Effects and Mechanisms of Tea and Its Bioactive Compounds for the Prevention and Treatment of Cardiovascular Diseases: An Updated Review

 ,
,  and
and 
Abstract
:1. Introduction
2. Epidemiological Studies
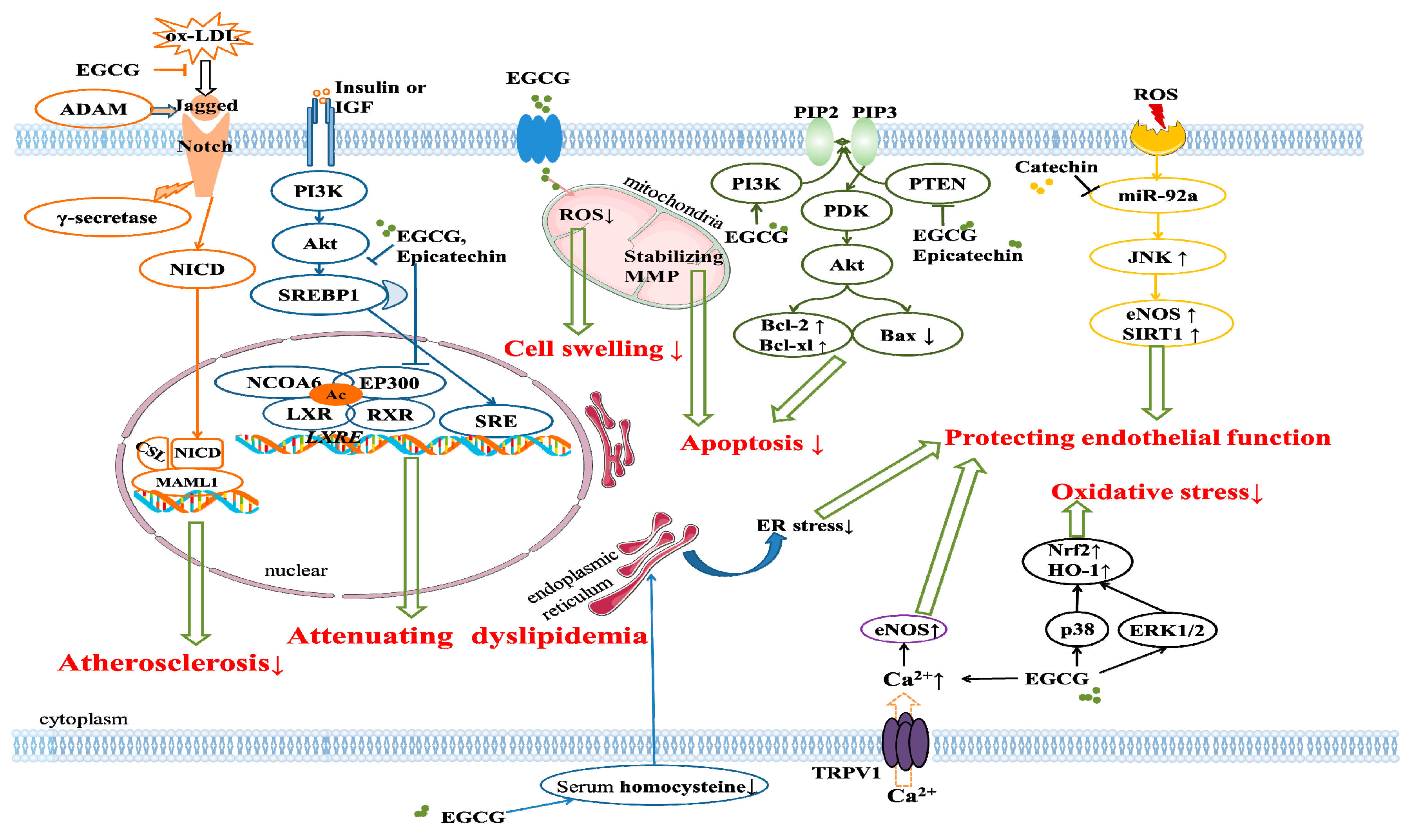
3. Experimental Studies
3.1. Lowering Blood Lipids
3.2. Ameliorating Ischemia/Reperfusion Injury
3.3. Protecting Endothelial Function
3.4. Protecting Cardiomyocyte Function
3.5. Reducing Oxidative Stress
3.6. Alleviating Inflammation
4. Clinical Trails
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Cardiovascular Disease. Available online: https://www.who.int/cardiovascular_diseases/en/ (accessed on 20 April 2019).
