
Inhibitory Control under Threat: The Role of Spontaneous Eye Blinks in Post-Traumatic Stress Disorder


Abstract
:1. Introduction
1.1. Spontaneous Eye Blink Rate (sEBR)
1.2. The Present Study
2. Methods
2.1. Participants
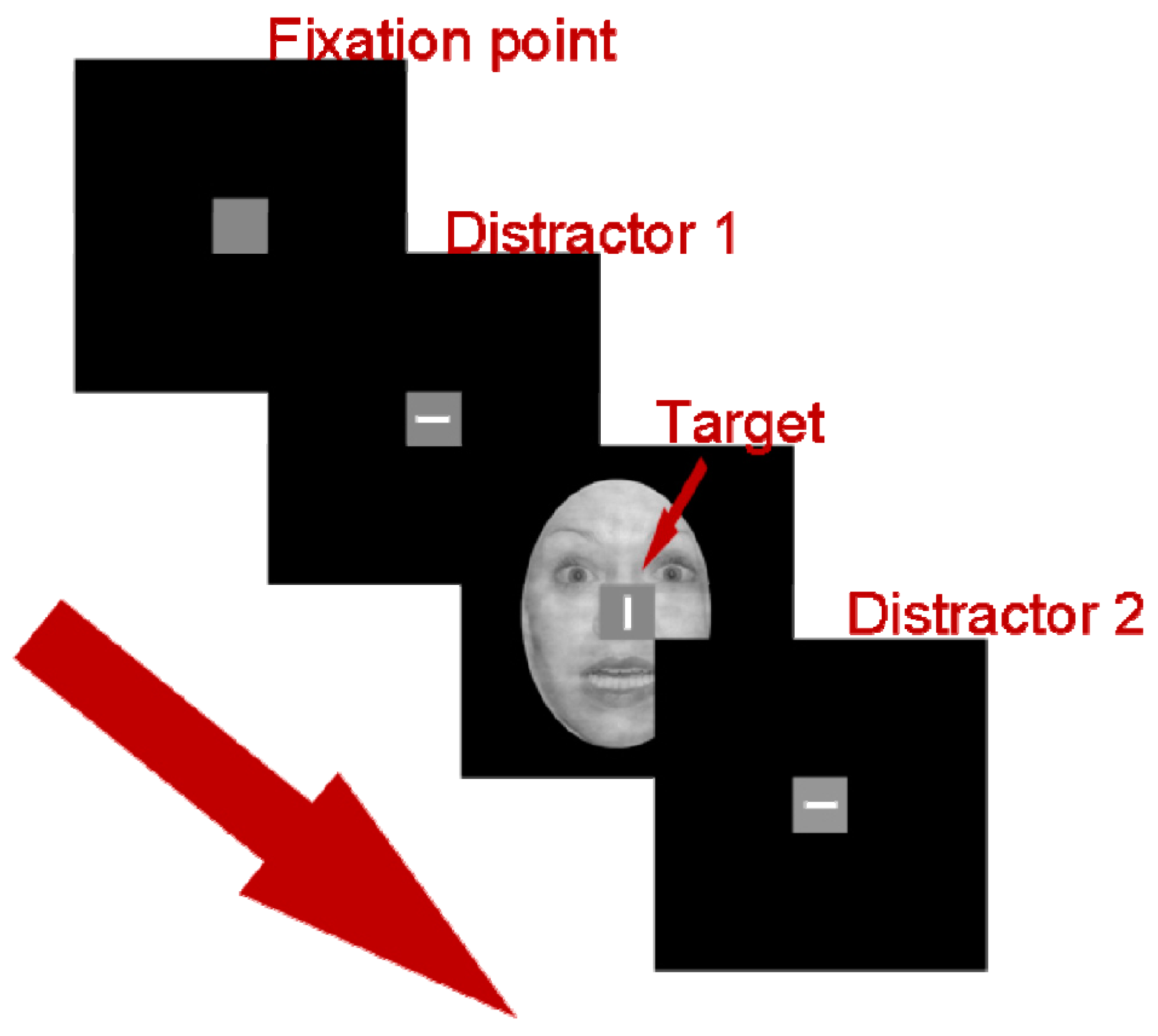
2.2. Stimulus, Apparatus, and Procedure
2.3. Data Recording and Analysis
3. Results
3.1. Demographic, Clinical, Physiological, and Behavioral Data
3.2. Inhibitory Control
3.3. Clinical Subscales
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Disclaimer
References
- Kessler, R.C.; Chiu, W.T.; Demler, O.; Merikangas, K.R.; Walters, E.E. Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the National Comorbidity Survey Replication. Arch. Gen. Psychiatry 2005, 62, 617–627. [Google Scholar] [CrossRef] [PubMed]
- Harrington, K.M.; Miller, M.W.; Wolf, E.J.; Reardon, A.F.; Ryabchenko, K.A.; Ofrat, S. Attention-deficit/hyperactivity disorder comorbidity in a sample of veterans with posttraumatic stress disorder. Compr. Psychiatry 2012, 53, 679–690. [Google Scholar] [CrossRef] [PubMed]
- Leskin, L.P.; White, P.M. Attentional networks reveal executive function deficits in posttraumatic stress disorder. Neuropsychology 2007, 21, 275–284. [Google Scholar] [CrossRef] [PubMed]
- Swick, D.; Honzel, N.; Larsen, J.; Ashley, V.; Justus, T. Impaired Response Inhibition in Veterans with Post-Traumatic Stress Disorder and Mild Traumatic Brain Injury. J. Int. Neuropsychol. Soc. 2012, 18, 917–926. [Google Scholar] [CrossRef] [PubMed]
- Clark, C.R.; Mcfarlane, A.C.; Morris, P.; Weber, D.L.; Sonkkilla, C.; Shaw, M.; Marcina, J.; Egan, G.F. Cerebral Function in Posttraumatic Stress Disorder during Verbal Working Memory Updating: A Positron Emission Tomography Study. Biol. Psychiatry 2003, 53, 474–481. [Google Scholar] [CrossRef]
- Walrath, L.C.; Goldstein, R.; Stern, J.A. The Endogenous Eyeblink. Psychophysiology 1984, 21, 22–34. [Google Scholar]
- Bristow, D.; Haynes, J.-D.; Sylvester, R.; Frith, C.D.; Rees, G. Blinking suppresses the neural response to unchanging retinal stimulation. Curr. Biol. 2005, 15, 1296–1300. [Google Scholar] [CrossRef] [PubMed]
- Yoon, H.W.; Chung, J.-Y.; Song, M.-S.; Park, H. Neural correlates of eye blinking; improved by simultaneous fMRI and EOG measurement. Neurosci. Lett. 2005, 381, 26–30. [Google Scholar] [CrossRef] [PubMed]
- Halgren, E.; Baudena, P.; Clarke, J.M.; Heit, G.; Liégeois, C.; Chauvel, P.; Musolino, A. Intracerebral potentials to rare target and distractor auditory and visual stimuli. I. Superior temporal plane and parietal lobe. Electroencephalogr. Clin. Neurophysiol. 1995, 94, 191–220. [Google Scholar] [CrossRef]
