
Randomized Clinical Trial of How Long-Term Glutathione Supplementation Offers Protection from Oxidative Damage and Improves HbA1c in Elderly Type 2 Diabetic Patients

 , , and
, , and
Abstract
:1. Introduction
2. Subjects, Materials, and Methods
2.1. Ethical Approval
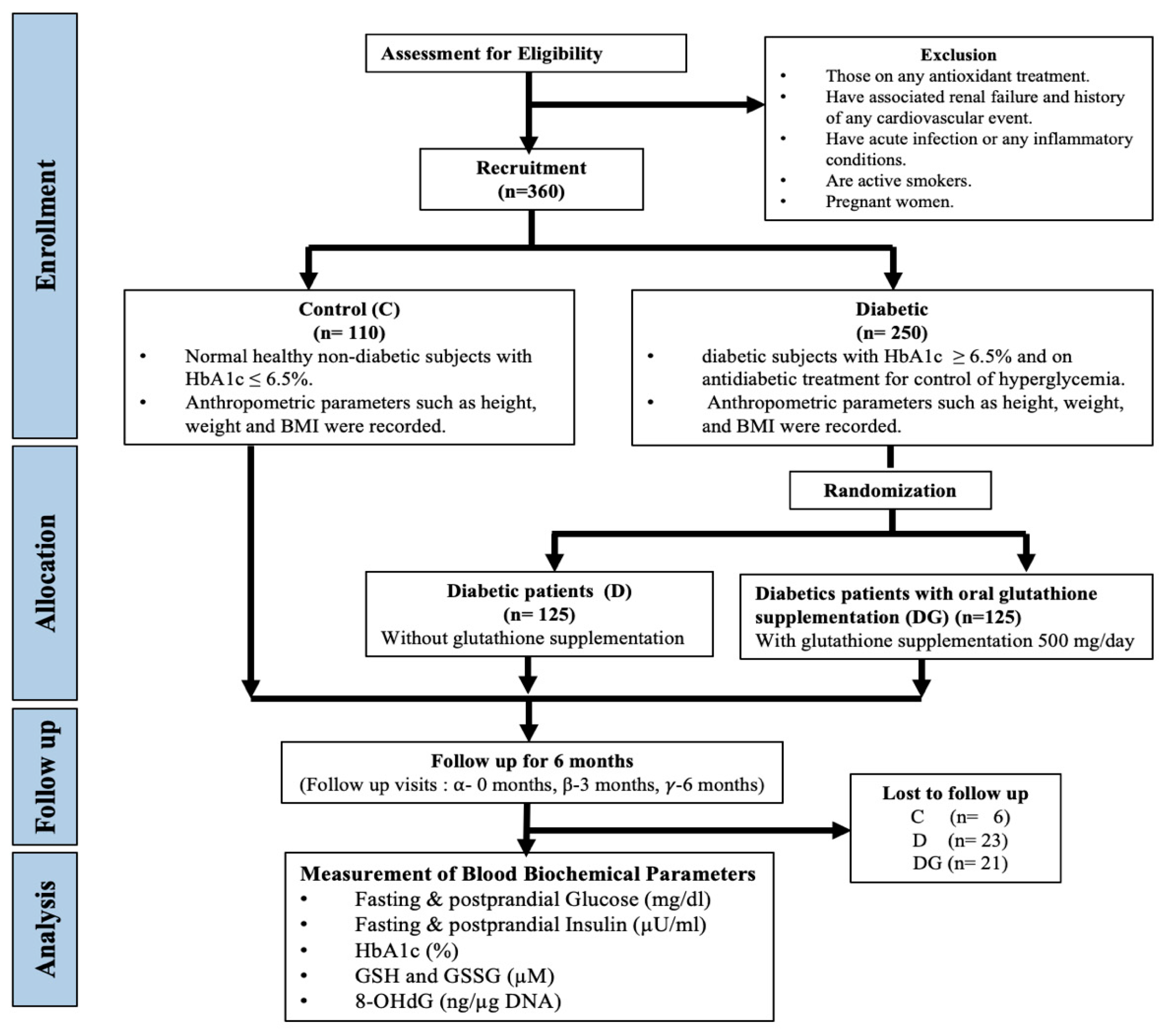
2.2. Study Design
2.3. Inclusion/Exclusion Criteria for Study Participants
2.4. Recruitment and Randomization for GSH Intervention
2.4.1. Sample Size Calculation
2.4.2. Sample Collection
2.5. Estimation of Blood Biochemical Parameters
2.6. Estimation of GSH and GSSG
2.7. Estimation of 8-OHdG
3. Results
3.1. Baseline Characteristics
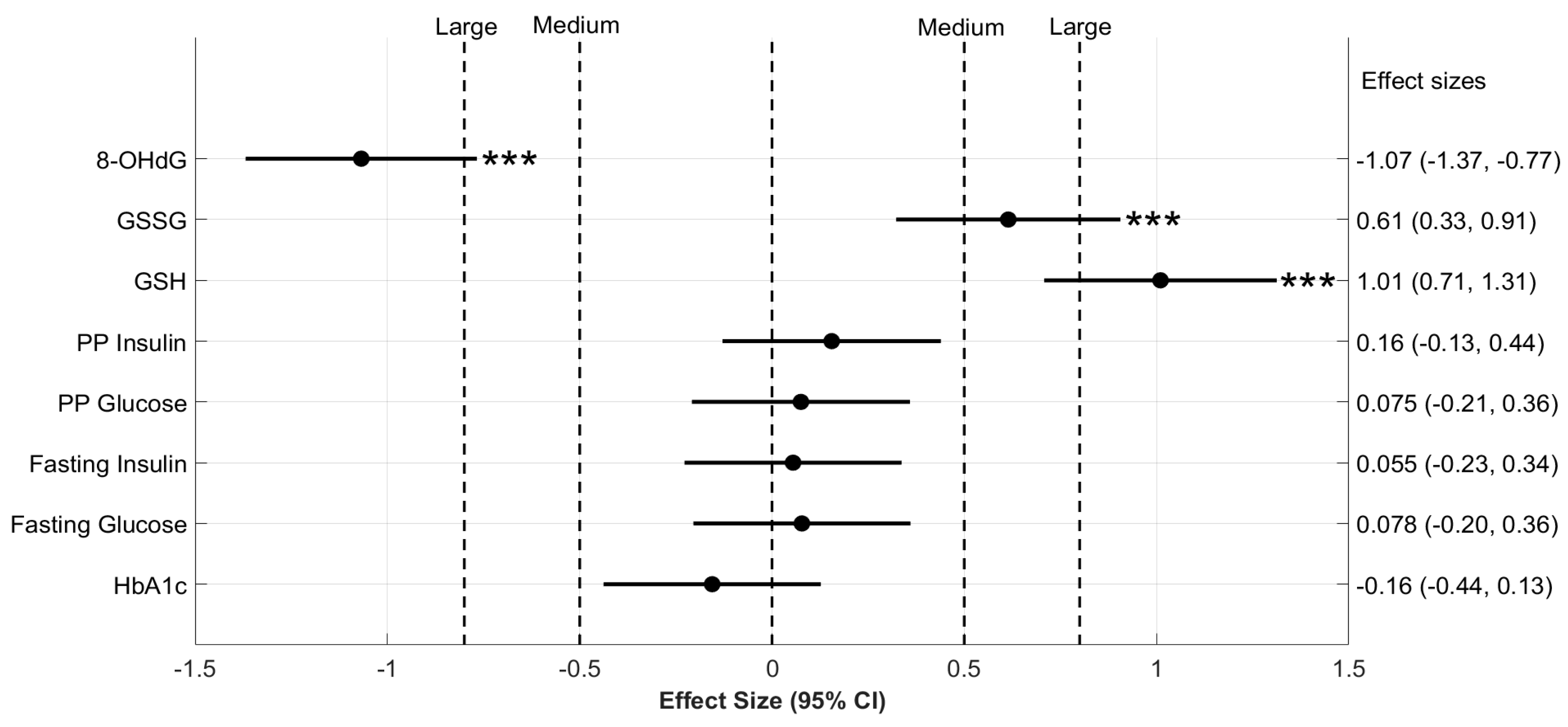
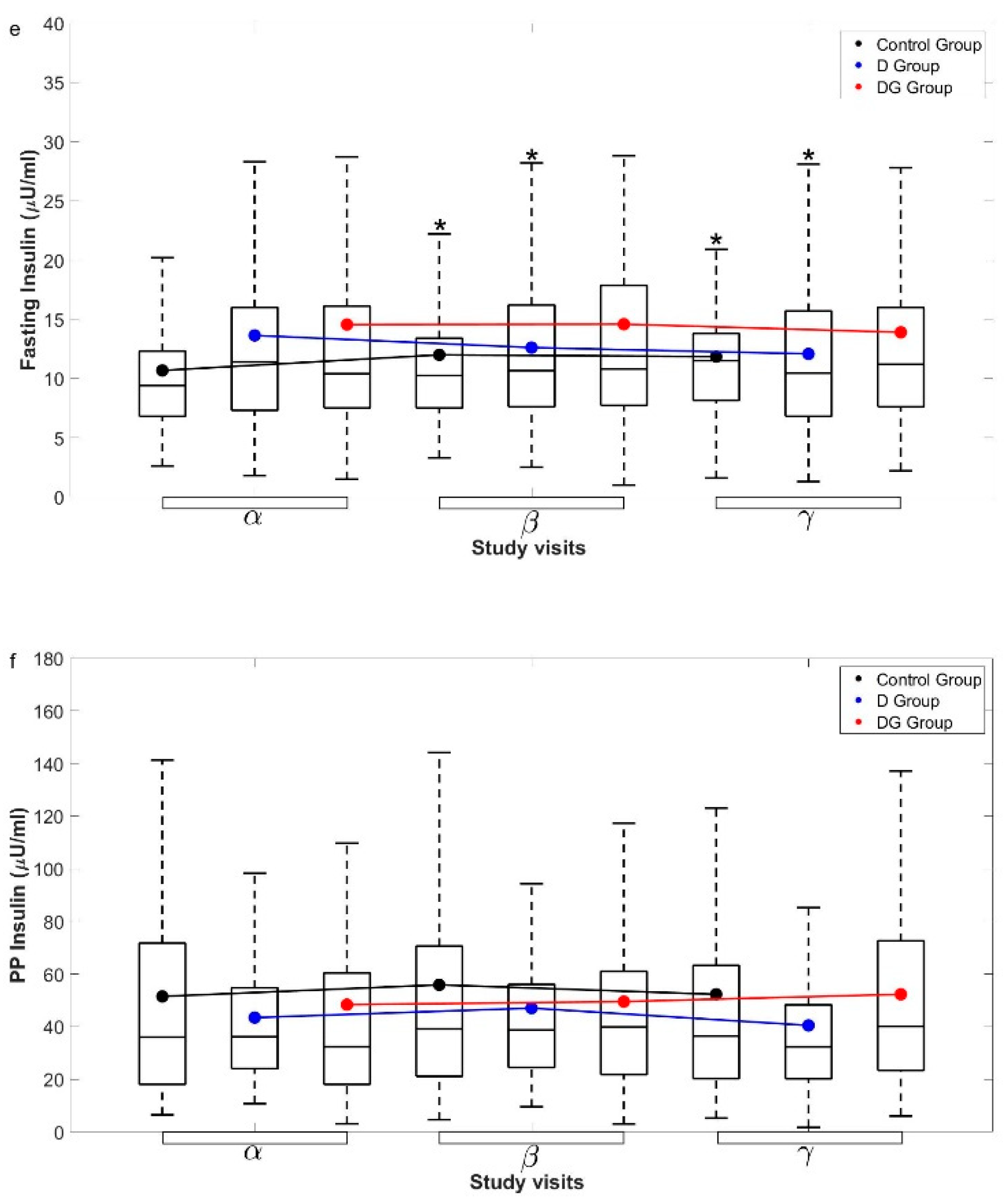
3.2. Oral GSH Supplementation Increases Erythrocyte GSH and Decreases Oxidative Damage to DNA but Does Not Alter Glycemia in Diabetic Patients over a Period of Six Months
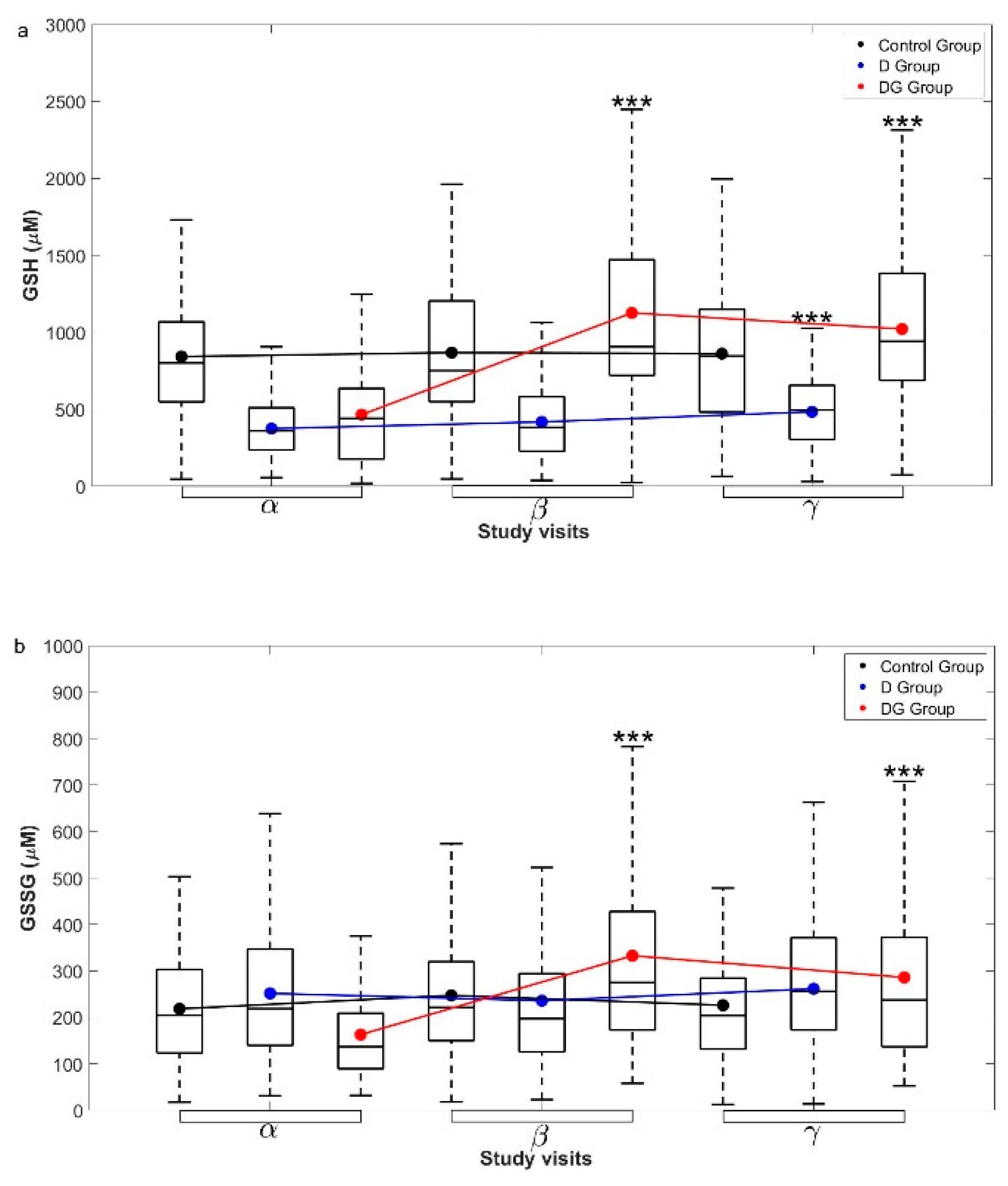
3.3. Oral GSH Supplementation Enhances Erythrocyte GSH in Diabetic Subjects within Three Months
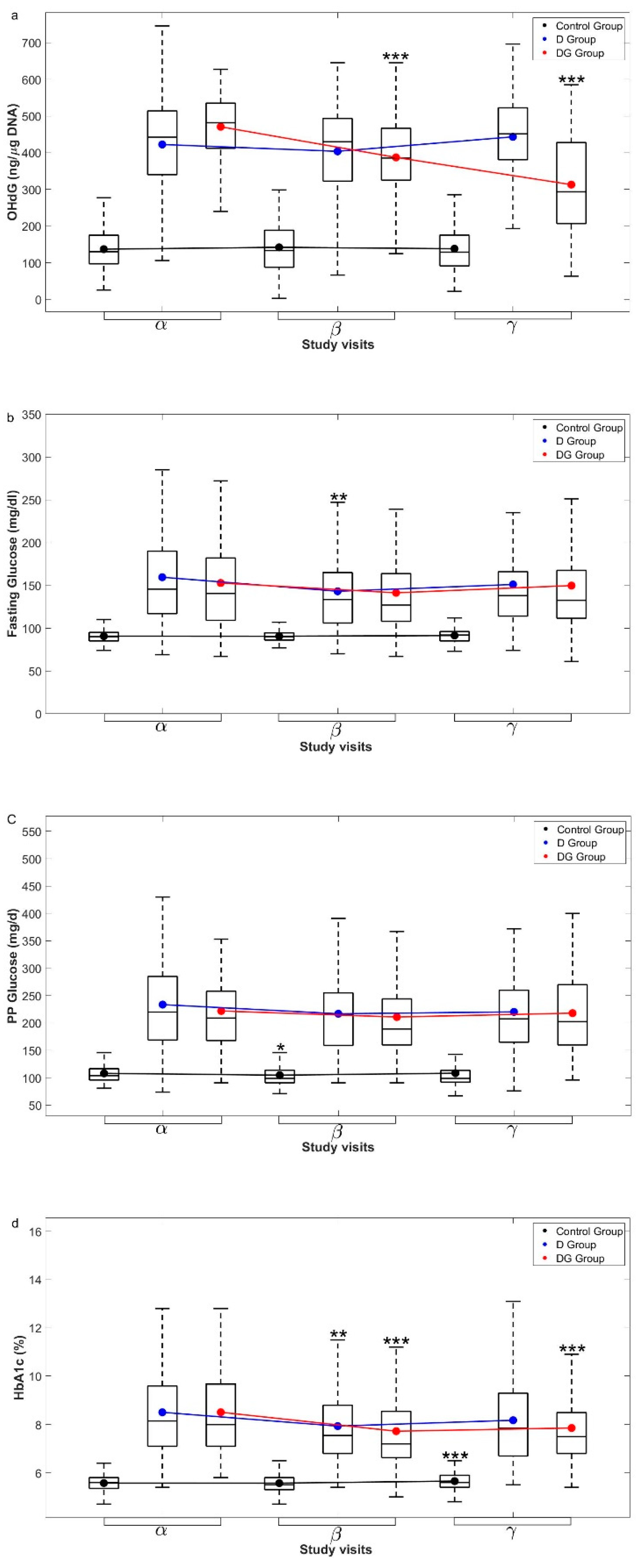
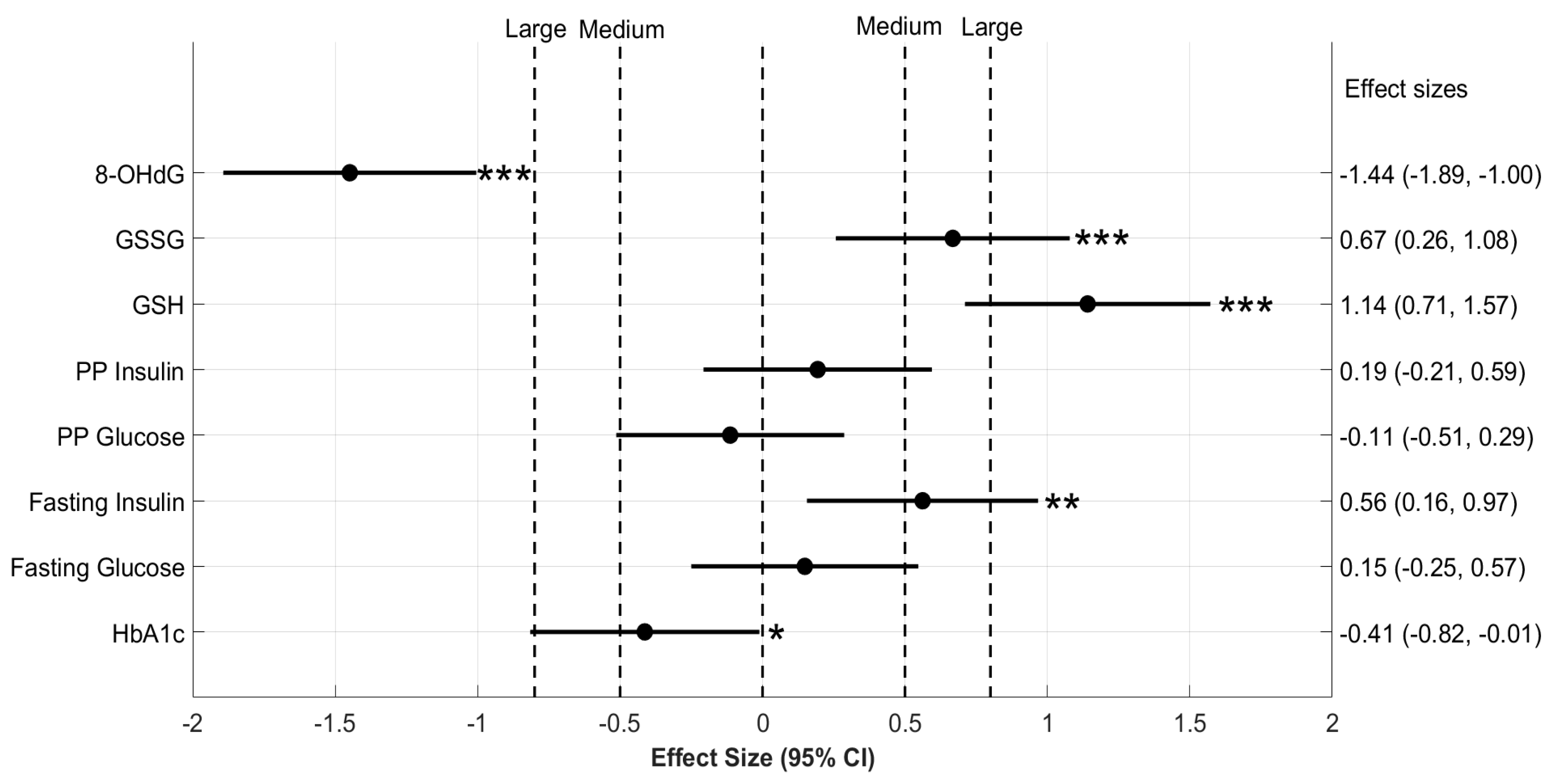
3.4. Oral GSH Supplementation Significantly Reduces 8-OHdG in Diabetic Subjects
3.5. HbA1c Levels Are Stabilized by Oral GSH Supplementation in Diabetic Patients
3.6. A Oral GSH Supplementation Significantly Reduces HbA1c in Elderly Diabetic Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Brownlee, M. The Pathobiology of Diabetic Complications: A Unifying Mechanism. Diabetes 2005, 54, 1615–1625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haber, C.A.; Lam, T.K.T.; Yu, Z.; Gupta, N.; Goh, T.; Bogdanovic, E.; Giacca, A.; Fantus, I.G. N-acetylcysteine and taurine prevent hyperglycemia-induced insulin resistance in vivo: Possible role of oxidative stress. Am. J. Physiol. Endocrinol. Metab. 