- Yusuf, S.; Reddy, S.; Ounpuu, S.; Anand, S. Global burden of cardiovascular diseases: part I: general considerations, the epidemiologic transition, risk factors, and impact of urbanization. Circulation 2001, 104, 2746–2753. [Google Scholar] [CrossRef] [PubMed]
- Zhao, C.N.; Meng, X.; Li, Y.; Li, S.; Liu, Q.; Tang, G.Y.; Li, H.B. Fruits for prevention and treatment of cardiovascular diseases. Nutrients 2017, 9, 598. [Google Scholar] [CrossRef] [PubMed]
- Tang, G.Y.; Meng, X.; Li, Y.; Zhao, C.N.; Liu, Q.; Li, H.B. Effects of vegetables on cardiovascular diseases and related mechanisms. Nutrients 2017, 9, 857. [Google Scholar] [CrossRef]
- Zheng, J.; Zhou, Y.; Li, S.; Zhang, P.; Zhou, T.; Xu, D.P.; Li, H.B. Effects and mechanisms of fruit and vegetable juices on cardiovascular diseases. Int. J. Mol. Sci. 2017, 18, 555. [Google Scholar] [CrossRef] [PubMed]
- Deng, G.F.; Xu, X.R.; Guo, Y.J.; Xia, E.Q.; Li, S.; Wu, S.; Chen, F.; Ling, W.H.; Li, H.B. Determination of antioxidant property and their lipophilic and hydrophilic phenolic contents in cereal grains. J. Funct. Foods 2012, 4, 906–914. [Google Scholar] [CrossRef]
- Zheng, J.; Zhou, Y.; Li, Y.; Xu, D.P.; Li, S.; Li, H.B. Spices for prevention and treatment of cancers. Nutrients 2016, 8, 495. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.J.; Deng, G.F.; Xu, X.R.; Wu, S.; Li, S.; Xia, E.Q.; Li, F.; Chen, F.; Ling, W.H.; Li, H.B. Antioxidant capacities, phenolic compounds and polysaccharide contents of 49 edible macro-fungi. Food Funct. 2012, 3, 1195–1205. [Google Scholar] [CrossRef] [PubMed]
- Angelino, D.; Godos, J.; Ghelfi, F.; Tieri, M.; Titta, L.; Lafranconi, A.; Marventano, S.; Alonzo, E.; Gambera, A.; Sciacca, S.; et al. Fruit and vegetable consumption and health outcomes: an umbrella review of observational studies. Int. J. Food Sci. Nutr. 2019, 15, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Aune, D.; Keum, N.; Giovannucci, E.; Fadnes, L.T.; Boffetta, P.; Greenwood, D.C.; Tonstad, S.; Vatten, L.J.; Riboli, E.; Norat, T. Whole grain consumption and risk of cardiovascular disease, cancer, and all cause and cause specific mortality: Systematic review and dose-response meta-analysis of prospective studies. BMJ 2016, 353, i2716. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Keogh, J.; Clifton, P.M. Nuts and cardio-metabolic disease: A review of meta-analyses. Nutrients 2018, 10, 1935. [Google Scholar] [CrossRef]
- Pang, J.; Zhang, Z.; Zheng, T.Z.; Bassig, B.A.; Mao, C.; Liu, X.; Zhu, Y.; Shi, K.; Ge, J.; Yang, Y.J.; et al. Green tea consumption and risk of cardiovascular and ischemic related diseases: A meta-analysis. Int. J. Cardiol. 2016, 202, 967–974. [Google Scholar] [CrossRef] [PubMed]
- Grosso, G.; Stepaniak, U.; Micek, A.; Topor-Mądry, R.; Pikhart, H.; Szafraniec, K.; Pająk, A. Association of daily coffee and tea consumption and metabolic syndrome: results from the Polish arm of the HAPIEE study. Eur. J. Nutr. 2015, 54, 1129–1137. [Google Scholar] [CrossRef] [PubMed]
- Hodgson, J.M.; Croft, K.D. Tea flavonoids and cardiovascular health. Mol. Aspects Med. 2010, 31, 495–502. [Google Scholar] [CrossRef] [PubMed]
- Higdon, J.V.; Frei, B. Tea catechins and polyphenols: Health effects, metabolism, and antioxidant functions. Crit. Rev. Food Sci. Nutr. 2003, 43, 89–143. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Gan, L.Q.; Li, S.K.; Zheng, J.C.; Xu, D.P.; Li, H.B. Effects of herbal infusions, tea and carbonated beverages on alcohol dehydrogenase and aldehyde dehydrogenase activity. Food Funct. 2014, 5, 42–49. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Li, S.; Li, H.B.; Deng, G.F.; Ling, W.H.; Xu, X.R. Antiproliferative activities of tea and herbal infusions. Food Funct. 2013, 4, 530–538. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.Y.; Zhao, C.N.; Cao, S.Y.; Tang, G.Y.; Gan, R.Y.; Li, H.B. Effects and mechanisms of tea for the prevention and management of cancers: An updated review. Crit. Rev. Food Sci. Nutr. 2019, in press. [Google Scholar] [CrossRef]
- Wang, X.; Ouyang, Y.Y.; Liu, J.; Zhao, G. Flavonoid intake and risk of CVD: A systematic review and meta-analysis of prospective cohort studies. Br. J. Nutr. 2014, 111, 1–11. [Google Scholar] [CrossRef]
- Grosso, G.; Micek, A.; Godos, J.; Pajak, A.; Sciacca, S.; Galvano, F.; Giovannucci, E.L. Dietary flavonoid and lignan intake and mortality in prospective cohort studies: systematic review and dose-response meta-analysis. Am. J. Epidemiol. 2017, 185, 1304–1316. [Google Scholar] [CrossRef]
- Grosso, G.; Godos, J.; Lamuela-Raventos, R.; Ray, S.; Micek, A.; Pajak, A.; Sciacca, S.; D’Orazio, N.; Del Rio, D.; Galvano, F. A comprehensive meta-analysis on dietary flavonoid and lignan intake and cancer risk: Level of evidence and limitations. Mol. Nutr. Food Res. 2017, 61, 1600930. [Google Scholar] [CrossRef]
- Liu, J.X.; Liu, S.W.; Zhou, H.M.; Hanson, T.; Yang, L.; Chen, Z.M.; Zhou, M.G. Association of green tea consumption with mortality from all-cause, cardiovascular disease and cancer in a Chinese cohort of 165,000 adult men. Eur. J. Epidemiol. 2016, 31, 853–865. [Google Scholar] [CrossRef] [PubMed]
