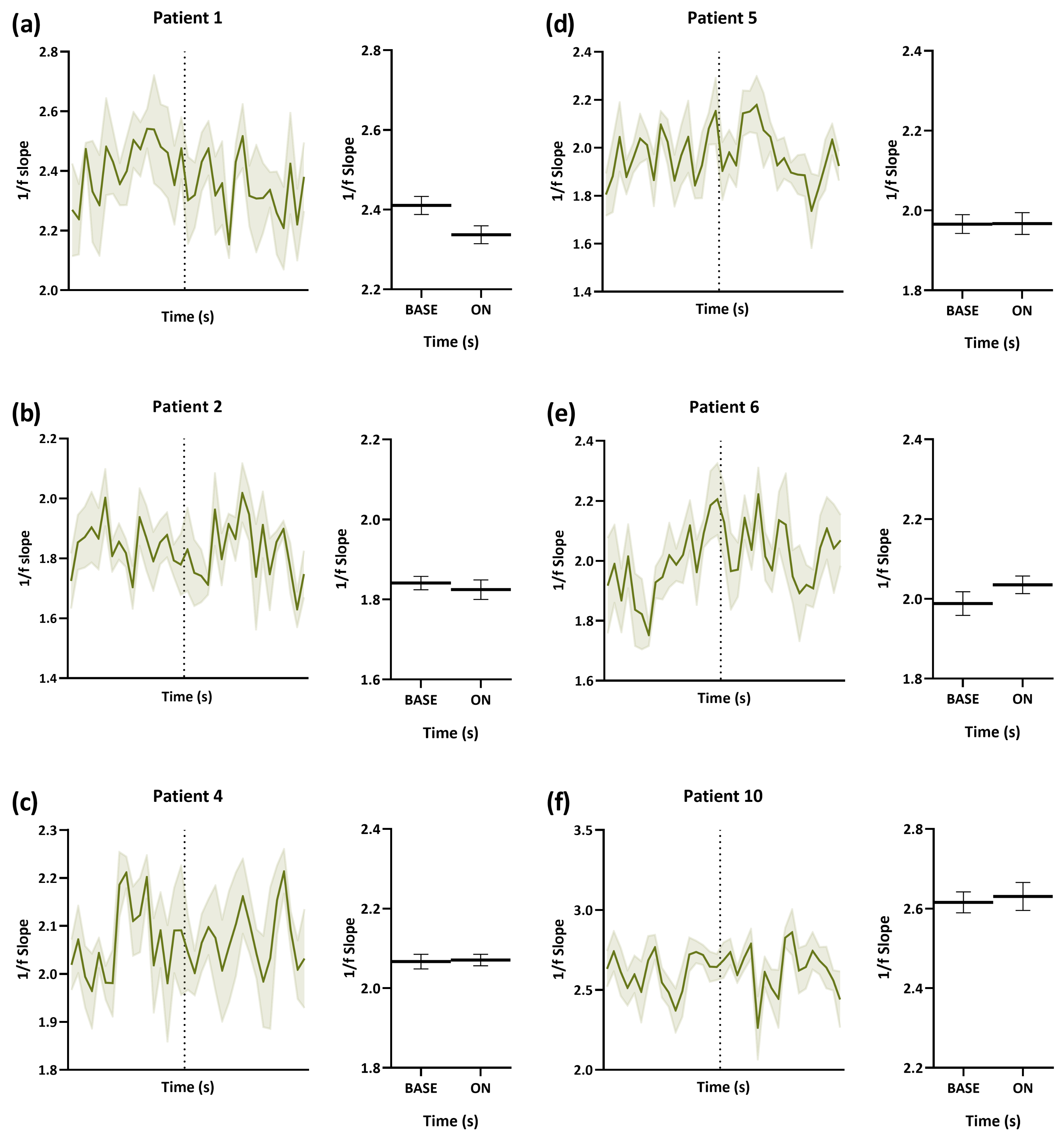
3.2. Dynamic Change in E/I from VNS-BASE to VNS-ON
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sillito, A. The contribution of inhibitory mechanisms to the receptive field properties of neurones in the striate cortex of the cat. J. Physiol. 1975, 250, 305–329. [Google Scholar] [CrossRef] [PubMed]
- Vogels, T.P.; Abbott, L. Gating multiple signals through detailed balance of excitation and inhibition in spiking networks. Nat. Neurosci. 2009, 12, 483–491. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, S.; Goldman, M.S. Balanced cortical microcircuitry for maintaining information in working memory. Nat. Neurosci. 2013, 16, 1306–1314. [Google Scholar] [CrossRef] [PubMed]
- Jedlicka, P.; Muellerleile, J.; Schwarzacher, S.W. Synaptic plasticity and excitation-inhibition balance in the dentate gyrus: Insights from in vivo recordings in Neuroligin-1, Neuroligin-2, and collybistin knockouts. Neural Plast. 2018, 2018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oberman, L.M. mGluR antagonists and GABA agonists as novel pharmacological agents for the treatment of autism spectrum disorders. Expert Opin. Investig. Drugs 2012, 21, 1819–1825. [Google Scholar] [CrossRef]
- Buzsaki, G.; Draguhn, A. Neuronal oscillations in cortical networks. Science 2004, 304, 1926–1929. [Google Scholar] [CrossRef] [Green Version]
- González-Ramírez, L.R.; Ahmed, O.J.; Cash, S.S.; Wayne, C.E.; Kramer, M.A. A biologically constrained, mathematical model of cortical wave propagation preceding seizure termination. PLoS Comput. Biol. 2015, 11, e1004065. [Google Scholar] [CrossRef]
- Engel, J. Excitation and inhibition in epilepsy. Can. J. Neurol. Sci. 1996, 23, 167–174. [Google Scholar] [CrossRef] [Green Version]
- Uhlhaas, P.J.; Singer, W. Abnormal neural oscillations and synchrony in schizophrenia. Nat. Rev. Neurosci. 2010, 11, 100–113. [Google Scholar] [CrossRef]
- Dani, V.S.; Chang, Q.; Maffei, A.; Turrigiano, G.G.; Jaenisch, R.; Nelson, S.B. Reduced cortical activity due to a shift in the balance between excitation and inhibition in a mouse model of Rett syndrome. Proc. Natl. Acad. Sci. USA 2005, 102, 12560–12565. [Google Scholar] [CrossRef] [Green Version]
- Mariani, J.; Coppola, G.; Zhang, P.; Abyzov, A.; Provini, L.; Tomasini, L.; Amenduni, M.; Szekely, A.; Palejev, D.; Wilson, M.; et al. FOXG1-dependent dysregulation of GABA/glutamate neuron differentiation in autism spectrum disorders. Cell 2015, 162, 375–390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rubenstein, J.; Merzenich, M.M. Model of autism: Increased ratio of excitation/inhibition in key neural systems. Genes Brain Behav. 2003, 2, 255–267. [Google Scholar] [CrossRef] [PubMed]
- Marafiga, J.R.; Pasquetti, M.V.; Calcagnotto, M.E. GABAergic interneurons in epilepsy: More than a simple change in inhibition. Epilepsy Behav. 2021, 121, 106935. [Google Scholar] [CrossRef] [PubMed]
