Multiple Effects of Ascorbic Acid against Chronic Diseases: Updated Evidence from Preclinical and Clinical Studies

 ,
,  ,
,  , , , , , ,
, , , , , ,
Abstract
:1. Introduction
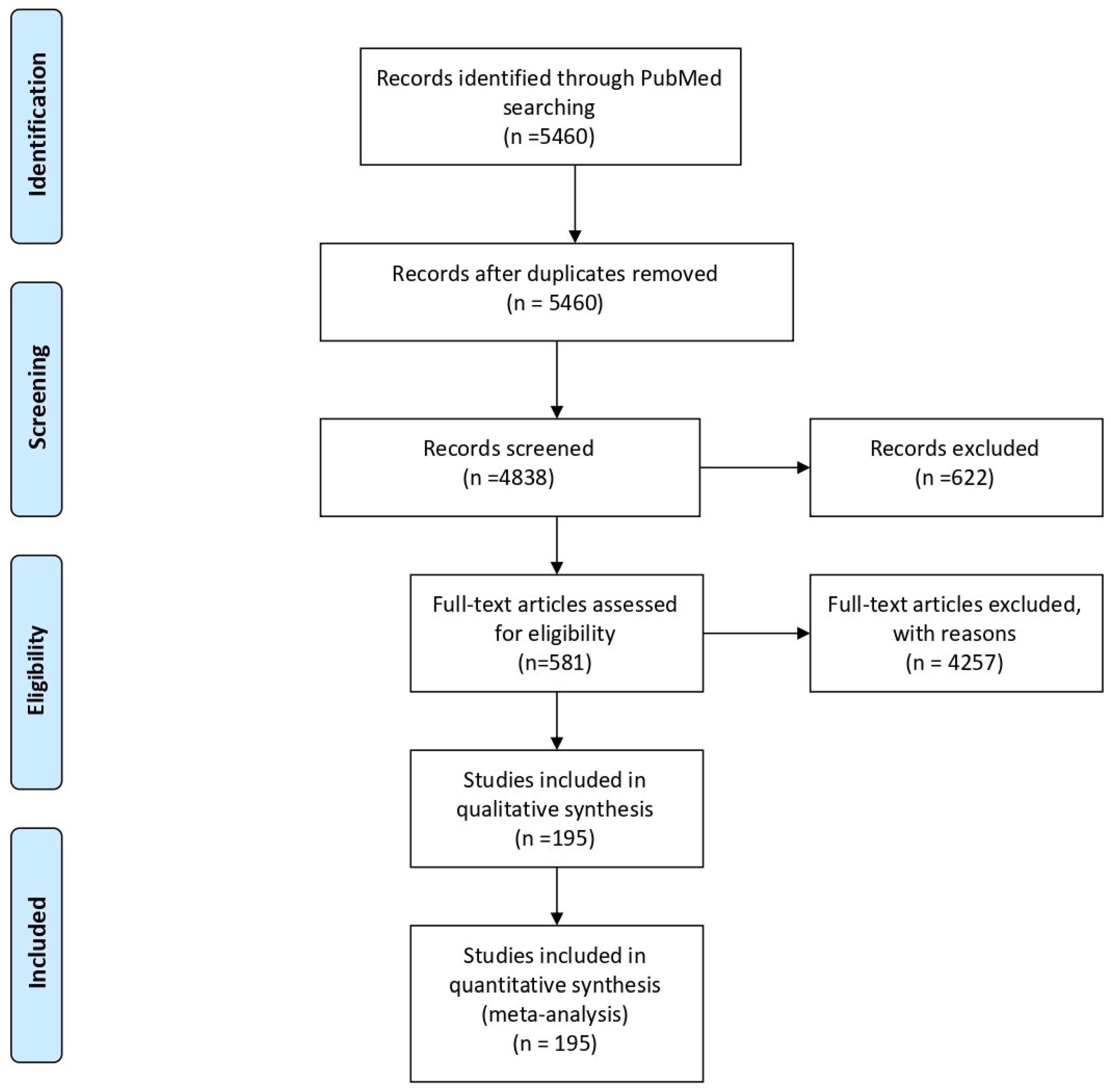
2. Materials and Methods
3. ASC Pharmacokinetics
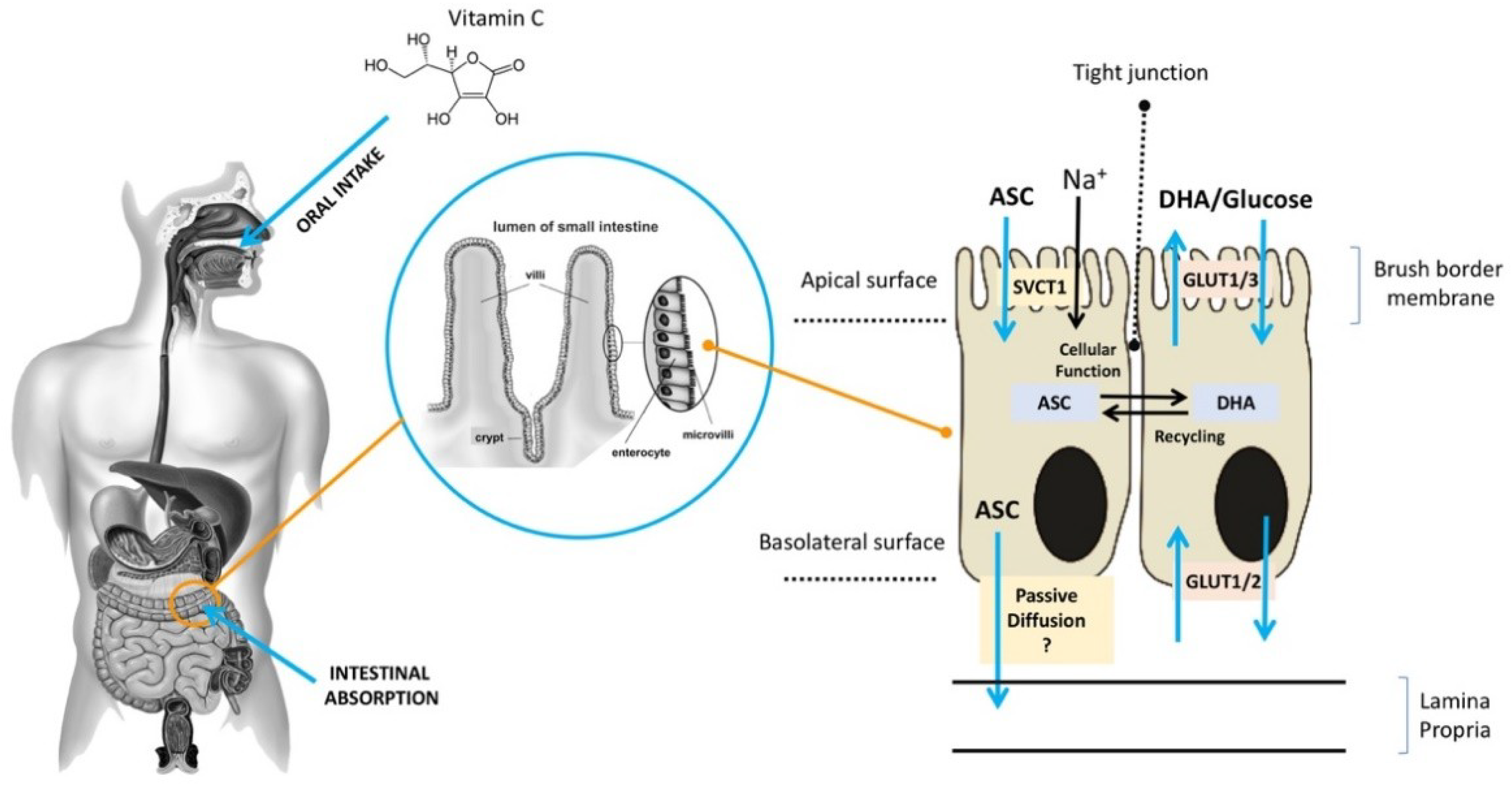
3.1. ASC Absorption
3.2. ASC Distribution
3.3. ASC Metabolism
3.4. ASC Excretion and Resorption
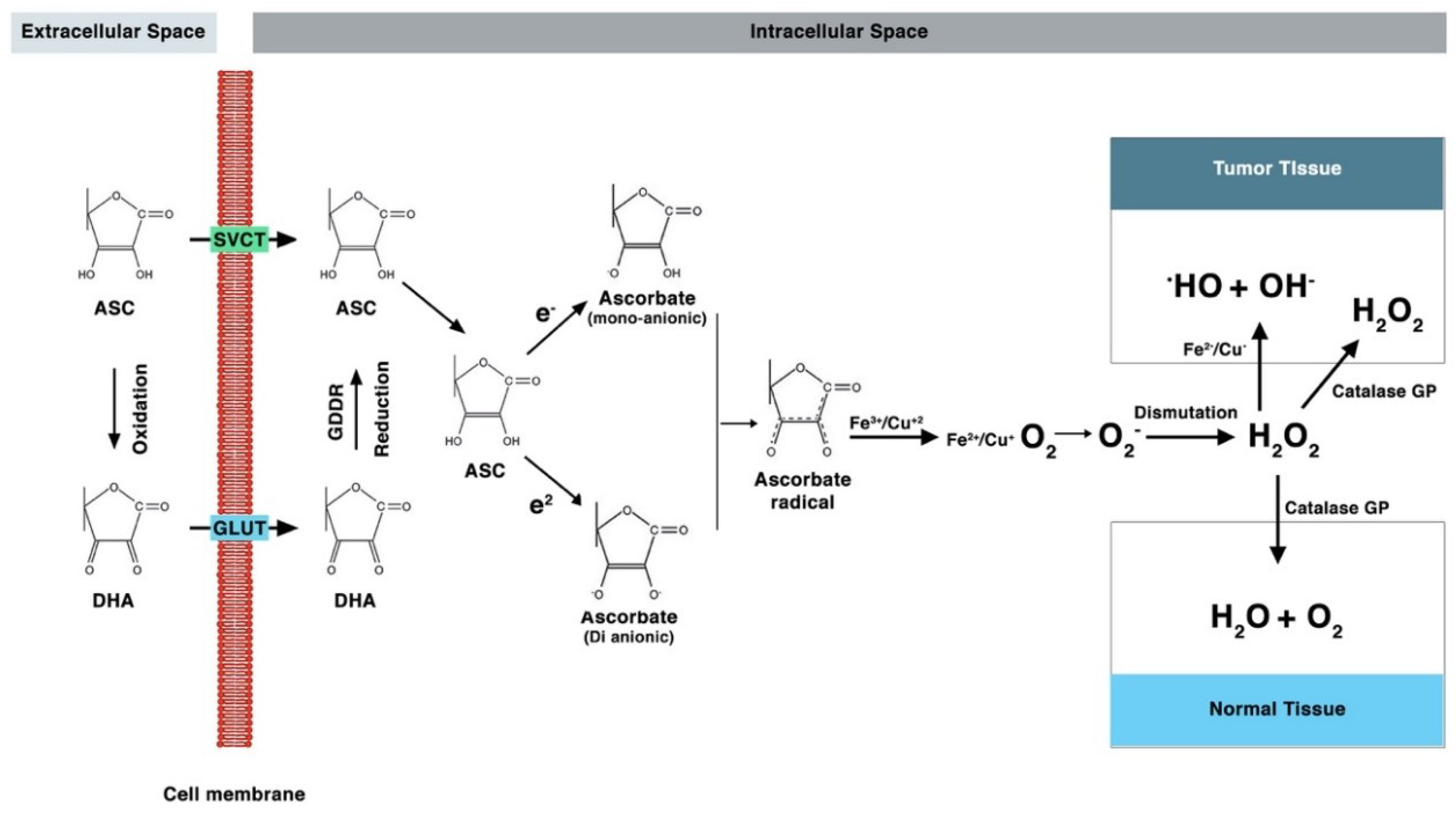
4. Mechanism of Action of Ascorbic Acid
5. Drug Interactions
6. Genetic Variance of ASC Uptake
7. Epigenetic Function of ASC
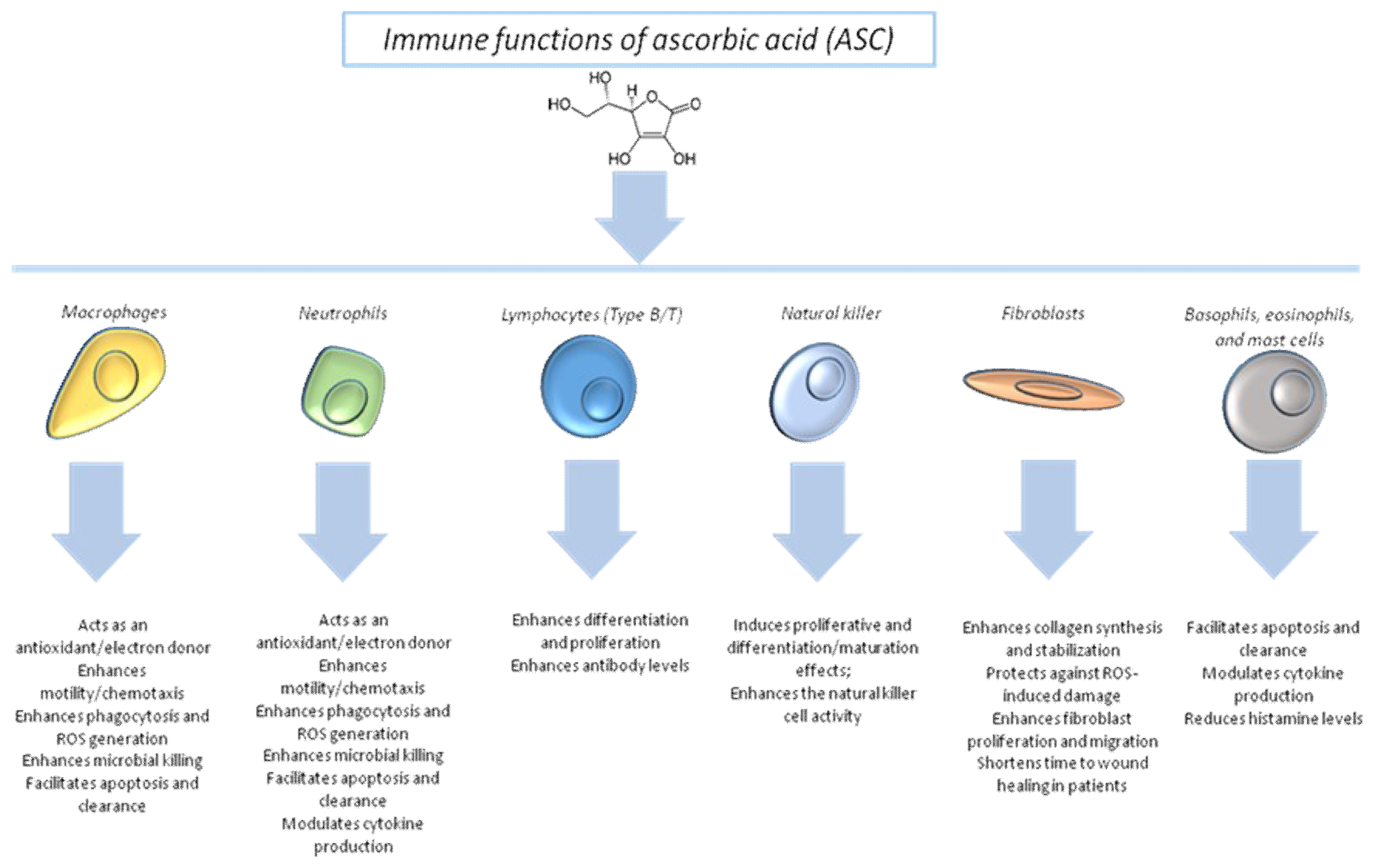
8. Immune Modulation by Ascorbic Acid
9. Cancer
9.1. Effect of Pharmacological ASC on Cancer Cells
9.2. ASC Administration in Clinical Studies
10. Role of ASC in the Management of Infectious Diseases
11. Cardioprotective and Vasculoprotective Properties of ASC
12. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Drouin, G.; Godin, J.; Page, B. The Genetics of ASC Loss in Vertebrates. Curr. Genom. 2011, 12, 371–378. [Google Scholar] [CrossRef] [PubMed]
- Baron, J. Sailors’ scurvy before and after James Lind—A reassessment. Nutr. Rev. 2009, 67, 315–332. [Google Scholar] [CrossRef] [PubMed]
- Verrax, J.; Buc Calderon, P. The controversial place of Vitamin C in cancer treatment. Biochem. Pharmacol. 2008, 76, 1644–1652. [Google Scholar] [CrossRef] [PubMed]
- Du, J.; Yuan, Y.; Si, T.; Lian, J.; Zhao, H. Customized optimization of metabolic pathways by combinatorial transcriptional engineering. Nucleic Acids Res. 2012, 40, e142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rivas, M.; Cobreros, L.; Zeidler, M.; Hombría, J. Plasticity of Drosophila Stat DNA binding shows an evolutionary basis for Stat transcription factor preferences. EMBO Rep. 2008, 9, 1114–1120. [Google Scholar] [CrossRef] [Green Version]
- Vera, A.; Simon, H. Situated Action: A Symbolic Interpretation. Cogn. Sci. 1993, 17, 7–48. [Google Scholar] [CrossRef] [Green Version]
- Tsukaguchi, H.; Tokui, T.; Mackenzie, B.; Berger, U.; Chen, X.; Wang, Y.; Brubaker, R.; Hediger, M. A family of mammalian Na+-dependent L-ascorbic acid transporters. Nature 1999, 399, 70–75. [Google Scholar] [CrossRef]
- Tveden-Nyborg, P.; Lykkesfeldt, J. Does ASC Deficiency Increase Lifestyle-Associated Vascular Disease Progression? Evidence Based on Experimental and Clinical Studies. Antioxid. Redox Signal. 2013 19, 2084–2104.
