
Different Effect Sizes of Motor Skill Training Combined with Repetitive Transcranial versus Trans-Spinal Magnetic Stimulation in Healthy Subjects


Abstract
:1. Introduction
2. Materials and Methods
2.1. Trial Design and Participants
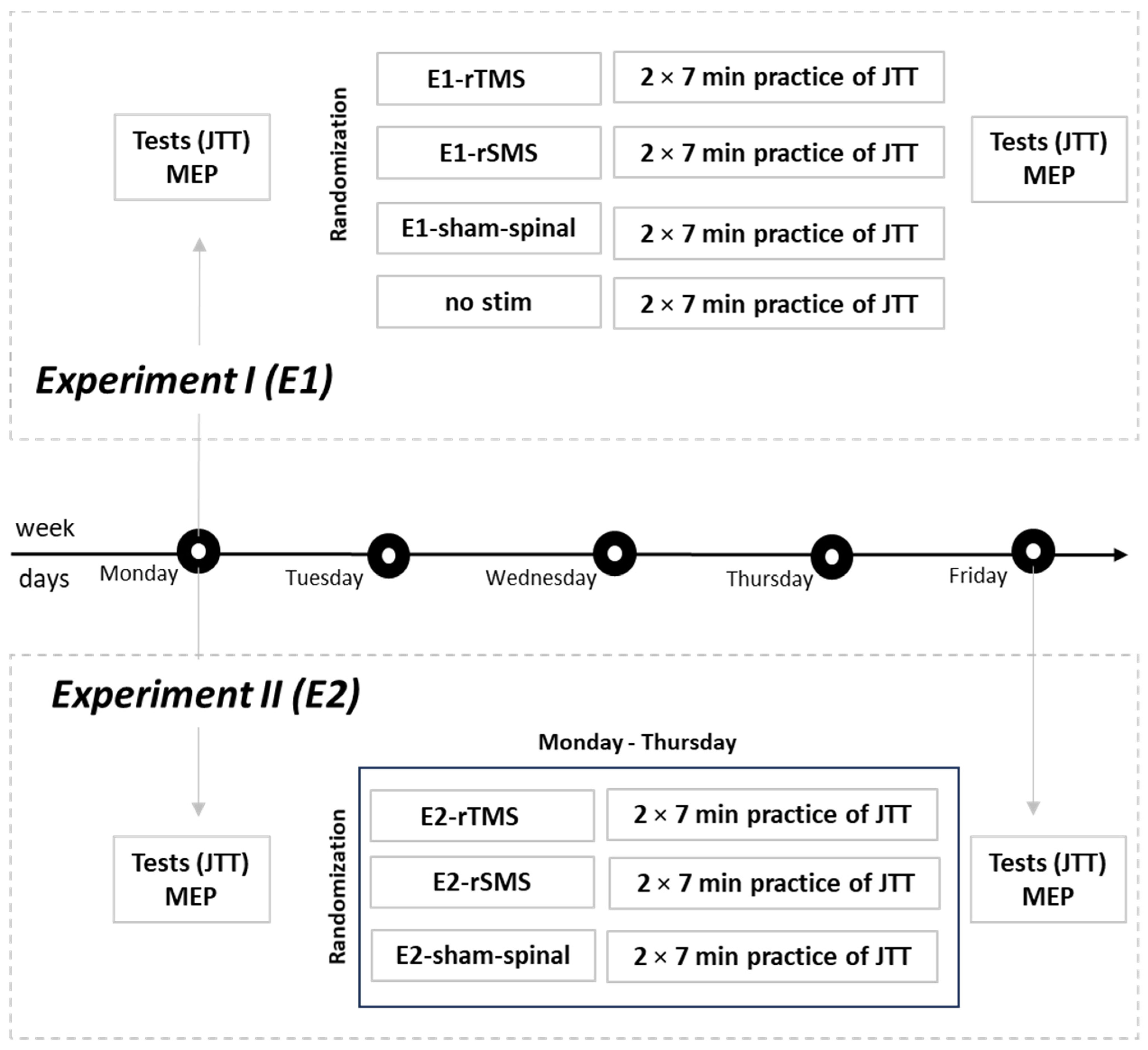
2.2. Experimental Procedure Experiment I (E1)
2.3. Experimental Procedure Experiment II (E2)
2.4. Motor Tests
2.5. Motor Training
2.6. MEP
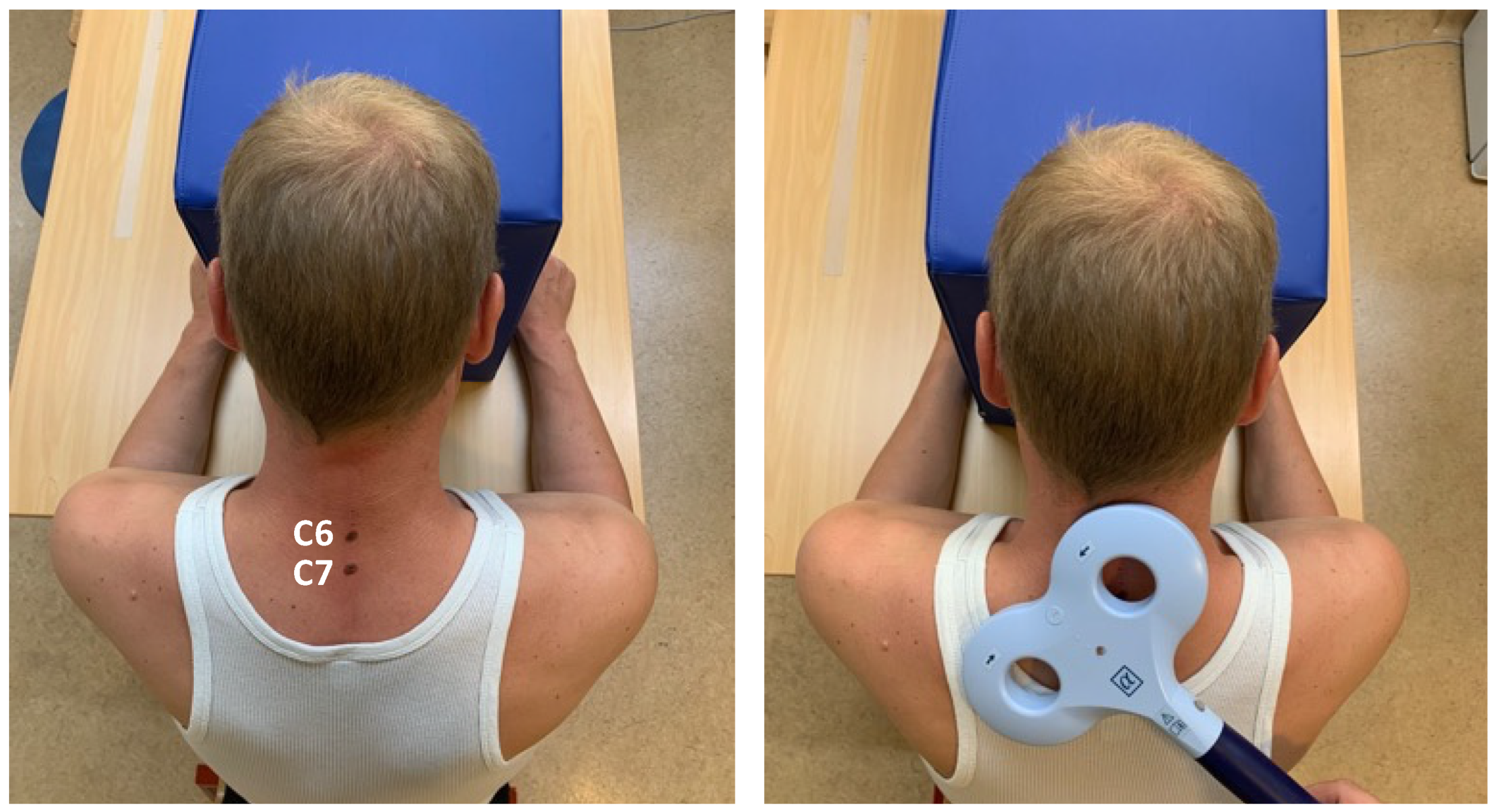
2.7. rTMS, rSMS, Spinal Sham Stimulation
2.8. Randomization and Blinding
2.9. Sample Size
2.10. Outcomes, Data Analysis, and Statistical Procedures
3. Results
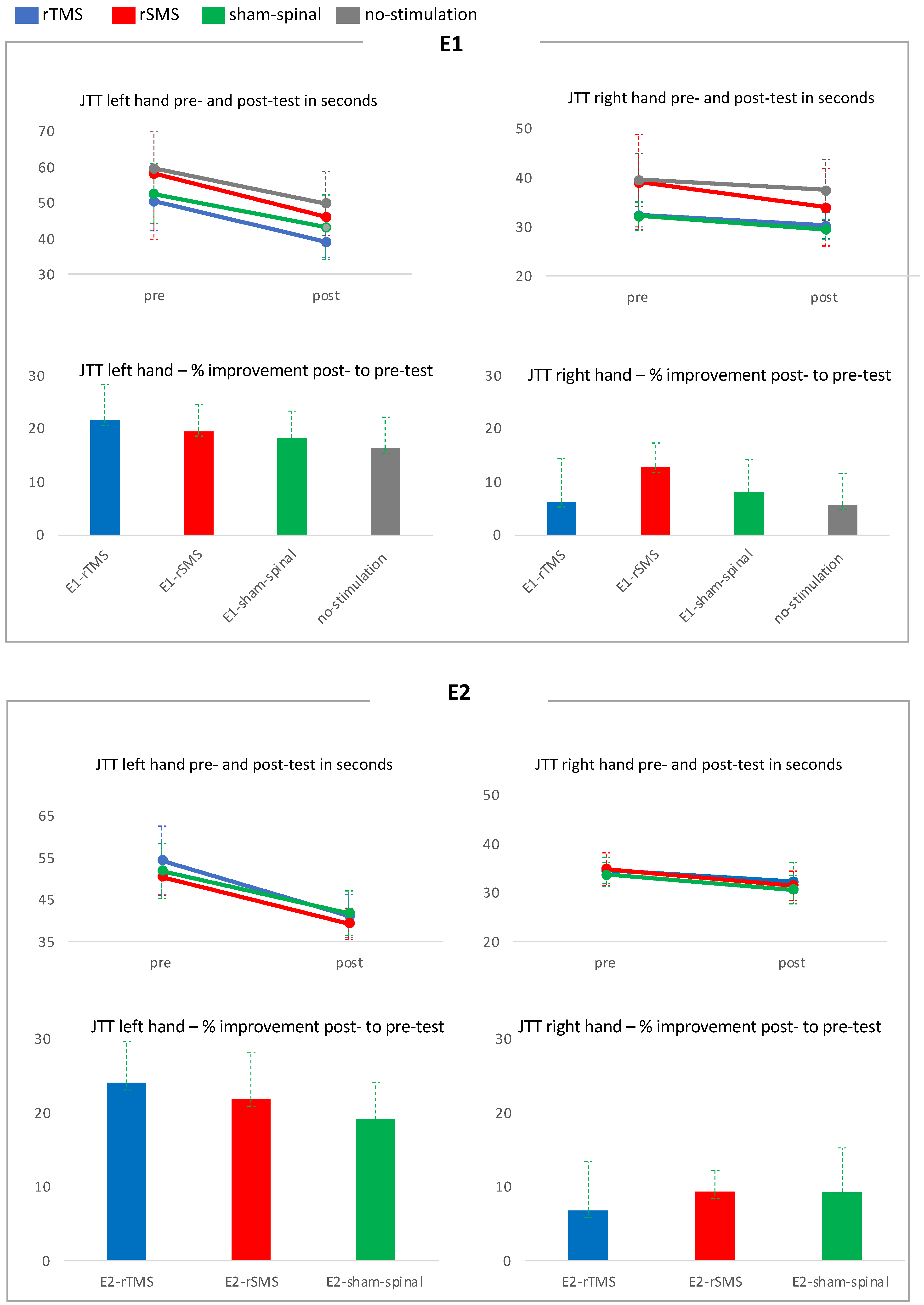
3.1. E1: JTT Pre- and Post-Test Results
- The baseline values of JTT left hand were not significantly different between groups (F (3,55) = 1.95; n.s.).
- There was a significant main effect for JTT (F (1,55) = 274.91; p < 0.001) showing a motor learning effect across all groups.
