
Is Virtual Reality Orientation Therapy Useful to Optimize Cognitive and Behavioral Functioning Following Severe Acquired Brain Injury? An Exploratory Study

 , ,
, ,  , , , , , and
, , , , , and 
Abstract
:1. Introduction
1.1. Severe Acquired Brain Injury
1.2. Cognitive Rehabilitation
1.3. Reality Orientation Therapy
1.4. Virtual Reality
2. Materials and Methods
2.1. Study Population
2.2. Procedures
2.3. Psychometric Measures
2.4. Standard ROT
2.5. Virtual ROT
2.6. Statistical Analysis
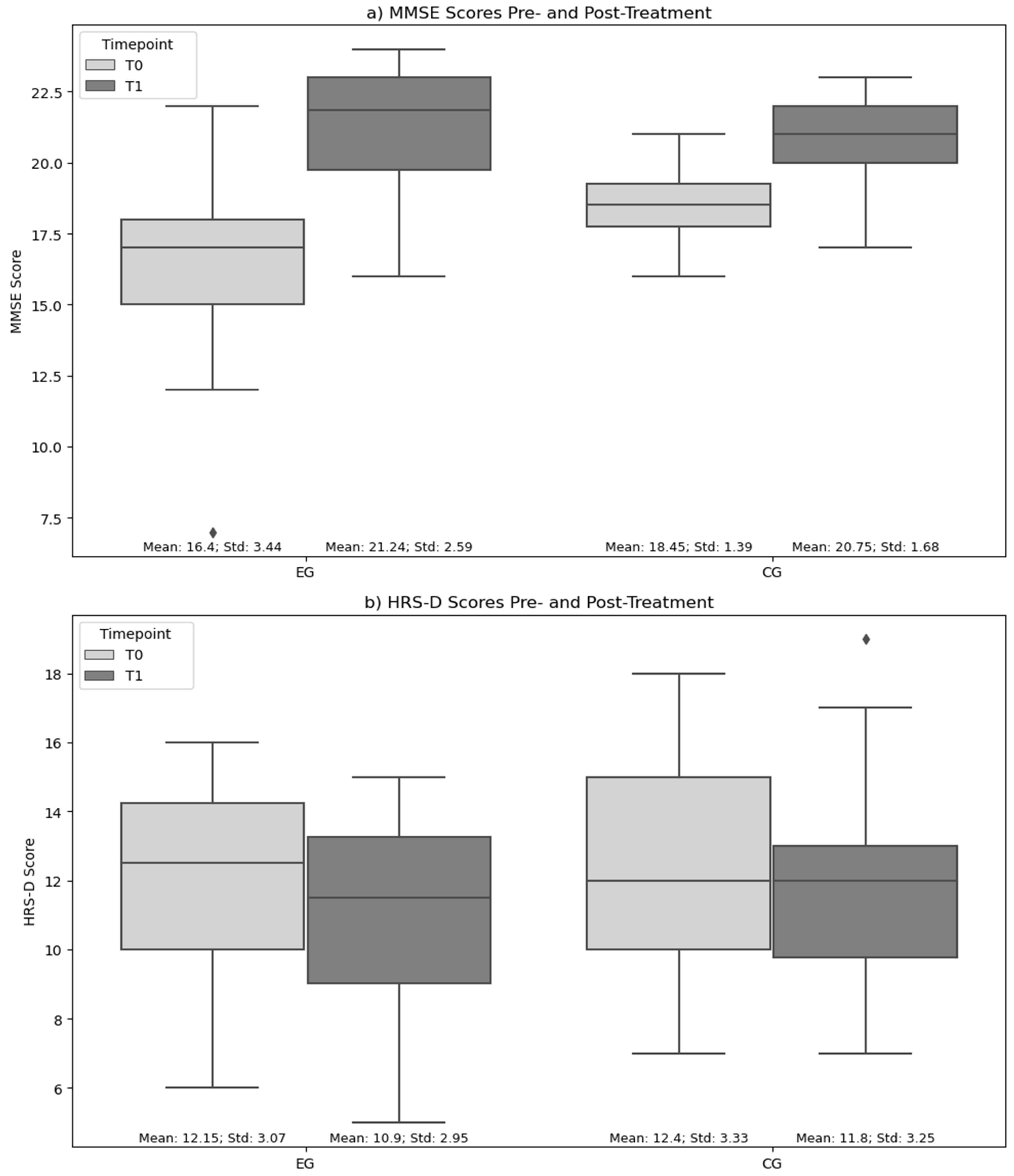
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Middleton, J.A. Acquired brain injury. Psychiatry 2008, 7, 304–307. [Google Scholar] [CrossRef]
- Turner-Stokes, L.; Pick, A.; Nair, A.; Disler, P.B.; Wade, D.T. Multi-disciplinary rehabilitation for acquired brain injury in adults of working age. Cochrane Database Syst. Rev. 2015, 2015, CD004170. [Google Scholar] [CrossRef] [PubMed]
- Hall, R.C.; Hall, R.C.; Chapman, M.J. Definition, diagnosis, and forensic implications of postconcussional syndrome. Psychosomatics 2005, 46, 195–202. [Google Scholar] [CrossRef] [PubMed]
- Holmqvist, K.; Kamwendo, K.; Ivarsson, A.B. Occupational therapists’ descriptions of their work with persons suffering from cognitive impairment following acquired brain injury. Scand. J. Occup. Ther. 2009, 16, 13–24. [Google Scholar] [CrossRef] [PubMed]
- Yip, B.C.; Man, D.W. Virtual reality (VR)-based community living skills training for people with acquired brain injury: A pilot study. Brain Inj. 2009, 23, 1017–1026. [Google Scholar] [CrossRef] [PubMed]
- Teasdale, G.; Maas, A.; Lecky, F.; Manley, G.; Stocchetti, N.; Murray, G. The Glasgow Coma Scale at 40 years: Standing the test of time. Lancet Neurol. 2014, 13, 844–854. [Google Scholar] [CrossRef] [PubMed]
- Alves, D.E.; Nilsen, W.; Fure SC, R.; Enehaug, H.; Howe, E.I.; Løvstad, M.; Fink, L.; Andelic, N.; Spjelkavik, Ø. What characterises work and workplaces that retain their employees following acquired brain injury? Systematic review. Occup. Environ. Med. 2020, 77, 122–130. [Google Scholar] [CrossRef] [PubMed]
- Fusco, A.; Galluccio, C.; Castelli, L.; Pazzaglia, C.; Pastorino, R.; Pires Marafon, D.; Bernabei, R.; Giovannini, S.; Padua, L. Severe Acquired Brain Injury: Prognostic Factors of Discharge Outcome in Older Adults. Brain Sci. 2022, 12, 1232. [Google Scholar] [CrossRef] [PubMed]
- Apperly, I.A.; Samson, D.; Chiavarino, C.; Humphreys, G.W. Frontal and temporo-parietal lobe contributions to theory of mind: Neuropsychological evidence from a false-belief task with reduced language and executive demands. J. Cogn. Neurosci. 2004, 16, 1773–1784. [Google Scholar] [CrossRef]
- Henry, J.D.; Phillips, L.H.; Crawford, J.R.; Ietswaart, M.; Summers, F. Theory of mind following traumatic brain injury: The role of emotion recognition and executive dysfunction. Neuropsychologia 2006, 44, 1623–1628. [Google Scholar] [CrossRef]