2003, 285, E744–E753. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ueno, Y.; Kizaki, M.; Nakagiri, R.; Kamiya, T.; Sumi, H.; Osawa, T. Dietary Glutathione Protects Rats from Diabetic Nephropathy and Neuropathy. J. Nutr. 2002, 132, 897–900. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jain, S.K.; Velusamy, T.; Croad, J.L.; Rains, J.L.; Bull, R. L-Cysteine supplementation lowers blood glucose, glycated hemoglobin, CRP, MCP-1, and oxidative stress and inhibits NF-κB activation in the livers of Zucker diabetic rats. Free Radic. Biol. Med. 2002, 46, 1633–1638. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El-Hafidi, M.; Franco, M.; Ramírez, A.R.; Sosa, J.S.; Flores, J.A.P.; Acosta, O.L.; Salgado, M.C.; Cardoso-Saldaña, G. Glycine Increases Insulin Sensitivity and Glutathione Biosynthesis and Protects against Oxidative Stress in a Model of Sucrose-Induced Insulin Resistance. Oxid. Med. Cell. Longev. 2018, 2018, 2101562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Townsend, D.M.; Tew, K.D.; Tapiero, H. The importance of glutathione in human disease. Biomed. Pharmacother. 2003, 57, 145–155. [Google Scholar] [CrossRef]
- Song, F.; Jia, W.; Yao, Y.; Hu, Y.; Lei, L.; Lin, J.; Sun, X.; Liu, L. Oxidative stress, antioxidant status and DNA damage in patients with impaired glucose regulation and newly diagnosed Type 2 diabetes. Clin. Sci. 2007, 112, 599–606. [Google Scholar] [CrossRef] [Green Version]
