Optimising Outcomes for Glioblastoma through Subspecialisation in a Regional Cancer Centre

Abstract
:1. Introduction
2. Methods
2.1. Neurosurgical Management
2.2. Neuropathological Features
2.3. Radiation Therapy
2.4. Systemic Therapy
2.5. Model of Care for Adjuvant Therapy
2.6. Follow-Up
2.7. Clinical Quality Indicators
2.8. Statistical Considerations
3. Results
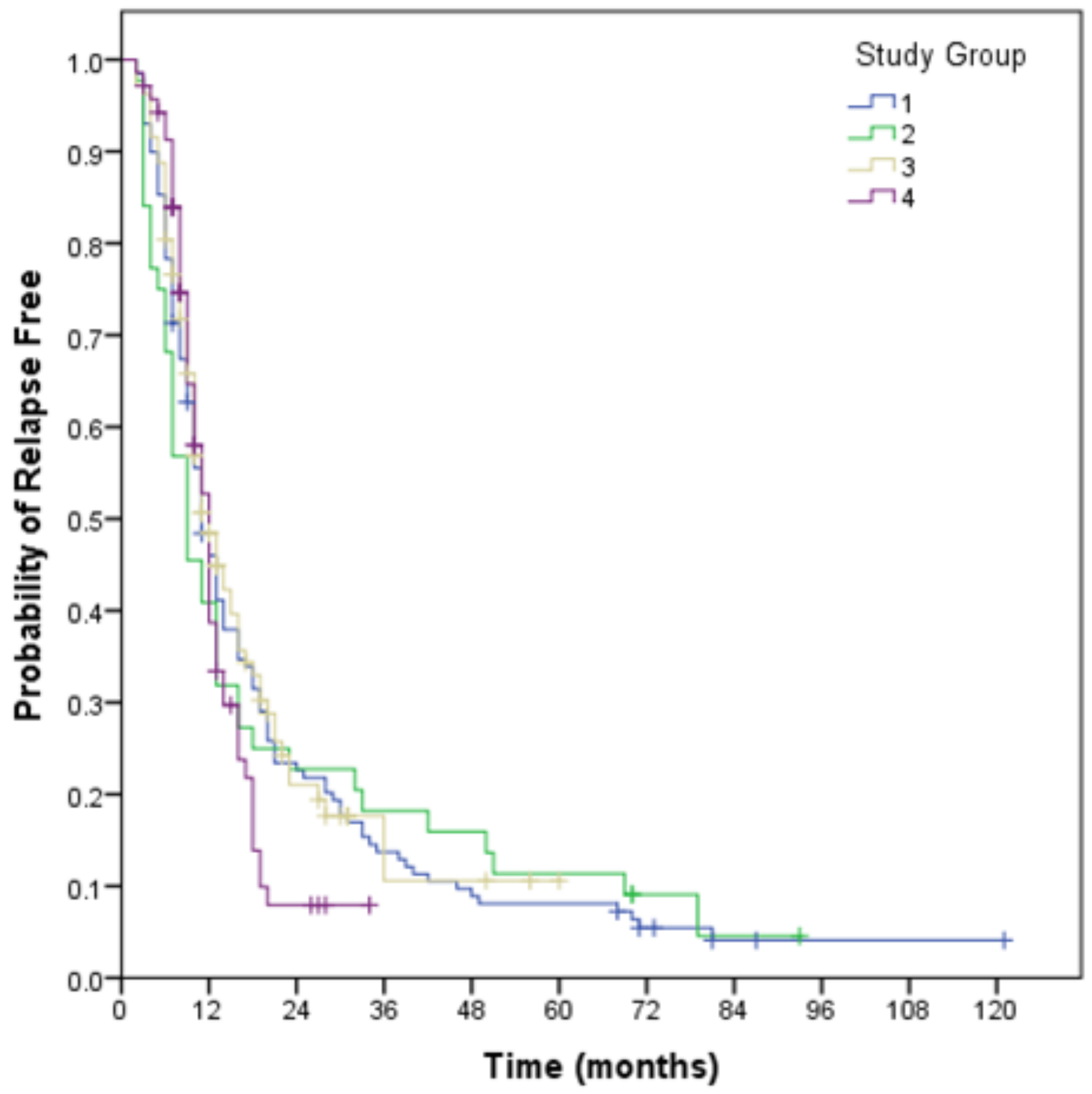
3.1. Relapse Free Survival
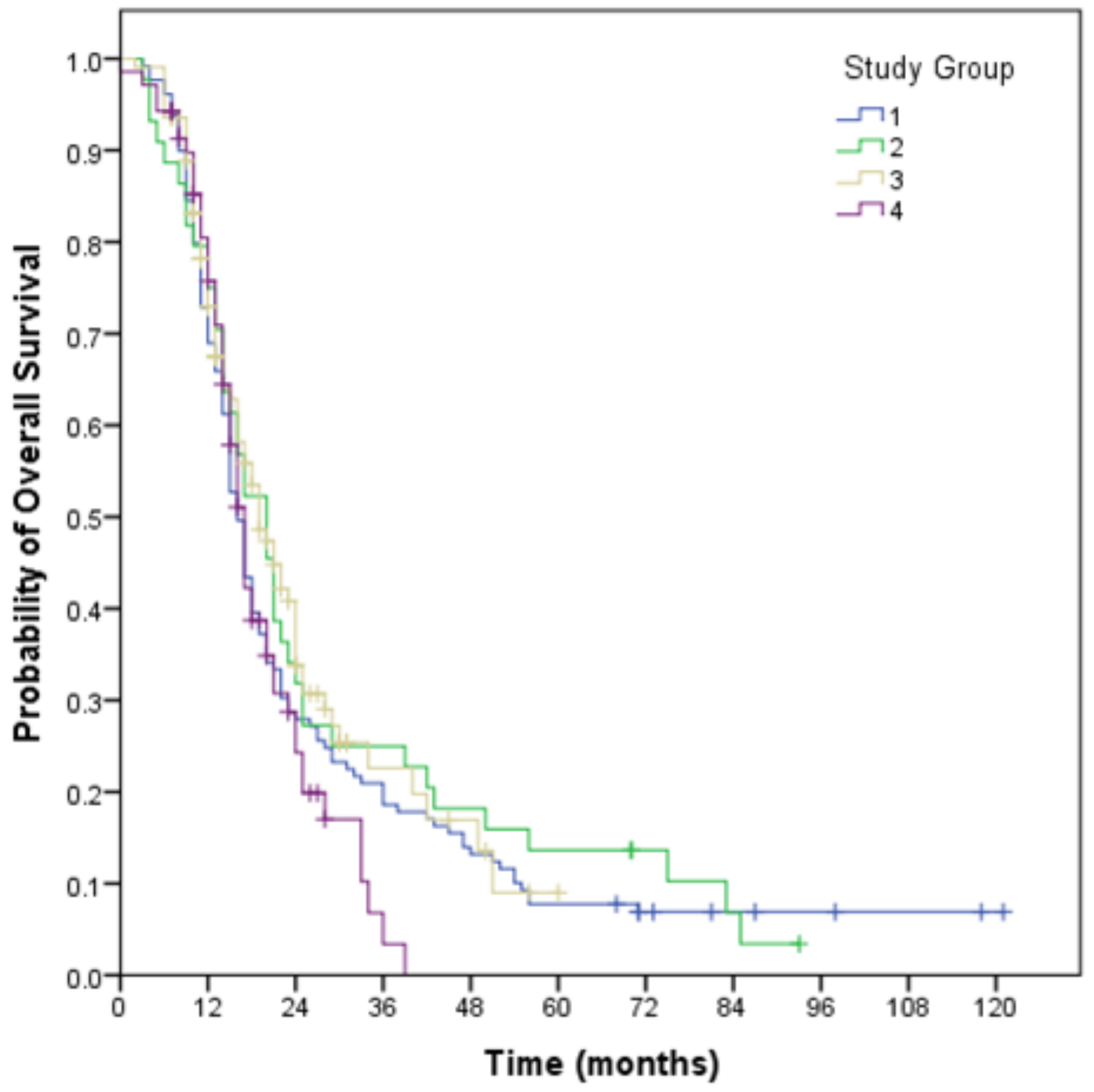
3.2. Overall Survival
3.3. Salvage Therapy
3.4. Analysis of Geographical Location Groups
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Stupp, R.; Mason, W.P.; van den Bent, M.J.; Weller, M.; Fisher, B.; Taphoorn, M.J.B.; Belanger, K.; Brandes, A.A.; Marosi, C.; Bogdahn, U.; et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N. Engl. J. Med. 2005, 352, 987–996. [Google Scholar] [CrossRef] [PubMed]
- Stupp, R.; Heqi, M.E.; Mason, W.P.; van den Bent, M.J.; Taphoorn, M.J.; Janzer, R.C.; Ludwin, S.K.; Allgeier, A.; Fisher, B.; Belanger, K.; et al. Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol. 2009, 10, 459–466. [Google Scholar] [CrossRef]
- Jayamanne, D.; Wheeler, H.; Cook, R.; Teo, C.; Brazier, D.; Schembri, G.; Kastelan, M.; Guo, L.; Back, M.F. Survival improvements with adjuvant therapy in patients with glioblastoma. ANZ J. Surg. 2018, 88, 196–201. [Google Scholar] [CrossRef] [PubMed]
- Johnson, D.R.; Leeper, H.E.; Uhm, J.H. Glioblastoma survival in the United States improved after Food and Drug Administration approval of bevacizumab: A population-based analysis. Cancer 2013, 119, 3489–3495. [Google Scholar] [CrossRef] [PubMed]