- Dower, J.I.; Geleijnse, J.M.; Hollman, P.C.H.; Soedamah-Muthu, S.S.; Kromhout, D. Dietary epicatechin intake and 25-y risk of cardiovascular mortality: The Zutphen Elderly Study. Am. J. Clin. Nutr. 2016, 104, 58–64. [Google Scholar] [CrossRef] [PubMed]
- Xu, P.; Ying, L.; Hong, G.J.; Wang, Y.F. The effects of the aqueous extract and residue of Matcha on the antioxidant status and lipid and glucose levels in mice fed a high-fat diet. Food Funct. 2016, 7, 294–300. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.M.; Asimi, S.; Wu, K.J.; Zheng, J.S.; Li, D. Black tea consumption and serum cholesterol concentration: Systematic review and meta-analysis of randomized controlled trials. Clin. Nutr. 2015, 34, 612–619. [Google Scholar] [CrossRef] [PubMed]
- Samavat, H.; Newman, A.R.; Wang, R.; Yuan, J.; Wu, A.H.; Kurzer, M.S. Effects of green tea catechin extract on serum lipids in postmenopausal women: a randomized, placebo-controlled clinical trial. Am. J. Clin. Nutr. 2016, 104, 1671–1682. [Google Scholar] [CrossRef] [PubMed]
- Saito, E.; Inoue, M.; Sawada, N.; Shimazu, T.; Yamaji, T.; Iwasaki, M.; Sasazuki, S.; Noda, M.; Iso, H.; Tsugane, S. Association of green tea consumption with mortality due to all causes and major causes of death in a Japanese population: The Japan Public Health Center-based Prospective Study (JPHC Study). Ann. Epidemiol. 2015, 25, 512–518. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.G.; Li, H.L.; Sun, J.W.; Yang, Y.; Ma, X.; Shu, X.O.; Zheng, W.; Xiang, Y.B. Green tea consumption and cause-specific mortality: Results from two prospective cohort studies in China. J. Epidemiol. 2017, 27, 36–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van den Brandt, P.A. Coffee or Tea? A prospective cohort study on the associations of coffee and tea intake with overall and cause-specific mortality in men versus women. Eur. J. Epidemiol. 2018, 33, 183–200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tian, C.; Huang, Q.; Yang, L.L.; Légaré, S.; Angileri, F.; Yang, H.D.; Li, X.L.; Min, X.W.; Zhang, C.; Xu, C.W.; et al. Green tea consumption is associated with reduced incident CHD and improved CHD-related biomarkers in the Dongfeng-Tongji cohort. Sci. Rep. 2016, 6, 24353. [Google Scholar] [CrossRef]
- Miller, P.E.; Zhao, D.; Frazier-Wood, A.C.; Michos, E.D.; Averill, M.; Sandfort, V.; Burke, G.L.; Polak, J.F.; Lima, J.A.C.; Post, W.S.; et al. Associations of coffee, tea, and caffeine intake with coronary artery calcification and cardiovascular events. Am. J. Med. 2017, 130, 188–197. [Google Scholar] [CrossRef]
- Ivey, K.L.; Hodgson, J.M.; Croft, K.D.; Lewis, J.R.; Prince, R.L. Flavonoid intake and all-cause mortality. Am. J. Clin. Nutr. 2015, 101, 1012–1020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grosso, G.; Stepaniak, U.; Topor-Mądry, R.; Szafraniec, K.; Pająk, A. Estimated dietary intake and major food sources of polyphenols in the Polish arm of the HAPIEE study. Nutrition 2014, 30, 1398–1403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Micek, A.; Grosso, G.; Polak, M.; Kozakiewicz, K.; Tykarski, A.; Puch Walczak, A.; Drygas, W.; Kwaśniewska, M.; Pająk, A.; On behalf of WOBASZ II Investigators. Association between tea and coffee consumption and prevalence of metabolic syndrome in Poland—Results from the WOBASZ II study (2013–2014). Int. J. Food Sci. Nutr. 2018, 69, 358–368. [Google Scholar] [CrossRef] [PubMed]
- Adriouch, S.; Lampuré, A.; Nechba, A.; Baudry, J.; Assmann, K.; Kesse-Guyot, E.; Hercberg, S.; Scalbert, A.; Touvier, M.; Fezeu, L.K. Prospective association between total and specific dietary polyphenol intakes and cardiovascular disease risk in the Nutrinet-Santé French cohort. Nutrients 2018, 10, 1587. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, A.; Iso, H.; Yamagishi, K.; Iwasaki, M.; Yamaji, T.; Miura, T.; Sawada, N.; Inoue, M.; Tsugane, S. Plasma tea catechins and risk of cardiovascular disease in middle-aged Japanese subjects: The JPHC study. Atherosclerosis 2018, 277, 90–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sowers, J.R.; Epstein, M.; Frohlich, E.D. Diabetes, hypertension, and cardiovascular disease—An update. Hypertension 2001, 37, 1053–1059. [Google Scholar] [CrossRef] [PubMed]
- Alkerwi, A.; Sauvageot, N.; Crichton, G.E.; Elias, M.F. Tea, but not coffee consumption, is associated with components of arterial pressure. The observation of cardiovascular risk factors study in Luxembourg. Nutr. Res. 2015, 35, 557–565. [Google Scholar] [CrossRef]
- Yin, J.Y.; Duan, S.Y.; Liu, F.C.; Yao, Q.K.; Tu, S.; Xu, Y.; Pan, C.W. Blood pressure is associated with tea consumption: A cross-sectional study in a rural, elderly population of Jiangsu China. J. Nutr. Health Aging 2017, 21, 1151–1159. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.E.; Li, J.J.; Wu, Y.T.; Ranjbar, S.; Xing, A.J.; Zhao, H.Y.; Wang, Y.X.; Shearer, G.C.; Bao, L.; Lichtenstein, A.H.; et al. Tea consumption and longitudinal change in high-density lipoprotein cholesterol concentration in Chinese adults. J. Am. Heart Assoc. 2018, 7, e008814. [Google Scholar] [CrossRef]
