Recurrent Hemorrhagic Conversion of Ischemic Stroke in a Patient with Mechanical Heart Valve: A Case Report and Literature Review


{kind=link}
{kind=link}
Abstract
:1. Introduction
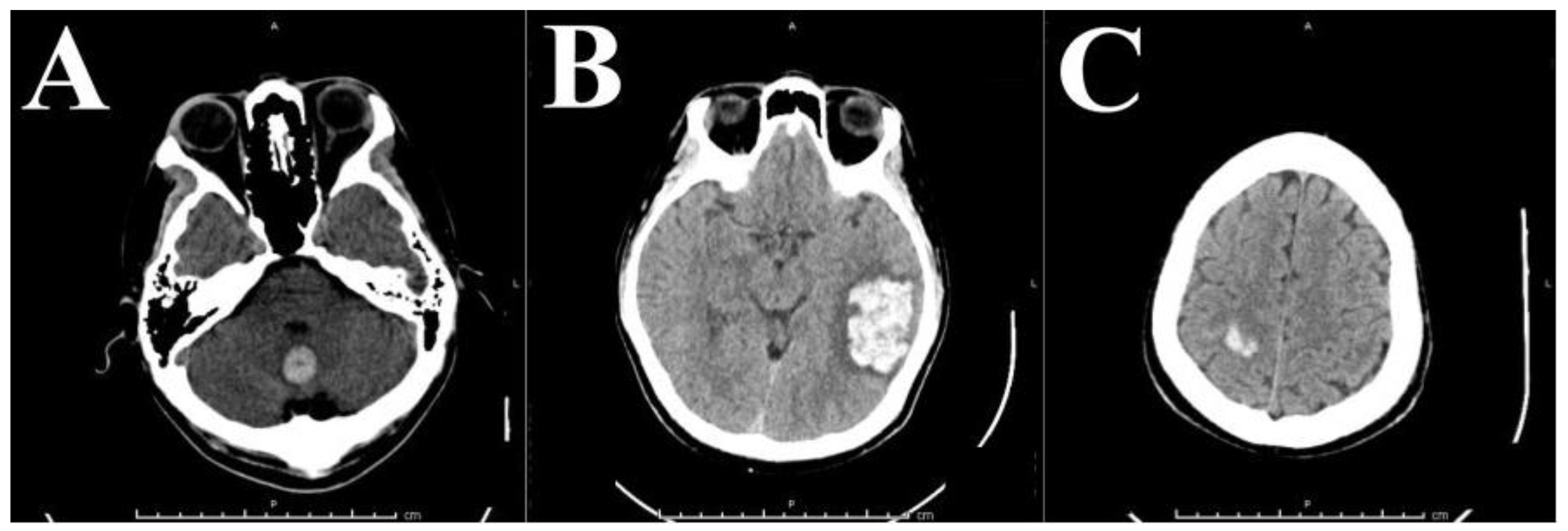
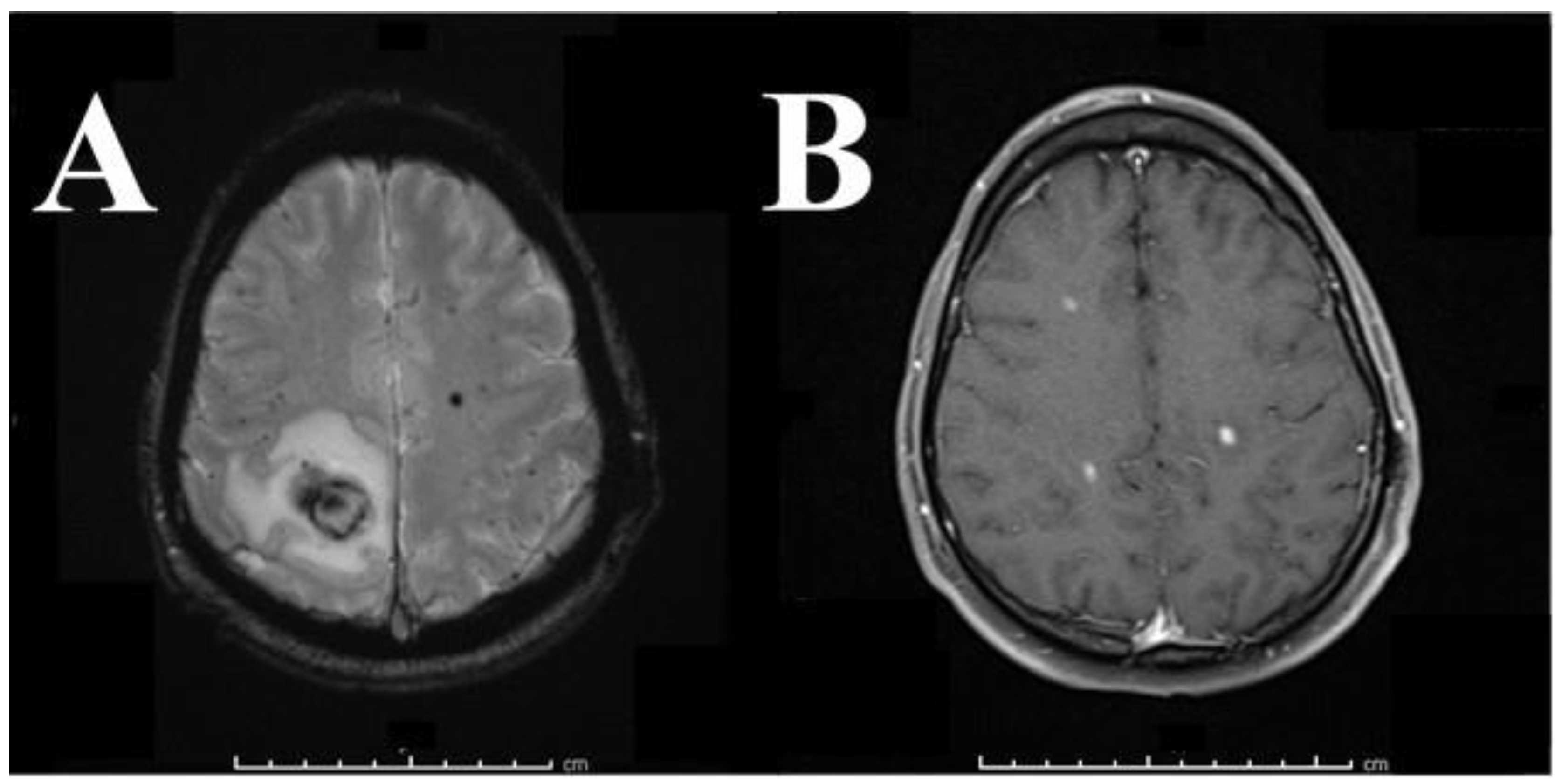
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Conflicts of Interest
Abbreviations
References
- Centers for Disease Control and Prevention, National Center for Health Statistics. Compressed Mortality File 1999–2009. CDC Wonder Online Database, Compiled for Compressed Mortality File 1999–2009 Series 20, No. 20, 2012. Underlying Cause-of-Death 1999–2009. Available online: http://Wonder.Cdc.Gov/Mortsql.Html (accessed on 22 October 2017).
- Centers for Disease Control and Prevention (CDC). Prevalence and most common causes of disability among adults—United States, 2005. Morb. Mortal. Wkly. Rep. 2009, 58, 421–426. [Google Scholar]
- Go, A.S.; Mozaffarian, D.; Roger, V.L.; Benjamin, E.J.; Berry, J.D.; Blaha, M.J.; Dai, S.; Ford, E.S.; Fox, C.S.; Franco, S.; et al. Heart disease and stroke statistics—2014 update: A report from the American Heart Association. Circulation 2014, 129, e28–e292. [Google Scholar] [CrossRef] [PubMed]
- Products—Data Briefs—Number 178—December 2014. Available online: https://www.cdc.gov/nchs/products/databriefs/db178.htm (accessed on 22 October 2017).