- Acharya, J.D.; Pande, A.J.; Joshi, S.M.; Yajnik, C.S.; Ghaskadbi, S.S. Treatment of hyperglycaemia in newly diagnosed diabetic patients is associated with a reduction in oxidative stress and improvement in β-cell function: Glucose Control Reduces Oxidative Stress. Diabetes Metab. Res. Rev. 2014, 30, 590–598. [Google Scholar] [CrossRef]
- Picu, A.; Petcu, L.; Ştefan, S.; Mitu, M.; Lixandru, D.; Ionescu-Tîrgovişte, C.; Pîrcălăbioru, G.G.; Ciulu-Costinescu, F.; Bubulica, M.-V.; Chifiriuc, M.C. Markers of Oxidative Stress and Antioxidant Defense in Romanian Patients with Type 2 Diabetes Mellitus and Obesity. Molecules 2017, 22, 714. [Google Scholar] [CrossRef]
- Schmitt, B.; Vicenzi, M.; Garrel, C.; Denis, F.M. Effects of N-acetylcysteine, oral glutathione (GSH) and a novel sublingual form of GSH on oxidative stress markers: A comparative crossover study. Redox Biol. 2017, 6, 198–205. [Google Scholar] [CrossRef] [Green Version]
- Buonocore, D.; Grosini, M.; Giardina, S.; Michelotti, A.; Carrabetta, M.; Seneci, A.; Verri, M.; Dossena, M.; Marzatico, F. Bioavailability study of an innovative orobuccal formulation of glutathione. Oxid. Med. Cell. Longev. 2016, 2016, 3286365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruggeman, B.K.; Storo, K.E.; Fair, H.M.; Wommack, A.J.; Carriker, C.R.; Smoliga, J.M. The absorptive effects of orobuccal non-liposomal nano-sized glutathione on blood glutathione parameters in healthy individuals: A pilot study. PLoS ONE 2019, 14, e0215815. [Google Scholar] [CrossRef] [PubMed]