- As expected, a significant main effect was also found for Hand (F (1,55) = 319.99; p < 0.001), indicating higher test performance with the dominant right hand.
- The interaction between JTT and Group was not significant (F (3,55) = 0.69; n.s.).
- The interaction between Hand and Group was not significant but showed a trend (F (3,55) = 2.31; p = 0.086).
- The interaction between JTT and Hand was significant (F (1,55) = 201.75; p < 0.001).
- Thus, the motor performance gain was dependent on laterality.
- Between-group analysis: JTT left and right hand showed no significant difference between groups.
- Within-group analysis: Paired t-test showed a significant increase for the left and right hand in all groups (Table 3).
- Effect sizes: The effect size of E1-rTMS was large (d = 0.8) compared to the no-stimulation group, medium compared to E1-sham-spinal (d = 0.6), and small compared to E1-rSMS (d = 0.4). The effect size of E1-rSMS was small compared to E1-sham-spinal (d = 0.3) and medium compared to the no-stimulation group (d = 0.6). The effect size of E1-sham-spinal was small compared to the no-stimulation group (d = 0.4) (Table 4).
3.2. E1: RMT, Amplitude and Latency
- There was no significant main effect for RMT (F (1,55) = 0.04; n.s.).
- The interaction between RMT and Group was not significant (F (3,55) = 0.69; n.s.).
- There was no significant main effect for Latency (F (1,55) = 1.97; n.s.).
- The interaction between Latency and Group was not significant (F (3,55) = 0.12; n.s.).
- The main effect for Amplitude (F (1,55) = 7.03; p = 0.01), as well as the interaction between Amplitude and Group, were significant (F (3,55) = 2.98; p = 0.04).
- Between-group analysis: MEP amplitude was not significantly different between groups.
- Within-group analysis: A significant enhancement in MEP amplitude within the rSMS group (p < 0.02) was found.