- Lykkesfeldt, J.; Poulsen, H. Is ASC supplementation beneficial? Lessons learned from randomised controlled trials. Br. J. Nutr. 2009, 103, 1251–1259. [Google Scholar] [CrossRef]
- Frei, B.; Birlouez-Aragon, I.; Lykkesfeldt, J. Authors’ Perspective: What is the Optimum Intake of ASC in Humans? Crit. Rev. Food Sci. Nutr. 2012, 52, 815–829. [Google Scholar] [CrossRef]
- Frikke-Schmidt, H.; Tveden-Nyborg, P.; Lykkesfeldt, J. ASC in human nutrition. In Vitamins in the Prevention of Human Disease; Herrmann, W., Obeid, R., Eds.; De Gruyter: Berlin, Germany, 2011; pp. 323–347. [Google Scholar]
- Carr, A.; Bozonet, S.; Pullar, J.; Simcock, J.; Vissers, M. A Randomized Steady-State Bioavailability Study of Synthetic versus Natural (Kiwifruit-Derived) ASC. Nutrients 2013, 5, 3684–3695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dachs, G.U.; Munn, D.G.; Carr, A.C.; Vissers, M.C.; Robinson, B.A. Consumption of ASC is below recommended daily intake in many cancer patients and healthy volunteers in Christchurch. N. Z. Med. J. 2014, 127, 73–76. [Google Scholar] [PubMed]
- Lykkesfeldt, J.; Christen, S.; Wallock, L.; Chang, H.; Jacob, R.; Ames, B. Ascorbate is depleted by smoking and repleted by moderate supplementation: A study in male smokers and nonsmokers with matched dietary antioxidant intakes. Am. J. Clin. Nutr. 2000, 71, 530–536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Du, J.; Cullen, J.; Buettner, G. Ascorbic acid: Chemistry, biology and the treatment of cancer. Biochim. Biophys. Acta—Rev. Cancer 2012, 1826, 443–457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.; Mackenzie, B.; Tsukaguchi, H.; Weremowicz, S.; Morton, C.; Hediger, M. Human ASC (l-Ascorbic Acid) Transporter SVCT1. Biochem. Biophys. Res. Commun. 2000, 267, 488–494. [Google Scholar] [CrossRef] [PubMed]
- Viscovich, M. ASC pharmacokinetics of plain and slow release formulations in smokers. Clin. Nutr. 2004, 23, 1043–1050. [Google Scholar] [CrossRef]
- Malo, C.; Wilson, J. Glucose Modulates ASC Transport in Adult Human Small Intestinal Brush Border Membrane Vesicles. J. Nutr. 2000, 130, 63–69. [Google Scholar] [CrossRef] [Green Version]
- Lindblad, M.; Tveden-Nyborg, P.; Lykkesfeldt, J. Regulation of ASC Homeostasis during Deficiency. Nutrients 2013, 5, 2860–2879. [Google Scholar] [CrossRef] [Green Version]