- Leiria, T.L.L.; Lopes, R.D.; Williams, J.B.; Katz, J.N.; Kalil, R.A.K.; Alexander, J.H. Antithrombotic therapies in patients with prosthetic heart valves: Guidelines translated for the clinician. J. Thromb. Thrombolysis 2011, 31, 514–522. [Google Scholar] [CrossRef] [PubMed]
- Dasi, L.P.; Simon, H.A.; Sucosky, P.; Yoganathan, A.P. Fluid Mechanics of Artificial Heart Valves. Clin. Exp. Pharmacol. Physiol. 2009, 36, 225–237. [Google Scholar] [CrossRef] [PubMed]
- Birkmeyer, N.J.; Birkmeyer, J.D.; Tosteson, A.N.; Grunkemeier, G.L.; Marrin, C.A.; O’Connor, G.T. Prosthetic valve type for patients undergoing aortic valve replacement: A decision analysis. Ann. Thorac. Surg. 2000, 70, 1946–1952. [Google Scholar] [CrossRef]
- Schulman, S.; Beyth, R.J.; Kearon, C.; Levine, M.N. Hemorrhagic complications of anticoagulant and thrombolytic treatment: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest 2008, 133, 257S–298S. [Google Scholar] [CrossRef] [PubMed]
- Flaherty, M.L.; Kissela, B.; Woo, D.; Kleindorfer, D.; Alwell, K.; Sekar, P.; Moomaw, C.J.; Haverbusch, M.; Broderick, J.P. The increasing incidence of anticoagulant-associated intracerebral hemorrhage. Neurology 2007, 68, 116–121. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, J.N.; Greenberg, S.M. Should anticoagulation be resumed after intracerebral hemorrhage? Clevel. Clin. J. Med. 2010, 77, 791–799. [Google Scholar] [CrossRef] [PubMed]
- Simard, J.M.; Kent, T.A.; Chen, M.; Tarasov, K.V.; Gerzanich, V. Brain oedema in focal ischaemia: Molecular pathophysiology and theoretical implications. Lancet Neurol. 2007, 6, 258–268. [Google Scholar] [CrossRef]
- AlKherayf, F.; Xu, Y.; Westwick, H.; Moldovan, I.D.; Wells, P.S. Timing of anticoagulant re-initiation following intracerebral hemorrhage in mechanical heart valves: Survey of neurosurgeons and thrombosis experts. Clin. Neurol. Neurosurg. 2017, 154, 23–27. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Yang, Y.; Sun, H.; Xing, Y. Hemorrhagic transformation after cerebral infarction: Current concepts and challenges. Ann. Transl. Med. 2014, 2. [Google Scholar] [CrossRef]
- Rossi, D.J.; Brady, J.D.; Mohr, C. Astrocyte metabolism and signaling during brain ischemia. Nat. Neurosci. 2007, 10, 1377–1386. [Google Scholar] [CrossRef] [PubMed]
- Warach, S.; Latour, L.L. Evidence of reperfusion injury, exacerbated by thrombolytic therapy, in human focal brain ischemia using a novel imaging marker of early blood-brain barrier disruption. Stroke 2004, 35, 2659–2661. [Google Scholar] [CrossRef] [PubMed]
- Heo, J.H.; Lucero, J.; Abumiya, T.; Koziol, J.A.; Copeland, B.R.; del Zoppo, G.J. Matrix metalloproteinases increase very early during experimental focal cerebral ischemia. J. Cereb. Blood Flow Metab. 1999, 19, 624–633. [Google Scholar] [CrossRef] [PubMed]
- Sumii, T.; Lo, E.H. Involvement of matrix metalloproteinase in thrombolysis-associated hemorrhagic transformation after embolic focal ischemia in rats. Stroke 2002, 33, 831–836. [Google Scholar] [CrossRef] [PubMed]
- Lu, A.; Suofu, Y.; Guan, F.; Broderick, J.P.; Wagner, K.R.; Clark, J.F. Matrix metalloproteinase-2 deletions protect against hemorrhagic transformation after 1 h of cerebral ischemia and 23 h of reperfusion. Neuroscience 2013, 253, 361–367. [Google Scholar] [CrossRef] [PubMed]
- Paciaroni, M.; Agnelli, G.; Corea, F.; Ageno, W.; Alberti, A.; Lanari, A.; Caso, V.; Micheli, S.; Bertolani, L.; Venti, M.; et al. Early hemorrhagic transformation of brain infarction: Rate, predictive factors, and influence on clinical outcome: Results of a prospective multicenter study. Stroke 2008, 39, 2249–2256. [Google Scholar] [CrossRef] [PubMed]
