Education and Income Predict Future Emotional Well-Being of Whites but Not Blacks: A Ten-Year Cohort




Abstract
:1. Background
2. Aims
3. Methods
3.1. Design
3.2. Ethical Considerations
3.3. Data Collection
3.4. Participants and Sampling
3.5. Analytical Sample
3.6. Follow-Up Data
3.7. Measures
3.8. Statistical Analysis
4. Results
4.1. Descriptive Statistics
4.2. Bivariate Correlations
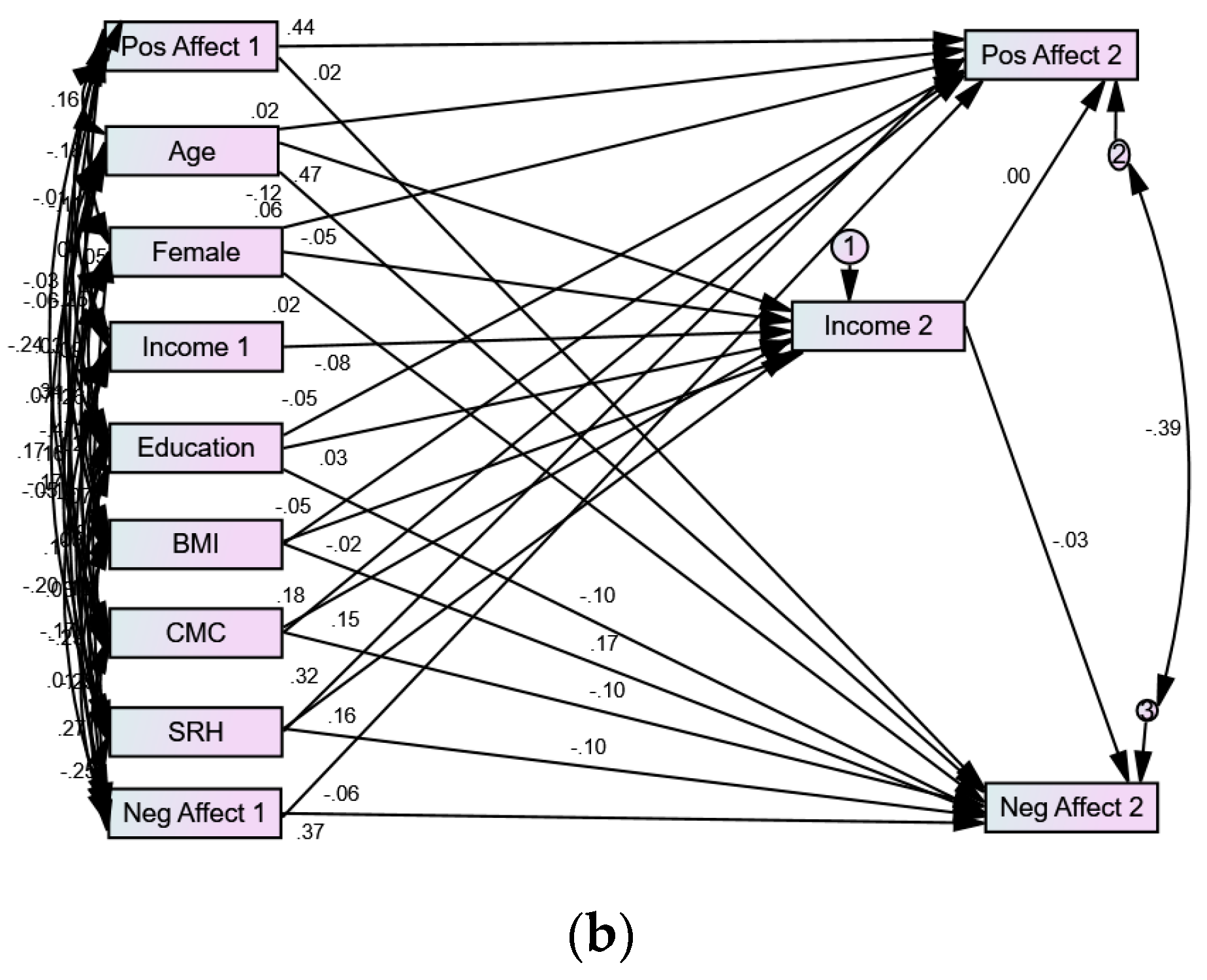
4.3. Multivariable Models
5. Discussion
5.1. Implications for Policies and Programs
5.2. Limitations and Future Directions for Research
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Adler, N.E.; Boyce, T.; Chesney, M.A.; Cohen, S.; Folkman, S.; Kahn, R.L.; Syme, S.L. Socioeconomic status and health: The challenge of the gradient. Am. Psychol. 1994, 49, 15–24. [Google Scholar] [CrossRef]
- Pratt, L.A.; Brody, D.J. Depression in the United States Household Population, 2005–2006; NCHS Data Brief No. 7; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2008.