- Corpe, C.; Eck, P.; Wang, J.; Al-Hasani, H.; Levine, M. Intestinal Dehydroascorbic Acid (DHA) Transport Mediated by the Facilitative Sugar Transporters, GLUT2 and GLUT8. J. Biol. Chem. 2013, 288, 9092–9101. [Google Scholar] [CrossRef] [Green Version]
- Vera, J.; Rivas, C.; Fischbarg, J.; Golde, D. Mammalian facilitative hexose transporters mediate the transport of dehydroascorbic acid. Nature 1993, 364, 79–82. [Google Scholar] [CrossRef]
- Mayersohn, M. Ascorbic acid absorption in man—pharmacokinetic implications. Eur. J. Pharmacol. 1972, 19, 140–142. [Google Scholar] [CrossRef]
- Kubler, W.; Gehler, J. Kinetics of intestinal absorption of ascorbic acid. Calculation of non-dosage-dependent absorption processes. Int. Z. Vitam. 1970, 40, 442–453. [Google Scholar]
- Lykkesfeldt, J.; Tveden-Nyborg, P. The Pharmacokinetics of Vitamin, C. Nutrients 2019, 11, 2412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corpe, C.P.; Tu, H.; Eck, P.; Wang, J.; Faulhaber-Walter, R.; Schnermann, J.; Margolis, S.; Padayatty, S.; Sun, H.; Wang, Y.; et al. ASC transporter Slc23a1 links renal reabsorption, ASC tissue accumulation, and perinatal survival in mice. J. Clin. Investig. 2010, 120, 1069–1083. [Google Scholar] [CrossRef] [Green Version]
- Paidi, M.D.; Schjoldager, J.G.; Lykkesfeldt, J.; Tveden-Nyborg, P. Chronic ASC deficiency promotes redox imbalance in the brain but does not alter sodium-dependent ASC transporter 2 expression. Nutrients 2014, 6, 1809–1822. [Google Scholar] [CrossRef] [Green Version]
- Søgaard, D.; Lindblad, M.M.; Paidi, M.D.; Hasselholt, S.; Lykkesfeldt, J.; Tveden-Nyborg, P. In vivo ASC deficiency in Guinea pigs increases ascorbate transporters in liver but not kidney and brain. Nutr. Res. 2014, 34, 639–645. [Google Scholar]
- Levine, M.; Conry-Cantilena, C.; Wang, Y.; Welch, R.W.; Washko, P.W.; Dhariwal, K.R.; Park, J.B.; Lazarev, A.; Graumlich, J.F.; King, J.; et al. VitaminC pharmacokinetics in healthy volunteers: Evidence for a recommended dietary allowance. Proc. Natl. Acad. Sci. USA 1996, 93, 3704–3709. [Google Scholar] [CrossRef] [Green Version]
- Feyaerts, A.F.; Luyten, W. Vitamin C as prophylaxis and adjunctive medical treatment for COVID-19? Nutrition 2020, 110948, 79–80. [Google Scholar] [CrossRef]