- Shao, L.R.; Habela, C.W.; Stafstrom, C.E. Pediatric epilepsy mechanisms: Expanding the paradigm of excitation/inhibition imbalance. Children 2019, 6, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiruska, P.; De Curtis, M.; Jefferys, J.G.; Schevon, C.A.; Schiff, S.J.; Schindler, K. Synchronization and desynchronization in epilepsy: Controversies and hypotheses. J. Physiol. 2013, 591, 787–797. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, Y.; Song, Y.; Ren, H.; Zhu, H.; Wang, Y.; Li, X.; Yan, W.; Wang, Y. Synchronization clusters located on epileptic onset zones in neocortical epilepsy. Acta Epileptol. 2022, 4, 42. [Google Scholar] [CrossRef]
- Cai, Y.; Yang, Z. Ferroptosis and its role in epilepsy. Front. Cell. Neurosci. 2021, 15, 696889. [Google Scholar] [CrossRef]
- Dehghani, N.; Peyrache, A.; Telenczuk, B.; Le Van Quyen, M.; Halgren, E.; Cash, S.S.; Hatsopoulos, N.G.; Destexhe, A. Dynamic balance of excitation and inhibition in human and monkey neocortex. Sci. Rep. 2016, 6, 23176. [Google Scholar] [CrossRef] [Green Version]
- Chao, H.T.; Chen, H.; Samaco, R.C.; Xue, M.; Chahrour, M.; Yoo, J.; Neul, J.L.; Gong, S.; Lu, H.C.; Heintz, N.; et al. Dysfunction in GABA signalling mediates autism-like stereotypies and Rett syndrome phenotypes. Nature 2010, 468, 263–269. [Google Scholar] [CrossRef] [Green Version]
- Calfa, G.; Li, W.; Rutherford, J.M.; Pozzo-Miller, L. Excitation/inhibition imbalance and impaired synaptic inhibition in hippocampal area CA3 of Mecp2 knockout mice. Hippocampus 2015, 25, 159–168. [Google Scholar] [CrossRef] [Green Version]
- Lee, L.J.; Tsytsarev, V.; Erzurumlu, R.S. Structural and functional differences in the barrel cortex of Mecp2 null mice. J. Comp. Neurol. 2017, 525, 3951–3961. [Google Scholar] [CrossRef]
- George, M.S.; Rush, A.J.; Sackeim, H.A.; Marangell, L.B. Vagus nerve stimulation (VNS): Utility in neuropsychiatric disorders. Int. J. Neuropsychopharmacol. 2003, 6, 73–83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Henry, T.R.; Bakay, R.A.; Votaw, J.R.; Pennell, P.B.; Epstein, C.M.; Faber, T.L.; Grafton, S.T.; Hoffman, J.M. Brain blood flow alterations induced by therapeutic vagus nerve stimulation in partial epilepsy: I. Acute effects at high and low levels of stimulation. Epilepsia 1998, 39, 983–990. [Google Scholar] [CrossRef] [PubMed]
- Henry, T.R.; Bakay, R.A.; Pennell, P.B.; Epstein, C.M.; Votaw, J.R. Brain blood-flow alterations induced by therapeutic vagus nerve stimulation in partial epilepsy: II. prolonged effects at high and low levels of stimulation. Epilepsia 2004, 45, 1064–1070. [Google Scholar] [CrossRef] [PubMed]
- Conway, C.R.; Sheline, Y.I.; Chibnall, J.T.; Bucholz, R.D.; Price, J.L.; Gangwani, S.; Mintun, M.A. Brain blood-flow change with acute vagus nerve stimulation in treatment-refractory major depressive disorder. Brain Stimul. 2012, 5, 163–171. [Google Scholar] [CrossRef] [Green Version]
- Ay, I.; Lu, J.; Ay, H.; Sorensen, A.G. Vagus nerve stimulation reduces infarct size in rat focal cerebral ischemia. Neurosci. Lett. 2009, 459, 147–151. [Google Scholar] [CrossRef]