- Sinha, R.; Sinha, I.; Calcagnotto, A.; Trushin, N.; Haley, J.S.; Schell, T.D.; Richie, J.P. Oral supplementation with liposomal glutathione elevates body stores of glutathione and markers of immune function. Eur. J. Clin. Nutr. 2018, 72, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Richie, J.P.; Nichenametla, S.; Neidig, W.; Calcagnotto, A.; Haley, J.S.; Schell, T.D.; Muscat, J.E. Randomized controlled trial of oral glutathione supplementation on body stores of glutathione. Eur. J. Nutr. 2015, 54, 251–263. [Google Scholar] [CrossRef] [PubMed]
- Allen, J.; Bradley, R.D. Effects of Oral Glutathione Supplementation on Systemic Oxidative Stress Biomarkers in Human Volunteers. J. Altern. Complement. Med. 2011, 17, 827–833. [Google Scholar] [CrossRef] [Green Version]
- Sekhar, R.V.; Patel, S.G.; Guthikonda, A.P.; Reid, M.; Balasubramanyam, A.; Taffet, G.E.; Jahoor, F. Deficient synthesis of glutathione underlies oxidative stress in aging and can be corrected by dietary cysteine and glycine supplementation. Am. J. Clin. Nutr. 2011, 94, 847–853. [Google Scholar] [CrossRef] [Green Version]
- Sekhar, R.V.; McKay, S.V.; Patel, S.G.; Guthikonda, A.P.; Reddy, V.T.; Balasubramanyam, A.; Jahoor, F. Glutathione Synthesis Is Diminished in Patients With Uncontrolled Diabetes and Restored by Dietary Supplementation With Cysteine and Glycine. Diabetes Care 2011, 34, 162–167. [Google Scholar] [CrossRef] [Green Version]
- Paolisso, G.; Di Maro, G.; Pizza, G.; D’Amore, A.; Sgambato, S.; Tesauro, P.; Varricchio, M.; D’Onofrio, F. Plasma GSH/GSSG affects glucose homeostasis in healthy subjects and non-insulin-dependent diabetics. Am. J. Physiol. Endocrinol. Metab. 1992, 263, E435–E440. [Google Scholar] [CrossRef]