- Hasselholt, S.; Tveden-Nyborg, P.; Lykkesfeldt, J. Distribution of ASC is tissue specific with early saturation of the brain and adrenal glands following differential oral dose regimens in guinea pigs. Br. J. Nutr. 2015, 113, 1539–1549. [Google Scholar] [CrossRef] [Green Version]
- Bode, A.M.; Cunningham, L.; Rose, R.C. Spontaneous decay of oxidized ascorbic acid (dehydro-L-ascorbic acid) evaluated by high-pressure liquid chromatography. Clin. Chem. 1990, 36, 1807–1809. [Google Scholar] [CrossRef]
- Lykkesfeldt, J.; Loft, S.; Nielsen, J.B.; Poulsen, H.E. Ascorbic acid and dehydroascorbic acid as biomarkers of oxidative stress caused by smoking. Am. J. Clin. Nutr. 1997, 65, 959–963. [Google Scholar] [CrossRef]
- May, J.M.; Qu, Z.C.; Whitesell, R.R. Ascorbic acid recycling enhances the antioxidant reserve of human erythrocytes. Biochemistry 1995, 34, 12721–12728. [Google Scholar] [CrossRef]
- Mardones, L.; Ormazabal, V.; Romo, X.; Jana, C.; Binder, P.; Pena, E.; Vergara, M.; Zuniga, F.A. The glucose transporter-2 (GLUT2) is a low affinity dehydroascorbic acid transporter. Biochem. Biophys. Res. Commun. 2011, 410, 7–12. [Google Scholar] [CrossRef]
- May, J.M.; Qu, Z.; Morrow, J.D. Mechanisms of ascorbic acid recycling in human erythrocytes. Biochim. Biophys. Acta 2001, 1528, 159–166. [Google Scholar] [CrossRef]
- Levine, M.; Wang, Y.; Padayatty, S.J.; Morrow, J. A new recommended dietary allowance of ASC for healthy young women. Proc. Natl. Acad. Sci. USA 2001, 98, 9842–9846. [Google Scholar] [CrossRef] [Green Version]
- Recalcati, S.; Gammella, E.; Buratti, P.; Cairo, G. Molecular regulation of cellular Iron balance. IUBMB Life 2017, 69, 389–398. [Google Scholar] [CrossRef] [Green Version]
- Ganz, T.; Nemeth, E. Iron homeostasis in host defence and inflammation. Nat. Rev. Immunol. 2015, 15, 500–510. [Google Scholar] [CrossRef] [Green Version]
- Beijnen, J.; Schellens, J. Drug interactions in oncology. Lancet Oncol. 2004, 5, 489–496. [Google Scholar] [CrossRef]
- Vissers, M.; Das, A. Potential Mechanisms of Action for ASC in Cancer: Reviewing the Evidence. Front. Physiol. 2018, 9, 809. [Google Scholar] [CrossRef] [Green Version]
- PharmGKB. Available online: http://pharmgkb.org (accessed on 20 July 2020).
- Gene: SLC23A1 (ENSG00000170482)—Variant Table—Homo_Sapiens—Ensembl Genome Browser 101. Available online: http://uswest.ensembl.org/Homo_sapiens/Gene/Variation_Gene/Table?db=core;g=ENSG00000170482;r=5:139367196-139384553 (accessed on 28 October 2020).