- Knight, R.T.; Scabini, D.; Woods, D.L.; Clayworth, C.C. Contributions of temporal-parietal junction to the human auditory P3. Brain Res. 1989, 502, 109–116. [Google Scholar] [CrossRef]
- Halgren, E.; Marinkovic, K.; Chauvel, P. Generators of the late cognitive potentials in auditory and visual oddball tasks. Electroencephalogr. Clin. Neurophysiol. 1998, 106, 156–164. [Google Scholar] [CrossRef]
- Ridderinkhof, K.R.; Ullsperger, M.; Crone, E.A.; Nieuwenhuis, S. The role of the medial frontal cortex in cognitive control. Science 2004, 306, 443–447. [Google Scholar] [CrossRef] [PubMed]
- Karson, C.N.; Kleinman, J.E.; Berman, K.F.; Phelps, B.H. An inverse correlation between spontaneous eye-blink rate and platelet monoamine oxidase activity. Br. J. Psychiatry 1983, 142, 43–46. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, M.S.; Redmond, D.E. MPTP lesions and dopaminergic drugs alter eye blink rate in African green monkeys. Pharmacol. Biochem. Behav. 1991, 38, 869–874. [Google Scholar] [CrossRef]
- Elsworth, J.D.; Lawrence, M.S.; Roth, R.H.; Taylor, J.R.; Mailman, R.B.; Nichols, D.E.; Lewis, M.H.; Redmond, D.E., Jr. D1 and D2 dopamine receptors independently regulate spontaneous blink rate in the vervet monkey. J. Pharmacol. Exp. Ther. 1991, 259, 595–600. [Google Scholar] [PubMed]
- Caplan, R.; Caplan, R.; Guthrie, D.; Guthrie, D.; Komo, S.; Komo, S. Blink rate in children with attention-deficit-hyperactivity disorder. Biol. Psychiatry 1996, 39, 1032–1038. [Google Scholar] [CrossRef]
- Pivik, R.T.; Dykman, R.A. Endogenous eye blinks in preadolescents: Relationship to information processing and performance. Biol. Psychol. 2004, 66, 191–219. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, Y.; Yamaoka, K. Blink activity and task difficulty. Percept. Mot. Skills 1993, 77, 55–66. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, R.; Walrath, L.C.; Stern, J.A. Blink activity in a discrimination task as a function of stimulus modality and schedule of presentation. Psychophysiology 1985, 22, 629–635. [Google Scholar] [CrossRef] [PubMed]
- Ohira, H. Eyeblink activity in a word-naming task as a function of semantic priming and cognitive load. Percept. Mot. Skills 1996, 82, 835–842. [Google Scholar] [CrossRef] [PubMed]
- Siegle, G.J.; Ichikawa, N.; Steinhauer, S. Blink before and after you think: Blinks occur prior to and following cognitive load indexed by pupillary responses. Psychophysiology 2008, 45, 679–687. [Google Scholar] [CrossRef] [PubMed]