- Louis, D.N.; Ohgaki, H.; Wiestler, O.D.; Cavenee, W.K.; Burger, P.C.; Jouvet, A.; Scheithauer, B.W.; Kleihues, P. The 2007 WHO classification of tumours of the central nervous system. Acta Neuropathol. 2007, 114, 97–109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Back, M.; Rodriguez, M.; Jayamanne, D.; Khasraw, M.; Lee, A.; Wheeler, H. Understanding the Revised Fourth Edition of the World Health Organization Classification of Tumours of the Central Nervous System (2016) for Clinical Decision-making: A Guide for Oncologists Managing Patients with Glioma. Clin. Oncol. 2018, 30, 556–562. [Google Scholar] [CrossRef] [PubMed]
- Stupp, R.; Hegi, M.E.; Gorlia, T.; Erridge, S.C.; Perry, J.; Hong, Y.K.; Aldape, K.D.; Lhermitte, B.; Pietsch, T.; Grujicic, D.; et al. Cilengitide combined with standard treatment for patients with newly diagnosed glioblastoma with methy-lated MGMT promoter (CENTRIC EORTC 26071-22072 study): A multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. 2014, 15, 1100–1108. [Google Scholar] [CrossRef]
- Chinot, O.L.; Wick, W.; Mason, W.; Henriksson, R.; Saran, F.; Nishikawa, R.; Carpentier, A.F.; Hoang-Xuan, K.; Kavan, P.; Cernea, D.; et al. Bevacizumab plus radiotherapy-temozolomide for newly diagnosed glioblastoma. N. Engl. J. Med. 2014, 370, 709–722. [Google Scholar] [CrossRef] [PubMed]
- Khasraw, M.; Lee, A.; McCowatt, S.; Kerestes, Z.; Buyse, M.E.; Back, M.; Kichenadasse, G.; Ackland, S.; Wheeler, H. Cilengitide with metronomic temozolomide, procarbazine, and standard radiotherapy in patients with glioblastoma and unmethylated MGMT gene promoter in ExCentric, an open-label phase II trial. J. Neurooncol. 2016, 128, 163–171. [Google Scholar] [CrossRef] [PubMed]