- Lazio, B.E.; Simard, J.M. Anticoagulation in neurosurgical patients. Neurosurgery 1999, 45, 838–847. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Zhang, Z.; Sun, W.; Koehler, R.C.; Huang, J. 17β-estradiol attenuates breakdown of blood-brain barrier and hemorrhagic transformation induced by tissue plasminogen activator in cerebral ischemia. Neurobiol. Dis. 2011, 44, 277–283. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Tsuji, K.; Lee, S.-R.; Ning, M.; Furie, K.L.; Buchan, A.M.; Lo, E.H. Mechanisms of hemorrhagic transformation after tissue plasminogen activator reperfusion therapy for ischemic stroke. Stroke 2004, 35, 2726–2730. [Google Scholar] [CrossRef] [PubMed]
- Ishiguro, M.; Mishiro, K.; Fujiwara, Y.; Chen, H.; Izuta, H.; Tsuruma, K.; Shimazawa, M.; Yoshimura, S.; Satoh, M.; Iwama, T.; et al. Phosphodiesterase-III Inhibitor Prevents Hemorrhagic Transformation Induced by Focal Cerebral Ischemia in Mice Treated with tPA. PLoS ONE 2010, 5, e15178. [Google Scholar] [CrossRef] [PubMed]
- Trouillas, P.; von Kummer, R. Classification and pathogenesis of cerebral hemorrhages after thrombolysis in ischemic stroke. Stroke 2006, 37, 556–561. [Google Scholar] [CrossRef] [PubMed]
- Dorado, L.; Millán, M.; de la Ossa, N.P.; Guerrero, C.; Gomis, M.; López-Cancio, E.; Ricciardi, A.C.; Dávalos, A. Influence of antiplatelet pre-treatment on the risk of intracranial haemorrhage in acute ischaemic stroke after intravenous thrombolysis. Eur. J. Neurol. 2010, 17, 301–306. [Google Scholar] [CrossRef] [PubMed]
- Pfeilschifter, W.; Spitzer, D.; Czech-Zechmeister, B.; Steinmetz, H.; Foerch, C. Increased Risk of Hemorrhagic Transformation in Ischemic Stroke Occurring During Warfarin Anticoagulation: An Experimental Study in Mice. Stroke 2011, 42, 1116–1121. [Google Scholar] [CrossRef] [PubMed]
- Adams, H.P. Emergent Use of Anticoagulation for Treatment of Patients with Ischemic Stroke. Stroke 2002, 33, 856–861. [Google Scholar] [CrossRef] [PubMed]
- Marsh, E.B.; Llinas, R.H.; Hillis, A.E.; Gottesman, R.F. Hemorrhagic transformation in patients with acute ischaemic stroke and an indication for anticoagulation. Eur. J. Neurol. 2013, 20, 962–967. [Google Scholar] [CrossRef] [PubMed]
- Labaf, A.; Grzymala-Lubanski, B.; Stagmo, M.; Lövdahl, S.; Wieloch, M.; Själander, A.; Svensson, P.J. Thromboembolism, major bleeding and mortality in patients with mechanical heart valves—A population-based cohort study. Thromb. Res. 2014, 134, 354–359. [Google Scholar] [CrossRef] [PubMed]
- Bourguignon, T.; Bergöend, E.; Mirza, A.; Ayegnon, G.; Neville, P.; Aupart, M.R.; Marchand, M. Risk factors for valve-related complications after mechanical heart valve replacement in 505 patients with long-term follow up. J. Heart Valve Dis. 2011, 20, 673–680. [Google Scholar] [PubMed]
- Misawa, Y. Valve-related complications after mechanical heart valve implantation. Surg. Today 2015, 45, 1205–1209. [Google Scholar] [CrossRef] [PubMed]
- Wijdicks, E.F.; Schievink, W.I.; Brown, R.D.; Mullany, C.J. The dilemma of discontinuation of anticoagulation therapy for patients with intracranial hemorrhage and mechanical heart valves. Neurosurgery 1998, 42, 769–773. [Google Scholar] [CrossRef] [PubMed]
- Hammermeister, K.E.; Sethi, G.K.; Henderson, W.G.; Oprian, C.; Kim, T.; Rahimtoola, S. A Comparison of Outcomes in Men 11 Years after Heart-Valve Replacement with a Mechanical Valve or Bioprosthesis. N. Engl. J. Med. 1993, 328, 1289–1296. [Google Scholar] [CrossRef] [PubMed]