- Fredrickson, B.; Joiner, T. Positive emotions trigger upwards spiral toward emotional well-being. Psychol. Sci. 2002, 13, 172–175. [Google Scholar] [CrossRef] [PubMed]
- Fredrickson, B.L. Cultivating positive emotions to optimize health and well-being. Prev. Treat. 2000, 3. [Google Scholar] [CrossRef]
- School of Education and Behavioural Sciences. Available online: https://www.researchgate.net/profile/Syed_Amin6/publication/321170536_INSIGHT_Journal_of_Applied_Research_in_Education/links/5a13169e0f7e9b1e572c9d5a/INSIGHT-Journal-of-Applied-Research-in-Education.pdf (accessed on 7 July 2017).
- Gallo, L.C.; Matthews, K.A. Understanding the association between socioeconomic status and physical health: Do negative emotions play a role? Psychol. Bull. 2003, 129, 10–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gallo, L.C. The Reserve Capacity Model as a Framework for Understanding Psychosocial Factors in Health Disparities. Appl. Psychol. Health Well-Being 2009, 1, 62–72. [Google Scholar] [CrossRef]
- Gallo, L.C.; Bogart, L.M.; Vranceanu, A.; Matthews, K.A.J. Socioeconomic Status, Resources, Psychological Experiences, and Emotional Responses: A Test of the Reserve Capacity Model. J. Personal. Soc. Psychol. 2005, 88, 386–399. [Google Scholar]
- Jakoby, N. Socioeconomic status differences in negative emotions. Sociol. Res. Online 2016, 21, 1–10. [Google Scholar] [CrossRef]
- Holahan, C.J.; Moos, R.H. Life stressors, personal and social resources, and depression: A 4-year structural model. J. Abnorm. Psychol. 1991, 100, 31–38. [Google Scholar] [CrossRef]
- Williams, D.R.; Sternthal, M. Understanding racial-ethnic disparities in health: Sociological contributions. J. Health Soc. Behav. 2010, 51, S15–S27. [Google Scholar] [CrossRef] [PubMed]
- Assari, S. Unequal Gain of Equal Resources across Racial Groups. Int. J. Health Policy Manag. 2018, 7, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Assari, S. Health Disparities due to Diminished Return among Black Americans: Public Policy Solutions. Soc. Issues Policy Rev. 2018, 12, 112–145. [Google Scholar] [CrossRef] [Green Version]
- Fuller-Rowell, T.E.; Curtis, D.S.; Doan, S.N.; Coe, C.L. Racial disparities in the health benefits of educational attainment: A study of inflammatory trajectories among African American and white adults. Psychosom. Med. 2015, 77, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Assari, S. Parental Education Better Helps White than Black Families Escape Poverty: National Survey of Children’s Health. Economies 2018, 6, 30. [Google Scholar] [CrossRef]
- Assari, S. Diminished Economic Return of Socioeconomic Status for Black Families. Soc. Sci. 2018, 7, 74. [Google Scholar] [CrossRef]
- Assari, S.; Lankarani, M.M. Education and Alcohol Consumption among Older Americans; Black-White Differences. Front. Public Health 2016, 4, 67. [Google Scholar] [CrossRef] [PubMed]
- Assari, S.; Mistry, R. Educational Attainment and Smoking Status in a National Sample of American Adults; Evidence for the Blacks’ Diminished Return. Int. J. Environ. Res. Public Health 2018, 15, 763. [Google Scholar] [CrossRef] [PubMed]
- Assari, S.; Lankarani, M.M. Educational Attainment Promotes Fruit and Vegetable Intake for Whites but Not Blacks. J 2018, 1, 5. [Google Scholar] [CrossRef]
- Assari, S. Combined Racial and Gender Differences in the Long-Term Predictive Role of Education on Depressive Symptoms and Chronic Medical Conditions. J. Racial Ethn. Health Dispar. 2017, 4, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Assari, S.; Thomas, A.; Caldwell, C.H.; Mincy, R.B. Blacks’ Diminished Health Return of Family Structure and Socioeconomic Status; 15 Years of Follow-up of a National Urban Sample of Youth. J. Urban Health 2018, 95, 21–35. [Google Scholar] [CrossRef] [PubMed]
- Assari, S.; Caldwell, C.H.; Mincy, R.B. Maternal Educational Attainment at Birth Promotes Future Self-Rated Health of White but Not Black Youth: A 15-Year Cohort of a National Sample. J. Clin. Med. 2018, 7, 93. [Google Scholar] [CrossRef] [PubMed]