- Kuba, R.; Guzaninová, M.; Brázdil, M.; Novák, Z.; Chrastina, J.; Rektor, I. Effect of vagal nerve stimulation on interictal epileptiform discharges: A scalp EEG study. Epilepsia 2002, 43, 1181–1188. [Google Scholar] [CrossRef]
- Santiago-Rodríguez, E.; Alonso-Vanegas, M.; Cárdenas-Morales, L.; Harmony, T.; Bernardino, M.; Fernández-Bouzas, A. Effects of two different cycles of vagus nerve stimulation on interictal epileptiform discharges. Seizure 2006, 15, 615–620. [Google Scholar] [CrossRef]
- Dimitrov, B.; Gatev, P. Effects of acute transcutaneous vagal stimulation on the EEG power maps, EEG sources distribution and steadiness of quiet and sensory-conflicted stance. In Proceedings of the Posture, Balance and the Brain, International Workshop Proceedings, Biomedical Data Journal, Thessaloniki, Greece, May 2015; pp. 45–54. [Google Scholar]
- Yokoyama, R.; Akiyama, Y.; Enatsu, R.; Suzuki, H.; Suzuki, Y.; Kanno, A.; Ochi, S.; Mikuni, N. The immediate effects of vagus nerve stimulation in intractable epilepsy: An intra-operative electrocorticographic analysis. Neurol. Med.-Chir. 2020, 60, 244–251. [Google Scholar] [CrossRef] [Green Version]
- Bartolomei, F.; Bonini, F.; Vidal, E.; Trébuchon, A.; Lagarde, S.; Lambert, I.; McGonigal, A.; Scavarda, D.; Carron, R.; Benar, C.G. How does vagal nerve stimulation (VNS) change EEG brain functional connectivity? Epilepsy Res. 2016, 126, 141–146. [Google Scholar] [CrossRef]
- Uchida, T.; Fujiwara, K.; Inoue, T.; Maruta, Y.; Kano, M.; Suzuki, M. Analysis of VNS effect on EEG connectivity with granger causality and graph theory. In Proceedings of the 2018 Asia-Pacific Signal and Information Processing Association Annual Summit and Conference (APSIPA ASC), Honolulu, HI, USA, 12–15 November 2018; pp. 861–864. [Google Scholar]
- Bodin, C.; Aubert, S.; Daquin, G.; Carron, R.; Scavarda, D.; McGonigal, A.; Bartolomei, F. Responders to vagus nerve stimulation (VNS) in refractory epilepsy have reduced interictal cortical synchronicity on scalp EEG. Epilepsy Res. 2015, 113, 98–103. [Google Scholar] [CrossRef] [PubMed]
- Sangare, A.; Marchi, A.; Pruvost-Robieux, E.; Soufflet, C.; Crepon, B.; Ramdani, C.; Chassoux, F.; Turak, B.; Landre, E.; Gavaret, M. The effectiveness of vagus nerve stimulation in drug-resistant epilepsy correlates with vagus nerve stimulation-induced electroencephalography desynchronization. Brain Connect. 2020, 10, 566–577. [Google Scholar] [CrossRef] [PubMed]
- Vespa, S.; Heyse, J.; Stumpp, L.; Liberati, G.; Ferrao Santos, S.; Rooijakkers, H.; Nonclercq, A.; Mouraux, A.; van Mierlo, P.; El Tahry, R. Vagus nerve stimulation elicits sleep EEG desynchronization and network changes in responder patients in epilepsy. Neurotherapeutics 2021, 18, 2623–2638. [Google Scholar] [CrossRef] [PubMed]