- Weller, M.; Butowski, N.; Tran, D.D.; Recht, L.D.; Lim, M.; Hirte, H.; Ashby, L.; Mechtler, L.; Goldlust, S.A.; Iwamoto, F.; et al. Rindopepimut with temozolomide for patients with newly diagnosed, EGFRvIII-expressing glioblastoma (ACT IV): A randomised, double-blind, international phase 3 trial. Lancet Oncol. 2017, 18, 1373–1385. [Google Scholar] [CrossRef]
- Jue, T.R.; Nozue, K.; Lester, A.J.; Joshi, S.; Schroder, L.B.; Whittaker, S.P.; Nixdorf, S.; Rapkins, R.W.; Khasraw, M.; McDonald, K.L. Veliparib in combination with radiotherapy for the treatment of MGMT unmethylated glioblastoma. J. Transl. Med. 2017, 15, 61. [Google Scholar] [CrossRef] [PubMed]
- Reardon, D.A.; Lassman, A.B.; van den Bent, M.; Kumthekar, P.; Merrell, R.; Scott, A.M.; Fichtel, L.; Sulman, E.P.; Gomez, E.; Fischer, J.; et al. Efficacy and safety results of ABT-414 in combination with radiation and temozolomide in newly diagnosed glioblastoma. Neuro. Oncol. 2017, 19, 965–975. [Google Scholar] [CrossRef] [PubMed]
- Omuro, A.; Vlahovic, G.; Lim, M.; Sahebjam, S.; Baehring, J.; Cloughesy, T.; Voloschin, A.; Ramkissoon, S.H.; Ligon, K.L.; Latek, R.; et al. Nivolumab with or without ipilimumab in patients with recurrent glioblastoma: Results from exploratory phase I cohorts of CheckMate 143. Neuro. Oncol. 2018, 20, 674–686. [Google Scholar] [CrossRef] [PubMed]
- Australian Bureau of Statistics. Available online: http://quickstats.censusdata.abs.gov.au/census_services/getproduct/census/2016/quickstat/LGA11650?opendocument (accessed on 10 September 2018).