- Senthilkumari, S.; Talwar, B.; Dharmalingam, K.; Ravindran, R.D.; Jayanthi, R.; Sundaresan, P.; Saravanan, C.; Young, I.S.; Dangour, A.D.; Fletcher, A.E. Polymorphisms in sodium-dependent ASC transporter genes and plasma, aqueous humor and lens nucleus ascorbate concentrations in an ascorbate depleted setting. Exp. Eye Res. 2014, 124, 24–30. [Google Scholar] [CrossRef]
- Erichsen, H.C.; Peters, U.; Eck, P.; Welch, R.; Schoen, R.E.; Yeager, M.; Levine, M.; Hayes, R.B.; Chanock, S. Genetic variation in sodium-dependent ASC transporters SLC23A1 and SLC23A2 and risk of advanced colorectal adenoma. Nutr. Cancer 2008, 60, 652–659. [Google Scholar] [CrossRef] [Green Version]
- Amir Shaghaghi, M.; Bernstein, C.N.; Serrano Leon, A.; El-Gabalawy, H.; Eck, P. Polymorphisms in the sodium-dependent ascorbate transporter gene SLC23A1 are associated with susceptibility to Crohn disease. Am. J. Clin. Nutr. 2014, 99, 378–383. [Google Scholar] [CrossRef] [Green Version]
- Wade, K.H.; Forouhi, N.G.; Cook, D.G.; Johnson, P.; McConnachie, A.; Morris, R.W.; Rodriguez, S.; Ye, Z.; Ebrahim, S.; Padmanabhan, S.; et al. Variation in the SLC23A1 gene does not influence cardiometabolic outcomes to the extent expected given its association with L-ascorbic acid. Am. J. Clin. Nutr. 2015, 101, 202–209. [Google Scholar] [CrossRef] [Green Version]
- Padayatty, S.; Levine, M. ASC: The known and the unknown and Goldilocks. Oral Dis. 2016, 22, 463–493. [Google Scholar] [CrossRef] [Green Version]
- Baylin, S.; Jones, P. Epigenetic Determinants of Cancer. Cold Spring Harb. Perspect. Biol. 2016, 8, a019505. [Google Scholar] [CrossRef] [Green Version]
- Chung, T.; Brena, R.; Kolle, G.; Grimmond, S.; Berman, B.; Laird, P.; Pera, M.; Wolvetang, E. ASC Promotes Widespread Yet Specific DNA Demethylation of the Epigenome in Human Embryonic Stem Cells. STEM Cells 2010, 28, 1848–1855. [Google Scholar] [CrossRef]
- Iwamori, N.; Zhao, M.; Meistrich, M.; Matzuk, M. The Testis-Enriched Histone Demethylase, KDM4D, Regulates Methylation of Histone H3 Lysine 9 During Spermatogenesis in the Mouse but Is Dispensable for Fertility1. Biol. Reprod. 2011, 84, 1225–1234. [Google Scholar] [CrossRef]
- Schmitz, S.; Albert, M.; Malatesta, M.; Morey, L.; Johansen, J.; Bak, M.; Tommerup, N.; Abarrategui, I.; Helin, K. Jarid1b targets genes regulating development and is involved in neural differentiation. EMBO J. 2011, 30, 4586–4600. [Google Scholar] [CrossRef] [Green Version]
- Wang, C.; Lee, J.; Cho, Y.; Xiao, Y.; Jin, Q.; Liu, C.; Ge, K. UTX regulates mesoderm differentiation of embryonic stem cells independent of H3K27 demethylase activity. Proc. Natl. Acad. Sci. USA 2012, 109, 15324–15329. [Google Scholar] [CrossRef] [Green Version]
- Dawlaty, M.; Breiling, A.; Le, T.; Raddatz, G.; Barrasa, M.; Cheng, A.; Gao, Q.; Powell, B.; Li, Z.; Xu, M.; et al. Combined Deficiency of Tet1 and Tet2 Causes Epigenetic Abnormalities but Is Compatible with Postnatal Development. Dev. Cell 2013, 24, 310–323. [Google Scholar] [CrossRef] [Green Version]
- Pan, Z.; Sikander, S.; Witherspoon, M.; Dizon, D.; Nguyen, T.; Benirsche, K.; Wiley, C.; Vrana, P.; Lipkin, S.M. Impaired placental trophoblast lineage differentiation in Alkbh1-/- mice. Dev. Dyn. 2008, 237, 316–327. [Google Scholar] [CrossRef] [PubMed]
- Esteban, M.; Wang, T.; Qin, B.; Yang, J.; Qin, D.; Cai, J.; Li, W.; Weng, Z.; Chen, J.; Ni, S.; et al. ASC Enhances the Generation of Mouse and Human Induced Pluripotent Stem Cells. Cell Stem Cell 2010, 6, 71–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stadtfeld, M.; Apostolou, E.; Ferrari, F.; Choi, J.; Walsh, R.; Chen, T.; Ooi, S.; Kim, S.; Bestor, T.; Shioda, T.; et al. Ascorbic acid prevents loss of Dlk1-Dio3 imprinting and facilitates generation of all–iPS cell mice from terminally differentiated B cells. Nat. Genet. 2012, 44, 398–405. [Google Scholar] [CrossRef] [PubMed]
- Kogut, M.; Lee, A.; Santin, E. Microbiome and pathogen interaction with the immune system. Poult. Sci. 2020, 99, 1906–1913. [Google Scholar] [CrossRef]
- Carr, A.; Maggini, S. Vitamin C and Immune Function. Nutrients 2017, 9, 1211. [Google Scholar] [CrossRef] [Green Version]
- Padayatty, S.; Katz, A.; Wang, Y.; Eck, P.; Kwon, O.; Lee, J.; Chen, S.; Corpe, C.; Dutta, A.; Dutta, S.; et al. ASC as an Antioxidant: Evaluation of Its Role in Disease Prevention. J. Am. Coll. Nutr. 2003, 22, 18–35. [Google Scholar] [CrossRef]
- Callus, C.; Vella, S.; Ferry, P. Scurvy is Back. Nutr. Metab. Insights 2018, 11, 117863881880909. [Google Scholar] [CrossRef] [Green Version]
- Hood, J. Cardiac Disorders in Scurvy. N. Engl. J. Med. 1970, 282, 282–283. [Google Scholar]
- Chambial, S.; Dwivedi, S.; Shukla, K.; John, P.; Sharma, P. ASC in Disease Prevention and Cure: An Overview. Indian J. Clin. Biochem. 2013, 28, 314–328. [Google Scholar] [CrossRef] [Green Version]
- Carr, A.; Frei, B. Toward a new recommended dietary allowance for ASC based on antioxidant and health effects in humans. Am. J. Clin. Nutr. 1999, 69, 1086–1107. [Google Scholar] [CrossRef] [Green Version]
- Wong, S.K.; Chin, K.Y.; Ima-Nirwana, S. Vitamin C: A Review on its Role in the Management of Metabolic Syndrome. Int. J. Med. Sci. 2020, 17, 1625–1638. [Google Scholar] [CrossRef]
- Ströhle, A.; Hahn, A. ASC und Immun function. Med. Monatsschrift Pharm. 2009, 32, 49–54. [Google Scholar]
- Traber, M.; Stevens, J. Vitamins C and E: Beneficial effects from a mechanistic perspective. Free Radic. Biol. Med. 2011, 51, 1000–1013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heitzer, T.; Just, H.; Münzel, T. Antioxidant ASC Improves Endothelial Dysfunction in Chronic Smokers. Circulation 1996, 94, 6–9. [Google Scholar] [CrossRef] [PubMed]
- Aydoğan, M.; Korkmaz, A.; Barlas, N.; Kolankaya, D. The effect of ASC on bisphenol A, nonylphenol and octylphenol induced brain damages of male rats. Toxicology 2008, 249, 35–39. [Google Scholar] [CrossRef]
- Smithard, D.; Langman, M. ASC and drug metabolism. BMJ 1977, 1, 1029–1030. [Google Scholar] [CrossRef] [Green Version]
