


Association of Serum Antioxidant Minerals and Type 2 Diabetes Mellitus in Chinese Urban Residents

 ,
,  , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Studying Population
2.2. Blood Sample Collection and Elements Analysis
2.3. Measurement of Covariates
2.4. Statistical Analysis
3. Results
3.1. Characteristics of the Participants
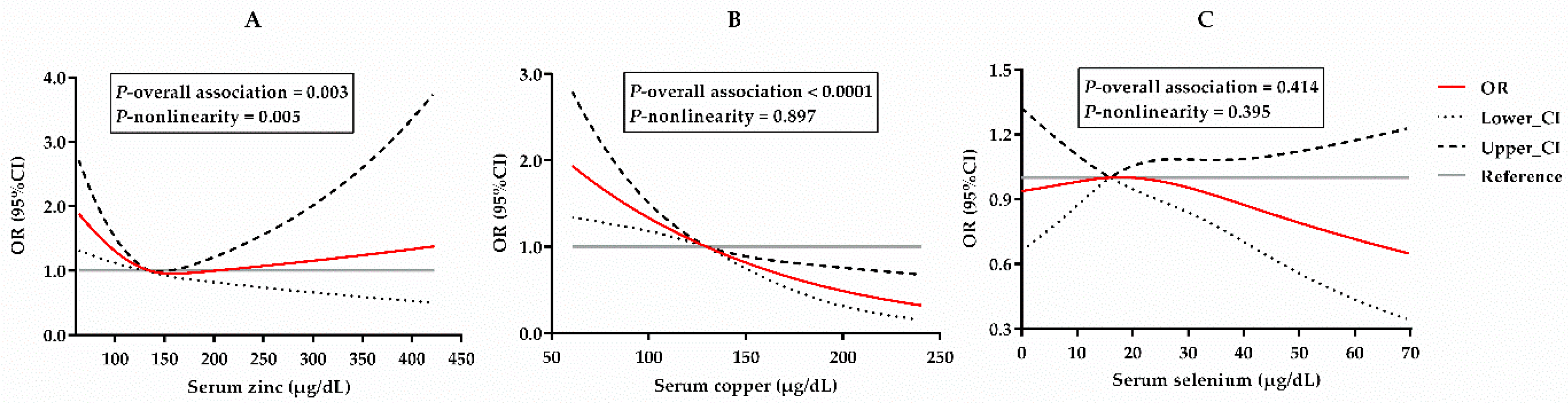
3.2. Independent Associations between Serum Minerals and T2DM
3.3. Subgroup Analysis and Joint Association
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Khan, M.A.B.; Hashim, M.J.; King, J.K.; Govender, R.D.; Mustafa, H.; Kaabi, J.A. Epidemiology of Type 2 Diabetes—Global Burden of Disease and Forecasted Trends. J. Epidemiol. Glob. Health 2019, 10, 107–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lascar, N.; Brown, J.; Pattison, H.; Barnett, A.H.; Bailey, C.J.; Bellary, S. Type 2 Diabetes in Adolescents and Young Adults. Lancet Diabetes Endocrinol. 2018, 6, 69–80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ali, M.K.; Pearson-Stuttard, J.; Selvin, E.; Gregg, E.W. Interpreting Global Trends in Type 2 Diabetes Complications and Mortality. Diabetologia 2022, 65, 3–13. [Google Scholar] [CrossRef]
- Zhang, N.; Du, S.M.; Ma, G.S. Current Lifestyle Factors That Increase Risk of T2DM in China. Eur. J. Clin. Nutr. 2017, 71, 832–838. [Google Scholar] [CrossRef] [PubMed]
- GBD 2017 Diet Collaborators. Health Effects of Dietary Risks in 195 Countries, 1990–2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Lancet 2019, 393, 1958–1972. [Google Scholar] [CrossRef] [Green Version]
- Lichtenstein, A.H.; Appel, L.J.; Vadiveloo, M.; Hu, F.B.; Kris-Etherton, P.M.; Rebholz, C.M.; Sacks, F.M.; Thorndike, A.N.; Horn, L.V.; Wylie-Rosett, J.; et al. 2021 Dietary Guidance to Improve Cardiovascular Health: A Scientific Statement from the American Heart Association. Circulation 2021, 144, e472–e487. [Google Scholar] [CrossRef]
- Forouhi, N.G.; Misra, A.; Mohan, V.; Taylor, R.; Yancy, W. Dietary and Nutritional Approaches for Prevention and Management of Type 2 Diabetes. BMJ 2018, 361, k2234. [Google Scholar] [CrossRef] [Green Version]
- Newsholme, P.; Cruzat, V.F.; Keane, K.N.; Carlessi, R.; de Bittencourt, P.I.H. Molecular Mechanisms of ROS Production and Oxidative Stress in Diabetes. Biochem. J. 2016, 473, 4527–4550. [Google Scholar] [CrossRef]
- Lewandowski, Ł.; Kepinska, M.; Milnerowicz, H. The Copper-zinc Superoxide Dismutase Activity in Selected Diseases. Eur. J. Clin. Invest. 2019, 49, e13036. [Google Scholar] [CrossRef] [Green Version]
- Marjani, A.; Moradi, A.; Saeedi, M. Plasma Lipid Peroxidation Zinc and Erythrocyte Cu-Zn Superoxide Dismutase Enzyme Activity in Patients with Type 2 Diabetes Mellitus in Gorgan City (South East of the Caspian Sea). J. Medical. Sci. 2007, 7, 585–590. [Google Scholar] [CrossRef]