- Hayward, M.D.; Hummer, R.A.; Sasson, I. Trends and group differences in the association between educational attainment and U.S. adult mortality: Implications for understanding education’s causal influence. Soc. Sci. Med. 2015, 127, 8–18. [Google Scholar] [CrossRef] [PubMed]
- Assari, S.; Lankarani, M.M. Race and Urbanity Alter the Protective Effect of Education but not Income on Mortality. Front. Public Health 2016, 4, 100. [Google Scholar] [CrossRef] [PubMed]
- Backlund, E.; Sorlie, P.D.; Johnson, N.J. A comparison of the relationships of education and income with mortality: The National Longitudinal Mortality Study. Soc. Sci. Med. 1999, 49, 1373–1384. [Google Scholar] [CrossRef]
- Everett, B.G.; Rehkopf, D.H.; Rogers, R.G. The Nonlinear Relationship between Education and Mortality: An Examination of Cohort, Race/Ethnic, and Gender Differences. Popul. Res. Policy Rev. 2013, 1, 32. [Google Scholar] [CrossRef] [PubMed]
- Assari, S.; Caldwell, C.H.; Mincy, R. Family Socioeconomic Status at Birth and Youth Impulsivity at Age 15; Blacks’ Diminished Return. Children 2018, 5, 58. [Google Scholar] [CrossRef] [PubMed]
- Assari, S. Family Income Reduces Risk of Obesity for White but Not Black Children. Children 2018, 5, 73. [Google Scholar] [CrossRef] [PubMed]
- Assari, S.; Hani, N. Household Income and Children’s Unmet Dental Care Need; Blacks’ Diminished Return. Dent. J. 2018, 6, 17. [Google Scholar] [CrossRef] [PubMed]
- Assari, S.; Moghani, M.L. Poverty Status and Childhood Asthma in White and Black Families: National Survey of Children’s Health. Healthcare 2018, 6, 62. [Google Scholar] [CrossRef] [PubMed]
- Assari, S. High Income Protects Whites but Not African Americans against Risk of Depression. Healthcare 2018, 6, 37. [Google Scholar] [CrossRef] [PubMed]
- Assari, S.; Lapeyrouse, L.M.; Neighbors, H.W. Income and Self-Rated Mental Health: Diminished Returns for High Income Black Americans. Behav. Sci. 2018, 8, 50. [Google Scholar] [CrossRef] [PubMed]
- Assari, S. Ethnic and Gender Differences in Additive Effects of Socio-economics, Psychiatric Disorders, and Subjective Religiosity on Suicidal Ideation among Blacks. Int. J. Prev. Med. 2015, 6, 53. [Google Scholar] [CrossRef] [PubMed]
- Assari, S.; Caldwell, C.H. High Risk of Depression in High-Income African American Boys. J. Racial Ethn. Health Dispar. 2017. [Google Scholar] [CrossRef] [PubMed]
- Assari, S. Social Determinants of Depression: The Intersections of Race, Gender, and Socioeconomic Status. Brain Sci. 2017, 7, 156. [Google Scholar] [CrossRef] [PubMed]
- Assari, S.; Nikahd, A.; Malekahmadi, M.R.; Lankarani, M.M.; Zamanian, H. Race by Gender Group Differences in the Protective Effects of Socioeconomic Factors Against Sustained Health Problems Across Five Domains. J. Racial Ethn. Health Dispar. 2016. [Google Scholar] [CrossRef] [PubMed]
- Ross, C.E.; Mirowsky, J. Refining the association between education and health: The effects of quantity, credential, and selectivity. Demography 1999, 36, 445–460. [Google Scholar] [CrossRef] [PubMed]
- Montez, J.K.; Hummer, R.A.; Hayward, M.D.; Woo, H.; Rogers, R.G. Trends in the educational gradient of US adult mortality from 1986 through 2006 by race, gender, and age group. Res. Aging 2011, 33, 145–171. [Google Scholar] [CrossRef] [PubMed]
- Hudson, D.L.; Bullard, K.M.; Neighbors, H.W.; Geronimus, A.T.; Yang, J.; Jackson, J.S. Are benefits conferred with greater socioeconomic position undermined by racial discrimination among African American men? J. Mens Health 2012, 9, 127–136. [Google Scholar] [CrossRef] [PubMed]
- Hudson, D.L. Race, Socioeconomic Position and Depression: The Mental Health Costs of Upward Mobility. Ph.D. Thesis, The University of Michigan, Ann Arbor, MI, USA, 2009. [Google Scholar]
- Radler, B.T.; Ryff, C.D. Who participates? Accounting for longitudinal retention in the MIDUS national study of health and well-being. J. Aging Health 2010, 22, 307–331. [Google Scholar] [CrossRef] [PubMed]
- Dienberg Love, G.; Seeman, T.E.; Weinstein, M.; Ryff, C.D. Bioindicators in the MIDUS national study: Protocol, measures, sample, and comparative context. J. Aging Health 2010, 22, 1059–1080. [Google Scholar] [CrossRef] [PubMed]
- Midlife in the United States (MIDUS). Available online: http://www.midus.wisc.edu (accessed on 7 July 2017).