- Thomas, W.R.; Holt, P.G. ASC and immunity: An assessment of the evidence. Clin. Exp. Immunol. 1978, 32, 370–379. [Google Scholar]
- Luo, G.; Xie, Z.Z.; Liu, F.Y.; Zhang, G.B. Effects of ASC on myocardial mitochondrial function and ATP content in hypoxic rats. Zhongguo Yao Li Xue Bao 1998, 19, 351–355. [Google Scholar]
- Gibson, S.L.; Moore, F.M.; Goldberg, A. Measurement of leucocyte ascorbic acid. Br. Med. J. 1966, 1, 1152–1153. [Google Scholar] [CrossRef] [Green Version]
- Mitmesser, S.H.; Ye, Q.; Evans, M.; Combs, M. Determination of plasma and leukocyte ASC concentrations in a randomized, double-blind, placebo-controlled trial with Ester-C. Springerplus 2016, 25, 1161. [Google Scholar] [CrossRef] [Green Version]
- Gess, B.; Lohmann, C.; Halfter, H.; Young, P. Sodium-dependent ASC transporter 2 (SVCT2) is necessary for the uptake of L-ascorbic acid into Schwann cells. Glia 2010, 58, 287–299. [Google Scholar] [PubMed]
- Bozonet, S.M.; Carr, A.C.; Pullar, J.M.; Vissers, M.C. Enhanced human neutrophil ASC status, chemotaxis and oxidant generation following dietary supplementation with ASC-rich SunGold kiwifruit. Nutrients 2015, 7, 2574–2588. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liugan, M.; Carr, A.C. ASC and Neutrophil Function: Findings from Randomized Controlled Trials. Nutrients 2019, 11, 2102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bursać-Mitrović, M.; Milovanović, D.; Mitić, R.; Jovanović, D.; Sovrlić, M.; Vasiljević, P.; Tomović, J.; Manojlović, N. Effects Of L-Ascorbic Acid and Alpha-Tocopherol on Biochemical Parameters Of Swimming-Induced Oxidative Stress In Serum Of Guinea Pigs. Afr. J. Tradit. Complement. Altern. Med. 2016, 13, 29–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boretti, A.; Banik, B.K. Intravenous ASC for reduction of cytokines storm in acute respiratory distress syndrome. PharmaNutrition 2020, 12, 100190. [Google Scholar] [CrossRef]
- Quagliariello, V.; Vecchione, R.; Coppola, C.; Di Cicco, C.; De Capua, A.; Piscopo, G.; Paciello, R.; Narciso, V.; Formisano, C.; Taglialatela-Scafati, O.; et al. Cardioprotective Effects of Nanoemulsions Loaded with Anti-Inflammatory Nutraceuticals against Doxorubicin-Induced Cardiotoxicity. Nutrients 2018, 10, 1304. [Google Scholar] [CrossRef] [Green Version]
- Kuhn, S.O.; Meissner, K.; Mayes, L.M.; Bartels, K. ASC in sepsis. Curr. Opin. Anaesthesiol. 2018, 31, 55–60. [Google Scholar] [CrossRef]
- Shin, T.G.; Kim, Y.J.; Ryoo, S.M.; Hwang, S.Y.; Jo, I.J.; Chung, S.P.; Choi, S.H.; Suh, G.J.; Kim, W.Y. Early ASC and Thiamine Administration to Patients with Septic Shock in Emergency Departments: Propensity Score-Based Analysis of a Before-and-After Cohort Study. J. Clin. Med. 2019, 16, 102. [Google Scholar] [CrossRef] [Green Version]
- Gorkom, G.N.Y.; Klein Wolterink, R.G.J.; Van Elssen, C.H.M.J.; Wieten, L.; Germeraad, W.T.V.; Bos, G.M.J. Influence of ASC on Lymphocytes: An Overview. Antioxidants (Basel) 2018, 7, 41. [Google Scholar] [CrossRef] [Green Version]
- Manning, J.; Mitchel, L.B.; Appadurai, D.A.; Shakya, A.; Pierce, L.J.; Wang, H.; Nganga, V.; Swanson, P.C.; May, J.M.; Tantin, D.; et al. ASC promotes maturation of T-cells. Antioxid. Redox Signal. 2013, 10, 2054–2067. [Google Scholar] [CrossRef] [Green Version]
- Huijskens, M.J.; Walczak, M.; Sarkar, S.; Atrafi, F.; Senden-Gijsbers, B.L.; Tilanus, M.G.; Bos, G.M.; Wieten, L.; Germeraad, W.T. Ascorbic acid promotes proliferation of natural killer cell populations in culture systems applicable for natural killer cell therapy. Cytotherapy 2015, 17, 613–620. [Google Scholar] [CrossRef] [PubMed]
- Silverstein, R.J.; Landsman, A.S. The effects of a moderate and high dose of ASC on wound healing in a controlled guinea pig model. J. Foot Ankle Surg. 1999, 38, 333–338. [Google Scholar] [CrossRef]
- Mousavi, S.; Bereswill, S.; Heimesaat, M.M. Immunomodulatory and Antimicrobial Effects of Vitamin C. Eur. J. Microbiol. Immunol. (Bp) 2019, 16, 973–979. [Google Scholar] [CrossRef] [PubMed]
- Kaur, B.; Rowe, B.; Stovold, E. ASC supplementation for asthma. Cochrane Database Syst. Rev. 2009, 2009, CD000993. [Google Scholar]
- Härtel, C.; Strunk, T.; Bucsky, P.; Schultz, C. Effects of Vitamin C on intracytoplasmic cytokine production in human whole blood monocytes and lymphocytes. Cytokine 2004, 27, 101–106. [Google Scholar] [CrossRef]
- Liu, Q.; Zhou, Y.H.; Yang, Z.Q. The cytokine storm of severe influenza and development of immunomodulatory therapy. Cell Mol. Immunol. 2016, 13, 3–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, Y.; Kim, H.; Bae, S.; Choi, J.; Lim, S.Y.; Lee, N.; Kong, J.M.; Hwang, Y.I.; Kang, J.S.; Lee, W.J. Vitamin C Is an Essential Factor on the Anti-viral Immune Responses through the Production of Interferon-α/β at the Initial Stage of Influenza A Virus (H3N2) Infection. Immune Netw. 2013, 13, 70–74. [Google Scholar] [CrossRef] [Green Version]
- Oudemans-van Straaten, H.M.; Spoelstra-de Man, A.M.; de Waard, M.C. Vitamin C revisited. Crit. Care 2014, 18, 460. [Google Scholar] [CrossRef] [Green Version]
- Cameron, E.; Pauling, L. Supplemental ascorbate in the supportive treatment of cancer: Prolongation of survival times in terminal human cancer. Proc. Natl. Acad. Sci. USA 1976, 73, 3685–3689. [Google Scholar] [CrossRef] [Green Version]
- Cameron, E.; Pauling, L. Supplemental ascorbate in the supportive treatment of cancer: Reevaluation of prolongation of survival times in terminal human cancer. Proc. Natl. Acad. Sci. USA 1978, 75, 4538–4542. [Google Scholar] [CrossRef] [Green Version]
- McCormick, W.J. Cancer: The preconditioning factor in pathogenesis; a new etiologic approach. Arch. Pediatr. 1954, 71, 313–322. [Google Scholar] [PubMed]
- McCormick, W.J. Cancer: A collagen disease, secondary to a nutritional deficiency. Arch. Pediatr. 1959, 76, 166–171. [Google Scholar]
- Cameron, E.; Rotman, D. Ascorbic acid, cell proliferation, and cancer. Lancet 1972, 299, 542. [Google Scholar] [CrossRef]