- Milders, M.; Ietswaart, M.; Crawford, J.R.; Currie, D. Impairments in theory of mind shortly after traumatic brain injury and at 1-year follow-up. Neuropsychology 2006, 20, 400–408. [Google Scholar] [CrossRef]
- de Sousa, A.; McDonald, S.; Rushby, J.; Li, S.; Dimoska, A.; James, C. Why don’t you feel how I feel? Insight into the absence of empathy after severe traumatic brain injury. Neuropsychologia 2010, 48, 3585–3595. [Google Scholar] [CrossRef]
- Spikman, J.M.; Timmerman, M.E.; Milders, M.V.; Veenstra, W.S.; van der Naalt, J. Social cognition impairments in relation to general cognitive deficits, injury severity, and prefrontal lesions in traumatic brain injury patients. J. Neurotrauma 2012, 29, 101–111. [Google Scholar] [CrossRef] [PubMed]
- Dahm, J.; Ponsford, J. Comparison of long-term outcomes following traumatic injury: What is the unique experience for those with brain injury compared with orthopaedic injury? Injury 2015, 46, 142–149. [Google Scholar] [CrossRef] [PubMed]
- Bornhofen, C.; McDonald, S. Emotion perception deficits following traumatic brain injury: A review of the evidence and rationale for intervention. J. Int. Neuropsychol. Soc. 2008, 14, 511–525. [Google Scholar] [CrossRef]
- Borgaro, S.R.; Prigatano, G.P. Early cognitive and affective sequelae of traumatic brain injury: A study using the BNI Screen for Higher Cerebral Functions. J. Head Trauma Rehabil. 2002, 17, 526–534. [Google Scholar] [CrossRef]
- Whelan-Goodinson, R.; Ponsford, J.; Schönberger, M. Validity of the Hospital Anxiety and Depression Scale to assess depression and anxiety following traumatic brain injury as compared with the Structured Clinical Interview for DSM-IV. J. Affect. Disord. 2009, 114, 94–102. [Google Scholar] [CrossRef] [PubMed]
- Spector, A.; Davies, S.; Woods, B.; Orrell, M. Orientamento alla realtà per la demenza: Una revisione sistematica delle prove di efficacia da studi randomizzati e controllati. Il Gerontol. 2000, 40, 206–212. [Google Scholar] [CrossRef]
- Anghinah, R.; Amorim, R.L.O.; Paiva, W.S.; Schmidt, M.T.; Ianof, J.N. Traumatic brain injury pharmacological treatment: Recommendations. Arq. Neuro-Psiquiatr. 2018, 76, 100–103. [Google Scholar] [CrossRef]
- De Luca, R.; Calabrò, R.S.; Bramanti, P. Cognitive rehabilitation after severe acquired brain injury: Current evidence and future directions. Neuropsychol. Rehabil. 2018, 28, 879–898. [Google Scholar] [CrossRef]
- Palmese, C.A.; Raskin, S.A. The rehabilitation of attention in individuals with mild traumatic brain injury, using the APT-II programme. Brain Inj. 2000, 14, 535–548. [Google Scholar] [CrossRef] [PubMed]
- Zencius, A.H.; Wesolowski, M.D.; Rodriguez, I.M. Improving orientation in head injured adults by repeated practice, multi-sensory input and peer participation. Brain Inj. 1998, 12, 53–61. [Google Scholar] [CrossRef]
- Moore, S.; Sandman, C.A.; McGrady, K.; Kesslak, J.P. Memory training improves cognitive ability in patients with dementia. Neuropsychol. Rehabil. 2001, 11, 245–261. [Google Scholar] [CrossRef]