- De Vega, R.G.; Fernández-Sánchez, M.L.; Fernández, J.C.; Menéndez, F.V.Á.; Sanz-Medel, A. Selenium Levels and Glutathione Peroxidase Activity in the Plasma of Patients with Type II Diabetes Mellitus. J. Trace Elem. Med. Bio. 2016, 37, 44–49. [Google Scholar] [CrossRef]
- Pompano, L.M.; Boy, E. Effects of Dose and Duration of Zinc Interventions on Risk Factors for Type 2 Diabetes and Cardiovascular Disease: A Systematic Review and Meta-Analysis. Adv. Nutr. 2020, 12, 141–160. [Google Scholar] [CrossRef] [PubMed]
- Sun, Q.; van Dam, R.M.; Willett, W.C.; Hu, F.B. Prospective Study of Zinc Intake and Risk of Type 2 Diabetes in Women. Diabetes Care 2009, 32, 629–634. [Google Scholar] [CrossRef] [Green Version]
- Lei, X.G.; Zhu, J.-H.; Cheng, W.-H.; Bao, Y.; Ho, Y.-S.; Reddi, A.R.; Holmgren, A.; Arnér, E.S.J. Paradoxical Roles of Antioxidant Enzymes: Basic Mechanisms and Health Implications. Physiol. Rev. 2016, 96, 307–364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lei, X.G.; Combs, G.F., Jr.; Sunde, R.A.; Caton, J.S.; Arthington, J.D.; Vatamaniuk, M.Z. Dietary Selenium Across Species. Annu. Rev. Nutr. 2022, 42, 337–375. [Google Scholar] [CrossRef] [PubMed]
- Stern, B.R.; Solioz, M.; Krewski, D.; Aggett, P.; Aw, T.-C.; Baker, S.; Crump, K.; Dourson, M.; Haber, L.; Hertzberg, R.; et al. Copper and Human Health: Biochemistry, Genetics, and Strategies for Modeling Dose-Response Relationships. J. Toxicol. Environ. Health Part B 2007, 10, 157–222. [Google Scholar] [CrossRef]
- Fan, J.; Zhang, T.; Yu, Y.; Zhang, B. Is Serum Zinc Status Related to Gestational Diabetes Mellitus? A Meta-analysis. Matern. Child Nutr. 2021, 17, e13239. [Google Scholar] [CrossRef]
- Qiu, Q.; Zhang, F.; Zhu, W.; Wu, J.; Liang, M. Copper in Diabetes Mellitus: A Meta-Analysis and Systematic Review of Plasma and Serum Studies. Biol. Trace Elem. Res. 2017, 177, 53–63. [Google Scholar] [CrossRef]
- Kong, F.-J.; Ma, L.-L.; Chen, S.-P.; Li, G.; Zhou, J.-Q. Serum Selenium Level and Gestational Diabetes Mellitus: A Systematic Review and Meta-Analysis. Nutr. J. 2016, 15, 94. [Google Scholar] [CrossRef] [Green Version]
- Xu, H.; Song, Y.; You, N.-C.; Zhang, Z.-F.; Greenland, S.; Ford, E.S.; He, L.; Liu, S. Prevalence and Clustering of Metabolic Risk Factors for Type 2 Diabetes among Chinese Adults in Shanghai, China. BMC Public Health 2010, 10, 683. [Google Scholar] [CrossRef]
- Liu, Y.; Zhou, D.; Zhang, Z.; Song, Y.; Zhang, D.; Zhao, T.; Chen, Z.; Sun, Y.; Zhang, D.; Yang, Y.; et al. Effects of Genetic Variants on Lipid Parameters and Dyslipidemia in a Chinese Population. J. Lipid Res. 2011, 52, 354–360. [Google Scholar] [CrossRef] [Green Version]
