
Oxidative Balance Score and New-Onset Type 2 Diabetes Mellitus in Korean Adults without Non-Alcoholic Fatty Liver Disease: Korean Genome and Epidemiology Study-Health Examinees (KoGES-HEXA) Cohort

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
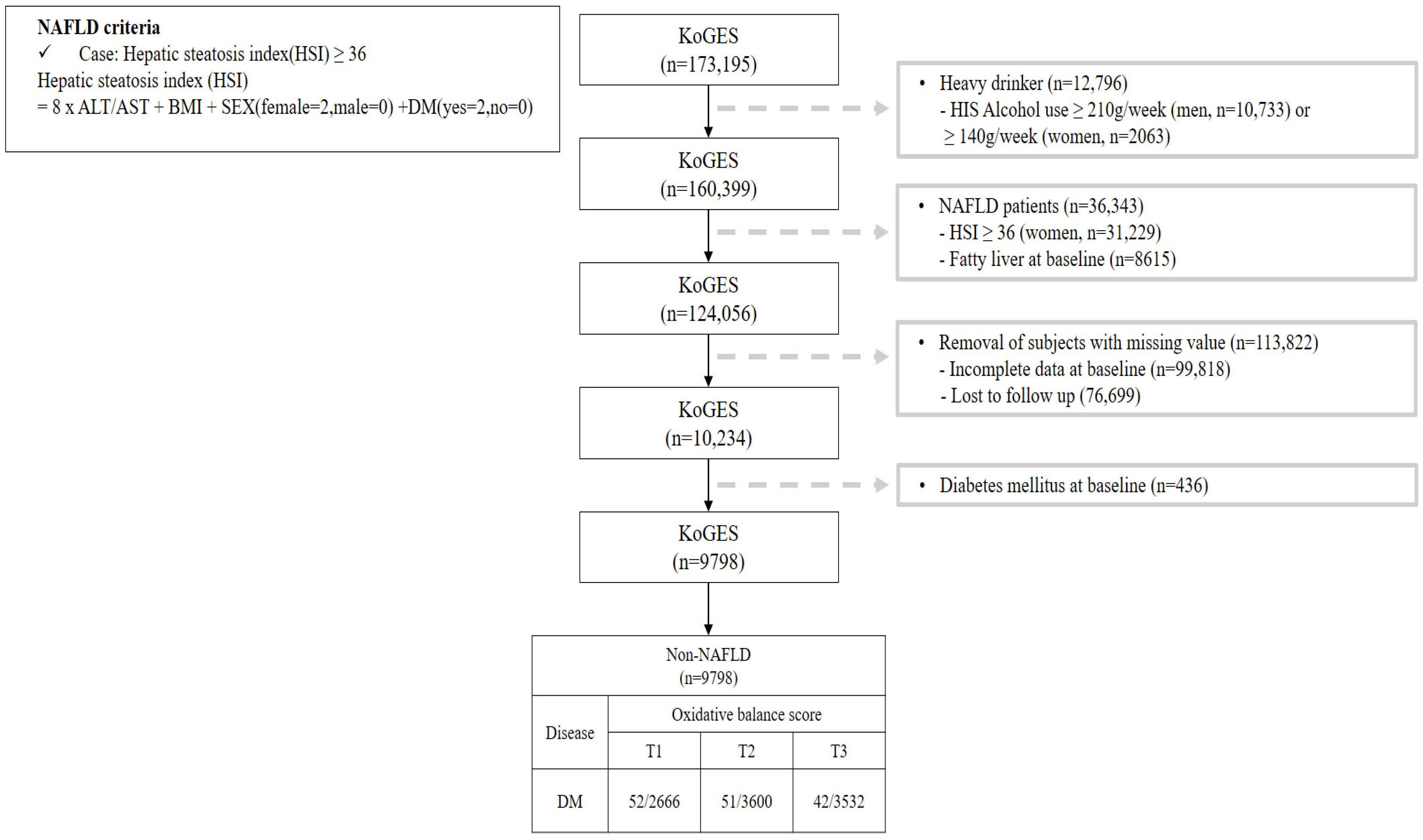
2.1. Study Design and Participants
2.2. Data Collection and Covariates
2.3. Assessment of Oxidative Balance Scores
2.4. Study Outcomes
2.5. Statistical Analysis
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sun, H.; Saeedi, P.; Karuranga, S.; Pinkepank, M.; Ogurtsova, K.; Duncan, B.B.; Stein, C.; Basit, A.; Chan, J.C.; Mbanya, J.C. IDF Diabetes Atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res. Clin. Pract. 2022, 183, 109119. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.A.; Kim, D.J.; Han, K.; Chon, S.; Moon, M.K. Screening for Prediabetes and Diabetes in Korean Nonpregnant Adults: A Position Statement of the Korean Diabetes Association, 2022. Diabetes Metab. J. 2022, 46, 819–826. [Google Scholar] [CrossRef] [PubMed]
- Cousin, E.; Schmidt, M.I.; Ong, K.L.; Lozano, R.; Afshin, A.; Abushouk, A.I.; Agarwal, G.; Agudelo-Botero, M.; Al-Aly, Z.; Alcalde-Rabanal, J.E. Burden of diabetes and hyperglycaemia in adults in the Americas, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Diabetes Endocrinol. 2022, 10, 655–667. [Google Scholar] [CrossRef] [PubMed]
- Sies, H. Oxidative stress: A concept in redox biology and medicine. Redox Biol. 2015, 4, 180–183. [Google Scholar] [CrossRef]
- Lee, J.-H.; Son, D.-H.; Kwon, Y.-J. Association between oxidative balance score and new-onset hypertension in adults: A community-based prospective cohort study. Front. Nutr. 2022, 9, 1066159. [Google Scholar] [CrossRef] [PubMed]
- Sohouli, M.H.; Rohani, P.; Hosseinzadeh, M.; Hekmatdoost, A. Adherence to oxidative balance scores and lower odds of non-alcoholic fatty liver disease: A case–control study. Sci. Rep. 2023, 13, 6140. [Google Scholar] [CrossRef]
- Son, D.-H.; Lee, H.S.; Seol, S.-Y.; Lee, Y.-J.; Lee, J.-H. Association between the oxidative balance score and incident chronic kidney disease in adults. Antioxidants 2023, 12, 335. [Google Scholar] [CrossRef]
- Kwon, Y.-J.; Park, H.-M.; Lee, J.-H. Inverse Association between Oxidative Balance Score and Incident Type 2 Diabetes Mellitus. Nutrients 2023, 15, 2497. [Google Scholar] [CrossRef]