- Quayhagen, M.P.; Quayhagen, M.; Corbeil, R.R.; Hendrix, R.C.; Jackson, J.E.; Snyder, L.; Bower, D. Coping with dementia: Evaluation of four nonpharmacologic interventions. Int. Psychogeriatr. 2000, 12, 249–265. [Google Scholar] [CrossRef]
- Veneziani, I.; Marra, A.; Formica, C.; Grimaldi, A.; Marino, S.; Quartarone, A.; Maresca, G. Applications of Artificial Intelligence in the Neuropsychological Assessment of Dementia: A Systematic Review. J. Pers. Med. 2024, 14, 113. [Google Scholar] [CrossRef] [PubMed]
- Sohlberg, M.M.; Mateer, C.A. Introduction to Cognitive Rehabilitation: Theory and Practice; Guilford Press: New York, NY, USA, 1989. [Google Scholar]
- Wood, R.L.; Fussey, I. Cognitive Rehabilitation in Perspective; Taylor and Francis: London, UK, 1990. [Google Scholar]
- Patrice, R.K.; Weiss, L.; Feintuch, U.; Katz, N.; Weiss, P.L. Virtual Reality in Neurorehabilitation. In Textbook of Neural Repair and Rehabilitation; Cambridge University Press: Cambridge, UK, 2006. [Google Scholar]
- Knight, R.G.; Titov, N. Use of virtual reality tasks to assess prospective memory: Applicability and evidence. Brain Impair. 2009, 10, 3–13. [Google Scholar] [CrossRef]
- Maggio, M.G.; De Luca, R.; Molonia, F.; Porcari, B.; Destro, M.; Casella, C.; Salvati, R.; Bramanti, P.; Calabro, R.S. Cognitive rehabilitation in patients with traumatic brain injury: A narrative review on the emerging use of virtual reality. J. Clin. Neurosci. 2019, 61, 1–4. [Google Scholar] [CrossRef]
- De Luca, R.; Bonanno, M.; Marra, A.; Rifici, C.; Pollicino, P.; Caminiti, A.; Castorina, M.V.; Santamato, A.; Quartarone, A.; Calabrò, R.S. Can Virtual Reality Cognitive Rehabilitation Improve Executive Functioning and Coping Strategies in Traumatic Brain Injury? A Pilot Study. Brain Sci. 2019, 13, 578. [Google Scholar] [CrossRef]
- Pennington, D.L.; Reavis, J.V.; Cano, M.T.; Walker, E.; Batki, S.L. L’impatto dell’esercizio fisico e della formazione sulla funzione esecutiva della realtà virtuale sulla cognizione tra i veterani del consumo eccessivo di alcolici con lesioni cerebrali traumatiche: Uno studio pilota di fattibilità. Davanti. Comport. Neurosci. 2022, 16, 802711. [Google Scholar] [CrossRef]
- Maresca, G.; Leonardi, S.; De Cola, M.C.; Giliberto, S.; Di Cara, M.; Corallo, F.; Quartarone, A.; Pidalà, A. Use of Virtual Reality in Children with Dyslexia. Children 2022, 9, 1621. [Google Scholar] [CrossRef]
- Koepp, M.J.; Gunn, R.N.; Lawrence, A.D.; Cunningham, V.J.; Dagher, A.; Jones, T.; Brooks, D.J.; Bench, C.J.; Grasby, P.M. Evidence for striatal dopamine release during a video game. Nature 1998, 393, 266–268. [Google Scholar] [CrossRef]
- Liu, H.; Cheng, Z.; Wang, S.; Jia, Y. Effects of virtual reality-based intervention on depression in stroke patients: A meta-analysis. Sci. Rep. 2023, 13, 4381. [Google Scholar] [CrossRef]
- Petersen, R.C.; Stevens, J.C.; Ganguli, M.; Tangalos, E.G.; Cummings, J.L.; DeKosky, S.T. Practice parameter: Early detection of dementia: Mild cognitive impairment (an evidence-based review). Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 2001, 56, 1133–1142. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Hamilton, M. Development of a rating scale for primary depressive illness. Br. J. Soc. Clin. Psychol. 1967, 6, 278–296. [Google Scholar] [CrossRef]