- National Institute on Aging Database of Longitudinal Studies. Available online: http://www.nia.nih.gov/ResearchInformation/ScientificResources/LongitudinalStudies.htm (accessed on 7 July 2017).
- Snowden, M.; Dhingra, S.S.; Keyes, C.L.; Anderson, L.A. Changes in mental well-being in the transition to late life: Findings from MIDUS I and II. Am. J. Public Health 2010, 100, 2385–2388. [Google Scholar] [CrossRef] [PubMed]
- Mroczek, D.K.; Kolarz, C.M. The effect of age on positive and negative affect: A developmental perspective on happiness. J. Personal. Soc. Psychol. 1998, 75, 1333–1349. [Google Scholar] [CrossRef]
- Grzywacz, J.G. Work-family spillover and health during midlife: Is managing conflict everything? Am. J. Health Promot. 2000, 14, 236–243. [Google Scholar] [CrossRef] [PubMed]
- Keyes, C.L.M. Subjective change and its consequences for emotional well-being. Motiv. Emot. 2000, 24, 67–83. [Google Scholar] [CrossRef]
- Walen, H.R.; Lachman, M.E. Social support and strain from partner, family, and friends: Costs and benefits for men and women in adulthood. J. Soc. Pers. Relatsh. 2000, 17, 5–30. [Google Scholar] [CrossRef]
- Mroczek, D.K. Age and Emotion in Adulthood. Curr. Dir. Psychol. Sci. 2001, 10, 87–90. [Google Scholar] [CrossRef]
- Brim, O.G.; Ryff, C.D.; Kessler, R.C. (Eds.) How Healthy Are We?: A National Study of Well-Being at Midlife; University of Chicago Press: Chicago, IL, USA, 2004. [Google Scholar]
- Allison, P.D. Structural Equation Modeling with Amos: Basic Concepts, Applications, and Programming, 2nd ed.; Taylor and Francis Group: New York, NY, USA, 2002. [Google Scholar]
- Arbuckle, J.L. Amos 18 User’s Guide; Amos Development Corporation: Chicago, IL USA, 2009. [Google Scholar]
- Kline, R.B. Principles and Practice of Structural Equation Modeling, 3rd ed.; Guilford Press: New York, NY, USA, 2011. [Google Scholar]
- Hu, G.; Bouchard, C.; Bray, G.A.; Greenway, F.L.; Johnson, W.D.; Newton, R.L.; Ravussin, E.; Ryan, D.H.; Katzmarzyk, P.T. Trunk versus extremity adiposity and cardiometabolic risk factors in white and African American adults. Diabetes Care 2011, 34, 1415–1418. [Google Scholar] [CrossRef] [PubMed]
- Dion, P.A. Interpreting structural equation modeling results: A reply to Martin and Cullen. J. Bus. Ethics 2008, 83, 365–368. [Google Scholar] [CrossRef]
- Lei, M.; Lomax, R.G. The effect of varying degrees of nonnormality in structural equation modeling. Struct. Equ. Model. 2005, 12, 1–27. [Google Scholar] [CrossRef]
- Tabachnick, B.G.; Fidell, L.S. Using Multivariate Statistics, 3rd ed.; Harper Collins: New York, NY, USA, 1996. [Google Scholar]
- Assari, S. The link between mental health and obesity: Role of individual and contextual factors. Int. J. Prev. Med. 2014, 5, 247–249. [Google Scholar] [PubMed]
- Assari, S.; Preiser, B.; Lankarani, M.M.; Caldwell, C.H. Subjective Socioeconomic Status Moderates the Association between Discrimination and Depression in African American Youth. Brain Sci. 2018, 8, 71. [Google Scholar] [CrossRef] [PubMed]