3.3. E2: JTT Pre- and Post-Test Results
- The baseline values of JTT left hand were not significantly different between groups (F (2,31) = 1.10; n.s.)
- There was a significant main effect for JTT (F (1,31) = 339.41; p < 0.001). Thus, all subjects improved their motor performance between pre- and post-test periods.
- A significant main effect was also found for Hand (F (1,31) = 343.24; p < 0.001), indicating that subjects performed better with their dominant right hand.
- The interaction between JTT and Group was not significant (F (2,31) = 0.81; n.s.).
- The interaction between Hand and Group was not significant (F (2,31) = 1.52; n.s.).
- The interaction between JTT and Hand was significant (F (1,32) = 158.16; p < 0.001). Thus, the motor performance gain was dependent on laterality.
- Between-group analysis: JTT left and right hand showed no significant difference between groups.
- Within-group analysis: Paired t-test showed a significant increase for the left and right hand in all groups (Table 7).
- Effect sizes:
- The effect size of E2-rTMS was large (d = 0.9) compared to the E2-sham-spinal group and was small compared to E2-rSMS (d = 0.4). The effect size of E2-rSMS was medium compared to E2-sham-spinal (d = 0.5) (Table 8).
3.4. E2: RMT, Amplitude and Latency
- There was no significant main effect for RMT (F (1,31) = 0.62; n.s.).
- The interaction between RMT and Group was not significant (F (2,31) = 0.26; n.s.).
- There was a significant main effect for Latency (F (1,31) = 4.19; p = 0.049). Latency was shorter for the post-measurement of the MEP.
- The interaction between Latency and Group was not significant (F (2,31) = 0.98; n.s.).
- There was no significant main effect for Amplitude (F (1,31) = 1.89; n.s.).
- The interaction between Amplitude and Group was not significant (F (2,31) = 0.34; n.s.).
- Within group analysis: The latency was only substantially reduced in the rSMS group from the pre- to post-test (p < 0.04).
4. Discussion
4.1. The Effect of rTMS
4.2. The Effect of Spinal Sham Stimulation
4.3. The Effect of rSMS and Prospects
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Natali, A.L.; Reddy, V.; Bordoni, B. Neuroanatomy, Corticospinal Cord Tract. In StatPearls; StatPearls: Treasure Island, FL, USA, 2023. [Google Scholar]
- Yang, Y.; Pan, H.; Pan, W.; Liu, Y.; Song, X.; Niu, C.M.; Feng, W.; Wang, J.; Xie, Q. Repetitive Transcranial Magnetic Stimulation on the Affected Hemisphere Enhances Hand Functional Recovery in Subacute Adult Stroke Patients: A Randomized Trial. Front. Aging Neurosci. 2021, 13, 636184. [Google Scholar] [CrossRef]
- Jelic, M.B.; Stevanovic, V.B.; Milanovic, S.D.; Ljubisavljevic, M.R.; Filipovic, S.R. Transcranial magnetic stimulation has no placebo effect on motor learning. Clin. Neurophysiol. 2013, 124, 1646–1651. [Google Scholar] [CrossRef] [PubMed]
- Fan, Z.; Wen, X.; Ding, X.; Wang, Q.; Wang, S.; Yu, W. Advances in biotechnology and clinical therapy in the field of peripheral nerve regeneration based on magnetism. Front. Neurol. 2023, 14, 1079757. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, J.F.; Klemar, B.; Hansen, H.J.; Sinkjaer, T. A new treatment of spasticity with repetitive magnetic stimulation in multiple sclerosis. J. Neurol. Neurosurg. Psychiatry 1995, 58, 254–255. [Google Scholar] [CrossRef] [PubMed]
- Jia, Y.; Liu, X.; Wei, J.; Li, D.; Wang, C.; Wang, X.; Liu, H. Modulation of the Corticomotor Excitability by Repetitive Peripheral Magnetic Stimulation on the Median Nerve in Healthy Subjects. Front. Neural. Circuits 2021, 15, 616084. [Google Scholar] [CrossRef] [PubMed]
- Struppler, A.; Binkofski, F.; Angerer, B.; Bernhardt, M.; Spiegel, S.; Drzezga, A.; Bartenstein, P. A fronto-parietal network is mediating improvement of motor function related to repetitive peripheral magnetic stimulation: A PET-H2O15 study. Neuroimage 2007, 36 (Suppl. 2), T174–T186. [Google Scholar] [CrossRef] [PubMed]