- Cappadona, I.; Ielo, A.; La Fauci, M.; Tresoldi, M.; Settimo, C.; De Cola, M.C.; Muratore, R.; De Domenico, C.; Di Cara, M.; Corallo, F.; et al. Feasibility and Effectiveness of Speech Intervention Implemented with a Virtual Reality System in Children with Developmental Language Disorders: A Pilot Randomized Control Trial. Children 2023, 10, 1336. [Google Scholar] [CrossRef] [PubMed]
- Castelli, L.; Iacovelli, C.; Fusco, A.; Amoruso, V.; Cuccagna, C.; Loreti, C.; Giovannini, S.; Padua, L. The Role of Technological Rehabilitation in Patients with Intensive Care Unit Weakness: A Randomized Controlled Pilot Study. J. Clin. Med. 2023, 12, 2612. [Google Scholar] [CrossRef]
- Peng, Q.C.; Yin, L.; Cao, Y. Effectiveness of Virtual Reality in the Rehabilitation of Motor Function of Patients with Subacute Stroke: A Meta-Analysis. Front. Neurol. 2021, 12, 639535. [Google Scholar] [CrossRef] [PubMed]
- Kober, S.E.; Wood, G.; Hofer, D.; Kreuzig, W.; Kiefer, M.; Neuper, C. Virtual reality in neurologic rehabilitation of spatial disorientation. J. Neuroeng. Rehabil. 2013, 10, 17. [Google Scholar] [CrossRef]
- Huygelier, H.; Schraepen, B.; Lafosse, C.; Vaes, N.; Schillebeeckx, F.; Michiels, K.; Note, E.; Vanden Abeele, V.; van Ee, R.; Gillebert, C.R. An immersive virtual reality game to train spatial attention orientation after stroke: A feasibility study. Applied neuropsychology. Adult 2022, 29, 915–935. [Google Scholar] [CrossRef]
- Painter, D.R.; Norwood, M.F.; Marsh, C.H.; Hine, T.; Harvie, D.; Libera, M.; Bernhardt, J.; Gan, L.; Zeeman, H. Immersive virtual reality gameplay detects visuospatial atypicality, including unilateral spatial neglect, following brain injury: A pilot study. J. Neuroeng. Rehabil. 2023, 20, 161. [Google Scholar] [CrossRef] [PubMed]
- Onieva-Zafra, M.D.; Hernández-Garcia, L.; Gonzalez-Del-Valle, M.T.; Parra-Fernández, M.L.; Fernandez-Martinez, E. Music Intervention with Reminiscence Therapy and Reality Orientation for Elderly People with Alzheimer Disease Living in a Nursing Home: A Pilot Study. Holist. Nurs. Pract. 2018, 32, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Li, J.; Liang, T.; Hasan, W.U.; Zaman, K.T.; Du, Y.; Xie, B.; Tao, C. Promoting Personalized Reminiscence Among Cognitively Intact Older Adults Through an AI-Driven Interactive Multimodal Photo Album: Development and Usability Study. JMIR Aging 2024, 7, e49415. [Google Scholar] [CrossRef] [PubMed]
- Aguirre, E.; Woods, R.T.; Spector, A.; Orrell, M. Cognitive stimulation for dementia: A systematic review of the evidence of effectiveness from randomised controlled trials. Ageing Res. Rev. 2013, 12, 253–262. [Google Scholar] [CrossRef] [PubMed]