- Chapman, M.J.; Ginsberg, H.N.; Amarenco, P.; Andreotti, F.; Boren, J.; Catapano, A.L.; Descamps, O.S.; Fisher, E.; Kovanen, P.T.; Kuivenhoven, J.A.; et al. Triglyceride-rich lipoproteins and high-density lipoprotein cholesterol in patients at high risk of cardiovascular disease: Evidence and guidance for management. Eur. Heart J. 2011, 32, 1345–1361. [Google Scholar] [CrossRef]
- Hao, G.; Li, W.; Teo, K.; Wang, X.Y.; Yang, J.G.; Wang, Y.; Liu, L.S.; Yusuf, S. Influence of tea consumption on acute myocardial infarction in China population: The INTERHEART China Study. Angiology 2015, 66, 265–270. [Google Scholar] [CrossRef] [PubMed]
- Bertolotti, M.; Maurantonio, M.; Gabbi, C.; Anzivino, C.; Carulli, N. Review article: hyperlipidaemia and cardiovascular risk. Aliment Pharm. Ther. 2005, 222, 28–30. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.; Hsu, Y.; Chen, Y.M.; Huang, W.C.; Huang, C.C.; Hsu, M.C. Effects of combined extract of cocoa, coffee, green tea and garcinia on lipid profiles, glycaemic markers and inflammatory responses in hamsters. BMC Complement. Altern. Med. 2015, 15, 269. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, M.; Kumazoe, M.; Nakamura, Y.; Won, Y.S.; Bae, J.; Yamashita, S.; Tachibana, H. The combination of green tea extract and eriodictyol inhibited high-fat/high-sucrose diet-induced cholesterol upregulation is accompanied by suppression of cholesterol synthesis enzymes. J. Nutr. Sci. Vitaminol. 2016, 62, 249–256. [Google Scholar] [CrossRef]
- Seo, D.B.; Jeong, H.W.; Kim, Y.J.; Kim, S.; Kim, J.; Lee, J.H.; Joo, K.; Choi, J.K.; Shin, S.S.; Lee, S.J. Fermented green tea extract exhibits hypolipidaemic effects through the inhibition of pancreatic lipase and promotion of energy expenditure. Brit. J. Nutr. 2017, 117, 177–186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yin, J.; Huang, F.; Yi, Y.; Yin, L.; Peng, D. EGCG attenuates atherosclerosis through the Jagged-1/Notch pathway. Int. J. Mol. Med. 2016, 37, 398–406. [Google Scholar] [CrossRef] [PubMed]
- Pan, L.L.; Wu, Y.; Wang, R.Q.; Chen, J.W.; Chen, J.; Zhang, Y.; Chen, Y.; Geng, M.; Xu, Z.D.; Dai, M.; et al. (−)-Epigallocatechin-3-Gallate ameliorates atherosclerosis and modulates hepatic lipid metabolic gene expression in apolipoprotein E knockout mice: Involvement of TTC39B. Front. Pharmacol. 2018, 9, 195. [Google Scholar]
- Suzuki-Sugihara, N.; Kishimoto, Y.; Saita, E.; Taguchi, C.; Kobayashi, M.; Ichitani, M.; Ukawa, Y.; Sagesaka, Y.M.; Suzuki, E.; Kondo, K. Green tea catechins prevent low-density lipoprotein oxidation via their accumulation in low-density lipoprotein particles in humans. Nutr. Res. 2016, 36, 16–23. [Google Scholar] [CrossRef]
- Cheng, H.; Xu, N.; Zhao, W.; Su, J.J.; Liang, M.R.; Xie, Z.W.; Wu, X.L.; Li, Q.L. (−)-Epicatechin regulates blood lipids and attenuates hepatic steatosis in rats fed high-fat diet. Mol. Nutr. Food Res. 2017, 61, 1700303. [Google Scholar] [CrossRef]
- Ding, S.B.; Jiang, J.J.; Yu, P.X.; Zhang, G.F.; Zhang, G.H.; Liu, X.T. Green tea polyphenol treatment attenuates atherosclerosis in high-fat diet-fed apolipoprotein E-knockout mice via alleviating dyslipidemia and upregulating autophagy. PLoS ONE 2017, 12, e0181666. [Google Scholar] [CrossRef]
- Panickar, K.S.; Qin, B.; Anderson, R.A. Ischemia-induced endothelial cell swelling and mitochondrial dysfunction are attenuated by cinnamtannin D1, green tea extract, and resveratrol in vitro. Nutr. Neurosci. 2015, 18, 297–306. [Google Scholar] [CrossRef] [PubMed]
- Martins, A.; Schimidt, H.L.; Garcia, A.; Altermann, C.D.C.; Santos, F.W.; Carpes, F.P.; Da Silva, W.C.; Mello-Carpes, P.B. Supplementation with different teas from Camellia sinensis prevents memory deficits and hippocampus oxidative stress in ischemia-reperfusion. Neurochem. Int. 2017, 108, 287–295. [Google Scholar] [CrossRef] [PubMed]
- Zeng, X.; Tan, X. Epigallocatechin-3-gallate and zinc provide anti-apoptotic protection against hypoxia/reoxygenation injury in H9c2 rat cardiac myoblast cells. Mol. Med. Rep. 2015, 12, 1850–1856. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Huang, X.; Shen, D.; Ming, Z.; Zheng, M.; Zhang, J. Polyphenol epigallocatechin-3-gallate inhibits hypoxia/reoxygenation-induced H9c2 cell apoptosis. Minerva Med. 2018, 109, 95–102. [Google Scholar] [PubMed]
- Othman, A.I.; Elkomy, M.M.; El-Missiry, M.A.; Dardor, M. Epigallocatechin-3-gallate prevents cardiac apoptosis by modulating the intrinsic apoptotic pathway in isoproterenol-induced myocardial infarction. Eur. J. Pharmacol. 2017, 794, 27–36. [Google Scholar] [CrossRef]
- Xuan, F.; Jian, J. Epigallocatechin gallate exerts protective effects against myocardial ischemia/reperfusion injury through the PI3K/Akt pathway-mediated inhibition of apoptosis and the restoration of the autophagic flux. Int. J. Mol. Med. 2016, 38, 328–336. [Google Scholar] [CrossRef]
- Qin, C.Y.; Zhang, H.W.; Gu, J.; Xu, F.; Liang, H.M.; Fan, K.J.; Shen, J.Y.; Xiao, Z.H.; Zhang, E.Y.; Hu, J. Mitochondrial DNA-induced inflammatory damage contributes to myocardial ischemia reperfusion injury in rats: Cardioprotective role of epigallocatechin. Mol. Med. Rep. 2017, 16, 7569–7576. [Google Scholar] [CrossRef] [Green Version]