- Paolisso, G.; Giugliano, D.; Pizza, G.; Gambardella, A.; Tesauro, P.; Varricchio, M.; D’Onofrio, F. Glutathione Infusion Potentiates Glucose-Induced Insulin Secretion in Aged Patients With Impaired Glucose Tolerance. Diabetes Care 1992, 15, 1–7. [Google Scholar] [CrossRef]
- ADA. Classification and Diagnosis of Diabetes. Diabetes Care 2016, 39, S13–S22. [Google Scholar] [CrossRef] [Green Version]
- Baker, M.A.; Cerniglia, G.J.; Zaman, A. Microtiter plate assay for the measurement of glutathione and glutathione disulfide in large numbers of biological samples. Anal. Biochem. 1990, 190, 360–365. [Google Scholar] [CrossRef]
- Modak, M.A.; Parab, P.B.; Ghaskadbi, S.S. Pancreatic Islets Are Very Poor in Rectifying Oxidative DNA Damage. Pancreas 2009, 38, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Hothorn, T.; Hornik, K.; van de Wiel, M.A.; Zeileis, A. A Lego System for Conditional Inference. Am. Stat. 2006, 60, 257–263. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Routledge: New York, NY, USA, 2013. [Google Scholar] [CrossRef]
- Sawilowsky, S.S. A Different Future For Social And Behavioral Science Research. J. Mod. Appl. Stat. Methods 2003, 2, 128–132. [Google Scholar] [CrossRef] [Green Version]
- Erdennal, M.; Sunal, E.; Kanbak, G. Age-related changes in the glutathione redox system. Cell Biochem. Funct. 2002, 20, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Kulkarni, R.; Acharya, J.; Ghaskadbi, S.; Goel, P. Thresholds of Oxidative Stress in Newly Diagnosed Diabetic Patients on Intensive Glucose-Control Therapy. PLoS ONE 2014, 9, e100897. [Google Scholar] [CrossRef] [PubMed]