- Ichikawa, N.; Ohira, H. Eyeblink activity as an index of cognitive processing: Temporal distribution of eyeblinks as an indicator of expectancy in semantic priming. Percept. Motor Skills 2004, 98, 131–140. [Google Scholar] [CrossRef] [PubMed]
- Hester, R.; Garavan, H. Working memory and executive function: The influence of content and load on the control of attention. Mem. Cogn. 2005, 33, 221–233. [Google Scholar] [CrossRef]
- Van Bochove, M.E.; Van der Haegen, L.; Notebaert, W.; Verguts, T. Blinking predicts enhanced cognitive control. Cogn. Affect. Behav. Neurosci. 2013, 13, 346–354. [Google Scholar] [CrossRef] [PubMed]
- Zhang, T.; Mou, D.; Wang, C.; Tan, F.; Jiang, Y.; Lijun, Z.; Li, H. Dopamine and executive function: Increased spontaneous eye blink rates correlate with better set-shifting and inhibition, but poorer updating. Int. J. Psychophysiol. 2015, 96, 155–161. [Google Scholar] [CrossRef] [PubMed]
- Melara, R.D.; Algom, D. Driven by information: A tectonic theory of Stroop effects. Psychol. Rev. 2003, 110, 422–471. [Google Scholar] [CrossRef] [PubMed]
- Melara, R.D.; Rao, A.; Tong, Y. The duality of selection: Excitatory and inhibitory processes in auditory selective attention. J. Exp. Psychol. Hum. Percept. Perform. 2002, 28, 279–306. [Google Scholar] [CrossRef] [PubMed]
- Dickie, E.W.; Brunet, A.; Akerib, V.; Armony, J.L. Neural correlates of recovery from post-traumatic stress disorder: A longitudinal fMRI investigation of memory encoding. Neuropsychologia 2011, 49, 1771–1778. [Google Scholar] [CrossRef] [PubMed]
- Dickie, E.W.; Brunet, A.; Akerib, V.; Armony, J.L. An fMRI investigation of memory encoding in PTSD: Influence of symptom severity. Neuropsychologia 2008, 46, 1522–1531. [Google Scholar] [CrossRef] [PubMed]
- Mazza, M.; Tempesta, D.; Pino, M.C.; Catalucci, A.; Gallucci, M.; Ferrara, M. Regional cerebral changes and functional connectivity during the observation of negative emotional stimuli in subjects with post-traumatic stress disorder. Eur. Arch. Psychiatry Clin. Neurosci. 2013, 263, 575–583. [Google Scholar] [CrossRef] [PubMed]
- Garfinkel, S.N.; Garfinkel, S.N.; Liberzon, I.; Liberzon, I. Neurobiology of PTSD: A Review of Neuroimaging Findings. Psychiatr. Ann. 2009, 39, 370–381. [Google Scholar] [CrossRef]
- Koenigs, M.; Huey, E.D.; Raymont, V.; Cheon, B.; Solomon, J.; Wassermann, E.M.; Grafman, J. Focal brain damage protects against post-traumatic stress disorder in combat veterans. Nat. Neurosci. 2008, 11, 232–237. [Google Scholar] [CrossRef] [PubMed]
- Robinson, O.J.; Charney, D.R.; Overstreet, C.; Vytal, K.; Grillon, C. The adaptive threat bias in anxiety: Amygdala-dorsomedial prefrontal cortex coupling and aversive amplification. NeuroImage 2012, 60, 523–529. [Google Scholar] [CrossRef] [PubMed]