- Salameh, A.; Schuster, R.; Daehnert, I.; Seeger, J.; Dhein, S. Epigallocatechin gallate reduces ischemia/reperfusion injury in isolated perfused rabbit hearts. Int. J. Mol. Sci. 2018, 19, 628. [Google Scholar] [CrossRef]
- Li, J.W.; Wang, X.Y.; Zhang, X.; Gao, L.; Wang, L.F.; Yin, X.H. (−)-Epicatechin protects against myocardial ischemia-induced cardiac injury via activation of the PTEN/PI3K/AKT pathway. Mol. Med. Rep. 2018, 17, 8300–8308. [Google Scholar] [CrossRef]
- Fang, J.F.; Dai, J.H.; Ni, M.; Cai, Z.Y.; Liao, Y.F. Catechin protects rat cardiomyocytes from hypoxia-induced injury by regulating microRNA-92a. Int. J. Clin. Exp. Pathol. 2018, 11, 3257–3266. [Google Scholar]
- Leung, F.P.; Yung, L.M.; Ngai, C.Y.; Cheang, W.S.; Tian, X.Y.; Lau, C.W.; Zhang, Y.; Liu, J.; Chen, Z.Y.; Bian, Z.X.; et al. Chronic black tea extract consumption improves endothelial function in ovariectomized rats. Eur. J. Nutr. 2016, 55, 1963–1972. [Google Scholar] [CrossRef] [PubMed]
- Cheang, W.S.; Ngai, C.Y.; Tam, Y.Y.; Tian, X.Y.; Wong, W.T.; Zhang, Y.; Lau, C.W.; Chen, Z.Y.; Bian, Z.X.; Huang, Y.; et al. Black tea protects against hypertension-associated endothelial dysfunction through alleviation of endoplasmic reticulum stress. Sci. Rep. 2015, 5, 10340. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.M.; Sun, Z.W.; Chu, P.; Li, H.L.; Ahsan, A.; Zhou, Z.R.; Zhang, Z.H.; Sun, B.; Wu, J.J.; Xi, Y.L.; et al. EGCG protects against homocysteine-induced human umbilical vein endothelial cells apoptosis by modulating mitochondrial-dependent apoptotic signaling and PI3K/Akt/eNOS signaling pathways. Apoptosis 2017, 22, 672–680. [Google Scholar] [CrossRef] [PubMed]
- Zhan, X.L.; Yang, X.H.; Gu, Y.H.; Guo, L.L.; Jin, H.M. Epigallocatechin gallate protects against homocysteine-induced vascular smooth muscle cell proliferation. Mol. Cell Biochem. 2018, 439, 131–140. [Google Scholar] [CrossRef] [PubMed]
- Guo, B.C.; Wei, J.; Su, K.H.; Chiang, A.N.; Zhao, J.F.; Chen, H.Y.; Shyue, S.K.; Lee, T.S. Transient receptor potential vanilloid type 1 is vital for (−)-epigallocatechin-3-gallate mediated activation of endothelial nitric oxide synthase. Mol. Nutr. Food Res. 2015, 59, 646–657. [Google Scholar] [CrossRef] [PubMed]
- Shibu, M.A.; Kuo, C.; Chen, B.; Ju, D.; Chen, R.; Lai, C.; Huang, P.; Viswanadha, V.P.; Kuo, W.; Huang, C. Oolong tea prevents cardiomyocyte loss against hypoxia by attenuating p-JNK mediated hypertrophy and enhancing P-IGF1R, p-Akt, and p-Badser136 activity and by fortifying Nrf2 antioxidation system. Environ. Toxicol. 2018, 33, 220–233. [Google Scholar] [CrossRef] [PubMed]
- Warren, C.M.; Karam, C.N.; Wolska, B.M.; Kobayashi, T.; de Tombe, P.P.; Arteaga, G.M.; Bos, J.M.; Ackerman, M.J.; Solaro, R.J. Green tea catechin normalizes the enhanced Ca2+ sensitivity of myofilaments regulated by a hypertrophic cardiomyopathy-associated mutation in human cardiac troponin I (K206I). Circ-Cardiovasc. Genet. 2015, 8, 765–773. [Google Scholar] [CrossRef]
- Muhammed, I.; Sankar, S.; Govindaraj, S. Ameliorative effect of epigallocatechin gallate on cardiac hypertrophy and fibrosis in aged rats. J. Cardiovasc. Pharm. 2018, 71, 65–75. [Google Scholar]
- Lombo, M.; Gonzalez-Rojo, S.; Fernandez-Diez, C.; Paz Herraez, M. Cardiogenesis impairment promoted by bisphenol A exposure is successfully counteracted by epigallocatechin gallate. Environ. Pollut. 2019, 246, 1008–1019. [Google Scholar] [CrossRef]
- Di Lorenzo, A.; Nabavi, S.F.; Sureda, A.; Moghaddam, A.H.; Khanjani, S.; Arcidiaco, P.; Nabavi, S.M.; Daglia, M. Antidepressive-like effects and antioxidant activity of green tea and GABA green tea in a mouse model of post-stroke depression. Mol. Nutr. Food Res. 2016, 60, 566–579. [Google Scholar] [CrossRef]
- Alves, M.G.; Martins, A.D.; Teixeira, N.F.; Rato, L.; Oliveira, P.F.; Silva, B.M. White tea consumption improves cardiac glycolytic and oxidative profile of prediabetic rats. J. Funct. Foods 2015, 14, 102–110. [Google Scholar] [CrossRef]
- Yang, G.Z.; Wang, Z.J.; Bai, F.; Qin, X.J.; Cao, J.; Lv, J.Y.; Zhang, M.S. Epigallocatechin-3-gallate protects HUVECs from PM2.5-induced oxidative stress injury by activating critical antioxidant pathways. Molecules 2015, 20, 6626–6639. [Google Scholar] [CrossRef] [PubMed]
- Oyama, J.I.; Shiraki, A.; Nishikido, T.; Maeda, T.; Komoda, H.; Shimizu, T.; Makino, N.; Node, K. EGCG, a green tea catechin, attenuates the progression of heart failure induced by the heart/muscle-specific deletion of MnSOD in mice. J. Cardiol. 2017, 69, 417–427. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Yan, Q.; Tang, S.; Xiao, W.; Tan, Z. L-Theanine protects H9c2 cells from hydrogen peroxide-induced apoptosis by enhancing antioxidant capability. Med. Sci. Monit. 2018, 24, 2109–2118. [Google Scholar] [CrossRef] [PubMed]