- Larsen, L.E.; Wadman, W.J.; Marinazzo, D.; van Mierlo, P.; Delbeke, J.; Daelemans, S.; Sprengers, M.; Thyrion, L.; Van Lysebettens, W.; Carrette, E.; et al. Vagus nerve stimulation applied with a rapid cycle has more profound influence on hippocampal electrophysiology than a standard cycle. Neurotherapeutics 2016, 13, 592–602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Lysebettens, W.; Vonck, K.; Larsen, L.E.; Stevens, L.; Bouckaert, C.; Germonpré, C.; Sprengers, M.; Carrette, E.; Delbeke, J.; Wadman, W.J.; et al. Identification of vagus nerve stimulation parameters affecting rat hippocampal electrophysiology without temperature effects. Brain Stimul. 2020, 13, 1198–1206. [Google Scholar] [CrossRef]
- Zanchetti, A.; Wang, S.; Moruzzi, G. The effect of vagal afferent stimulation on the EEG pattern of the cat. Electroencephalogr. Clin. Neurophysiol. 1952, 4, 357–361. [Google Scholar] [CrossRef]
- Alexander, G.M.; Huang, Y.Z.; Soderblom, E.J.; He, X.P.; Moseley, M.A.; McNamara, J.O. Vagal nerve stimulation modifies neuronal activity and the proteome of excitatory synapses of amygdala/piriform cortex. J. Neurochem. 2017, 140, 629–644. [Google Scholar] [CrossRef] [Green Version]
- Bancaud, J. La Stéréo-Électroencéphalographie dans l’Épilepsie: Informations Neurophysiopathologiques Apportées par l’Investigation Fonctionnelle Stéreotaxique: Rapport Présenté a la Société d’Électroencéphalographie de Langue Française (Marseille, Octobre 1962); Masson: Paris, France, 1965. [Google Scholar]
- Mullin, J.P.; Shriver, M.; Alomar, S.; Najm, I.; Bulacio, J.; Chauvel, P.; Gonzalez-Martinez, J. Is SEEG safe? A systematic review and meta-analysis of stereo-electroencephalography–related complications. Epilepsia 2016, 57, 386–401. [Google Scholar] [CrossRef] [Green Version]
- Englot, D.J. A modern epilepsy surgery treatment algorithm: Incorporating traditional and emerging technologies. Epilepsy Behav. 2018, 80, 68–74. [Google Scholar] [CrossRef]
- Jobst, B.C.; Bartolomei, F.; Diehl, B.; Frauscher, B.; Kahane, P.; Minotti, L.; Sharan, A.; Tardy, N.; Worrell, G.; Gotman, J. Intracranial EEG in the 21st Century. Epilepsy Curr. 2020, 20, 180–188. [Google Scholar] [CrossRef]
- Bancaud, J. angelergues R, Bernouilli C, Bonis a, Bordas-Ferrer M, Bresson M, Buser P, Covello L, Morel P, szikla G, takeda a, talairach J: Functional stereotaxic exploration (sEEG) of epilepsy. Electroencephalogr. Clin. Neurophysiol. 1970, 28, 85–86. [Google Scholar] [PubMed]
- González-Martínez, J.; Bulacio, J.; Thompson, S.; Gale, J.; Smithason, S.; Najm, I.; Bingaman, W. Technique, results, and complications related to robot-assisted stereoelectroencephalography. Neurosurgery 2016, 78, 169–180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Podkorytova, I.; Hoes, K.; Lega, B. Stereo-encephalography versus subdural electrodes for seizure localization. Neurosurg. Clin. 2016, 27, 97–109. [Google Scholar] [CrossRef]
- Jiang, H.; Kokkinos, V.; Ye, S.; Urban, A.; Bagić, A.; Richardson, M.; He, B. Interictal SEEG Resting-State Connectivity Localizes the Seizure Onset Zone and Predicts Seizure Outcome. Adv. Sci. 2022, 9, 2200887. [Google Scholar] [CrossRef] [PubMed]