- Golmohammadi, M.; Ayremlou, P.; Zarrin, R. Higher oxidative balance score is associated with better glycemic control among Iranian adults with type-2 diabetes. Int. J. Vitam. Nutr. Res. 2019, 91, 31–39. [Google Scholar] [CrossRef]
- Wu, C.; Ren, C.; Song, Y.; Gao, H.; Pang, X.; Zhang, L. Gender-specific effects of oxidative balance score on the prevalence of diabetes in the US population from NHANES. Front. Endocrinol. 2023, 14, 1148417. [Google Scholar] [CrossRef]
- Targher, G.; Tilg, H.; Byrne, C.D. Non-alcoholic fatty liver disease: A multisystem disease requiring a multidisciplinary and holistic approach. Lancet Gastroenterol. Hepatol. 2021, 6, 578–588. [Google Scholar] [CrossRef] [PubMed]
- Park, J.I.; Kim, S.W.; Nam-Goong, I.S.; Song, K.H.; Yu, J.H.; Jeong, J.Y.; Cho, E.H. Questionnaire-Based Survey of Diabetes Self-Care Activities and Barriers among Young Korean Adults with Early-Onset Diabetes. Yonsei Med. J. 2024, 65, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Bril, F.; Cusi, K. Nonalcoholic fatty liver disease: The new complication of type 2 diabetes mellitus. Endocrinol. Metab. Clin. 2016, 45, 765–781. [Google Scholar] [CrossRef]
- Tanase, D.M.; Gosav, E.M.; Costea, C.F.; Ciocoiu, M.; Lacatusu, C.M.; Maranduca, M.A.; Ouatu, A.; Floria, M. The intricate relationship between type 2 diabetes mellitus (T2DM), insulin resistance (IR), and nonalcoholic fatty liver disease (NAFLD). J. Diabetes Res. 2020, 2020, 3920196. [Google Scholar] [CrossRef] [PubMed]
- Valenti, L.; Bugianesi, E.; Pajvani, U.; Targher, G. Nonalcoholic fatty liver disease: Cause or consequence of type 2 diabetes? Liver Int. 2016, 36, 1563–1579. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Han, B.-G.; Group, K. Cohort profile: The Korean genome and epidemiology study (KoGES) consortium. Int. J. Epidemiol. 2017, 46, e20. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.-H.; Kim, D.; Kim, H.J.; Lee, C.-H.; Yang, J.I.; Kim, W.; Kim, Y.J.; Yoon, J.-H.; Cho, S.-H.; Sung, M.-W. Hepatic steatosis index: A simple screening tool reflecting nonalcoholic fatty liver disease. Dig. Liver Dis. 2010, 42, 503–508. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.H.; Sohn, W.; Cho, Y.K. The effect of moderate alcohol drinking in nonalcoholic fatty liver disease. Clin. Mol. Hepatol. 2020, 26, 662. [Google Scholar] [CrossRef]