- Cameron, E.; Campbell, A. The orthomolecular treatment of cancer II. Clinical trial of high-dose ascorbic acid supplements in advanced human cancer. Chem.-Biol. Interact. 1974, 9, 285–315. [Google Scholar] [CrossRef]
- Cameron, E.; Campbell, A.; Jack, T. The orthomolecular treatment of cancer. Chem. Biol. Interact. 1975, 11, 387–393. [Google Scholar] [CrossRef]
- Creagan, E.; Moertel, C.; O’Fallon, J.; Schutt, A.; O’Connell, M.; Rubin, J.; Frytak, S. Failure of High-Dose ASC (Ascorbic Acid) Therapy to Benefit Patients with Advanced Cancer. N. Engl. J. Med. 1979, 301, 687–690. [Google Scholar] [CrossRef] [PubMed]
- Moertel, C.; Fleming, T.; Creagan, E.; Rubin, J.; O’Connell, M.; Ames, M. High-Dose ASC versus Placebo in the Treatment of Patients with Advanced Cancer Who Have Had No Prior Chemotherapy. N. Engl. J. Med. 1985, 312, 137–141. [Google Scholar] [CrossRef] [PubMed]
- Lykkesfeldt, J. On the effect of vitamin C intake on human health: How to (mis)interprete the clinical evidence. Redox Biol. 2020, 34, 101532. [Google Scholar] [CrossRef] [PubMed]
- Rowe, S.; Carr, A.C. Global Vitamin C Status and Prevalence of Deficiency: A Cause for Concern? Nutrients 2020, 12, 2008. [Google Scholar] [CrossRef]
- Padayatty, S.; Sun, H.; Wang, Y.; Riordan, H.; Hewitt, S.; Katz, A.; Wesley, R.; Levine, M. ASC Pharmacokinetics: Implications for Oral and Intravenous Use. Ann. Intern. Med. 2004, 140, 533. [Google Scholar] [CrossRef]
- Chen, Q.; Espey, M.; Krishna, M.; Mitchell, J.; Corpe, C.; Buettner, G.; Shacter, E.; Levine, M. Pharmacologic ascorbic acid concentrations selectively kill cancer cells: Action as a pro-drug to deliver hydrogen peroxide to tissues. Proc. Natl. Acad. Sci. USA 2005, 102, 13604–13609. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Q.; Espey, M.; Sun, A.; Lee, J.; Krishna, M.; Shacter, E.; Choyke, P.; Pooput, C.; Kirk, K.; Buettner, G.; et al. Ascorbate in pharmacologic concentrations selectively generates ascorbate radical and hydrogen peroxide in extracellular fluid in vivo. Proc. Natl. Acad. Sci. USA 2007, 104, 8749–8754. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Q.; Espey, M.; Sun, A.; Pooput, C.; Kirk, K.; Krishna, M.; Khosh, D.; Drisko, J.; Levine, M. Pharmacologic doses of ascorbate act as a prooxidant and decrease growth of aggressive tumor xenografts in mice. Proc. Natl. Acad. Sci. USA 2008, 105, 11105–11109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verrax, J.; Calderon, P. Pharmacologic concentrations of ascorbate are achieved by parenteral administration and exhibit antitumoral effects. Free Radic. Biol. Med. 2009, 47, 32–40. [Google Scholar] [CrossRef]
- Du, J.; Martin, S.; Levine, M.; Wagner, B.; Buettner, G.; Wang, S.; Taghiyev, A.; Du, C.; Knudson, C.; Cullen, J. Mechanisms of Ascorbate-Induced Cytotoxicity in Pancreatic Cancer. Clin. Cancer Res. 2010, 16, 509–520. [Google Scholar] [CrossRef] [Green Version]
- Takemura, Y.; Satoh, M.; Satoh, K.; Hamada, H.; Sekido, Y.; Kubota, S. High dose of ascorbic acid induces cell death in mesothelioma cells. Biochem. Biophys. Res. Commun. 2010, 394, 249–253. [Google Scholar] [CrossRef]
- Hong, S.; Lee, S.; Moon, J.; Hwang, J.; Kim, D.; Ko, E.; Kim, H.; Cho, I.; Kang, J.; Kim, D.; et al. SVCT-2 in breast cancer acts as an indicator for L-ascorbate treatment. Oncogene 2012, 32, 1508–1517. [Google Scholar] [CrossRef] [Green Version]
- Espey, M.; Chen, P.; Chalmers, B.; Drisko, J.; Sun, A.; Levine, M.; Chen, Q. Pharmacologic ascorbate synergizes with gemcitabine in preclinical models of pancreatic cancer. Free Radic. Biol. Med. 2011, 50, 1610–1619. [Google Scholar] [CrossRef] [Green Version]
- Ma, Y.; Chapman, J.; Levine, M.; Polireddy, K.; Drisko, J.; Chen, Q. High-Dose Parenteral Ascorbate Enhanced Chemosensitivity of Ovarian Cancer and Reduced Toxicity of Chemotherapy. Sci. Transl. Med. 2014, 6, ra18–ra222. [Google Scholar] [CrossRef]
- Hatem, E.; Azzi, S.; El Banna, N.; He, T.; Heneman-Masurel, A.; Vernis, L.; Baïlle, D.; Masson, V.; Dingli, F.; Loew, D.; et al. Auranofin/ASC: A Novel Drug Combination Targeting Triple-Negative Breast Cancer. J. Natl. Cancer Inst. 2018, 111, 597–608. [Google Scholar] [CrossRef]
- O’Leary, B.; Houwen, F.; Johnson, C.; Allen, B.; Mezhir, J.; Berg, D.; Cullen, J.; Spitz, D. Pharmacological Ascorbate as an Adjuvant for Enhancing Radiation-Chemotherapy Responses in Gastric Adenocarcinoma. Radiat. Res. 2018, 189, 456. [Google Scholar] [CrossRef] [PubMed]
- Graczyk-Jarzynka, A.; Goral, A.; Muchowicz, A.; Zagozdzon, R.; Winiarska, M.; Bajor, M.; Trzeciecka, A.; Fidyt, K.; Krupka, J.; Cyran, J.; et al. Inhibition of thioredoxin-dependent H2O2 removal sensitizes malignant B-cells to pharmacological ascorbate. Redox Biol. 2019, 21, 101062. [Google Scholar] [CrossRef] [PubMed]
- Du, J.; Cieslak, J.; Welsh, J.; Sibenaller, Z.; Allen, B.; Wagner, B.; Kalen, A.; Doskey, C.; Strother, R.; Button, A.; et al. Pharmacological Ascorbate Radiosensitizes Pancreatic Cancer. Cancer Res. 2015, 75, 3314–3326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, Y.; Wu, Q.; Chen, D.; Chen, L.; Wang, Z.; Ren, C.; Mo, H.; Chen, Y.; Sheng, H.; Wang, Y.; et al. Pharmacological Ascorbate Suppresses Growth of Gastric Cancer Cells with GLUT1 Overexpression and Enhances the Efficacy of Oxaliplatin Through Redox Modulation. Theranostics 2018, 8, 1312–1326. [Google Scholar] [CrossRef] [Green Version]
- El Banna, N.; Hatem, E.; Heneman-Masurel, A.; Léger, T.; Baïlle, D.; Vernis, L.; Garcia, C.; Martineau, S.; Dupuy, C.; Vagner, S.; et al. Redox modifications of cysteine-containing proteins, cell cycle arrest and translation inhibition: Involvement in ASC-induced breast cancer cell death. Redox Biol. 2019, 26, 101290. [Google Scholar] [CrossRef]
- Padayatty, S. Intravenously administered ASC as cancer therapy: Three cases. Can. Med. Assoc. J. 2006, 174, 937–942. [Google Scholar] [CrossRef] [Green Version]
- Hoffer, L.; Levine, M.; Assouline, S.; Melnychuk, D.; Padayatty, S.; Rosadiuk, K.; Rousseau, C.; Robitaille, L.; Miller, W. Phase I clinical trial of i.v. ascorbic acid in advanced malignancy. Ann. Oncol. 2008, 19, 1969–1974. [Google Scholar] [CrossRef]