- Guo, X.; Zhou, D.; An, P.; Wu, Q.; Wang, H.; Wu, A.; Mu, M.; Zhang, D.; Zhang, Z.; Wang, H.; et al. Associations between Serum Hepcidin, Ferritin and Hb Concentrations and Type 2 Diabetes Risks in a Han Chinese Population. Brit. J. Nutr. 2013, 110, 2180–2185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alberti, K.G.M.M.; Zimmet, P.Z.; Consultation, W. Definition, Diagnosis and Classification of Diabetes Mellitus and Its Complications. Part 1: Diagnosis and Classification of Diabetes Mellitus. Provisional Report of a WHO Consultation. Diabet. Med. 1998, 15, 539–553. [Google Scholar] [CrossRef]
- Sun, L.; Yu, Y.; Huang, T.; An, P.; Yu, D.; Yu, Z.; Li, H.; Sheng, H.; Cai, L.; Xue, J.; et al. Associations between Ionomic Profile and Metabolic Abnormalities in Human Population. PLoS ONE 2012, 7, e38845. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huth, C.; Beuerle, S.; Zierer, A.; Heier, M.; Herder, C.; Kaiser, T.; Koenig, W.; Kronenberg, F.; Oexle, K.; Rathmann, W.; et al. Biomarkers of iron metabolism are independently associated with impaired glucose metabolism and type 2 diabetes: The KORA F4 study. Eur. J. Endocrinol. 2015, 173, 643–653. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Podmore, C.; Meidtner, K.; Schulze, M.B.; Scott, R.A.; Ramond, A.; Butterworth, A.S.; Di Angelantonio, E.; Danesh, J.; Arriola, L.; Barricarte, A.; et al. Association of Multiple Biomarkers of Iron Metabolism and Type 2 Diabetes: The EPIC-InterAct Study. Diabetes Care 2016, 39, 572–581. [Google Scholar] [CrossRef] [Green Version]
- Orban, E.; Schwab, S.; Thorand, B.; Huth, C. Association of iron indices and type 2 diabetes: A meta-analysis of observational studies. Diabetes-Metab. Res. Rev. 2014, 30, 372–394. [Google Scholar] [CrossRef]
- Liu, J.; Li, Q.; Yang, Y.; Ma, L. Iron metabolism and type 2 diabetes mellitus: A meta-analysis and systematic review. J. Diabetes Investig. 2020, 11, 946–955. [Google Scholar] [CrossRef]
- Desquilbet, L.; Mariotti, F. Dose-response Analyses Using Restricted Cubic Spline Functions in Public Health Research. Stat. Med. 2010, 29, 1037–1057. [Google Scholar] [CrossRef]
- Zhang, P.; Li, T.; Wu, X.; Nice, E.C.; Huang, C.; Zhang, Y. Oxidative Stress and Diabetes: Antioxidative Strategies. Front. Med. 2020, 14, 583–600. [Google Scholar] [CrossRef]
- Beckman, J.A.; Paneni, F.; Cosentino, F.; Creager, M.A. Diabetes and Vascular Disease: Pathophysiology, Clinical Consequences, and Medical Therapy: Part II. Eur. Heart J. 2013, 34, 2444–2452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pelmenschikov, V.; Siegbahn, P.E.M. Copper−Zinc Superoxide Dismutase: Theoretical Insights into the Catalytic Mechanism. Inorg. Chem. 2005, 44, 3311–3320. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Zhao, L.; Man, Q.; Wang, J.; Zhao, W.; Zhang, J. Dietary Micronutrients Intake Status among Chinese Elderly People Living at Home: Data from CNNHS 2010–2012. Nutrients 2019, 11, 1787. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, J.; Hu, Y.; Li, M.; Liu, X.; Wang, R.; Mao, D.; Yang, X.; Yang, L. Zinc Nutritional Status and Risk Factors of Elderly in the China Adult Chronic Disease and Nutrition Surveillance 2015. Nutrients 2021, 13, 3086. [Google Scholar] [CrossRef]