- Kovacs-Nolan, J.; Rupa, P.; Matsui, T.; Tanaka, M.; Konishi, T.; Sauchi, Y.; Sato, K.; Ono, S.; Mine, Y. In Vitro and ex Vivo Uptake of Glutathione (GSH) across the Intestinal Epithelium and Fate of Oral GSH after in Vivo Supplementation. J. Agric. Food Chem. 2014, 62, 9499–9506. [Google Scholar] [CrossRef]
- Hanigan, M.H. Gamma-Glutamyl Transpeptidase. In Advances in Cancer Research; Townsend, D.M., Tew, K.D., Eds.; Elsevier: Amsterdam, The Netherlands, 2014; pp. 103–141. [Google Scholar]
- Anjaneyulu, K.; Anjaneyulu, R.; Sener, A.; Malaisse, W.J. The stimulus-secretion coupling of glucose-induced insulin release. Thiol: Disulfide balance in pancreatic islets. Biochimie 1982, 64, 29–36. [Google Scholar] [CrossRef]
- Lenzen, S.; Drinkgern, J.; Tiedge, M. Low antioxidant enzyme gene expression in pancreatic islets compared with various other mouse tissues. Free Radic. Biol. Med. 1996, 20, 463–466. [Google Scholar] [CrossRef]
- Ammon, H.P.T.; Klumpp, S.; Fuss, A.; Verspohl, E.J.; Jaeschke, H.; Wendel, A.; Müller, P. A possible role of plasma glutathione in glucose-mediated insulin secretion: In Vitro and In Vivo studies in rats. Diabetologia 1989, 32, 797–800. [Google Scholar] [CrossRef] [Green Version]
- Yabe, D.; Seino, Y. Type 2 diabetes via β-cell dysfunction in east Asian people. Lancet Diabetes Endocrinol. 2016, 4, 2–3. [Google Scholar] [CrossRef]
- Prasad, R.B.; Asplund, O.; Shukla, S.R.; Wagh, R.; Kunte, P.; Bhat, D.; Parekh, M.; Shah, M.; Phatak, S.; Käräjämäki, A.; et al. Subgroups of patients with young-onset type 2 diabetes in India reveal insulin deficiency as a major driver. Diabetologia 2022, 65, 65–78. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; An, H.; Ni, K.; Chen, B.; Li, H.; Li, Y.; Sheng, G.; Zhou, C.; Xie, M.; Chen, S.; et al. Glutathione prevents chronic oscillating glucose intake-induced β-cell dedifferentiation and failure. Cell Death Dis. 2019, 10, 321. [Google Scholar] [CrossRef] [PubMed]