- Sadaghiani, S.; Brookes, M.J.; Baillet, S. Connectomics of human electrophysiology. NeuroImage 2022, 247, 118788. [Google Scholar] [CrossRef] [PubMed]
- Specchio, N.; Wirrell, E.C.; Scheffer, I.E.; Nabbout, R.; Riney, K.; Samia, P.; Guerreiro, M.; Gwer, S.; Zuberi, S.M.; Wilmshurst, J.M.; et al. International League Against Epilepsy classification and definition of epilepsy syndromes with onset in childhood: Position paper by the ILAE Task Force on Nosology and Definitions. Epilepsia 2022, 63, 1398–1442. [Google Scholar] [CrossRef] [PubMed]
- Kwan, P.; Arzimanoglou, A.; Berg, A.T.; Brodie, M.J.; Allen Hauser, W.; Mathern, G.; Moshé, S.L.; Perucca, E.; Wiebe, S.; French, J. Definition of Drug Resistant Epilepsy: Consensus Proposal by the ad Hoc TASK Force of the ILAE Commission on Therapeutic Strategies. 2010. Available online: https://onlinelibrary.wiley.com/doi/full/10.1111/j.1528-1167.2009.02397.x (accessed on 22 March 2023).
- Révész, D.; Rydenhag, B.; Ben-Menachem, E. Complications and safety of vagus nerve stimulation: 25 years of experience at a single center. J. Neurosurg. Pediatr. 2016, 18, 97–104. [Google Scholar] [CrossRef] [Green Version]
- Delorme, A.; Makeig, S. EEGLAB: An open source toolbox for analysis of single-trial EEG dynamics including independent component analysis. J. Neurosci. Methods 2004, 134, 9–21. [Google Scholar] [CrossRef] [Green Version]
- Lagarde, S.; Roehri, N.; Lambert, I.; Trebuchon, A.; McGonigal, A.; Carron, R.; Scavarda, D.; Milh, M.; Pizzo, F.; Colombet, B.; et al. Interictal stereotactic-EEG functional connectivity in refractory focal epilepsies. Brain 2018, 141, 2966–2980. [Google Scholar] [CrossRef] [Green Version]
- Miller, K.J.; Sorensen, L.B.; Ojemann, J.G.; Den Nijs, M. Power-law scaling in the brain surface electric potential. PLoS Comput. Biol. 2009, 5, e1000609. [Google Scholar] [CrossRef] [Green Version]
- Lombardi, F.; Herrmann, H.J.; de Arcangelis, L. Balance of excitation and inhibition determines 1/f power spectrum in neuronal networks. Chaos Interdiscip. J. Nonlinear Sci. 2017, 27, 047402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, R.; Peterson, E.J.; Voytek, B. Inferring synaptic excitation/inhibition balance from field potentials. Neuroimage 2017, 158, 70–78. [Google Scholar] [CrossRef] [PubMed]
- Donoghue, T.; Haller, M.; Peterson, E.J.; Varma, P.; Sebastian, P.; Gao, R.; Noto, T.; Lara, A.H.; Wallis, J.D.; Knight, R.T.; et al. Parameterizing neural power spectra into periodic and aperiodic components. Nat. Neurosci. 2020, 23, 1655–1665. [Google Scholar] [CrossRef]
- Castoro, M.A.; Yoo, P.B.; Hincapie, J.G.; Hamann, J.J.; Ruble, S.B.; Wolf, P.D.; Grill, W.M. Excitation properties of the right cervical vagus nerve in adult dogs. Exp. Neurol. 2011, 227, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Bunch, S.; DeGiorgio, C.; Krahl, S.; Britton, J.; Green, P.; Lancman, M.; Murphy, J.; Olejniczak, P.; Shih, J.; Heck, C. Vagus nerve stimulation for epilepsy: Is output current correlated with acute response? Acta Neurol. Scand. 2007, 116, 217–220. [Google Scholar] [CrossRef]