- Lee, H.-Y.; Shin, J.; Kim, G.-H.; Park, S.; Ihm, S.-H.; Kim, H.C.; Kim, K.-i.; Kim, J.H.; Lee, J.H.; Park, J.-M. 2018 Korean Society of Hypertension Guidelines for the management of hypertension: Part II-diagnosis and treatment of hypertension. Clin. Hypertens. 2019, 25, 20. [Google Scholar] [CrossRef]
- Miller, W.G.; Kaufman, H.W.; Levey, A.S.; Straseski, J.A.; Wilhelms, K.W.; Yu, H.Y.; Klutts, J.S.; Hilborne, L.H.; Horowitz, G.L.; Lieske, J. National Kidney Foundation Laboratory Engagement Working Group recommendations for implementing the CKD-EPI 2021 race-free equations for estimated glomerular filtration rate: Practical guidance for clinical laboratories. Clin. Chem. 2022, 68, 511–520. [Google Scholar] [CrossRef]
- Jin, E.-S.; Shim, J.-S.; Kim, S.E.; Bae, J.H.; Kang, S.; Won, J.C.; Shin, M.-J.; Jin, H.Y.; Moon, J.; Lee, H. Dyslipidemia Fact Sheet in South Korea, 2022. Diabetes Metab. J. 2023, 47, 632–642. [Google Scholar] [CrossRef] [PubMed]
- Ahn, Y.; Kwon, E.; Shim, J.; Park, M.; Joo, Y.; Kimm, K.; Park, C.; Kim, D. Validation and reproducibility of food frequency questionnaire for Korean genome epidemiologic study. Eur. J. Clin. Nutr. 2007, 61, 1435–1441. [Google Scholar] [CrossRef] [PubMed]
- ElSayed, N.A.; Aleppo, G.; Aroda, V.R.; Bannuru, R.R.; Brown, F.M.; Bruemmer, D.; Collins, B.S.; Gaglia, J.L.; Hilliard, M.E.; Isaacs, D. 2. Classification and diagnosis of diabetes: Standards of care in diabetes—2023. Diabetes Care 2023, 46, S19–S40. [Google Scholar] [CrossRef]
- Bellary, S.; Kyrou, I.; Brown, J.E.; Bailey, C.J. Type 2 diabetes mellitus in older adults: Clinical considerations and management. Nat. Rev. Endocrinol. 2021, 17, 534–548. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, A.; Petracca, G.; Beatrice, G.; Tilg, H.; Byrne, C.D.; Targher, G. Non-alcoholic fatty liver disease and risk of incident diabetes mellitus: An updated meta-analysis of 501 022 adult individuals. Gut 2021, 70, 962–969. [Google Scholar] [CrossRef]
- Meex, R.C.; Watt, M.J. Hepatokines: Linking nonalcoholic fatty liver disease and insulin resistance. Nat. Rev. Endocrinol. 2017, 13, 509–520. [Google Scholar] [CrossRef]
- Van Hoydonck, P.G.; Temme, E.H.; Schouten, E.G. A dietary oxidative balance score of vitamin C, β-carotene and iron intakes and mortality risk in male smoking Belgians. J. Nutr. 2002, 132, 756–761. [Google Scholar] [CrossRef]