- Assari, S.; Lankarani, M.M.; Caldwell, C.H. Does Discrimination Explain High Risk of Depression among High-Income African American Men? Behav. Sci. 2018, 8, 40. [Google Scholar] [CrossRef] [PubMed]
- Assari, S. Socioeconomic Status and Self-Rated Oral Health; Diminished Return among Hispanic Whites. Dent. J. 2018, 6, 11. [Google Scholar] [CrossRef] [PubMed]
- Assari, S.; Caldwell, C.H. Social Determinants of Perceived Discrimination among Black Youth: Intersection of Ethnicity and Gender. Children 2018, 5, 24. [Google Scholar] [CrossRef] [PubMed]
- Assari, S. Life Expectancy Gain Due to Employment Status Depends on Race, Gender, Education, and Their Intersections. J. Racial Ethn. Health Dispar. 2018, 5, 375–386. [Google Scholar] [CrossRef] [PubMed]
- Azizi, M.; Mohamadian, F.; Ghajarieah, M.; Direkvand-Moghadam, A. The Effect of Individual Factors, Socioeconomic and Social Participation on Individual Happiness: A Cross-Sectional Study. J. Clin. Diagn. Res. 2017, 11, VC01–VC04. [Google Scholar] [CrossRef] [PubMed]
- Phelan, J.C.; Link, B.G.; Tehranifar, P. Social conditions as fundamental causes of health inequalities: Theory, evidence, and policy implications. J. Health Soc. Behav. 2010, 51, S28–S40. [Google Scholar] [CrossRef] [PubMed]
- Link, B.G.; Phelan, J. Social Conditions as Fundamental Causes of Health Inequalities. In Handbook of Medical Sociology; Prentice Hall: Upper Saddle River, NJ, USA, 2010; pp. 3–17. [Google Scholar]
- Link, B.; Phelan, J. Social conditions as fundamental causes of disease. J. Health Soc. Behav 1995, 36, 80–94. [Google Scholar] [CrossRef]
- Phelan, J.C.; Link, B.G. Is racism a fundamental cause of inequalities in health? Annu. Rev. Sociol. 2015, 41, 311–330. [Google Scholar] [CrossRef]
- Ben-Shlomo, Y.; Diana Kuh, D. A life course approach to chronic disease epidemiology: Conceptual models, empirical challenges and interdisciplinary perspectives. Int. J. Epidemiol. 2002, 31, 285–293. [Google Scholar] [CrossRef] [PubMed]
- Kuh, D.; Ben-Shlomo, Y.; Lynch, J.; Hallqvist, J.; Power, C. Life course epidemiology. J. Epidemiol. Commun. Health 2003, 57, 778. [Google Scholar] [CrossRef]
- Lynch, J.; Smith, G.D. A life course approach to chronic disease epidemiology. Annu. Rev. Public Health 2005, 26, 1–35. [Google Scholar] [CrossRef] [PubMed]
- Keyes, C.L. The Black-White paradox in health: Flourishing in the face of social inequality and discrimination. J. Personal. 2009, 77, 1677–1706. [Google Scholar] [CrossRef] [PubMed]
- Hudson, D.L.; Neighbors, H.W.; Geronimus, A.T.; Jackson, J.S. Racial Discrimination, John Henryism, and Depression among African Americans. J. Black Psychol. 2016, 42, 221–243. [Google Scholar] [CrossRef] [PubMed]
- Hudson, D.L.; Eaton, J.; Banks, A.; Sewell, W.; Neighbors, H. “Down in the Sewers”: Perceptions of Depression and Depression Care Among African American Men. Am. J. Mens Health 2018, 12, 126–137. [Google Scholar] [CrossRef] [PubMed]
- Fuller-Rowell, T.E.; Doan, S.N. The social costs of academic success across ethnic groups. Child Dev. 2010, 81, 1696–1713. [Google Scholar] [CrossRef] [PubMed]
- Zajacova, A.; Everett, B.G. The nonequivalent health of high school equivalents. Soc. Sci. Q. 2014, 95, 221–238. [Google Scholar] [CrossRef] [PubMed]