- Puvimanasinghe, J.P.; Steyerberg, E.W.; Takkenberg, J.J.; Eijkemans, M.J.; van Herwerden, L.A.; Bogers, A.J.; Habbema, J.D. Prognosis after aortic valve replacement with a bioprosthesis: Predictions based on meta-analysis and microsimulation. Circulation 2001, 103, 1535–1541. [Google Scholar] [CrossRef] [PubMed]
- Hammermeister, K.; Sethi, G.K.; Henderson, W.G.; Grover, F.L.; Oprian, C.; Rahimtoola, S.H. Outcomes 15 years after valve replacement with a mechanical versus a bioprosthetic valve: Final report of the Veterans Affairs randomized trial. J. Am. Coll. Cardiol. 2000, 36, 1152–1158. [Google Scholar] [CrossRef]
- Oxenham, H.; Bloomfield, P.; Wheatley, D.J.; Lee, R.J.; Cunningham, J.; Prescott, R.J.; Miller, H.C. Twenty year comparison of a Bjork-Shiley mechanical heart valve with porcine bioprostheses. Heart 2003, 89, 715–721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rahimtoola, S.H. Choice of prosthetic heart valve for adult patients. J. Am. Coll. Cardiol. 2003, 41, 893–904. [Google Scholar] [CrossRef]
- Cannegieter, S.C.; Rosendaal, F.R.; Briët, E. Thromboembolic and bleeding complications in patients with mechanical heart valve prostheses. Circulation 1994, 89, 635–641. [Google Scholar] [CrossRef] [PubMed]
- Ruel, M.; Masters, R.G.; Rubens, F.D.; Bédard, P.J.; Pipe, A.L.; Goldstein, W.G.; Hendry, P.J.; Mesana, T.G. Late incidence and determinants of stroke after aortic and mitral valve replacement. Ann. Thorac. Surg. 2004, 78, 77–83. [Google Scholar] [CrossRef] [PubMed]
- Robinson, A.A.; Ikuta, K.; Soverow, J. Anticoagulation for the Acute Management of Ischemic Stroke. Yale J. Biol. Med. 2014, 87, 199–206. [Google Scholar] [PubMed]
- Vongpatanasin, W.; Hillis, L.D.; Lange, R.A. Prosthetic heart valves. N. Engl. J. Med. 1996, 335, 407–416. [Google Scholar] [CrossRef] [PubMed]
- Yacoub, M.; Rasmi, N.R.; Sundt, T.M.; Lund, O.; Boyland, E.; Radley-Smith, R.; Khaghani, A.; Mitchell, A. Fourteen-year experience with homovital homografts for aortic valve replacement. J. Thorac. Cardiovasc. Surg. 1995, 110, 186–193. [Google Scholar] [CrossRef]
- O’Brien, M.F.; Stafford, E.G.; Gardner, M.A.; Pohlner, P.G.; Tesar, P.J.; Cochrane, A.D.; Mau, T.K.; Gall, K.L.; Smith, S.E. Allograft aortic valve replacement: Long-term follow-up. Ann. Thorac. Surg. 1995, 60, S65–S70. [Google Scholar] [CrossRef]
- Vandvik, P.O.; Lincoff, A.M.; Gore, J.M.; Gutterman, D.D.; Sonnenberg, F.A.; Alonso-Coello, P.; Akl, E.A.; Lansberg, M.G.; Guyatt, G.H.; Spencer, F.A. Primary and secondary prevention of cardiovascular disease: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 2012, 141, e637S–e668S. [Google Scholar] [CrossRef] [PubMed]


© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tarver, M.J.; Schmidt, T.; Koltz, M.T. Recurrent Hemorrhagic Conversion of Ischemic Stroke in a Patient with Mechanical Heart Valve: A Case Report and Literature Review. Brain Sci. 2018, 8, 12. https://doi.org/10.3390/brainsci8010012
Tarver MJ, Schmidt T, Koltz MT. Recurrent Hemorrhagic Conversion of Ischemic Stroke in a Patient with Mechanical Heart Valve: A Case Report and Literature Review. Brain Sciences. 2018; 8(1):12. https://doi.org/10.3390/brainsci8010012
Chicago/Turabian StyleTarver, Micheal Jace, Tyler Schmidt, and Michael T. Koltz. 2018. "Recurrent Hemorrhagic Conversion of Ischemic Stroke in a Patient with Mechanical Heart Valve: A Case Report and Literature Review" Brain Sciences 8, no. 1: 12. https://doi.org/10.3390/brainsci8010012
APA StyleTarver, M. J., Schmidt, T., & Koltz, M. T. (2018). Recurrent Hemorrhagic Conversion of Ischemic Stroke in a Patient with Mechanical Heart Valve: A Case Report and Literature Review. Brain Sciences, 8(1), 12. https://doi.org/10.3390/brainsci8010012