- Hernández-Ruiz, Á.; García-Villanova, B.; Guerra-Hernández, E.; Amiano, P.; Ruiz-Canela, M.; Molina-Montes, E. A review of a priori defined oxidative balance scores relative to their components and impact on health outcomes. Nutrients 2019, 11, 774. [Google Scholar] [CrossRef]
- Kong, S.Y.J.; Bostick, R.M.; Flanders, W.D.; McClellan, W.M.; Thyagarajan, B.; Gross, M.D.; Judd, S.; Goodman, M. Oxidative balance score, colorectal adenoma, and markers of oxidative stress and inflammation. Cancer Epidemiol. Biomark. Prev. 2014, 23, 545–554. [Google Scholar] [CrossRef]
- Cho, A.-R.; Kwon, Y.-J.; Lim, H.-J.; Lee, H.S.; Kim, S.; Shim, J.-Y.; Lee, H.-R.; Lee, Y.-J. Oxidative balance score and serum γ-glutamyltransferase level among Korean adults: A nationwide population-based study. Eur. J. Nutr. 2018, 57, 1237–1244. [Google Scholar] [CrossRef]
- Cho, A.-R.; Kwon, Y.-J.; Lee, J.-H. Oxidative balance score is inversely associated with the incidence of non-alcoholic fatty liver disease. Clin. Nutr. 2023, 42, 1292–1300. [Google Scholar] [CrossRef] [PubMed]
- Pan, A.; Wang, Y.; Talaei, M.; Hu, F.B.; Wu, T. Relation of active, passive, and quitting smoking with incident type 2 diabetes: A systematic review and meta-analysis. Lancet Diabetes Endocrinol. 2015, 3, 958–967. [Google Scholar] [CrossRef] [PubMed]
- Carbone, S.; Del Buono, M.G.; Ozemek, C.; Lavie, C.J. Obesity, risk of diabetes and role of physical activity, exercise training and cardiorespiratory fitness. Prog. Cardiovasc. Dis. 2019, 62, 327–333. [Google Scholar] [CrossRef] [PubMed]
- Emdin, S.; Dodson, G.; Cutfield, J.; Cutfield, S. Role of zinc in insulin biosynthesis: Some possible zinc-insulin interactions in the pancreatic B-cell. Diabetologia 1980, 19, 174–182. [Google Scholar] [CrossRef] [PubMed]
- Seo, J.-A.; Song, S.-W.; Han, K.; Lee, K.-J.; Kim, H.-N. The associations between serum zinc levels and metabolic syndrome in the Korean population: Findings from the 2010 Korean National Health and Nutrition Examination Survey. PLoS ONE 2014, 9, e105990. [Google Scholar] [CrossRef]
- Ruz, M.; Carrasco, F.; Rojas, P.; Basfi-Fer, K.; Hernández, M.C.; Pérez, A. Nutritional effects of zinc on metabolic syndrome and type 2 diabetes: Mechanisms and main findings in human studies. Biol. Trace Elem. Res. 2019, 188, 177–188. [Google Scholar] [CrossRef]
- Institute of Medicine (US) Panel on Micronutrients. Dietary Reference Intakes for Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc; National Academies Press (US): Washington, DC, USA, 2001.