- Williams, D.R.; Mohammed, S.A.; Leavell, J.; Collins, C. Race, socioeconomic status, and health: Complexities, ongoing challenges, and research opportunities. Ann. N. Y. Acad. Sci. 2010, 1186, 69–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferraro, K.F.; Kelley-Moore, J.A. Self-rated health and mortality among black and white adults: Examining the dynamic evaluation thesis. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2001, 56, S195–S205. [Google Scholar] [CrossRef]
- Sellers, S.L.; Neighbors, H.W. Effects of Goal-Striving Stress on the Mental Health of Black Americans. J. Health Soc. Behav. 2008, 49, 92–103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neighbors, H.W.; Sellers, S.L.; Zhang, R.; Jackson, J.S. Goal-striving stress and racial differences in mental health. Race Soc. Probl. 2011, 3, 51–62. [Google Scholar] [CrossRef]
- Sellers, S.L.; Neighbors, H.W.; Bonham, V.L. Goal-striving stress and the mental health of college-educated Black American Men: The protective effects of system-blame. Am. J. Orthopsychiatr. 2011, 81, 507. [Google Scholar] [CrossRef] [PubMed]
- Messersmith, E.E.; Schulenberg, J.E. Goal attainment, goal striving, and well-being during the transition to adulthood: A ten-year US national longitudinal study. New Dir. Child Adolesc. Dev. 2010, 2010, 27–40. [Google Scholar] [CrossRef] [PubMed]
- Assari, S.; Howard Caldwell, C. Income and Depression among Black; Gender by Ethnic Differences in a National Sample. J. Racial Ethn. Health Dispar. 2015, 2, 481–493. [Google Scholar] [CrossRef] [PubMed]
- Oliver, M.L.; Shapiro, T.M. Black Wealth/White Wealth; Routledge: New York, NY, USA, 1995. [Google Scholar]
- Oliver, M.L.; Shapiro, T.M. Black Wealth, White Wealth: A New Perspective on Racial Inequality; Taylor & Francis: New York, NY, USA, 2013. [Google Scholar]
- Shapiro, T.; Meschede, T.; Osoro, S. The Roots of the Widening Racial Wealth Gap: Explaining the Black-White Economic Divide; Research and Policy Brief; Institute on Assets and Social Policy, Brandeis University: Waltham, MA, USA, 2013. [Google Scholar]
- Pompili, M.; Innamorati, M.; Forte, A.; Longo, L.; Mazzetta, C.; Erbuto, D.; Lamis, D.A. Insomnia as a predictor of high-lethality suicide attempts. Int. J. Clin. Pract. 2013, 67, 1311–1316. [Google Scholar] [CrossRef] [PubMed]
- Saunders, E.F.; Fernandez-Mendoza, J.; Kamali, M.; Assari, S.; McInnis, M.G. The effect of poor sleep quality on mood outcome differs between men and women: A longitudinal study of bipolar disorder. J. Affect. Disord. 2015, 180, 90–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Assari, S.; Sonnega, A.; Pepin, R.; Leggett, A. Residual effects of restless sleep over depressive symptoms on chronic medical conditions: Race by gender differences. J. Racial Ethn. Health Dispar. 2017, 4, 59–69. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| All n = 3731 | Whites n = 3596 | Blacks n = 135 | ||||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | |
| Age | 47.41 | 12.39 | 47.44 | 12.40 | 46.57 | 12.25 |