- Fahoum, F.; Boffini, M.; Kann, L.; Faini, S.; Gordon, C.; Tzadok, M.; El Tahry, R. VNS parameters for clinical response in Epilepsy. Brain Stimul. 2022, 15, 814–821. [Google Scholar] [CrossRef]
- Borland, M.; Vrana, W.; Moreno, N.; Fogarty, E.; Buell, E.; Sharma, P.; Engineer, C.; Kilgard, M. Cortical map plasticity as a function of vagus nerve stimulation intensity. Brain Stimul. 2016, 9, 117–123. [Google Scholar] [CrossRef] [Green Version]
- Hachem, L.D.; Wong, S.M.; Ibrahim, G.M. The vagus afferent network: Emerging role in translational connectomics. Neurosurg. Focus 2018, 45, E2. [Google Scholar] [CrossRef] [Green Version]
- Goddard, G.V. Development of epileptic seizures through brain stimulation at low intensity. Nature 1967, 214, 1020–1021. [Google Scholar] [CrossRef]
- Kairiss, E.; Racine, R.; Smith, G. The development of the interictal spike during kindling in the rat. Brain Res. 1984, 322, 101–110. [Google Scholar] [CrossRef]
- Racine, R.; Paxinos, G.; Mosher, J.; Kairiss, E. The effects of various lesions and knife-cuts on septal and amygdala kindling in the rat. Brain Res. 1988, 454, 264–274. [Google Scholar] [CrossRef]
- Maurer, S.V.; Williams, C.L. The cholinergic system modulates memory and hippocampal plasticity via its interactions with non-neuronal cells. Front. Immunol. 2017, 8, 1489. [Google Scholar] [CrossRef] [Green Version]
- Diaz Verdugo, C.; Myren-Svelstad, S.; Aydin, E.; Van Hoeymissen, E.; Deneubourg, C.; Vanderhaeghe, S.; Vancraeynest, J.; Pelgrims, R.; Cosacak, M.I.; Muto, A.; et al. Glia-neuron interactions underlie state transitions to generalized seizures. Nat. Commun. 2019, 10, 3830. [Google Scholar] [CrossRef] [Green Version]
- Amiri, M.; Bahrami, F.; Janahmadi, M. Modified thalamocortical model: A step towards more understanding of the functional contribution of astrocytes to epilepsy. J. Comput. Neurosci. 2012, 33, 285–299. [Google Scholar] [CrossRef] [PubMed]
- Volnova, A.; Tsytsarev, V.; Ganina, O.; Vélez-Crespo, G.E.; Alves, J.M.; Ignashchenkova, A.; Inyushin, M. The anti-epileptic effects of carbenoxolone in vitro and in vivo. Int. J. Mol. Sci. 2022, 23, 663. [Google Scholar] [CrossRef] [PubMed]
- Cendes, F.; Andermann, F.; Gloor, P.; Evans, A.; Jones-Gotman, M.; Watson, C.; Melanson, D.; Olivier, A.; Peters, T.; Lopes-Cendes, I.; et al. MRI volumetric measurement of amygdala and hippocampus in temporal lobe epilepsy. Neurology 1993, 43, 719. [Google Scholar] [CrossRef] [PubMed]
- Saukkonen, A.; Kälviäinen, R.; Partanen, K.; Vainio, P.; Riekkinen, P.; Pitkänen, A. Do seizures cause neuronal damage? A MRI study in newly diagnosed, and chronic epilepsy. Neuroreport 1994, 6, 219. [Google Scholar] [CrossRef]