- Chiu, H.Y.; Chen, P.Y.; Chen, Y.T.; Huang, H.C. Reality orientation therapy benefits cognition in older people with dementia: A meta-analysis. Int. J. Nurs. Stud. 2018, 86, 20–28. [Google Scholar] [CrossRef] [PubMed]
- Kume, Y.; Nagaoka, M.; Uemura, S.; Saito, A.; Tsugaruya, M.; Fujita, T.; Terui, Y.; Kodama, A.; Sato, A.; Ota, H.; et al. Effect of a multicomponent programme based on reality orientation therapy on the physical performance and cognitive function of elderly community-dwellers: A quasi-experimental study. Psychogeriatrics 2023, 23, 847–855. [Google Scholar] [CrossRef] [PubMed]
- Tadaka, E.; Kanagawa, K. A randomized controlled trial of a group care program for community-dwelling elderly people with dementia. Jpn. J. Nurs. Sci. 2004, 1, 19–25. [Google Scholar] [CrossRef]
- Camargo, C.H.F.; Ladeira, M.A.; Serpa, R.A.; Jobbins, V.A.; Filho, C.R.P.; Welling, L.C.; Teive, H.A.G. The Effectiveness of Reality Orientation Therapy in the Treatment of Parkinson Disease Dementia. Am. J. Alzheimer’s Dis. Other Dement. 2018. advance online publication. [Google Scholar] [CrossRef] [PubMed]
- Alashram, A.R.; Annino, G.; Padua, E.; Romagnoli, C.; Mercuri, N.B. Cognitive rehabilitation post traumatic brain injury: A systematic review for emerging use of virtual reality technology. J. Clin. Neurosci. 2019, 66, 209–219. [Google Scholar] [CrossRef]
- Leonardi, S.; Maggio, M.G.; Russo, M.; Bramanti, A.; Arcadi, F.A.; Naro, A.; Calabrò, R.S.; De Luca, R. Cognitive recovery in people with relapsing/remitting multiple sclerosis: A randomized clinical trial on virtual reality-based neurorehabilitation. Clin. Neurol. Neurosurg. 2021, 208, 106828. [Google Scholar] [CrossRef]
- Alemanno, F.; Houdayer, E.; Emedoli, D.; Locatelli, M.; Mortini, P.; Mandelli, C.; Raggi, A.; Iannaccone, S. Efficacy of virtual reality to reduce chronic low back pain: Proof-of-concept of a non-pharmacological approach on pain, quality of life, neuropsychological and functional outcome. PLoS ONE 2019, 14, e0216858. [Google Scholar] [CrossRef] [PubMed]
- Demeco, A.; Zola, L.; Frizziero, A.; Martini, C.; Palumbo, A.; Foresti, R.; Buccino, G.; Costantino, C. Immersive Virtual Reality in Post-Stroke Rehabilitation: A Systematic Review. Sensors 2023, 23, 1712. [Google Scholar] [CrossRef] [PubMed]
- Tieri, G.; Morone, G.; Paolucci, S.; Iosa, M. Virtual reality in cognitive and motor rehabilitation: Facts, fiction and fallacies. Expert Rev. Med. Devices 2018, 15, 107–117. [Google Scholar] [CrossRef]
- Sanchez-Vives, M.V.; Slater, M. From presence to consciousness through virtual reality. Nat. Rev. Neurosci. 2005, 6, 332–339. [Google Scholar] [CrossRef]
- Benabid, A.L.; Costecalde, T.; Eliseyev, A.; Charvet, G.; Verney, A.; Karakas, S.; Foerster, M.; Lambert, A.; Morinière, B.; Abroug, N.; et al. An exoskeleton controlled by an epidural wireless brain-machine interface in a tetraplegic patient: A proof-of-concept demonstration. Lancet Neurol. 2019, 18, 1112–1122. [Google Scholar] [CrossRef]