- Hotamisligil, G.S. Inflammation and metabolic disorders. Nature 2006, 444, 860–867. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Liu, J.; Pang, X.; Zhang, X.; Wang, S.; Wu, D. Epigallocatechin-3-gallate inhibits angiotensin II-induced C-reactive protein generation through interfering with the AT1-ROS-ERK1/2 signaling pathway in hepatocytes. Naunyn Schmiedebergs Arch. Pharmacol. 2016, 389, 1225–1234. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.F.; Xiang, Z.M.; Wang, Y.; Li, X.; Fang, C.Y.; Song, S.; Li, C.L.; Yu, H.S.; Wang, H.; Yan, L.; et al. (−)-Epigallocatechin gallate targets Notch to attenuate the inflammatory response in the immediate early stage in human macrophages. Front. Immunol. 2017, 8, 433. [Google Scholar] [CrossRef] [PubMed]
- Kumazoe, M.; Nakamura, Y.; Yamashita, M.; Suzuki, T.; Takamatsu, K.; Huang, Y.; Bae, J.; Yamashita, S.; Murata, M.; Yamada, S.; et al. Green tea polyphenol epigallocatechin-3-gallate suppresses toll-like receptor 4 expression via upregulation of E3 ubiquitin-protein ligase RNF216. J. Biol. Chem. 2017, 292, 4077–4088. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, E.; Kataoka, S.; Mukai, Y.; Sato, M.; Sato, S. Green tea extract intake during lactation modified cardiac macrophage infiltration and AMP-activated protein kinase phosphorylation in weanling rats from undernourished mother during gestation and lactation. J. Dev. Orig. Health Dis. 2017, 8, 178–187. [Google Scholar] [CrossRef]
- Clifford, M.N.; van der Hooft, J.J.; Crozier, A. Human studies on the absorption, distribution, metabolism, and excretion of tea polyphenols. Am. J. Clin. Nutr. 2013, 98, 1619S–1630S. [Google Scholar] [CrossRef]
- Zhang, J.; Nie, S.; Wang, S. Nanoencapsulation enhances epigallocatechin-3-gallate stability and its antiatherogenic bioactivities in macrophages. J. Agric. Food Chem. 2013, 61, 9200–9209. [Google Scholar] [CrossRef] [PubMed]
- Mena, P.; Bresciani, L.; Brindani, N.; Ludwig, I.A.; Pereira-Caro, G.; Angelino, D.; Llorach, R.; Calani, L.; Brighenti, F.; Clifford, M.N.; et al. Phenyl-γ-valerolactones and phenylvaleric acids, the main colonic metabolites of flavan-3-ols: synthesis, analysis, bioavailability, and bioactivity. Nat. Prod. Rep. 2019, 36, 714–752. [Google Scholar] [CrossRef] [PubMed]
- Pereira-Caro, G.; Moreno-Rojas, J.M.; Brindani, N.; Del Rio, D.; Lean, M.E.J.; Hara, Y.; Crozier, A. Bioavailability of black tea theaflavins: Absorption, metabolism, and colonic catabolism. J. Agric. Food Chem. 2017, 65, 5365–5374. [Google Scholar] [CrossRef] [PubMed]
- Imbe, H.; Sano, H.; Miyawaki, M.; Fujisawa, R.; Miyasato, M.; Nakatsuji, F.; Haseda, F.; Tanimoto, K.; Terasaki, J.; Maeda-Yamamoto, M.; et al. “Benifuuki” green tea, containing O-methylated EGCG reduces serum low-density lipoprotein cholesterol and lectin-like oxidized low-density lipoprotein receptor-1 ligands containing apolipoprotein B: A double-blind, placebo-controlled randomized trial. J. Funct. Foods 2016, 25, 25–37. [Google Scholar] [CrossRef]
- Igarashi, Y.; Obara, T.; Ishikuro, M.; Matsubara, H.; Shigihara, M.; Metoki, H.; Kikuya, M.; Sameshima, Y.; Tachibana, H.; Maeda-Yamamotog, M.; et al. Randomized controlled trial of the effects of consumption of ‘Yabukita’ or ‘Benifuuki’ encapsulated tea-powder on low-density lipoprotein cholesterol level and body weight. Food Nutr. Res. 2017, 61, 1334484. [Google Scholar] [CrossRef]
- Venkatakrishnan, K.; Chiu, H.F.; Cheng, J.C.; Chang, Y.; Lu, Y.Y.; Han, Y.C.; Shen, Y.C.; Tsai, K.S.; Wang, C.K. Comparative studies on the hypolipidemic, antioxidant and hepatoprotective activities of catechin-enriched green and oolong tea in a double-blind clinical trial. Food Funct. 2018, 9, 1205–1213. [Google Scholar] [CrossRef]
- Orem, A.; Alasalvar, C.; Kural, B.V.; Yaman, S.; Orem, C.; Karadag, A.; Pelvan, E.; Zawistowski, J. Cardio-protective effects of phytosterol-enriched functional black tea in mild hypercholesterolemia subjects. J. Funct. Foods 2017, 31, 311–319. [Google Scholar] [CrossRef]
- Wasilewski, R.; Ubara, E.O.; Klonizakis, M. Assessing the effects of a short-term green tea intervention in skin microvascular function and oxygen tension in older and younger adults. Microvasc. Res. 2016, 107, 65–71. [Google Scholar] [CrossRef]
- Nogueira, L.D.P.; Nogueira Neto, J.F.; Klein, M.R.S.T.; Sanjuliani, A.F. Short-term effects of green tea on blood pressure, endothelial function, and metabolic profile in obese prehypertensive women: A crossover randomized clinical trial. J. Am. Coll. Nutr. 2017, 36, 108–115. [Google Scholar] [CrossRef]
- De Jesús Romero-Prado, M.M.; Curiel-Beltrán, J.A.; Miramontes-Espino, M.V.; Cardona-Muñoz, E.G.; Rios-Arellano, A.; Balam-Salazar, L.B. Dietary flavonoids added to pharmacological antihypertensive therapy are effective in improving blood pressure. Basic Clin. Pharmacol. 2015, 117, 57–64. [Google Scholar] [CrossRef]
- Grassi, D.; Draijer, R.; Desideri, G.; Mulder, T.; Ferri, C. Black tea lowers blood pressure and wave reflections in fasted and postprandial conditions in hypertensive patients: A randomised study. Nutrients 2015, 7, 1037–1051. [Google Scholar] [CrossRef]
- Grassi, D.; Draijer, R.; Schalkwijk, C.; Desideri, G.; D’Angeli, A.; Francavilla, S.; Mulder, T.; Ferri, C. Black tea increases circulating endothelial progenitor cells and improves flow mediated dilatation counteracting deleterious effects from a fat load in hypertensive patients: A randomized controlled study. Nutrients 2016, 8, 727. [Google Scholar] [CrossRef] [PubMed]