- Murphy, E.W.; Willis, B.W.; Watt, B.K. Provisional Tables on the Zinc Content of Foods. J. Am. Diet. Assoc. 1975, 66, 345–355. [Google Scholar] [CrossRef]
- Eshak, E.S.; Iso, H.; Maruyama, K.; Muraki, I.; Tamakoshi, A. Associations between Dietary Intakes of Iron, Copper and Zinc with Risk of Type 2 Diabetes Mellitus: A Large Population-Based Prospective Cohort Study. Clin. Nutr. 2018, 37, 667–674. [Google Scholar] [CrossRef] [Green Version]
- Yuan, Y.; Xiao, Y.; Yu, Y.; Liu, Y.; Feng, W.; Qiu, G.; Wang, H.; Liu, B.; Wang, J.; Zhou, L.; et al. Associations of Multiple Plasma Metals with Incident Type 2 Diabetes in Chinese Adults: The Dongfeng-Tongji Cohort. Environ. Pollut. 2018, 237, 917–925. [Google Scholar] [CrossRef]
- Li, X.T.; Yu, P.F.; Gao, Y.; Guo, W.H.; Wang, J.; Liu, X.; Gu, A.H.; Ji, G.X.; Dong, Q.; Wang, B.S.; et al. Association between Plasma Metal Levels and Diabetes Risk: A Case-Control Study in China. Biomed. Environ. Sci. 2017, 30, 482–491. [Google Scholar]
- Zhang, H.; Yan, C.; Yang, Z.; Zhang, W.; Niu, Y.; Li, X.; Qin, L.; Su, Q. Alterations of Serum Trace Elements in Patients with Type 2 Diabetes. J. Trace Elem. Med. Bio. 2017, 40, 91–96. [Google Scholar] [CrossRef]
- Shan, Z.; Bao, W.; Zhang, Y.; Rong, Y.; Wang, X.; Jin, Y.; Song, Y.; Yao, P.; Sun, C.; Hu, F.B.; et al. Interactions between Zinc Transporter-8 Gene (SLC30A8) and Plasma Zinc Concentrations for Impaired Glucose Regulation and Type 2 Diabetes. Diabetes 2013, 63, 1796–1803. [Google Scholar] [CrossRef] [Green Version]
- Cui, Z.; Zhou, H.; Liu, K.; Wu, M.; Li, S.; Meng, S.; Meng, H. Dietary Copper and Selenium Intakes and the Risk of Type 2 Diabetes Mellitus: Findings from the China Health and Nutrition Survey. Nutrients 2022, 14, 2055. [Google Scholar] [CrossRef] [PubMed]
- Cui, Z.; Chen, H.; Lu, W.; Wang, P.; Zhou, Z.; Zhang, N.; Wang, Z.; Lin, T.; Song, Y.; Liu, L.; et al. The Association Between Plasma Copper Concentration and Prevalence of Diabetes in Chinese Adults With Hypertension. Front. Public Health 2022, 10, 888219. [Google Scholar] [CrossRef]
- Zhang, Z.; Zhao, S.; Wu, H.; Qin, W.; Zhang, T.; Wang, Y.; Tang, Y.; Qi, S.; Cao, Y.; Gao, X. Cross-Sectional Study: Relationship between Serum Trace Elements and Hypertension. J. Trace Elem. Med. Bio. 2022, 69, 126893. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Wang, D.; Ouyang, Y.; Huang, F.; Ding, G.; Zhang, B. Do Chinese Children Get Enough Micronutrients? Nutrients 2017, 9, 397. [Google Scholar] [CrossRef] [Green Version]