- Krause, P.; Straube, A. Peripheral repetitive magnetic stimulation induces intracortical inhibition in healthy subjects. Neurol. Res. 2008, 30, 690–694. [Google Scholar] [CrossRef] [PubMed]
- Oldfield, R.C. The assessment and analysis of handedness: The Edinburgh inventory. Neuropsychologia 1971, 9, 97–113. [Google Scholar] [CrossRef] [PubMed]
- Rossi, S.; Antal, A.; Bestmann, S.; Bikson, M.; Brewer, C.; Brockmoller, J.; Carpenter, L.L.; Cincotta, M.; Chen, R.; Daskalakis, J.D.; et al. Safety and recommendations for TMS use in healthy subjects and patient populations, with updates on training, ethical and regulatory issues: Expert Guidelines. Clin. Neurophysiol. 2021, 132, 269–306. [Google Scholar] [CrossRef] [PubMed]
- Jebsen, R.H.; Taylor, N.; Trieschmann, R.B.; Trotter, M.J.; Howard, L.A. An objective and standardized test of hand function. Arch. Phys. Med. Rehabil. 1969, 50, 311–319. [Google Scholar] [PubMed]
- Rossini, P.M.; Barker, A.T.; Berardelli, A.; Caramia, M.D.; Caruso, G.; Cracco, R.Q.; Dimitrijevic, M.R.; Hallett, M.; Katayama, Y.; Lucking, C.H.; et al. Non-invasive electrical and magnetic stimulation of the brain, spinal cord and roots: Basic principles and procedures for routine clinical application. Report of an IFCN committee. Electroencephalogr. Clin. Neurophysiol. 1994, 91, 79–92. [Google Scholar] [CrossRef] [PubMed]
- Groppa, S.; Oliviero, A.; Eisen, A.; Quartarone, A.; Cohen, L.G.; Mall, V.; Kaelin-Lang, A.; Mima, T.; Rossi, S.; Thickbroom, G.W.; et al. A practical guide to diagnostic transcranial magnetic stimulation: Report of an IFCN committee. Clin. Neurophysiol. 2012, 123, 858–882. [Google Scholar] [CrossRef] [PubMed]
- Rossini, P.M.; Burke, D.; Chen, R.; Cohen, L.G.; Daskalakis, Z.; Di Iorio, R.; Di Lazzaro, V.; Ferreri, F.; Fitzgerald, P.B.; George, M.S.; et al. Non-invasive electrical and magnetic stimulation of the brain, spinal cord, roots and peripheral nerves: Basic principles and procedures for routine clinical and research application. An updated report from an I.F.C.N. Committee. Clin. Neurophysiol. 2015, 126, 1071–1107. [Google Scholar] [CrossRef] [PubMed]
- Goldsworthy, M.R.; Hordacre, B.; Ridding, M.C. Minimum number of trials required for within- and between-session reliability of TMS measures of corticospinal excitability. Neuroscience 2016, 320, 205–209. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, J.F.; Sinkjaer, T. Long-lasting depression of soleus motoneurons excitability following repetitive magnetic stimuli of the spinal cord in multiple sclerosis patients. Mult. Scler. 1997, 3, 18–30. [Google Scholar] [CrossRef] [PubMed]
- Doig, G.S.; Simpson, F. Randomization and allocation concealment: A practical guide for researchers. J. Crit. Care 2005, 20, 187–191, discussion 191–183. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Quartarone, A.; Bagnato, S.; Rizzo, V.; Morgante, F.; Sant’angelo, A.; Battaglia, F.; Messina, C.; Siebner, H.R.; Girlanda, P. Distinct changes in cortical and spinal excitability following high-frequency repetitive TMS to the human motor cortex. Exp. Brain Res. 2005, 161, 114–124. [Google Scholar] [CrossRef]
- Shmuelof, L.; Yang, J.; Caffo, B.; Mazzoni, P.; Krakauer, J.W. The neural correlates of learned motor acuity. J. Neurophysiol. 2014, 112, 971–980. [Google Scholar] [CrossRef]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef]
- Siebner, H.R.; Funke, K.; Aberra, A.S.; Antal, A.; Bestmann, S.; Chen, R.; Classen, J.; Davare, M.; Di Lazzaro, V.; Fox, P.T.; et al. Transcranial magnetic stimulation of the brain: What is stimulated?—A consensus and critical position paper. Clin. Neurophysiol. 2022, 140, 59–97. [Google Scholar] [CrossRef] [PubMed]