- Lorenz, M.; Rauhut, F.; Hofer, C.; Gwosc, S.; Mueller, E.; Praeger, D.; Zimmermann, B.F.; Wernecke, K.; Baumann, G.; Stangl, K.; et al. Tea-induced improvement of endothelial function in humans: No role for epigallocatechin gallate (EGCG). Sci. Rep. 2017, 7, 2279. [Google Scholar] [CrossRef] [PubMed]
- Sanguigni, V.; Manco, M.; Sorge, R.; Gnessi, L.; Francomano, D. Natural antioxidant ice cream acutely reduces oxidative stress and improves vascular function and physical performance in healthy individuals. Nutrition 2017, 33, 225–233. [Google Scholar] [CrossRef] [PubMed]
- Dower, J.I.; Geleijnse, J.M.; Gijsbers, L.; Schalkwijk, C.; Kromhout, D.; Hollman, P.C. Supplementation of the pure flavonoids epicatechin and quercetin affects some biomarkers of endothelial dysfunction and inflammation in (pre)hypertensive adults: A randomized double-blind, placebo-controlled, crossover trial. J. Nutr. 2015, 145, 1459–1463. [Google Scholar] [CrossRef] [PubMed]
- Luximon-Ramma, A.; Bahorun, T.; Crozier, A.; Zbarsky, V.; Datla, K.P.; Dexter, D.T.; Aruoma, O.I. Characterization of the antioxidant functions of flavonoids and proanthocyanidins in Mauritian black teas. Food Res. Int. 2005, 38, 357–367. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Subjects | Study Type | Effects | Risk Estimates (95%CI) | Ref. |
|---|---|---|---|---|
| 90,914 Japanese participants aged 40–69 y | cohort study | Reducing the risk of heart disease and cerebrovascular disease | heart disease: 0.70 (0.56–0.87) for 3–4 cups/day; cerebrovascular disease: 0.73 (0.56–0.94) for 3–4 cups/day | [27] |
| 165,000 Chinese adult men without pre-existing disease | cohort study | Reducing the risk of CVDs | 0.93(0.85–1.01) for ≤5 g/day; 0.91 (0.85–0.98) for 5–10 g/day; 0.86 (0.79–0.93) for >10 g/day | [22] |
| 74,941 women aged 40–70 y and 61,491 men aged 40–74 y in China | cohort study | Reducing the risk of CVDs | 0.86 (0.77–0.97) | [28] |
| 120,852 men and women in the Netherlands aged 55–69 y | cohort study | Reducing the risk of CVDs | 0.72 (0.57–0.91) for 2–3 cups/day in men | [29] |
| 19,471 participants free of CHD, stroke or cancer | cohort study | Reducing the risk of CHD | 0.89 (0.81–0.98) | [30] |
| 6508 participants from Multi-Ethnic Study of Atherosclerosis | cohort study | Slowing the progression of coronary artery calcium | 0.71 (0.53–0.95) for ≥1 cup/day | [31] |
| 1063 women aged >75 y in Australia | cohort study | Reducing the mortality of CVDs | 0.34 (0.17–0.69) for data from USDA; 0.32 (0.16–0.61) for data from Phenol-Explorer databases | [32] |
| 774 Dutch men aged 65–84 y | cohort study | Reducing the risk of CVDs | 0.54 (0.31–0.96) | [23] |
| 80,182 Chinese participants aged 37–61 y free of CVDs, cancers, and cholesterol-lowering agent use | cohort study | Increasing blood HDL-C | NA | [40] |
| 29,876 participants aged 40–69 y free of heart disease, stroke, or cancer in Japan | case-control study | Lowering the risk of stroke in non-smoking men | 0.53 (0.29–0.98) | [36] |
| 1352 participants aged 18–69 y in Luxembourg | cross-sectional study | Decreasing the SBP and pulse pressure | NA | [38] |
| 4579 participants aged ≥60 y in China | cross-sectional study | Lowering DBP and the risk of hypertension | 0.79 (0.65–0.95) | [39] |
| 5856 participants (case 2909, control 2947) in China | case-control study | Increasing the risk of acute myocardial infarction | 1.29 (1.03–1.61) for 4 cups/d | [42] |
| Substances | Subjects | Study Type | Dose | Effects and Mechanisms | Ref. |
|---|---|---|---|---|---|
| Green tea extract | Male C57BL/6J mice | In vivo | 0.2% (w/w) | HMGCR↓, HMGCS↓, cholesterol↓ | [45] |
| Matcha | Male ICR mice | In vivo | 0.025%, 0.05%, 0.075% (w/w) | TC↓, TG↓, LDL-C↓, serum glucose↓; HDL↑, SOD↑, MAD↑ | [24] |
| Bacillus-fermented green tea | Pancreatic lipase; Sprague-Dawley male Rats | In vitro and in vivo | IC50 0.48 mg/mL; 500mg/kg | TG↓, pancreatic lipase activity↓ | [46] |
| Green tea infusion | Male Wistar rats | In vivo | 400 mg/kg | Hippocampal oxidative stress↓, necrosis↓ | [53] |
| GABA green tea | Male balb/c mice | In vivo | 50 and 100 mg/kg | Oxidative stress↓; Antioxidant endogenous defenses↑ | [71] |
| Green tea extract | Pregnant Wistar rats | In vivo | 0.12%, 0.24% | Cardiac macrophage infiltration↓; Insulin↑ | [80] |
| Black tea | Female Sprague-Dawley rats | In vivo | 15 mg/kg/day | NADPH oxidases↓, ROS↓; Flow-mediated dilatation↑ | [62] |
| Black tea | Rat aortic endothelial cells; Male Sprague Dawley rats | In vitro and in vivo | 0.3–5 μM; 15 mg/kg/day | Endothelial injury↓, serum homocysteine↓, endoplasmic reticulum stress↓ | [63] |
| Oolong tea | H9c2 cardiac myoblast cells; Neonatal rat ventricular cardiomyocytes | In vitro | 100, 200, 400 mg/mL | Cardiomyocyte loss ↓, hypertrophy ↓ | [67] |
| White tea | Male Wistar rats | In vivo | 1 g/100 mL | Cardiac glycolytic↑, antioxidant capacity↑ | [72] |
| EGCG | Human umbilical vein endothelial cells; ApoE−/− mice | In vitro and in vivo | 50 µM; 0.8 g/L | Endothelial dysfunction↓; Jagged-1/Notch activated | [47] |