- Del Guerra, S.; Lupi, R.; Marselli, L.; Masini, M.; Bugliani, M.; Sbrana, S.; Torri, S.; Pollera, M.; Boggi, U.; Mosca, F.; et al. Functional and molecular defects of pancreatic islets in human type 2 diabetes. Diabetes 2005, 54, 727–735. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inzucchi, S.E.; Bergenstal, R.M.; Buse, J.B.; Diamant, M.; Ferrannini, E.; Nauck, M.; Peters, A.L.; Tsapas, A.; Wender, R.; Matthews, D.R. Management of hyperglycemia in type 2 diabetes: A patient-centered approach: Position statement of the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 2012, 35, 1364–1379. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Biochemical Variables | Control ----------------- Median (25th–75th Percentile) | D ----------- Median (25th–75th Percentile) | DG ---------- Median (25th–75th Percentile) |
|---|---|---|---|
| Age (years) | 39.5 (33.5–49) | 55.5 (47–61) *** | 56 (48–61) *** |
| BMI (kg/m2) | 26.1 (23.5–28.2) | 26.3 (22.7–29.2) | 26.8 (23.8–29.8) |
| HbA1c (%) | 5.6 (5.4–5.8) | 8.1 (7.1–9.6) *** | 8 (7.1–9.7) *** |
| Fasting Glucose (mg/dL) | 90 (85–95) | 147 (120–190) *** | 140.5 (109–182) *** |
| Fasting Insulin (µU/mL) | 9.4 (6.8–12.3) | 11.9 (7.4–17.1) ** | 10.4 (7.5–16.1) * |
| PP Glucose (mg/dL) | 104 (96–117) | 220 (169–285) *** | 209 (168–258) *** |
| PP Insulin (µU/mL) | 36 (18.1–71.7) | 36.2 (24–54.8) | 32.4 (18.1–60.4) |
| GSH (µM) | 801 (548–1068) | 379 (243–533) *** | 440 (176–635) *** |
| GSSG (µM) | 205 (124–303) | 215 (139–326) | 137 (89–209) ***,### |