- Rounis, E.; Lee, L.; Siebner, H.R.; Rowe, J.B.; Friston, K.J.; Rothwell, J.C.; Frackowiak, R.S. Frequency specific changes in regional cerebral blood flow and motor system connectivity following rTMS to the primary motor cortex. Neuroimage 2005, 26, 164–176. [Google Scholar] [CrossRef] [PubMed]
- Jung, J.; Bungert, A.; Bowtell, R.; Jackson, S.R. Modulating Brain Networks With Transcranial Magnetic Stimulation Over the Primary Motor Cortex: A Concurrent TMS/fMRI Study. Front. Hum. Neurosci. 2020, 14, 31. [Google Scholar] [CrossRef] [PubMed]
- Bestmann, S.; Swayne, O.; Blankenburg, F.; Ruff, C.C.; Haggard, P.; Weiskopf, N.; Josephs, O.; Driver, J.; Rothwell, J.C.; Ward, N.S. Dorsal premotor cortex exerts state-dependent causal influences on activity in contralateral primary motor and dorsal premotor cortex. Cereb. Cortex 2008, 18, 1281–1291. [Google Scholar] [CrossRef] [PubMed]
- Bestmann, S.; Baudewig, J.; Siebner, H.R.; Rothwell, J.C.; Frahm, J. BOLD MRI responses to repetitive TMS over human dorsal premotor cortex. Neuroimage 2005, 28, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Lappchen, C.H.; Ringer, T.; Blessin, J.; Schulz, K.; Seidel, G.; Lange, R.; Hamzei, F. Daily iTBS worsens hand motor training—A combined TMS, fMRI and mirror training study. Neuroimage 2015, 107, 257–265. [Google Scholar] [CrossRef] [PubMed]
- Hamada, M.; Murase, N.; Hasan, A.; Balaratnam, M.; Rothwell, J.C. The role of interneuron networks in driving human motor cortical plasticity. Cereb. Cortex 2013, 23, 1593–1605. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Alonso, V.; Cheeran, B.; Rio-Rodriguez, D.; Fernandez-Del-Olmo, M. Inter-individual variability in response to non-invasive brain stimulation paradigms. Brain Stimul. 2014, 7, 372–380. [Google Scholar] [CrossRef]
- Lopez-Alonso, V.; Cheeran, B.; Fernandez-del-Olmo, M. Relationship Between Non-invasive Brain Stimulation-induced Plasticity and Capacity for Motor Learning. Brain Stimul. 2015, 8, 1209–1219. [Google Scholar] [CrossRef]
- Lopez-Alonso, V.; Fernandez-Del-Olmo, M.; Costantini, A.; Gonzalez-Henriquez, J.J.; Cheeran, B. Intra-individual variability in the response to anodal transcranial direct current stimulation. Clin. Neurophysiol. 2015, 126, 2342–2347. [Google Scholar] [CrossRef]
- Lopez-Alonso, V.; Liew, S.L.; Fernandez Del Olmo, M.; Cheeran, B.; Sandrini, M.; Abe, M.; Cohen, L.G. A Preliminary Comparison of Motor Learning Across Different Non-invasive Brain Stimulation Paradigms Shows No Consistent Modulations. Front. Neurosci. 2018, 12, 253. [Google Scholar] [CrossRef]
- Wiethoff, S.; Hamada, M.; Rothwell, J.C. Variability in response to transcranial direct current stimulation of the motor cortex. Brain. Stimul. 2014, 7, 468–475. [Google Scholar] [CrossRef] [PubMed]
- Ridding, M.C.; Ziemann, U. Determinants of the induction of cortical plasticity by non-invasive brain stimulation in healthy subjects. J. Physiol. 2010, 588, 2291–2304. [Google Scholar] [CrossRef] [PubMed]
- Talelli, P.; Cheeran, B.J.; Teo, J.T.; Rothwell, J.C. Pattern-specific role of the current orientation used to deliver Theta Burst Stimulation. Clin. Neurophysiol. 2007, 118, 1815–1823. [Google Scholar] [CrossRef] [PubMed]
- Cheeran, B.; Talelli, P.; Mori, F.; Koch, G.; Suppa, A.; Edwards, M.; Houlden, H.; Bhatia, K.; Greenwood, R.; Rothwell, J.C. A common polymorphism in the brain-derived neurotrophic factor gene (BDNF) modulates human cortical plasticity and the response to rTMS. J. Physiol. 2008, 586, 5717–5725. [Google Scholar] [CrossRef] [PubMed]
- Hinder, M.R.; Goss, E.L.; Fujiyama, H.; Canty, A.J.; Garry, M.I.; Rodger, J.; Summers, J.J. Inter- and Intra-individual variability following intermittent theta burst stimulation: Implications for rehabilitation and recovery. Brain Stimul. 2014, 7, 365–371. [Google Scholar] [CrossRef] [PubMed]