- Liberzon, I.; Sripada, C.S. The functional neuroanatomy of PTSD: A critical review. Prog. Brain Res. 2008, 167, 151–169. [Google Scholar] [PubMed]
- Melara, R.D.; Ruglass, L.; Fertuck, E.; Hien, D.A. Self-Regulation of Threat in Post-traumatic Stress Disorder: Associations between Inhibitory Control and Dissociative Symptomatology. BMC Public Health 2017. in preparation. [Google Scholar]
- Eriksen, B.A.; Eriksen, C.W. Effects of noise letters upon the identification of a target letter in a nonsearch task. Percept. Psychophys. 1974, 16, 143–149. [Google Scholar] [CrossRef]
- Blake, D.D.; Weathers, F.W.; Nagy, L.M.; Kaloupek, D.G.; Gusman, F.D.; Charney, D.S.; Keane, T.M. The development of a Clinician-Administered PTSD Scale. J. Traum. Stress 1995, 8, 75–90. [Google Scholar] [CrossRef]
- First, M.B.; Gibbon, M. The Structured Clinical Interview for DSM-IV Axis I Disorders (SCID-I) and the Structured Clinical Interview for DSM-IV Axis II Disorders (SCID-II); John Wiley & Sons Inc.: Hoboken, NJ, USA, 2004. [Google Scholar]
- Briere, J. Multiscale Dissociation Inventory (MDI); Psychological Assessment Resources: Odessa, FL, USA, 2002. [Google Scholar]
- Brown, L.; Sherbenou, R.J.; Johnsen, S.K. Test of Non-Verbal Intelligence (TONI-3), 3rd ed.; Pro-Ed: Austin, TX, USA, 1997. [Google Scholar]
- Beck, A.T.; Steer, R.A.; Brown, G.K. Manual for the Beck Depression Inventory-II; Psychological Corporation: San Antonio, TX, USA, 1996. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders DSM-IV-TR Fourth Edition (Text Revision), 4th ed.; American Psychiatric Association: Washington, DC, USA, 2000. [Google Scholar]
- Tottenham, N.; Tanaka, J.W.; Leon, A.C.; McCarry, T.; Nurse, M.; Hare, T.A.; Marcus, D.J.; Westerlund, A.; Casey, B.J.; Nelson, C. The NimStim set of facial expressions: Judgments from untrained research participants. Psychiatry Res. 2009, 168, 242–249. [Google Scholar] [CrossRef] [PubMed]
- Lang, P.J.; Bradley, M.M.; Cuthbert, B.N. International Affective Picture System (IAPS): Technical Manual and Affective Ratings. Available online: http://www2.unifesp.br/dpsicobio/Nova_versao_pagina_psicobio/adap/instructions.pdf (accessed on 25 January 2017).
- Garner, W.R. The Processing of Information and Structure; Erlbaum: Potomac, MD, USA, 1974. [Google Scholar]
- Yoder, N. PeakFinder. Available online: https://www.mathworks.com/matlabcentral/fileexchange/25500-peakfinder-x0--sel--thresh--extrema--includeendpoints--interpolate-?requestedDomain=www.mathworks.com (accessed on 25 January 2017).