- Thomas, M.S.; Calle, M.; Fernandez, M.L. Healthy plant-based diets improve dyslipidemias, insulin resistance, and inflammation in metabolic syndrome. A narrative review. Adv. Nutr. 2023, 14, 44–54. [Google Scholar] [CrossRef] [PubMed]
- Chow, L.S.; Gerszten, R.E.; Taylor, J.M.; Pedersen, B.K.; Van Praag, H.; Trappe, S.; Febbraio, M.A.; Galis, Z.S.; Gao, Y.; Haus, J.M. Exerkines in health, resilience and disease. Nat. Rev. Endocrinol. 2022, 18, 273–289. [Google Scholar] [CrossRef]
- Jo, H.; Kim, J.-Y.; Jung, M.-Y.; Ahn, Y.-S.; Chang, S.-J.; Koh, S.-B. Leisure time physical activity to reduce metabolic syndrome risk: A 10-year community-based prospective study in Korea. Yonsei Med. J. 2020, 61, 218–228. [Google Scholar] [CrossRef]
- Khan, T.A.; Field, D.; Chen, V.; Ahmad, S.; Mejia, S.B.; Kahleová, H.; Rahelić, D.; Salas-Salvadó, J.; Leiter, L.A.; Uusitupa, M. Combination of multiple low-risk lifestyle behaviors and incident type 2 diabetes: A systematic review and dose-response meta-analysis of prospective cohort studies. Diabetes Care 2023, 46, 643–656. [Google Scholar] [CrossRef]
- Seo, D.H.; Suh, Y.J.; Cho, Y.; Ahn, S.H.; Seo, S.; Hong, S.; Lee, Y.H.; Choi, Y.J.; Lee, E.; Kim, S.H. Effect of Dapagliflozin in Combination with Lobeglitazone and Metformin in Korean Patients with Type 2 Diabetes in Real-World Clinical Practice. Yonsei Med. J. 2022, 63, 825–833. [Google Scholar] [CrossRef] [PubMed]
- Ando, Y.; Jou, J.H. Nonalcoholic fatty liver disease and recent guideline updates. Clin. Liver Dis. 2021, 17, 23. [Google Scholar] [CrossRef] [PubMed]
- Lakkur, S.; Goodman, M.; Bostick, R.M.; Citronberg, J.; McClellan, W.; Flanders, W.D.; Judd, S.; Stevens, V.L. Oxidative balance score and risk for incident prostate cancer in a prospective US cohort study. Ann. Epidemiol. 2014, 24, 475–478.e4. [Google Scholar] [CrossRef] [PubMed]
- Dash, C.; Goodman, M.; Flanders, W.D.; Mink, P.J.; McCullough, M.L.; Bostick, R.M. Using pathway-specific comprehensive exposure scores in epidemiology: Application to oxidative balance in a pooled case-control study of incident, sporadic colorectal adenomas. Am. J. Epidemiol. 2013, 178, 610–624. [Google Scholar] [CrossRef]
- Sumida, Y.; Nakajima, A.; Itoh, Y. Limitations of liver biopsy and non-invasive diagnostic tests for the diagnosis of nonalcoholic fatty liver disease/nonalcoholic steatohepatitis. World J. Gastroenterol. 2014, 20, 475. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| OBS Components | Property | Male | Female | ||||
|---|---|---|---|---|---|---|---|
| T1 | T2 | T3 | T1 | T2 | T3 | ||
| Dietary OBS components | |||||||
| Dietary fiber (g/day) | A | ≤5.65 | 5.65< ≤7.85 | >7.85 | ≤5.35 | 5.35< ≤7.7 | >7.7 |
| Carotene (ug/day) | A | ≤2627.76 | 2627.76< ≤4735.96 | >4735.96 | ≤2744.36 | 2744.36< ≤4883.75 | >4883.75 |