| 8-OHdG (ng/µg DNA) | 129.97 (97.2–175.2) | 442.33 (340.26–514) *** | 481.71 (412.23–535.11) **,## |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kalamkar, S.; Acharya, J.; Kolappurath Madathil, A.; Gajjar, V.; Divate, U.; Karandikar-Iyer, S.; Goel, P.; Ghaskadbi, S. Randomized Clinical Trial of How Long-Term Glutathione Supplementation Offers Protection from Oxidative Damage and Improves HbA1c in Elderly Type 2 Diabetic Patients. Antioxidants 2022, 11, 1026. https://doi.org/10.3390/antiox11051026
Kalamkar S, Acharya J, Kolappurath Madathil A, Gajjar V, Divate U, Karandikar-Iyer S, Goel P, Ghaskadbi S. Randomized Clinical Trial of How Long-Term Glutathione Supplementation Offers Protection from Oxidative Damage and Improves HbA1c in Elderly Type 2 Diabetic Patients. Antioxidants. 2022; 11(5):1026. https://doi.org/10.3390/antiox11051026
Chicago/Turabian StyleKalamkar, Saurabh, Jhankar Acharya, Arjun Kolappurath Madathil, Vijay Gajjar, Uma Divate, Sucheta Karandikar-Iyer, Pranay Goel, and Saroj Ghaskadbi. 2022. "Randomized Clinical Trial of How Long-Term Glutathione Supplementation Offers Protection from Oxidative Damage and Improves HbA1c in Elderly Type 2 Diabetic Patients" Antioxidants 11, no. 5: 1026. https://doi.org/10.3390/antiox11051026
APA StyleKalamkar, S., Acharya, J., Kolappurath Madathil, A., Gajjar, V., Divate, U., Karandikar-Iyer, S., Goel, P., & Ghaskadbi, S. (2022). Randomized Clinical Trial of How Long-Term Glutathione Supplementation Offers Protection from Oxidative Damage and Improves HbA1c in Elderly Type 2 Diabetic Patients. Antioxidants, 11(5), 1026. https://doi.org/10.3390/antiox11051026