- Siddiqi, S.M.; Sun, C.; Wu, X.; Shah, I.; Mehmood, A. The Correlation between Dietary Selenium Intake and Type 2 Diabetes: A Cross-Sectional Population-Based Study on North Chinese Adults. Biomed. Res. Int. 2020, 2020, 8058463. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.; Shen, T. Association of Dietary and Serum Selenium Concentrations with Glucose Level and Risk of Diabetes Mellitus: A Cross Sectional Study of National Health and Nutrition Examination Survey, 1999–2006. J. Trace Elem. Med. Bio. 2021, 63, 126660. [Google Scholar] [CrossRef]
- Lv, Y.; Xie, L.; Dong, C.; Yang, R.; Long, T.; Yang, H.; Chen, L.; Zhang, L.; Chen, X.; Luo, X.; et al. Co-Exposure of Serum Calcium, Selenium and Vanadium Is Nonlinearly Associated with Increased Risk of Type 2 Diabetes Mellitus in a Chinese Population. Chemosphere 2021, 263, 128021. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Total (n = 1443) | Non-T2DM (n = 962) | T2DM (n = 481) | P | |
|---|---|---|---|---|
| Age, years | 60.8 ± 8.3 | 60.8 ± 8.2 | 60.9 ± 8.3 | — |
| Gender | — | |||
| Men | 573 (39.7) | 382 (39.7) | 191 (39.7) | |
| Women | 870 (60.3) | 580 (60.3) | 290 (60.3) | |
| Height, cm | 160.4 ± 7.9 | 159.9 ± 7.9 | 161.5 ± 7.7 | 0.0002 |
| Weight, kg | 63.3 ± 9.9 | 62.4 ± 9.7 | 65.0 ± 10.0 | <0.0001 |
| BMI, kg/m2 | 24.6 ± 3.2 | 24.4 ± 3.2 | 24.9 ± 3.3 | 0.005 |
| Waist circumference, cm | 83.7 ± 10.6 | 82.4 ± 10.8 | 86.4 ± 9.7 | <0.0001 |
| Hip circumference, cm | 96.7 ± 10.1 | 96.5 ± 11.2 | 97.1 ± 7.6 | 0.239 |
| Systolic blood pressure, mmHg | 135.4 ± 19.7 | 132.8 ± 17.8 | 140.4 ± 22.2 | <0.0001 |
| Diastolic blood pressure, mmHg | 81.0 ± 9.8 | 81.0 ± 9.5 | 81.1 ± 10.4 | 0.858 |
| Fasting blood glucose, mmol/L | 5.9 ± 2.5 | 4.7 ± 0.6 | 8.4 ± 2.9 | <0.0001 |
| HDL-C, mmol/L | 1.3 ± 0.3 | 1.3 ± 0.3 | 1.2 ± 0.3 | <0.0001 |
| LDL-C, mmol/L | 2.7 ± 0.7 | 2.7 ± 0.6 | 2.7 ± 0.7 | 0.860 |
| Total cholesterol, mmol/L | 4.8 ± 1.0 | 4.9 ± 0.9 | 4.6 ± 1.1 | <0.0001 |
| Triglycerides, mmol/L | 1.4 (1.0, 2.1) | 1.4 (0.9, 2.0) | 1.6 (1.1, 2.3) | <0.0001 |
| Zinc, μg/dL | 140.2 ± 57.6 | 147.7 ± 60.6 | 125.2 ± 47.6 | <0.0001 |
| Copper, μg/dL | 130.7 ± 41.2 | 139.5 ± 40.7 | 113.2 ± 36.2 | <0.0001 |
| Selenium, μg/dL | 16.1 (11.9, 22.6) | 17.6 (12.5, 23.9) | 13.8 (11.3, 19.5) | <0.0001 |
| Iron, μg/dL | 548.4 (410.3, 767.7) | 538.1 (404.1, 717.1) | 576.7 (428.4, 910.9) | 0.001 |
| T2DM, OR (95%CI) | ||||||
|---|---|---|---|---|---|---|
| Serum Minerals | n | Median | Cases (%) | Crude Model | Adjust Model 1 | Adjust Model 2 |
| Zinc, μg/dL | ||||||
| As categorical variable (3 groups) | ||||||
| Tertile 1 (<116.9) | 481 | 96.6 | 244 (50.7) | 1 (reference) | 1 (reference) | 1 (reference) |
| Tertile 2 (116.9 to 151.3) | 481 | 135 | 130 (27.0) | 0.34 (0.26, 0.46) | 0.39 (0.28, 0.52) | 0.54 (0.39, 0.77) |