- Pais-Vieira, C.; Figueiredo, J.G.; Perrotta, A.; Matos, D.; Aguiar, M.; Ramos, J.; Gato, M.; Poleri, T.; Pais-Vieira, M. Activation of a Rhythmic Lower Limb Movement Pattern during the Use of a Multimodal Brain-Computer Interface: A Case Study of a Clinically Complete Spinal Cord Injury. Life 2024, 14, 396. [Google Scholar] [CrossRef] [PubMed]
- Lindner, P.; Miloff, A.; Fagernäs, S.; Andersen, J.; Sigeman, M.; Andersson, G.; Furmark, T.; Carlbring, P. Therapist-led and self-led one-session virtual reality exposure therapy for public speaking anxiety with consumer hardware and software: A randomized controlled trial. J. Anxiety Disord. 2019, 61, 45–54. [Google Scholar] [CrossRef]
- Sunkara, C.; Thakkar, R.; Ong, T.; Bunnell, B.E. Characterizing Consumer Smartphone Apps for Virtual Reality-Based Exposure Therapy: Content Analysis. J. Med. Internet Res. 2023, 25, e41807. [Google Scholar] [CrossRef]
- Wiley, E.; Khattab, S.; Tang, A. Examining the effect of virtual reality therapy on cognition post-stroke: A systematic review and meta-analysis. Disabil. Rehabil. Assist. Technol. 2022, 17, 50–60. [Google Scholar] [CrossRef]
- Impellizzeri, F.; Naro, A.; Basile, G.; Bramanti, A.; Gazia, F.; Galletti, F.; Militi, D.; Petralito, F.; Calabrò, R.S.; Milardi, D. Does cybersickness affect virtual reality training using the Computer Assisted Rehabilitation Environment (CAREN)? Preliminary results from a case-control study in Parkinson’s disease. Physiother. Theory Pract. 2022, 38, 2603–2611. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| All | EG | CG | p-Value | |
|---|---|---|---|---|
| Participants | 40 | 20 (50.0) | 20 (50.0) | - |
| Male | 21 (52.5) | 10 (50.0) | 11 (55.0) | 1.00 |
| Age (years) | 46.17 ± 15.02 | 47.30 ± 14.03 | 45.05 ± 16.23 | 0.64 |
| Education (years) | 10.15 ± 3.11 | 10.65 ± 2.98 | 9.65 ± 3.23 | 0.32 |
| Rehabilitation Program | Intervention | Individual Session Duration | Type of Intervention | Exercise Time | Cognitive Domains |
|---|---|---|---|---|---|
| 3-month standard approach, paper and pencil, face to face | S-ROT + Psychological support | 3 weekly sessions of 60 min | S-ROT (45 min) | 15 min 15 min 15 min | Personal/autobiographical orientation Temporal orientation Spatial orientation |
| Psychological Support | 15 min | Motivation and mood | |||
| 3-month virtual approach VRRS interface | VR-ROT + Psychological support | 3 weekly sessions of 60 min | V-ROT (45 min) | The same exercise time as the conventional ROT training group. | The same cognitive domains as the conventional ROT training group. |
| Psychological Support |
| Domain | Sub Domains | Short Description | Standard Tasks Paper-and-Pencil Approach— Human Interface | Virtual Activities Virtual-PC-Based Interface |
|---|---|---|---|---|