| Income1 (Personal) * | 27,511.15 | 27,372.27 | 27,686.58 | 27,563.13 | 22,810.08 | 21,187.33 |
| Income 2 (household) * | 42,525.09 | 40,669.14 | 42,661.16 | 40,868.10 | 38,423.42 | 34,032.02 |
| Self-Rated Health (SRH)* | 7.58 | 1.50 | 7.57 | 1.49 | 7.84 | 1.72 |
| Chronic Medical Conditions (CMC)* | 2.31 | 2.35 | 2.31 | 2.34 | 2.49 | 2.66 |
| Body Mass Index (BMI)* | 26.69 | 5.19 | 26.59 | 5.09 | 29.35 | 6.93 |
| Positive Affect 1 * | 3.41 | 0.71 | 3.41 | 0.71 | 3.55 | 0.75 |
| Positive Affect 2 | 3.43 | 0.70 | 3.43 | 0.70 | 3.55 | 0.79 |
| Negative Affect 1 | 1.50 | 0.58 | 1.50 | 0.58 | 1.55 | 0.76 |
| Negative Affect 2 * | 1.50 | 0.57 | 1.50 | 0.56 | 1.65 | 0.82 |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | |
| Race (Black) | 1 | 0.05 ** | −0.01 | −0.04 * | −0.03 * | 0.03 | 0.03 * | 0.01 | 0.10 ** | 0.04 | 0.03 * | 0.02 | 0.05 ** |
| Gender (Female) | 1 | −0.02 | −0.09 ** | −0.38 ** | −0.16 ** | −0.01 | 0.14 ** | −0.10 ** | −0.03 | −0.01 | 0.09 ** | 0.09 ** | |
| Age | 1 | −0.11 ** | −0.12 ** | 0.39 ** | 0.03 * | 0.16 ** | 0.01 ** | 0.11 ** | 0.14 ** | −0.12 ** | −0.10 ** | ||
| Education | 1 | 0.26 ** | 0.06 ** | 0.05 ** | −0.11 ** | −0.10 ** | 0.02 | 0.03 | −0.07 ** | −0.11 ** | |||
| Income 1 | 1 | 0.08 ** | 0.09 ** | −0.17 ** | 0.01 | 0.04 * | 0.07 ** | −0.11 ** | −0.15 ** | ||||
| Income 2 | 1 | 0.01 | 0.06 ** | 0.04 * | 0.05 ** | 0.10 ** | −0.08 ** | −0.10 ** | |||||
| Self-Rated Health (SRH) | 1 | −0.39 ** | −0.25 ** | 0.39 ** | 0.32 ** | −0.34 ** | −0.27 ** | ||||||
| Chronic Medical Conditions (CMC) | 1 | 0.17 ** | −0.31 ** | −0.23 ** | 0.39 ** | 0.28 ** | |||||||
| Body Mass Index (BMI) | 1 | −0.05 ** | −0.06 ** | 0.05 ** | 0.08 ** | ||||||||
| Positive Affect 1 | 1 | 0.53 ** | −0.63 ** | −0.37 ** | |||||||||
| Positive Affect 2 | 1 | −0.38 ** | −0.61 ** | ||||||||||
| Negative Affect 1 | 1 | 0.50 ** | |||||||||||
| Negative Affect 2 | 1 | ||||||||||||
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | |
| Race (Black) | 1 | 0.05 ** | −0.01 | −0.04 * | −0.03 * | 0.03 | 0.03 * | 0.01 | 0.10 ** | 0.04 | 0.03 * | 0.02 | 0.05 ** |
| Gender (Female) | 1 | −0.02 | −0.09 ** | −0.38 ** | −0.16 ** | −0.01 | 0.14 ** | −0.10 ** | −0.03 | −0.01 | 0.09 ** | 0.09 ** | |
| Age | 1 | −0.11 ** | −0.12 ** | 0.39 ** | 0.03 * | 0.16 ** | 0.01 ** | 0.11 ** | 0.14 ** | −0.12 ** | −0.10 ** | ||
| Education | 1 | 0.26 ** | 0.06 ** | 0.05 ** | −0.11 ** | −0.10 ** | 0.02 | 0.03 | −0.07 ** | −0.11 ** | |||
| Income 1 | 1 | 0.08 ** | 0.09 ** | −0.17 ** | 0.01 | 0.04 * | 0.07 ** | −0.11 ** | −0.15 ** | ||||
| Income 2 | 1 | 0.01 | 0.06 ** | 0.04 * | 0.05 ** | 0.10 ** | −0.08 ** | −0.10 ** | |||||
| Self-Rated Health (SRH) | 1 | −0.39 ** | −0.25 ** | 0.39 ** | 0.32 ** | −0.34 ** | −0.27 ** | ||||||
| Chronic Medical Conditions (CMC) | 1 | 0.17 ** | −0.31 ** | −0.23 ** | 0.39 ** | 0.28 ** | |||||||
| Body Mass Index (BMI) | 1 | −0.05 ** | −0.06 ** | 0.05 ** | 0.08 ** | ||||||||
| Positive Affect 1 | 1 | 0.53 ** | −0.63 ** | −0.37 ** | |||||||||
| Positive Affect 2 | 1 | −0.38 ** | −0.61 ** | ||||||||||
| Negative Affect 1 | 1 | 0.50 ** | |||||||||||
| Negative Affect 2 | 1 |