| Riboflavin (mg/day) | A | ≤0.84 | 0.84< ≤1.16 | >1.16 | ≤0.8 | 0.8< ≤1.11 | >1.11 |
| Niacin (mg/day) | A | ≤12.43 | 12.43< ≤16.76 | >16.76 | ≤11 | 11< ≤14.88 | >14.88 |
| Vitamin B6 (mg/day) | A | ≤1.28 | 1.28< ≤1.69 | >1.69 | ≤1.18 | 1.18< ≤1.6 | >1.6 |
| Total folate (mcg/day) | A | ≤264.07 | 264.07< ≤371.51 | >371.51 | ≤247.1 | 247.1< ≤354.44 | >354.44 |
| Vitamin C (mg/day) | A | ≤65.53 | 65.53< ≤104.21 | >104.21 | ≤67.89 | 67.89< ≤108.89 | >108.89 |
| Vitamin E (ATE) (mg/day) | A | ≤6.99 | 6.99< ≤9.75 | >9.75 | ≤6.69 | 6.69< ≤9.58 | >9.58 |
| Calcium (mg/day) | A | ≤367.08 | 367.08< ≤528.09 | >528.09 | ≤343.99 | 343.99< ≤504.23 | >504.23 |
| Zinc (mg/day) | A | ≤6.38 | 6.38< ≤8.05 | >8.05 | ≤5.7 | 5.7< ≤7.44 | >7.44 |
| Total fat (g/day) | P | ≤25.52 | 25.52< ≤38.31 | >38.31 | ≤22.92 | 22.92< ≤34.57 | >34.57 |
| Iron (mg/day) | P | ≤10.77 | 10.77< ≤14.69 | >14.69 | ≤10.08 | 10.08< ≤14.15 | >14.15 |
| Lifestyle OBS components | |||||||
| Physical activity a | A | Inactive or low activity | Active | Very active | Inactive or low activity | Active | Very active |
| Alcohol (g/day) b | P | None | 0< ≤30 | ≥30 | None | 0< ≤20 | ≥20 |
| Body mass index (kg/m2) | P | ≤23.23 | 23.23< ≤25.47 | >25.47 | ≤22.26 | 22.26< ≤24.67 | >24.67 |
| Smoking status c | P | Never smoker | Former smoker | Current smoker | Never smoker | Former smoker | Current smoker |
| Tertile Scores for “A” | T1 score: 0 | T2 score: 1 | T3 score: 2 | T1 score: 0 | T2 score: 1 | T3 score: 2 | |
| Tertile Scores for “P” d | T1 score: 2 | T2 score: 1 | T3 score: 0 | T1 score: 2 | T2 score: 1 | T3 score: 0 | |
| Total | Group 1 | Group 2 | Group 3 | ||
|---|---|---|---|---|---|
| (n = 9798) | T1 [3, 15] (n = 2666) | T2 (15, 22] (n = 3600) | T3 (22, 31] (n = 3532) | p-Value | |
| Sex (men) | 2396 (24.5) | 769 (28.8) | 887 (24.6) | 740 (21.0) | <0.001 |
| Age (years) | 54.0 ± 8.0 | 53.5 ± 8.1 | 53.8 ± 8.2 | 54.5 ± 7.7 | <0.001 |
| BMI (kg/m2) | 22.8 ± 2.2 | 23.2 ± 2.3 | 22.8 ± 2.2 | 22.5 ± 2.2 | <0.001 |
| Waist circumference (cm) | 77.4 ± 7.6 | 78.4 ± 7.7 | 77.5 ± 7.6 | 76.7 ± 7.4 | <0.001 |
| Systolic BP (mmHg) | 120.5 ± 14.4 | 120.7 ± 14.5 | 120.2 ± 14.5 | 120.7 ± 14.4 | 0.284 |
| Diastolic BP (mmHg) | 73.9 ± 9.2 | 74.2 ± 9.4 | 73.8 ± 9.2 | 73.7 ± 9.1 | 0.065 |
| FPG (mg/dL) | 92.4 ± 12.0 | 92.4 ± 12.4 | 92.3 ± 11.4 | 92.5 ± 12.3 | 0.663 |
| Total cholesterol (mg/dL) | 199.0 ± 35.0 | 200.4 ± 35.7 | 198.2 ± 34.7 | 198.8 ± 34.8 | 0.042 |
| HDL cholesterol (mg/dL) | 56.8 ± 13.7 | 56.3 ± 13.6 | 56.7 ± 13.7 | 57.3 ± 13.8 | 0.008 |
| Triglyceride (mg/dL) | 111.7 ± 68.3 | 115.3 ± 68.5 | 111.8 ± 68.1 | 109.0 ± 68.2 | 0.001 |
| Smoking status, n (%) a | <0.001 | ||||
| Never smoker | 7958 (81.2) | 2027 (76.0) | 2919 (81.1) | 3012 (85.3) | |