- Pitkänen, A.; Tuunanen, J.; Kälviäinen, R.; Partanen, K.; Salmenperä, T. Amygdala damage in experimental and human temporal lobe epilepsy. Epilepsy Res. 1998, 32, 233–253. [Google Scholar] [CrossRef]
- Shipton, O.A.; El-Gaby, M.; Apergis-Schoute, J.; Deisseroth, K.; Bannerman, D.M.; Paulsen, O.; Kohl, M.M. Left–right dissociation of hippocampal memory processes in mice. Proc. Natl. Acad. Sci. USA 2014, 111, 15238–15243. [Google Scholar] [CrossRef] [Green Version]
- Vonck, K.; De Herdt, V.; Bosman, T.; Dedeurwaerdere, S.; Van Laere, K.; Boon, P. Thalamic and limbic involvement in the mechanism of action of vagus nerve stimulation, a SPECT study. Seizure 2008, 17, 699–706. [Google Scholar] [CrossRef]
- Bohning, D.E.; Lomarev, M.P.; Denslow, S.; Nahas, Z.; Shastri, A.; George, M.S. Feasibility of vagus nerve stimulation–synchronized blood oxygenation level–dependent functional MRI. Investig. Radiol. 2001, 36, 470–479. [Google Scholar] [CrossRef] [PubMed]
- Kraus, T.; Hösl, K.; Kiess, O.; Schanze, A.; Kornhuber, J.; Forster, C. BOLD fMRI deactivation of limbic and temporal brain structures and mood enhancing effect by transcutaneous vagus nerve stimulation. J. Neural Transm. 2007, 114, 1485–1493. [Google Scholar] [CrossRef] [PubMed]
- Van Laere, K.; Vonck, K.; Boon, P.; Versijpt, J.; Dierckx, R. Perfusion SPECT changes after acute and chronic vagus nerve stimulation in relation to prestimulus condition and long-term clinical efficacy. J. Nucl. Med. 2002, 43, 733–744. [Google Scholar] [PubMed]
- Dedeurwaerdere, S.; Cornelissen, B.; Van Laere, K.; Vonck, K.; Achten, E.; Slegers, G.; Boon, P. Small animal positron emission tomography during vagus nerve stimulation in rats: A pilot study. Epilepsy Res. 2005, 67, 133–141. [Google Scholar] [CrossRef]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ooi, Q.Y.; Qin, X.; Yuan, Y.; Zhang, X.; Yao, Y.; Hao, H.; Li, L. Alteration of Excitation/Inhibition Imbalance in the Hippocampus and Amygdala of Drug-Resistant Epilepsy Patients Treated with Acute Vagus Nerve Stimulation. Brain Sci. 2023, 13, 976. https://doi.org/10.3390/brainsci13070976
Ooi QY, Qin X, Yuan Y, Zhang X, Yao Y, Hao H, Li L. Alteration of Excitation/Inhibition Imbalance in the Hippocampus and Amygdala of Drug-Resistant Epilepsy Patients Treated with Acute Vagus Nerve Stimulation. Brain Sciences. 2023; 13(7):976. https://doi.org/10.3390/brainsci13070976
Chicago/Turabian StyleOoi, Qian Yi, Xiaoya Qin, Yuan Yuan, Xiaobin Zhang, Yi Yao, Hongwei Hao, and Luming Li. 2023. "Alteration of Excitation/Inhibition Imbalance in the Hippocampus and Amygdala of Drug-Resistant Epilepsy Patients Treated with Acute Vagus Nerve Stimulation" Brain Sciences 13, no. 7: 976. https://doi.org/10.3390/brainsci13070976
APA StyleOoi, Q. Y., Qin, X., Yuan, Y., Zhang, X., Yao, Y., Hao, H., & Li, L. (2023). Alteration of Excitation/Inhibition Imbalance in the Hippocampus and Amygdala of Drug-Resistant Epilepsy Patients Treated with Acute Vagus Nerve Stimulation. Brain Sciences, 13(7), 976. https://doi.org/10.3390/brainsci13070976