| Whites | Blacks | ||||||
|---|---|---|---|---|---|---|---|
| Estimate | S.E. | p | Estimate | S.E. | p | ||
| Education | Income 2 | 0.09 | 0.22 | <0.001 | 0.03 | 1.50 | 0.765 |
| Gender | Income 2 | −0.12 | 0.22 | <0.001 | −0.05 | 1.61 | 0.615 |
| Income 1 | Income 2 | 0.06 | 0.00 | 0.001 | −0.08 | 0.00 | 0.467 |
| Age | Income 2 | 0.40 | 0.01 | <0.001 | 0.47 | 0.06 | <0.001 |
| Self-Rated Health (SRH) | Income 2 | −0.01 | 0.08 | 0.814 | 0.16 | 0.46 | 0.131 |
| Chronic Medical Conditions (CMC) | Income 2 | 0.03 | 0.05 | 0.183 | 0.15 | 0.29 | 0.151 |
| Body Mass Index (BMI) | Income 2 | 0.00 | 0.02 | 0.866 | −0.02 | 0.11 | 0.836 |
| Positive Affect 1 | Positive Affect 2 | 0.44 | 0.02 | <0.001 | 0.44 | 0.09 | <0.001 |
| Negative Affect 1 | Negative Affect 2 | 0.39 | 0.02 | <0.001 | 0.37 | 0.10 | <0.001 |
| Education | Positive Affect 2 | 0.02 | 0.02 | 0.25 | −0.05 | 0.11 | 0.44 |
| Income 2 | Positive Affect 2 | 0.06 | 0.00 | <0.001 | −0.01 | 0.01 | 0.962 |
| Income 2 | Negative Affect 2 | −0.04 | 0.00 | 0.014 | −0.03 | 0.01 | 0.817 |
| Age | Negative Affect 2 | −0.05 | 0.00 | 0.003 | −0.12 | 0.01 | 0.190 |
| Age | Positive Affect 2 | 0.07 | 0.00 | <0.001 | 0.02 | 0.01 | 0.787 |
| Gender | Negative Affect 2 | 0.02 | 0.02 | 0.156 | 0.02 | 0.14 | 0.769 |
| Gender | Positive Affect 2 | 0.02 | 0.02 | 0.173 | 0.06 | 0.12 | 0.414 |
| Education | Negative Affect 2 | −0.07 | 0.02 | <0.001 | −0.11 | 0.13 | 0.172 |
| Negative Affect 1 | Positive Affect 2 | −0.04 | 0.02 | 0.066 | −0.06 | 0.08 | 0.469 |
| Body Mass Index (BMI) | Positive Affect 2 | 0.00 | 0.00 | 0.892 | −0.05 | 0.01 | 0.518 |
| Body Mass Index (BMI) | Negative Affect 2 | 0.01 | 0.00 | 0.572 | 0.17 | 0.01 | 0.036 |
| Chronic Medical Conditions (CMC) | Positive Affect 2 | −0.06 | 0.01 | <0.001 | 0.18 | 0.02 | 0.016 |
| Chronic Medical Conditions (CMC) | Negative Affect 2 | 0.10 | 0.00 | <0.001 | −0.1 | 0.03 | 0.225 |
| Self-Rated Health (SRH) | Positive Affect 2 | 0.10 | 0.01 | <0.001 | 0.32 | 0.04 | <0.001 |
| Self-Rated Health (SRH) | Negative Affect 2 | −0.07 | 0.01 | <0.001 | −0.11 | 0.04 | 0.236 |
| Positive Affect 1 | Negative Affect 2 | −0.07 | 0.02 | <0.001 | 0.02 | 0.10 | 0.785 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Assari, S.; Preiser, B.; Kelly, M. Education and Income Predict Future Emotional Well-Being of Whites but Not Blacks: A Ten-Year Cohort. Brain Sci. 2018, 8, 122. https://doi.org/10.3390/brainsci8070122
Assari S, Preiser B, Kelly M. Education and Income Predict Future Emotional Well-Being of Whites but Not Blacks: A Ten-Year Cohort. Brain Sciences. 2018; 8(7):122. https://doi.org/10.3390/brainsci8070122
Chicago/Turabian StyleAssari, Shervin, Brianna Preiser, and Marisa Kelly. 2018. "Education and Income Predict Future Emotional Well-Being of Whites but Not Blacks: A Ten-Year Cohort" Brain Sciences 8, no. 7: 122. https://doi.org/10.3390/brainsci8070122
APA StyleAssari, S., Preiser, B., & Kelly, M. (2018). Education and Income Predict Future Emotional Well-Being of Whites but Not Blacks: A Ten-Year Cohort. Brain Sciences, 8(7), 122. https://doi.org/10.3390/brainsci8070122