| ORIENTATION | Personal Orientation | The capacity to combine information related to our personal history and identity, including our age, civil status, or education level. | Activities that require patients to answer a series of questions about their personal life have been designed to rehabilitate personal orientation, with varying levels of difficulty and assistance depending on the patient’s specific needs. The objective is to observe and select the usual stimuli that are given, which may include photos (of friends, pets, etc.) that are emotionally meaningful for patients. Audio–video materials, like voice recordings of family, friends, and colleagues, can also be used to listen to emotional–meaningful songs or to observe preferred scenes from favored movies or videos about personal life events (such as childbirth, significant events, etc.). | Virtual activities have been developed to improve personal orientation by requiring patients to answer a series of questions about their personal life. The patient’s specific needs can affect the level of difficulty and assistance provided for these virtual tasks. Emotional virtual images, such as personal settings or biographical virtual photos (about their home, wife, mother...), can be viewed and selected. Using VRRS integrated to the virtual system, patients can listen to to affective audio–video materials such as voice recordings of family members, music tracks that are emotionally meaningful, a main list of favorite movie scenes, and videos of personal life scenes (birth of children, significant personal events in life). |
| Spatial Orientation | The capacity to manage information concerning one’s starting point, current location, destination, etc. | In the program for spatial orientation, patients were taught to connect different objects to the places where they can be bought and the professionals who work there through exercises. The aim was to promote spatial awareness by recalling memories of places, cities, or streets, using impromptu paper-and-pencil materials. This involved conducting visual–spatial tasks and spatial awareness exercises, resolving traditional puzzles, identifying the location of 2D objects (center, right–left), drawing activities, and recognizing shapes and spatial relationships. | Spatial orientation was addressed in the virtual program by incorporating virtual exercises that involved patients connecting objects to places where they can be purchased and the professionals who work there. In order to foster spatial orientation in a virtual environment and promote topographic sense and perception, virtual reasoning activities can be used to recognize places, cities, and different locations. This can include managing virtual orientation tasks, completing spatial awareness activities by completing virtual puzzles or adjusting the position of virtual elements (center, right–left), and exploring interactive maps and shapes through virtual drawing or painting. | |