- Inghilleri, M.; Conte, A.; Curra, A.; Frasca, V.; Lorenzano, C.; Berardelli, A. Ovarian hormones and cortical excitability. An rTMS study in humans. Clin. Neurophysiol. 2004, 115, 1063–1068. [Google Scholar] [CrossRef]
- Conde, V.; Vollmann, H.; Sehm, B.; Taubert, M.; Villringer, A.; Ragert, P. Cortical thickness in primary sensorimotor cortex influences the effectiveness of paired associative stimulation. Neuroimage 2012, 60, 864–870. [Google Scholar] [CrossRef] [PubMed]
- Karabanov, A.; Thielscher, A.; Siebner, H.R. Transcranial brain stimulation: Closing the loop between brain and stimulation. Curr. Opin. Neurol. 2016, 29, 397–404. [Google Scholar] [CrossRef]
- Li, L.M.; Uehara, K.; Hanakawa, T. The contribution of interindividual factors to variability of response in transcranial direct current stimulation studies. Front. Cell. Neurosci. 2015, 9, 181. [Google Scholar] [CrossRef] [PubMed]
- Zrenner, C.; Belardinelli, P.; Muller-Dahlhaus, F.; Ziemann, U. Closed-Loop Neuroscience and Non-Invasive Brain Stimulation: A Tale of Two Loops. Front. Cell. Neurosci. 2016, 10, 92. [Google Scholar] [CrossRef]
- Guerra, A.; Lopez-Alonso, V.; Cheeran, B.; Suppa, A. Variability in non-invasive brain stimulation studies: Reasons and results. Neurosci. Lett. 2020, 719, 133330. [Google Scholar] [CrossRef] [PubMed]
- Sollmann, N.; Goblirsch-Kolb, M.F.; Ille, S.; Butenschoen, V.M.; Boeckh-Behrens, T.; Meyer, B.; Ringel, F.; Krieg, S.M. Comparison between electric-field-navigated and line-navigated TMS for cortical motor mapping in patients with brain tumors. Acta. Neurochir. 2016, 158, 2277–2289. [Google Scholar] [CrossRef] [PubMed]
- Ward, N.S.; Newton, J.M.; Swayne, O.B.; Lee, L.; Thompson, A.J.; Greenwood, R.J.; Rothwell, J.C.; Frackowiak, R.S. Motor system activation after subcortical stroke depends on corticospinal system integrity. Brain 2006, 129, 809–819. [Google Scholar] [CrossRef] [PubMed]
- Rapisarda, G.; Bastings, E.; de Noordhout, A.M.; Pennisi, G.; Delwaide, P.J. Can motor recovery in stroke patients be predicted by early transcranial magnetic stimulation? Stroke 1996, 27, 2191–2196. [Google Scholar] [CrossRef] [PubMed]
- Escudero, J.V.; Sancho, J.; Bautista, D.; Escudero, M.; Lopez-Trigo, J. Prognostic value of motor evoked potential obtained by transcranial magnetic brain stimulation in motor function recovery in patients with acute ischemic stroke. Stroke 1998, 29, 1854–1859. [Google Scholar] [CrossRef] [PubMed]
- Stinear, C.M.; Barber, P.A.; Petoe, M.; Anwar, S.; Byblow, W.D. The PREP algorithm predicts potential for upper limb recovery after stroke. Brain 2012, 135, 2527–2535. [Google Scholar] [CrossRef] [PubMed]
- Ameli, M.; Grefkes, C.; Kemper, F.; Riegg, F.P.; Rehme, A.K.; Karbe, H.; Fink, G.R.; Nowak, D.A. Differential effects of high-frequency repetitive transcranial magnetic stimulation over ipsilesional primary motor cortex in cortical and subcortical middle cerebral artery stroke. Ann. Neurol. 2009, 66, 298–309. [Google Scholar] [CrossRef] [PubMed]
- Fawaz, S.I.; Izumi, S.I.; Hamada, S.M.; Omara, A.A.; Wassef, G.O.; Saber, H.G.; Salama, S.M. Role of Cervical Spinal Magnetic Stimulation in Improving Posture and Functional Ambulation of Patients with Relapsing Remitting Multiple Sclerosis. Rehabil. Res. Pract. 2022, 2022, 6009104. [Google Scholar] [CrossRef]
- Nielsen, J.F.; Sinkjaer, T.; Jakobsen, J. Treatment of spasticity with repetitive magnetic stimulation; a double-blind placebo-controlled study. Mult. Scler. 1996, 2, 227–232. [Google Scholar] [CrossRef]