- Barbato, G.; della Monica, C.; Costanzo, A.; De Padova, V. Dopamine activation in Neuroticism as measured by spontaneous eye blink rate. Physiol. Behav. 2012, 105, 332–336. [Google Scholar] [CrossRef] [PubMed]
- Shin, L.M.; Liberzon, I. The Neurocircuitry of Fear, Stress, and Anxiety Disorders. Neuropsychopharmacology 2010, 35, 169–191. [Google Scholar] [CrossRef] [PubMed]
- Badgaiyan, R.D.; Wack, D.; Wack, D. Evidence of Dopaminergic Processing of Executive Inhibition. PLoS ONE 2011, 6, e28075. [Google Scholar] [CrossRef] [PubMed]
- Cools, R.; D’Esposito, M. Inverted-U–Shaped Dopamine Actions on Human Working Memory and Cognitive Control. Biol. Psychiatry 2011, 69, e113–e125. [Google Scholar] [CrossRef] [PubMed]
- Hamner, M.B.; Diamond, B.I. Elevated plasma dopamine in posttraumatic stress disorder: A preliminary report. Biol. Psychiatry 1993, 33, 304–306. [Google Scholar] [CrossRef]
- Glover, D.A.; Powers, M.B.; Bergman, L.; Smits, J.A.J.; Telch, M.J.; Stuber, M. Urinary dopamine and turn bias in traumatized women with and without PTSD symptoms. Behav. Brain Res. 2003, 144, 137–141. [Google Scholar] [CrossRef]
- Thomaes, K.; Dorrepaal, E.; Draijer, N.; de Ruiter, M.B.; Elzinga, B.M.; van Balkom, A.J.; Smit, J.H.; Veltman, D.J. Treatment effects on insular and anterior cingulate cortex activation during classic and emotional Stroop interference in child abuse-related complex post-traumatic stress disorder. Psychol. Med. 2012, 42, 2337–2349. [Google Scholar] [CrossRef] [PubMed]
- Assadi, S.M.; Yücel, M.; Pantelis, C. Dopamine modulates neural networks involved in effort-based decision-making. Neurosci. Biobehav. Rev. 2009, 33, 383–393. [Google Scholar] [CrossRef] [PubMed]
- Cisler, J.M.; Wolitzky-Taylor, K.B.; Adams, T.G., Jr.; Babson, K.A.; Badour, C.L.; Willems, J.L. The emotional Stroop task and posttraumatic stress disorder: A meta-analysis. Clin. Psychol. Rev. 2011, 31, 817–828. [Google Scholar] [CrossRef] [PubMed]
- Mogg, K.; Bradley, B.; Miles, F.; Dixon, R. BRIEF REPORT Time course of attentional bias for threat scenes: Testing the vigilance-avoidance hypothesis. Cogn. Emot. 2004, 18, 689–700. [Google Scholar] [CrossRef]
- Lanius, R.A.; Frewen, P.A.; Vermetten, E.; Yehuda, R. Fear conditioning and early life vulnerabilities: Two distinct pathways of emotional dysregulation and brain dysfunction in PTSD. Eur. J. Psychotraumatol. 2010, 1, 585. [Google Scholar] [CrossRef] [PubMed]
- Grillon, C.; Morgan, C. Fear-Potentiated Startle Conditioning to Explicit and Contextual Cues in Gulf War Veterans With Posttraumatic Stress Disorder. J. Abnorm. Psychol. 1999, 108, 134–142. [Google Scholar] [CrossRef] [PubMed]
- Pole, N.; Neylan, T.C.; Best, S.R.; Orr, S.P.; Orr, S.P.; Marmar, C.R.; Marmar, C.R. Fear-potentiated startle and posttraumatic stress symptoms in urban police officers. J. Traum. Stress 2003, 16, 471–479. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| PTSD (n = 19) | TE (n = 16) | HC (n = 15) | Test Statistic | p | |
|---|---|---|---|---|---|
| Gender | |||||
| Male | 10 | 8 | 5 | χ2(2, N = 50) = 1.38 | 0.50 |