| EGCG | ApoE−/− mice | In vivo | 40 mg/kg/d | IL-6↓, TNF-α↓, TG↓, TC↓, LDL↓; IL-10↑, HDL↑, LXR/SREBP-1 pathways modulated | [48] |
| EGCG | H9c2 cardiac myoblast cells | In vitro | 5, 10, 15, and 20 µM | Hypoxia/reoxygenation induced apoptosis↓ | [54] |
| EGCG | H9c2 cardiac myoblast cells | In vitro | 10 μM | Apoptosis↓; Stabilizing mitochondrial membrane potential | [55] |
| EGCG | Albino Westar rats | In vivo | 15 mg/kg. | Myocardial infarction↓ | [56] |
| EGCG | Male Sprague-Dawley rats | In vivo | 10 mg/kg | Myocardial apoptosis↓ | [57] |
| EGCG | Chinchilla rabbit heart | In vitro | 20 μM/L | Oxidative stress↓; ATP↑ | [59] |
| EGCG | Male Wistar rats | In vivo | 10 mg/kg | Plasma mtDNA↓, TNF↓, IL-6 ↓, IL-8↓, ventricular arrhythmia↓ | [58] |
| EGCG | Human umbilical vein endothelial cells | In vitro | 10, 20, 30 µM | Apoptosis↓ | [64] |
| EGCG | Human aortic smooth muscle cells | In vitro | 20 µM | Homocysteine-induced proliferation↓ | [65] |
| EGCG | Bovine aortic endothelial cells; WT C57BL mice and TRPV1−/− mice | In vitro and in vivo | 0, 1.25, 2.5, 10, 20 μM; 10 μM | Angiogenesis↑ | [66] |
| EGCG | Wistar albino rats | In vivo | 200 mg/kg | Cardiac hypertrophy↓, fibrosis↓, LDL↓, VLDL↓, TG↓, TC↓; HDL↑, TGFβ↑, TNFα↑, NF-κB↑ | [69] |
| EGCG | Zebrafish embryos | In vivo | 50, 100 μM | Damage caused by bisphenol A↓ | [70] |
| EGCG | Human umbilical vein endothelial cells | In vitro | 50, 100, 200, 300, 400 μM | Oxidative stress↓; Nrf2↑, HO-1↑ | [73] |
| EGCG | Heart/muscle-specific MnSOD-deficient mice | In vivo | 10 mg/L, 100 mg/L | Myocardial oxidative stress↓, free fatty acid↓ | [74] |
| EGCG | Male Sprague-Dawley rats | In vivo | 25, 50 mg/kg/day | Ang II type 1 receptor↓, ERK1/2↓; PPARγ ↑ | [77] |
| EGCG | Human monocyte cell line | In vitro | 50 µg/mL | Inflammatory response↓ | [78] |
| EGCG | Male C57/BL6 mice | In vivo | 0, 2.5, 5, 10 μM | TLR4 expression↓ | [79] |
| Epicatechin | Male Sprague-Dawley rats | In vivo | 10, 20, 40 mg/kg | TC↓, LDL-C↓, TG↓; HDL-C↑ | [50] |
| Theanine | H9c2 cardiac myoblast cells | In vitro | 0, 4, 8, 16 μM | Peroxide-induced apoptosis↓, ROS↓; SOD↑ | [75] |
| Subjects | Substances | Treatments | Effects and Mechanisms | Ref. |
|---|---|---|---|---|
| 155 healthy participants | A green tea containing O-methylated catechin | 12 g/d for 12 weeks | LDL-C↓, LAB↓ | [85] |
| 151 participants aged 30–70 y | Green tea | 1.8 g/d for 12 weeks | LDL-C↓ | [86] |
| 15 participants aged 18–35 y and 15 participants aged 55–75 y | Green tea | 2 cups/d for 14 days | Improving SBP and skin microvascular function | [89] |
| 20 women aged 32.7–49.5 y | Green tea extract | 500 mg for 4 weeks | SBP↓ | [90] |
| 50 healthy men | Green tea | A single dose of 200 mg EGCG | Improving flow-mediated dilation | [94] |
| 14 healthy individuals | Green tea polyphenol-enriched ice cream | A single dose of 100 g | Oxidative stress↓,Vascular function↑ | [95] |
| 79 hypertension patients aged 20–55 y | Flavonoids from green tea | 425.8 ± 13.9 mg epicatechin equivalents for 6 months | SBP ↓, DBP↓ | [91] |
| 60 individuals with mild hypercholesterolemia | Catechin-enriched green or oolong tea | 780.6 mg/d or 640.4 mg/d catechin for 12 weeks | TC↓, LDL-C↓, TG↓ | [87] |
| 1075 healthy postmenopausal women | Catechins | 1315 mg for 1 year | TC↓, LDL-C↓, non-HDL-C levels↓ | [26] |
| 99 participants aged 25–60 y with mild hypercholesterolemia | Phytosterol-enriched instant black tea | 2.5 g/d for 4 weeks | Blood lipids↓ | [88] |
| 19 hypertensive patients | Black tea | 129 mg/d flavonoids for 8 days | SBP↓ | [92] |
| 19 hypertension patients | Black tea | 150 mg polyphenols for 8 days | Endothelial function↑ | [93] |
| 37 (Pre)hypertensive participants aged 40–80 y | Epicatechin or quercetin-3-glucoside | 100 mg/d or 160 mg/d, respectively, for 4 weeks | Inflammation↓,Endothelial function ↑ | [96] |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cao, S.-Y.; Zhao, C.-N.; Gan, R.-Y.; Xu, X.-Y.; Wei, X.-L.; Corke, H.; Atanasov, A.G.; Li, H.-B. Effects and Mechanisms of Tea and Its Bioactive Compounds for the Prevention and Treatment of Cardiovascular Diseases: An Updated Review. Antioxidants 2019, 8, 166. https://doi.org/10.3390/antiox8060166
Cao S-Y, Zhao C-N, Gan R-Y, Xu X-Y, Wei X-L, Corke H, Atanasov AG, Li H-B. Effects and Mechanisms of Tea and Its Bioactive Compounds for the Prevention and Treatment of Cardiovascular Diseases: An Updated Review. Antioxidants. 2019; 8(6):166. https://doi.org/10.3390/antiox8060166
Chicago/Turabian StyleCao, Shi-Yu, Cai-Ning Zhao, Ren-You Gan, Xiao-Yu Xu, Xin-Lin Wei, Harold Corke, Atanas G. Atanasov, and Hua-Bin Li. 2019. "Effects and Mechanisms of Tea and Its Bioactive Compounds for the Prevention and Treatment of Cardiovascular Diseases: An Updated Review" Antioxidants 8, no. 6: 166. https://doi.org/10.3390/antiox8060166
APA StyleCao, S. -Y., Zhao, C. -N., Gan, R. -Y., Xu, X. -Y., Wei, X. -L., Corke, H., Atanasov, A. G., & Li, H. -B. (2019). Effects and Mechanisms of Tea and Its Bioactive Compounds for the Prevention and Treatment of Cardiovascular Diseases: An Updated Review. Antioxidants, 8(6), 166. https://doi.org/10.3390/antiox8060166