| Tertile 3 (≥151.3) | 481 | 172.8 | 107 (22.3) | 0.26 (0.19, 0.35) | 0.28 (0.20, 0.39) | 0.52 (0.35, 0.77) |
| P-trend | <0.0001 | <0.0001 | 0.001 | |||
| As categorical variable (2 groups) | ||||||
| Low (<135.0) | 721 | 107.6 | 321 (44.5) | 1 (reference) | 1 (reference) | 1 (reference) |
| High (≥135.0) | 722 | 161.2 | 160 (22.2) | 0.34 (0.27, 0.43) | 0.36 (0.28, 0.47) | 0.61 (0.44, 0.83) |
| P | <0.0001 | <0.0001 | 0.0016 | |||
| Copper, μg/dL | ||||||
| As categorical variable (3 groups) | ||||||
| Tertile 1 (<106.5) | 481 | 88.5 | 256 (53.2) | 1 (reference) | 1 (reference) | 1 (reference) |
| Tertile 2 (106.5 to <149.8) | 481 | 129.9 | 143 (29.7) | 0.41 (0.30, 0.56) | 0.40 (0.29, 0.54) | 0.45 (0.32, 0.63) |
| Tertile 3 (≥149.8) | 481 | 169.8 | 82 (17.1) | 0.19 (0.14, 0.28) | 0.23 (0.16, 0.33) | 0.25 (0.17, 0.37) |
| P-trend | <0.0001 | <0.0001 | <0.0001 | |||
| As categorical variable (2 groups) | ||||||
| Low (<129.9) | 721 | 96.2 | 350 (48.5) | 1 (reference) | 1 (reference) | 1 (reference) |
| High (≥129.9) | 722 | 159.6 | 131 (18.1) | 0.22 (0.17, 0.28) | 0.25 (0.18, 0.33) | 0.32 (0.24, 0.44) |
| P | <0.0001 | <0.0001 | <0.0001 | |||
| Selenium, μg/dL | ||||||
| As categorical variable (3 groups) | ||||||
| Tertile 1 (<13.2) | 481 | 10.5 | 213 (44.3) | 1 (reference) | 1 (reference) | 1 (reference) |
| Tertile 2 (13.2 to <20.1) | 481 | 16.1 | 157 (32.6) | 0.61 (0.47, 0.79) | 0.65 (0.49, 0.86) | 0.87 (0.63, 1.20) |
| Tertile 3 (≥20.1) | 481 | 28.3 | 111 (23.1) | 0.37 (0.28, 0.49) | 0.46 (0.34, 0.62) | 0.78 (0.55, 1.10) |
| P-trend | <0.0001 | <0.0001 | 0.252 | |||
| As categorical variable (2 groups) | ||||||
| Low (<16.1) | 721 | 11.9 | 308 (42.7) | 1 (reference) | 1 (reference) | 1 (reference) |
| High (≥16.1) | 722 | 22.6 | 173 (24.0) | 0.41 (0.32, 0.51) | 0.48 (0.38, 0.62) | 0.78 (0.58, 1.04) |
| P | <0.0001 | <0.0001 | 0.089 | |||
| Zinc as a Binary Variable | Copper as a Binary Variable | Selenium as a Binary Variable | |||||
|---|---|---|---|---|---|---|---|
| Subgroups | n (%) | OR (95% CI) | P-Interaction | OR (95% CI) | P-Interaction | OR (95% CI) | P-Interaction |
| Age, years | |||||||
| <60 | 612 (42.4) | 0.65 (0.41, 1.03) | 0.027 | 0.49 (0.31, 0.77) | 0.002 | 0.68 (0.45, 1.02) | 0.723 |
| ≥60 | 831 (57.6) | 0.52 (0.33, 0.81) | 0.24 (0.15, 0.37) | 0.97 (0.63, 1.5) | |||
| Gender | |||||||
| Men | 573 (39.7) | 0.75 (0.45, 1.24) | 0.910 | 0.33 (0.2, 0.54) | 0.788 | 0.83 (0.5, 1.38) | 0.879 |
| Women | 870 (60.3) | 0.54 (0.36, 0.81) | 0.31 (0.21, 0.47) | 0.72 (0.5, 1.04) | |||
| BMI, kg/m2 | |||||||
| <24 | 642 (44.5) | 0.52 (0.24, 1.13) | 0.464 | 0.13 (0.06, 0.31) | 0.003 | 0.96 (0.47, 1.95) | 0.152 |
| ≥24 | 801 (55.5) | 0.47 (0.28, 0.79) | 0.58 (0.36, 0.93) | 0.81 (0.5, 1.31) | |||
| Hypertension | |||||||
| No | 749 (51.9) | 0.82 (0.45, 1.48) | 0.162 | 0.57 (0.33, 1.01) | 0.001 | 0.61 (0.35, 1.07) | 0.969 |