- Mitsui, T.; Arii, Y.; Taniguchi, K.; Tsutsumi, S.; Takahara, M.; Mabuchi, M.; Sumitomo, N.; Matsuura, M.; Kuroda, Y. Efficacy of Repetitive Trans-spinal Magnetic Stimulation for Patients with Parkinson’s Disease: A Randomised Controlled Trial. Neurotherapeutics 2022, 19, 1273–1282. [Google Scholar] [CrossRef] [PubMed]
- Powell, M.P.; Verma, N.; Sorensen, E.; Carranza, E.; Boos, A.; Fields, D.P.; Roy, S.; Ensel, S.; Barra, B.; Balzer, J.; et al. Epidural stimulation of the cervical spinal cord for post-stroke upper-limb paresis. Nat. Med. 2023, 29, 689–699. [Google Scholar] [CrossRef] [PubMed]
- Read, D.J.; Matthews, W.B.; Higson, R.H. The effect of spinal cord stimulation on function in patients with multiple sclerosis. Brain 1980, 103, 803–833. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| E1 Groups | Mean Time Pre-Test | Mean Time Post-Test | Increase in % |
|---|---|---|---|
| E1-rTMS | 50.4 ± 8.1 s | 39.1 ± 4.4 s | 21.6 ± 6.7% |
| E1-rSMS | 58.1 ± 18.5 s | 46.1 ± 3.8 s | 19.5 ± 5.1% |
| E1-sham-spinal | 52.5 ± 8.4 s | 43.2 ± 9.0 s | 18.2 ± 5.1% |
| no-stimulation | 59.6 ± 10.2 s | 49.8 ± 8.9 s | 16.3 ± 5.8% |
| E1 Groups | Mean Time Pre-Test | Mean Time Post-Test | Increase in % |
|---|---|---|---|
| E1-rTMS | 32.4 ± 2.5 s | 30.3 ± 2.7 s | 6.2 ± 8.2% |
| E1-rSMS | 39.1 ± 9.7 s | 34.0 ± 7.9 s | 12.8 ± 4.4% |
| E1-sham-spinal | 32.2 ± 2.9 s | 29.5 ± 2.1 s | 8.1 ± 6.0% |
| no-stimulation | 39.6 ± 5.4 s | 37.5 ± 6.2 s | 5.7 ± 5.8% |
| E1 Groups | JTT Left Hand | JTT Right Hand |
|---|---|---|
| E1-rTMS | 4.0 × 10−7 | 0.009 |
| E1-rSMS | 1.2 × 10−6 | 1.6 × 10−6 |
| E1-sham-spinal | 2.0 × 10−8 | 0.0003 |
| no-stimulation | 1.8 × 10−7 | 0.002 |
| E1 Groups | E1-rTMS | E1-rSMS | E1-Sham-Spinal |
|---|---|---|---|
| E1-rTMS | - | - | - |
| E1-rSMS | 0.4 | - | - |
| E1-sham-spinal | 0.6 | 0.3 | - |
| no-stimulation | 0.8 | 0.6 | 0.4 |
| E2 Groups | Mean Time Pre-Test | Mean Time Post-Test | Increase in % |
|---|---|---|---|
| E2-rTMS | 54.4 ± 8.2 s | 41.1 ± 5.1 s | 24.1 ± 5.6% |
| E2-rSMS | 50.5 ± 4.4 s | 39.4 ± 3.7 s | 21.9 ± 6.3% |
| E2-sham-spinal | 51.9 ± 6.6 s | 41.8 ± 5.3 s | 19.2 ± 5.0% |
| E2 Groups | Mean Time Pre-Test | Mean Time Post-Test | Increase in % |
|---|---|---|---|
| E2-rTMS | 34.6 ± 2.7 s | 32.3 ± 3.9 s | 6.8 ± 6.6% |
| E2-rSMS | 34.8 ± 3.4 s | 31.5 ± 3.0 s | 9.4 ± 2.9% |
| E2-sham-spinal | 33.7 ± 2.5 s | 30.6 ± 2.9 s | 9.3 ± 6.0% |
| E2 Groups | JTT Left Hand | JTT Right Hand |
| E2-rTMS | 3.1 × 10−8 | 0.0007 |
| E2-rSMS | 1.0 × 10−9 | 2.6 × 10−7 |
| E2-sham-spinal | 3.1 × 10−6 | 1.3 × 10−5 |
| E2 Groups | E1-rTMS | E1-rSMS |
|---|---|---|
| E2-rTMS | - | - |
| E2-rSMS | 0.4 | - |
| E2-sham-spinal | 0.9 | 0.5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hamzei, F.; Ritter, A.; Pohl, K.; Stäps, P.; Wieduwild, E. Different Effect Sizes of Motor Skill Training Combined with Repetitive Transcranial versus Trans-Spinal Magnetic Stimulation in Healthy Subjects. Brain Sci. 2024, 14, 165. https://doi.org/10.3390/brainsci14020165
Hamzei F, Ritter A, Pohl K, Stäps P, Wieduwild E. Different Effect Sizes of Motor Skill Training Combined with Repetitive Transcranial versus Trans-Spinal Magnetic Stimulation in Healthy Subjects. Brain Sciences. 2024; 14(2):165. https://doi.org/10.3390/brainsci14020165
Chicago/Turabian StyleHamzei, Farsin, Alexander Ritter, Kristin Pohl, Peggy Stäps, and Eric Wieduwild. 2024. "Different Effect Sizes of Motor Skill Training Combined with Repetitive Transcranial versus Trans-Spinal Magnetic Stimulation in Healthy Subjects" Brain Sciences 14, no. 2: 165. https://doi.org/10.3390/brainsci14020165
APA StyleHamzei, F., Ritter, A., Pohl, K., Stäps, P., & Wieduwild, E. (2024). Different Effect Sizes of Motor Skill Training Combined with Repetitive Transcranial versus Trans-Spinal Magnetic Stimulation in Healthy Subjects. Brain Sciences, 14(2), 165. https://doi.org/10.3390/brainsci14020165