| Female | 9 | 8 | 10 | ||
| Age M (SD) | 35.3 (10.1) | 34.3 (12.0) | 33.4 (9.7) | F(2, 47) = 0.129 | 0.88 |
| Education (years) M (SD) | 14.7 (1.9) | 14.3 (1.8) | 14.1 (4.7) | F(2, 47) = 0.151 | 0.86 |
| Race/Ethnicity | |||||
| White | 3 | 3 | 3 | χ2(2, N = 50) = 2.61 | 0.27 |
| Black | 8 | 5 | 6 | ||
| Latino | 6 | 3 | 4 | ||
| Asian | 1 | 4 | 1 | ||
| Other | 1 | 1 | 1 | ||
| Trauma type (LEC) | |||||
| Physical Abuse/Assault | 16 | 11 | 3 | χ2(2, N = 50) = 5.93 | 0.00 |
| Sexual Trauma | 17 | 11 | 1 | ||
| Natural Disaster | 6 | 6 | 7 | ||
| War/Combat | 2 | 2 | 2 | ||
| Other | 36 | 44 | 24 | ||
| BDI | 11.3 (7.9) | 3.8 (5.4) | 0.47 (0.92) | F(2, 47) = 15.8 | 0.00 |
| Blink rate (mean) M (SD) | |||||
| Non-threat faces | 15.9 (8.5) | 20.8 (9.2) | 19.4 (15.4) | F(2, 47) = 0.898 | 0.41 |
| Threat faces | 15.2 (9.1) | 20.1 (8.5) | 19.6 (12.2) | F(2, 47) = 1.292 | 0.28 |
| Non-threat IAPS | 17.3 (9.4) | 19.4 (11.3) | 17.6 (11.1) | F(2, 47) = 0.200 | 0.82 |
| Threat IAPS | 16.3 (8.4) | 17.5 (12.2) | 17.3 (10.1) | F(2, 47) = 0.066 | 0.94 |
| Overall | 16.3 (8.4) | 19.2 (9.5) | 18.2 (11.3) | F(2, 47) = 0.408 | 0.67 |
| Flanker interference M (SD) | |||||
| Non-threat faces | 112.1 (100.0) | 133.1 (102.0) | 111.8 (89.8) | F(2, 47) = 0.923 | 0.41 |
| Threat faces | 98.7 (86.3) | 114.9 (110.4) | 119.2 (108.3) | F(2, 47) = 0.999 | 0.38 |
| Non-threat IAPS | 119.4 (97.3) | 142.5 (105.9) | 97.8 (63.9) | F(2, 47) = 0.200 | 0.82 |
| Threat IAPS | 94.0 (83.7) | 140.2 (129.7) | 109.2 (69.2) | F(2, 47) = 0.254 | 0.78 |
| Overall | 106.0 (84.2) | 132.7 (104.0) | 109.4 (78.2) | F(2, 47) = 0.436 | 0.65 |
| Interference Condition | PTSD Blink Rate (n = 19) | TE Blink Rate (n = 16) | HC Blink Rate (n = 15) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| NF | TF | NI | TI | NF | TF | NI | TI | NF | TF | NI | TI | |
| Non-threat Faces | 0.363 | −0.225 | −0.295 | |||||||||
| Threat Faces | 0.284 | −0.201 | −0.196 | |||||||||
| Non-threat IAPS | 0.415 † | −0.219 | −0.158 | |||||||||
| Threat IAPS | 0.510 * | −0.201 | −0.286 | |||||||||
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rubin, M.; Hien, D.A.; Das, D.; Melara, R.D. Inhibitory Control under Threat: The Role of Spontaneous Eye Blinks in Post-Traumatic Stress Disorder. Brain Sci. 2017, 7, 16. https://doi.org/10.3390/brainsci7020016
Rubin M, Hien DA, Das D, Melara RD. Inhibitory Control under Threat: The Role of Spontaneous Eye Blinks in Post-Traumatic Stress Disorder. Brain Sciences. 2017; 7(2):16. https://doi.org/10.3390/brainsci7020016
Chicago/Turabian StyleRubin, Mikael, Denise A. Hien, Dipanjana Das, and Robert D. Melara. 2017. "Inhibitory Control under Threat: The Role of Spontaneous Eye Blinks in Post-Traumatic Stress Disorder" Brain Sciences 7, no. 2: 16. https://doi.org/10.3390/brainsci7020016
APA StyleRubin, M., Hien, D. A., Das, D., & Melara, R. D. (2017). Inhibitory Control under Threat: The Role of Spontaneous Eye Blinks in Post-Traumatic Stress Disorder. Brain Sciences, 7(2), 16. https://doi.org/10.3390/brainsci7020016