| Former smoker | 1224 (12.5) | 382 (14.3) | 453 (12.6) | 389 (11.0) | |
| Current smoker | 616 (6.3) | 257 (9.6) | 228 (6.3) | 131 (3.7) | |
| Alcohol intake, n (%) b | <0.001 | ||||
| Never drinker | 5763 (58.8) | 1369 (51.4) | 2083 (57.9) | 2311 (65.4) | |
| Former drinker | 310 (3.2) | 84 (3.2) | 117 (3.2) | 109 (3.1) | |
| Current drinker | 3725 (38.0) | 1213 (45.5) | 1400 (38.9) | 1112 (31.5) | |
| Regular exercise (Yes) c | 5604 (57.2) | 1339 (50.2) | 2051 (57.0) | 2214 (62.7) | <0.001 |
| Hypertension, n (%) | 1526 (15.6) | 421 (15.8) | 547 (15.2) | 558 (15.8) | 0.731 |
| Dyslipidemia, n (%) | 2507 (25.6) | 739 (27.7) | 909 (25.2) | 859 (24.3) | 0.008 |
| CKD, n (%) | 73 (0.7) | 17 (0.6) | 37 (1.0) | 19 (0.5) | 0.042 |
| Group 1 | Group 2 | Group 3 | |||
|---|---|---|---|---|---|
| T1 [3, 15] (n = 2666) | T2 (15, 22] (n = 3600) | T3 (22, 31] (n = 3532) | p for Trend | ||
| New cases of type 2 diabetes mellitus, n | 52 | 51 | 42 | ||
| Mean follow-up, years | 3.63 | 3.54 | 3.44 | ||
| Person-years of follow-up | 9682 | 12,736 | 12,157 | ||
| Incidence rate/1000 person-years | 5.37 | 4.00 | 3.45 | ||
| Incidence rate per 1000 person-years | |||||
| Model 1 | HR (95% CI) | 1.00 (reference) | 0.76 (0.52–1.12) | 0.66 (0.44–0.99) | 0.043 |
| p-value | 0.164 | 0.044 | |||
| Model 2 | HR (95% CI) | 1.00 (reference) | 0.78 (0.52–1.16) | 0.62 (0.40–0.95) | 0.029 |
| p-value | - | 0.213 | 0.029 | ||
| Model 3 | HR (95% CI) | 1.00 (reference) | 0.79 (0.53–1.18) | 0.60 (0.39–0.93) | 0.017 |
| p-value | - | 0.247 | 0.023 | ||
| Univariable | Multivariable * | |||
|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Dietary OBS components | ||||
| Dietary fiber (ref. T1) | ||||
| T2 | 0.76 (0.51–1.13) | 0.182 | 0.55 (0.33–0.90) | 0.017 |
| T3 | 0.74 (0.50–1.10) | 0.132 | 0.56 (0.30–1.05) | 0.071 |
| Carotene (ref. T1) | ||||
| T2 | 0.85 (0.56–1.29) | 0.437 | 1.01 (0.62–1.64) | 0.982 |
| T3 | 1.17 (0.79–1.73) | 0.425 | 2.02 (1.18–3.44) | 0.010 |
| Riboflavin (ref. T1) | ||||
| T2 | 0.93 (0.63–1.38) | 0.721 | 1.24 (0.76–2.03) | 0.395 |
| T3 | 0.81 (0.54–1.21) | 0.301 | 0.91 (0.48–1.71) | 0.766 |
| Niacin (ref. T1) | ||||
| T2 | 0.85 (0.58–1.26) | 0.429 | 0.79 (0.48–1.29) | 0.338 |
| T3 | 0.76 (0.51–1.13) | 0.180 | 0.74 (0.39–1.39) | 0.347 |
| Vitamin B6 (ref. T1) | ||||
| T2 | 0.85 (0.58–1.26) | 0.429 | 1.79 (1.08–2.96) | 0.024 |
| T3 | 0.76 (0.51–1.13) | 0.180 | 0.84 (0.42–1.69) | 0.626 |
| Total folate (ref. T1) | ||||
| T2 | 1.29 (0.88–1.90) | 0.188 | 0.57 (0.35–0.93) | 0.025 |
| T3 | 0.71 (0.46–1.10) | 0.125 | 0.65 (0.36–1.19) | 0.161 |
| Vitamin C (ref. T1) | ||||
| T2 | 0.68 (0.45–1.01) | 0.055 | 1.15 (0.70–1.88) | 0.583 |
| T3 | 0.71 (0.48–1.04) | 0.080 | 1.15 (0.65–2.06) | 0.626 |
| Vitamin E (ATE) (ref. T1) | ||||