- Morgan, G.W.; Barton, M.; Atkinson, C.; Millar, J.; Kumar Gogna, N.; Yeoh, E. ‘GAP’ in radiotherapy services in Australia and New Zealand in 2009. J. Med. Imaging Radiat. Oncol. 2010, 54, 287–297. [Google Scholar] [CrossRef] [PubMed]
- Australian Institute of Health and Welfare. 2017. Available online: http://www.aihw.gov.au/acim-books/ (accessed on 3 February 2018).
- Birkmeyer, J.D.; Siewers, A.E.; Finlayson, E.V.; Stukel, T.A.; Lucas, F.L.; Batista, I.; Welch, H.G.; Wennberg, D.E. Hospital volume and surgical mortality in the United States. N. Engl. J. Med. 2002, 346, 1128–1137. [Google Scholar] [CrossRef] [PubMed]
- Archampong, D.; Borowski, D.; Wille-Jørgensen, P.; Iversen, L.H. Workload and surgeon’s specialty for outcome after colorectal cancer surgery. Cochrane Database Syst. Rev. 2012, 6, CD005. [Google Scholar]
- Merrill, A.L.; Jha, A.K.; Dimick, J.B. Clinical Effect of Surgical Volume. N. Engl. J. Med. 2016, 374, 1380–1382. [Google Scholar] [CrossRef] [PubMed]
- Hölscher, A.H.; Metzger, R.; Brabender, J.; Vallböhmer, D.; Bollschweiler, E. High-volume centers—Effect of case load on outcome in cancer surgery. Onkologie 2004, 27, 412–416. [Google Scholar] [CrossRef] [PubMed]
- Boero, I.J.; Paravati, A.J.; Xu, B.; Cohen, E.E.; Mell, L.K.; Le, Q.T.; Murphy, J.D. Importance of Radiation Oncologist Experience Among Patients with Head-and-Neck Cancer Treated with Intensity-Modulated Radiation Therapy. J. Clin. Oncol. 2016, 34, 684–690. [Google Scholar] [CrossRef] [PubMed]
- Wuthrick, E.; Zhang, Q.; Machtay, M.; Rosenthal, D.I.; Nguyen-Tan, P.F.; Fortin, A.; Silverman, C.L.; Raben, A.; Kim, H.E.; Horwitz, E.M.; et al. Institutional Clinical Trial Accrual Volume and Survival of Patients with Head and Neck Cancer. J. Clin. Oncol. 2015, 33, 156–164. [Google Scholar] [CrossRef] [PubMed]
- Eaton, B.R.; Pugh, S.L.; Bradley, J.D.; Masters, G.; Kavadi, V.S.; Narayan, S.; Nedzi, L.; Robinson, C.; Wynn, R.B.; Koprowski, C.; et al. Institutional Enrollment and Survival Among NSCLC Patients Receiving Chemoradiation: NRG Oncology Radiation Therapy Oncology Group (RTOG) 0617. J. Natl. Cancer Inst. 2016, 108, djw034. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Subgroup | Number (352) | |
|---|---|---|
| Age at Diagnosis | <50 years >50 years Median | 86 (24%) 266 (76%) 43 years |
| Year of Diagnosis | 2008–2010 2011–2014 2015–2018 | 109 (31%) 125 (36%) 118 (33%) |
| Tumour Site | Temporal Frontal Parietal Occipital Thalamic Other | 110 (31%) 101 (29%) 89 (25%) 26 (7%) 20 (6%) 6 (2%) |
| Extent of Resection | Near-Total Subtotal Biopsy | 156 (44%) 142 (40%) 54 (16%) |
| Ki67% | <20 20–30 31–50 >50 Unknown | 48 (14%) 122 (35%) 93 (26%) 49 (14%) 40 (11%) |
| Isocitrate Dehydrogenase (IDH) Mutation | Wildtype Mutation Unknown | 244 (69%) 17 (5%) 91 (26%) |