| Yes | 694 (48.1) | 0.69 (0.38, 1.24) | 0.10 (0.05, 0.23) | 1.05 (0.61, 1.82) | |||
| Copper, μg/dL | |||||||
| <129.9 | 721 (50.0) | 0.46 (0.27, 0.78) | 0.030 | - | - | 0.44 (0.26, 0.76) | 0.001 |
| ≥129.9 | 722 (50.0) | 0.57 (0.29, 1.10) | - | 1.07 (0.56, 2.07) | |||
| Zinc, μg/dL | |||||||
| <135.0 | 721 (50.0) | - | - | 0.15 (0.07, 0.31) | 0.030 | 0.67 (0.38, 1.18) | 0.152 |
| ≥135.0 | 722 (50.0) | - | 0.43 (0.24, 0.77) | 0.82 (0.44, 1.51) | |||
| Selenium, μg/dL | |||||||
| <16.1 | 721 (50.0) | 0.71 (0.39, 1.28) | 0.152 | 0.16 (0.08, 0.34) | 0.001 | - | - |
| ≥16.1 | 722 (50.0) | 0.51 (0.28, 0.93) | 0.56 (0.31, 0.99) | - | |||
| T2DM, OR (95% CI) | ||||||
|---|---|---|---|---|---|---|
| Combined Variables | n | Cases (%) | Crude Model | Adjust Model 1 | Adjust Model 2 | |
| Copper, μg/dL | Zinc, μg/dL | |||||
| ≥129.9 | ≥135.0 | 544 | 97 (17.8) | 1 (reference) | 1 (reference) | 1 (reference) |
| ≥129.9 | <135.0 | 178 | 34 (19.1) | 1.01 (0.64, 1.60) | 1.14 (0.71, 1.84) | 1.08 (0.67, 1.76) |
| <129.9 | ≥135.0 | 178 | 63 (35.4) | 2.59 (1.74, 3.84) | 2.35 (1.54, 3.58) | 2.18 (1.42, 3.36) |
| <129.9 | <135.0 | 543 | 287 (52.9) | 5.72 (4.20, 7.80) | 5.16 (3.69, 7.21) | 4.77 (3.35, 6.79) |
| P-trend | <0.0001 | <0.0001 | <0.0001 | |||
| Copper, μg/dL | Selenium, μg/dL | |||||
| ≥129.9 | ≥16.1 | 504 | 95 (18.9) | 1 (reference) | 1 (reference) | 1 (reference) |
| ≥129.9 | <16.1 | 218 | 36 (16.5) | 0.80 (0.52, 1.25) | 0.75 (0.48, 1.19) | 0.65 (0.41, 1.05) |
| <129.9 | ≥16.1 | 218 | 78 (35.8) | 2.38 (1.63, 3.47) | 2.25 (1.51, 3.37) | 1.86 (1.23, 2.82) |
| <129.9 | <16.1 | 503 | 272 (54.1) | 5.89 (4.26, 8.13) | 4.77 (3.38, 6.75) | 3.70 (2.54, 5.38) |
| P-trend | <0.0001 | <0.0001 | <0.0001 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
He, J.; Chen, F.; Wan, S.; Luo, Y.; Luo, J.; He, S.; Zhou, D.; An, P.; Zeng, P. Association of Serum Antioxidant Minerals and Type 2 Diabetes Mellitus in Chinese Urban Residents. Antioxidants 2023, 12, 62. https://doi.org/10.3390/antiox12010062
He J, Chen F, Wan S, Luo Y, Luo J, He S, Zhou D, An P, Zeng P. Association of Serum Antioxidant Minerals and Type 2 Diabetes Mellitus in Chinese Urban Residents. Antioxidants. 2023; 12(1):62. https://doi.org/10.3390/antiox12010062
Chicago/Turabian StyleHe, Jingjing, Fangyan Chen, Sitong Wan, Yongting Luo, Junjie Luo, Shuli He, Daizhan Zhou, Peng An, and Ping Zeng. 2023. "Association of Serum Antioxidant Minerals and Type 2 Diabetes Mellitus in Chinese Urban Residents" Antioxidants 12, no. 1: 62. https://doi.org/10.3390/antiox12010062
APA StyleHe, J., Chen, F., Wan, S., Luo, Y., Luo, J., He, S., Zhou, D., An, P., & Zeng, P. (2023). Association of Serum Antioxidant Minerals and Type 2 Diabetes Mellitus in Chinese Urban Residents. Antioxidants, 12(1), 62. https://doi.org/10.3390/antiox12010062