| T2 | 0.85 (0.57–1.29) | 0.454 | 1.28 (0.80–2.05) | 0.309 |
| T3 | 0.94 (0.63–1.39) | 0.758 | 1.12 (0.64–1.98) | 0.693 |
| Calcium (ref. T1) | ||||
| T2 | 0.86 (0.58–1.28) | 0.464 | 0.71 (0.44–1.15) | 0.163 |
| T3 | 0.84 (0.56–1.25) | 0.383 | 0.98 (0.59–1.62) | 0.927 |
| Zinc (ref. T1) | ||||
| T2 | 0.59 (0.38–0.89) | 0.013 | 0.67 (0.40–1.12) | 0.124 |
| T3 | 0.82 (0.56–1.19) | 0.289 | 0.96 (0.51–1.80) | 0.906 |
| Total fat (ref. T3) | ||||
| T2 | 1.08 (0.72–1.61) | 0.723 | 0.75 (0.47–1.20) | 0.228 |
| T1 | 1.13 (0.76–1.69) | 0.540 | 0.50 (0.27–0.90) | 0.020 |
| Iron (ref. T3) | ||||
| T2 | 1.11 (0.75–1.64) | 0.611 | 1.17 (0.71–1.93) | 0.542 |
| T1 | 1.11 (0.74–1.67) | 0.602 | 1.08 (0.55–2.12) | 0.829 |
| Lifestyle OBS components | ||||
| Physical activity (ref. inactive or low activity) a | ||||
| Active | 1.34 (0.80–2.22) | 0.264 | 1.20 (0.71–2.00) | 0.497 |
| Very active | 0.92 (0.41–2.07) | 0.841 | 1.02 (0.45–2.30) | 0.963 |
| Alcohol (ref. Male: 0–30 g/day; Female: 0-20 g/day) | ||||
| None | 1.18 (0.84–1.66) | 0.346 | 1.38 (0.94–2.03) | 0.100 |
| Body mass index (ref. T3) | ||||
| T2 | 0.61 (0.41–0.91) | 0.016 | 0.73 (0.49–1.10) | 0.137 |
| T1 | 0.47 (0.31–0.71) | <0.001 | 0.52 (0.33–0.80) | 0.003 |
| Smoke (ref. Current smoker) b | ||||
| Former smoker | 0.64 (0.35–1.17) | 0.145 | 1.23 (0.58–2.61) | 0.586 |
| Never smoker | 0.42 (0.26–0.69) | <0.000 | 1.39 (0.63–3.09) | 0.412 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moon, M.-E.; Jung, D.H.; Heo, S.-J.; Park, B.; Lee, Y.J. Oxidative Balance Score and New-Onset Type 2 Diabetes Mellitus in Korean Adults without Non-Alcoholic Fatty Liver Disease: Korean Genome and Epidemiology Study-Health Examinees (KoGES-HEXA) Cohort. Antioxidants 2024, 13, 107. https://doi.org/10.3390/antiox13010107
Moon M-E, Jung DH, Heo S-J, Park B, Lee YJ. Oxidative Balance Score and New-Onset Type 2 Diabetes Mellitus in Korean Adults without Non-Alcoholic Fatty Liver Disease: Korean Genome and Epidemiology Study-Health Examinees (KoGES-HEXA) Cohort. Antioxidants. 2024; 13(1):107. https://doi.org/10.3390/antiox13010107
Chicago/Turabian StyleMoon, Mid-Eum, Dong Hyuk Jung, Seok-Jae Heo, Byoungjin Park, and Yong Jae Lee. 2024. "Oxidative Balance Score and New-Onset Type 2 Diabetes Mellitus in Korean Adults without Non-Alcoholic Fatty Liver Disease: Korean Genome and Epidemiology Study-Health Examinees (KoGES-HEXA) Cohort" Antioxidants 13, no. 1: 107. https://doi.org/10.3390/antiox13010107
APA StyleMoon, M. -E., Jung, D. H., Heo, S. -J., Park, B., & Lee, Y. J. (2024). Oxidative Balance Score and New-Onset Type 2 Diabetes Mellitus in Korean Adults without Non-Alcoholic Fatty Liver Disease: Korean Genome and Epidemiology Study-Health Examinees (KoGES-HEXA) Cohort. Antioxidants, 13(1), 107. https://doi.org/10.3390/antiox13010107