| O-6 methylguanine DNA methyltransferase (MGMT) Methylation | No Yes Unknown | 97 (28%) 79 (22%) 176 (50%) |
| Eastern Cooperative Oncology Group (ECOG) PreRT | 0 1 2 3, 4 | 104 (29%) 146 (41%) 75 (21%) 27 (8%) |
| Subgroup | All Patients 2008–2018 (352) | Group 1 Metro 2008–2013 (129) | Group 2 Regional 2008–2013 (44) | Group 3 Metro 2013–2018 (109) | Group 4 Regional 2013–2018 (70) | |
|---|---|---|---|---|---|---|
| Age <50 years | Median (months) 95% CI | 24 months (19.3–28.7) | 23 (13.9–32.1) | NA | 24 (20.5–27.5) | 16 (12.8–19.2) |
| Extent of Resection (Near Total) | Median (months) 95% CI | 21 months (18.6–23.4) | 19 (15.3–22.7) | 22 (18.5–25.5) | 21 (15.6–26.4) | 20 (15.4–26.4) |
| Performance Status (ECOG 0, 1) | Median (months) 95% CI | 20 months (18.0–22.0) | 17 (14.7–19.3) | 21 (17.1–24.9) | 23 (20.2–25.8) | 18 (15.1–20.9) |
| MGMT (Methylated) | Median (months) 95% CI | 28 months (17.6–38.4) | 36 (10.2–61.8) | NA | 28 (19.8–36.2) | 20 (13.3–20.0) |
| Outcome | All Patients 2008–2018 (352) | Group 1 Metro 2008–2013 (129) | Group 2 Regional 2008–2013 (44) | Group 3 Metro 2013–2018 (109) | Group 4 Regional 2013–2018 (70) | |
|---|---|---|---|---|---|---|
| Overall Survival | Median (months) 95% CI | 17 (15.5–18.5) | 16 (14.5–17.5) | 20 (16.0–24.0) | 19 (15.3–22.7) | 17 (15.4–18.6) |
| Relapse Free Survival | Median (months) 95% CI | 11 (10.0–12.0) | 11 (9.2–12.8) | 9 (5.3–12.7) | 12 (9.6–14.4) | 12 (10.7–13.3) |
| Clinical Trial Accrual | % involved | 22% | 29% | 18% | 17% | 18% |
| Repeat Craniotomy at Salvage | % use | 35% | 30% | 32% | 43% | 31% |
| Bevacizumab Use at Salvage | % use post 2011 | 73% | 65% | 48% | 58% | 73% |
| Re-irradiation at Salvage | % use post 2011 | 21% | 16% | 14% | 20% | 24% |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Back, M.; Jayamanne, D.; Cove, N.; Wheeler, H.; Khasraw, M.; Guo, L.; Back, J.; Wong, M. Optimising Outcomes for Glioblastoma through Subspecialisation in a Regional Cancer Centre. Brain Sci. 2018, 8, 186. https://doi.org/10.3390/brainsci8100186
Back M, Jayamanne D, Cove N, Wheeler H, Khasraw M, Guo L, Back J, Wong M. Optimising Outcomes for Glioblastoma through Subspecialisation in a Regional Cancer Centre. Brain Sciences. 2018; 8(10):186. https://doi.org/10.3390/brainsci8100186
Chicago/Turabian StyleBack, Michael, Dasantha Jayamanne, Nicola Cove, Helen Wheeler, Mustafa Khasraw, Linxin Guo, Jemimah Back, and Matthew Wong. 2018. "Optimising Outcomes for Glioblastoma through Subspecialisation in a Regional Cancer Centre" Brain Sciences 8, no. 10: 186. https://doi.org/10.3390/brainsci8100186
APA StyleBack, M., Jayamanne, D., Cove, N., Wheeler, H., Khasraw, M., Guo, L., Back, J., & Wong, M. (2018). Optimising Outcomes for Glioblastoma through Subspecialisation in a Regional Cancer Centre. Brain Sciences, 8(10), 186. https://doi.org/10.3390/brainsci8100186