| Temporal Orientation | The ability to keep track of information about various events or situations and arrange it in chronological order. It encompasses information related to the day, time, month, year, and the moment of engaging in certain behaviors, holidays, seasons, etc. | Tasks that require patients to provide information on the time, month, and seasons of the year are designed to improve temporal orientation. Managing information about days, times, and months can be achieved by using the repetition and recall of specific information, like personal data and events, in conjunction with face-to-face activities to increase temporal orientation abilities. SABI patients are required to provide the time, day, month, year, and current season in this activity, with the option to select the month they are currently in during the exercise. | Virtual tasks are available to patients to improve their temporal orientation by requiring them to tell the time, month, and season of the year. Increasing temporal orientation abilities can be achieved by repeating and recalling specific information, such as personal data and personal events; managing information related to days, times, and months; and utilizing VVRs and virtual environments. VR is used to continuously transmit information through visual, written, or auditory modes. |
| EG | CG | |||
|---|---|---|---|---|
| Median (1st Qu.–3rd Qu.) | Median (1st Qu.–3rd Qu.) | p-Value | ||
| MMSE | T0 | 17.00 (15.00–18.00) | 18.5 (17.75–19.25) | 0.021 |
| T1 | 21.85 (19.75–23.00) | 21.00 (20.00–22.00) | 0.251 | |
| p-value | <0.001 | <0.001 | ||
| HRS-D | T0 | 12.50 (10.00–14.25) | 12.00 (10.00–15.00) | 0.806 |
| T1 | 11.50 (10.00–16.00) | 12.00 (9.75–13.00) | 0.366 | |
| p-value | <0.001 | 0.124 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Luca, R.; Calderone, A.; Gangemi, A.; Rifici, C.; Bonanno, M.; Maggio, M.G.; Cappadona, I.; Veneziani, I.; Ielo, A.; Corallo, F.; et al. Is Virtual Reality Orientation Therapy Useful to Optimize Cognitive and Behavioral Functioning Following Severe Acquired Brain Injury? An Exploratory Study. Brain Sci. 2024, 14, 410. https://doi.org/10.3390/brainsci14050410
De Luca R, Calderone A, Gangemi A, Rifici C, Bonanno M, Maggio MG, Cappadona I, Veneziani I, Ielo A, Corallo F, et al. Is Virtual Reality Orientation Therapy Useful to Optimize Cognitive and Behavioral Functioning Following Severe Acquired Brain Injury? An Exploratory Study. Brain Sciences. 2024; 14(5):410. https://doi.org/10.3390/brainsci14050410
Chicago/Turabian StyleDe Luca, Rosaria, Andrea Calderone, Antonio Gangemi, Carmela Rifici, Mirjam Bonanno, Maria Grazia Maggio, Irene Cappadona, Isabella Veneziani, Augusto Ielo, Francesco Corallo, and et al. 2024. "Is Virtual Reality Orientation Therapy Useful to Optimize Cognitive and Behavioral Functioning Following Severe Acquired Brain Injury? An Exploratory Study" Brain Sciences 14, no. 5: 410. https://doi.org/10.3390/brainsci14050410
APA StyleDe Luca, R., Calderone, A., Gangemi, A., Rifici, C., Bonanno, M., Maggio, M. G., Cappadona, I., Veneziani, I., Ielo, A., Corallo, F., Quartarone, A., Cardile, D., & Calabrò, R. S. (2024). Is Virtual Reality Orientation Therapy Useful to Optimize Cognitive and Behavioral Functioning Following Severe Acquired Brain Injury? An Exploratory Study. Brain Sciences, 14(5), 410. https://doi.org/10.3390/brainsci14050410