- Vollbracht, C.; Schneider, B.; Leendert, V.; Weiss, G.; Auerbach, L.; Beuth, J. Intravenous ASC administration improves quality of life in breast cancer patients during chemo-/radiotherapy and aftercare: Results of a retrospective, multicentre, epidemiological cohort study in Germany. In Vivo 2011, 25, 983–990. [Google Scholar]
- Takahashi, H.; Mizuno, H.; Yanagisawa, A. High-dose intravenous ASC improves quality of life in cancer patients. Personal. Med. Univ. 2012, 1, 49–53. [Google Scholar] [CrossRef]
- Stephenson, C.; Levin, R.; Spector, T.; Lis, C. Phase I clinical trial to evaluate the safety, tolerability, and pharmacokinetics of high-dose intravenous ascorbic acid in patients with advanced cancer. Cancer Chemother. Pharmacol. 2013, 72, 139–146. [Google Scholar] [CrossRef] [Green Version]
- Monti, D.; Mitchell, E.; Bazzan, A.; Littman, S.; Zabrecky, G.; Yeo, C.; Pillai, M.; Newberg, A.; Deshmukh, S.; Levine, M. Phase I Evaluation of Intravenous Ascorbic Acid in Combination with Gemcitabine and Erlotinib in Patients with Metastatic Pancreatic Cancer. PLoS ONE 2012, 7, e29794. [Google Scholar] [CrossRef] [PubMed]
- Welsh, J.; Wagner, B.; van’t Erve, T.; Zehr, P.; Berg, D.; Halfdanarson, T.; Yee, N.; Bodeker, K.; Du, J.; Roberts, L.; et al. Pharmacological ascorbate with gemcitabine for the control of metastatic and node-positive pancreatic cancer (PACMAN): Results from a phase I clinical trial. Cancer Chemother. Pharmacol. 2013, 71, 765–775. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoffer, L.; Robitaille, L.; Zakarian, R.; Melnychuk, D.; Kavan, P.; Agulnik, J.; Cohen, V.; Small, D.; Miller, W. High-Dose Intravenous ASC Combined with Cytotoxic Chemotherapy in Patients with Advanced Cancer: A Phase I-II Clinical Trial. PLoS ONE 2015, 10, e0120228. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, T.; Højgaard, M.; Andersen, J.; Jørgensen, N.; Zerahn, B.; Kristensen, B.; Henriksen, T. Weekly ascorbic acid infusion in castration-resistant prostate cancer patients: A single-arm phase II trial. Transl. Androl. Urol. 2017, 6, 517–528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schoenfeld, J.; Sibenaller, Z.; Mapuskar, K.; Wagner, B.; Cramer-Morales, K.; Furqan, M.; Sandhu, S.; Carlisle, T.; Smith, M.; Abu Hejleh, T.; et al. O2⋅− and H2O2- Mediated Disruption of Fe Metabolism Causes the Differential Susceptibility of NSCLC and GBM Cancer Cells to Pharmacological Ascorbate. Cancer Cell 2017, 31, 487–500.e8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polireddy, K.; Dong, R.; Reed, G.; Yu, J.; Chen, P.; Williamson, S.; Violet, P.; Pessetto, Z.; Godwin, A.; Fan, F.; et al. High Dose Parenteral Ascorbate Inhibited Pancreatic Cancer Growth and Metastasis: Mechanisms and a Phase I/IIa study. Sci. Rep. 2017, 7, 17188. [Google Scholar] [CrossRef] [Green Version]
- Zhao, H.; Zhu, H.; Huang, J.; Zhu, Y.; Hong, M.; Zhu, H.; Zhang, J.; Li, S.; Yang, L.; Lian, Y.; et al. The synergy of ASC with decitabine activates TET2 in leukemic cells and significantly improves overall survival in elderly patients with acute myeloid leukemia. Leuk. Res. 2018, 66, 1–7. [Google Scholar] [CrossRef]
- Lv, H.; Wang, C.; Fang, T.; Li, T.; Lv, G.; Han, Q.; Yang, W.; Wang, H. ASC preferentially kills cancer stem cells in hepatocellular carcinoma via SVCT-2. Precis. Oncol. 2018, 2, 1. [Google Scholar] [CrossRef] [Green Version]
- Wang, F.; He, M.; Wang, Z.; Li, S.; Jin, Y.; Ren, C.; Shi, S.; Bi, B.; Chen, S.; Lv, Z.; et al. Phase I study of high-dose ascorbic acid with mFOLFOX6 or FOLFIRI in patients with metastatic colorectal cancer or gastric cancer. BMC Cancer 2019, 19, 460. [Google Scholar] [CrossRef]
- Fritz, H.; Flower, G.; Weeks, L.; Cooley, K.; Callachan, M.; McGowan, J.; Skidmore, B.; Kirchner, L.; Seely, D. Intravenous ASC and Cancer. Integr. Cancer Ther. 2014, 13, 280–300. [Google Scholar] [CrossRef]
- Jacobs, C.; Hutton, B.; Ng, T.; Shorr, R.; Clemons, M. Is There a Role for Oral or Intravenous Ascorbate (ASC) in Treating Patients with Cancer? A Systematic Review. Oncologist 2015, 20, 210–223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carr, A.; Cook, J. Intravenous ASC for Cancer Therapy—Identifying the Current Gaps in Our Knowledge. Front. Physiol. 2018, 9. [Google Scholar] [CrossRef] [PubMed]
- Nauman, G.; Gray, J.; Parkinson, R.; Levine, M.; Paller, C. Systematic Review of Intravenous Ascorbate in Cancer Clinical Trials. Antioxidants 2018, 7, 89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iddir, M.; Brito, A.; Dingeo, G.; Fernandez Del Campo, S.S.; Samouda, H.; La Frano, M.R.; Bohn, T. Strengthening the Immune System and Reducing Inflammation and Oxidative Stress through Diet and Nutrition: Considerations during the COVID-19 Crisis. Nutrients 2020, 12, 1562. [Google Scholar] [CrossRef]
- Wu, R.; Wang, L.; Kuo, H.-C.D.; Shannar, A.; Peter, R.; Chou, P.J.; Li, S.; Hudlikar, R.; Liu, X.; Liu, Z.; et al. An Update on Current Therapeutic Drugs Treating COVID-19. Curr. Pharmacol. Rep. 2020, 6, 1–15. [Google Scholar] [CrossRef]
- Lozano-Sepulveda, S.A.; Bryan-Marrugo, O.L.; Cordova-Fletes, C.; Gutierrez-Ruiz, M.C.; Rivas-Estilla, A.M. Oxidative stress modulation in hepatitis C virus infected cells. World J. Hepatol. 2015, 7, 2880–2889. [Google Scholar] [CrossRef]
- Carr, A.C. A new clinical trial to test high-dose ASC in patients with COVID-19. Crit. Care 2020, 24, 133. [Google Scholar] [CrossRef] [Green Version]
- Tan, S.H.S.; Hong, C.C.; Saha, S.; Murphy, D.; Hui, J.H. Medications in COVID-19 patients: Summarizing the current literature from an orthopaedic perspective. Int. Orthop. 2020, 12, e7560. [Google Scholar] [CrossRef]
- Jalloh, M.A.; Gregory, P.J.; Hein, D.; Risoldi Cochrane, Z.; Rodriguez, A. Dietary supplement interactions with antiretrovirals: A systematic review. Int. J. STD AIDS 2017, 28, 4–15. [Google Scholar] [CrossRef]
- Musisi, E.; Matovu, D.K.; Bukenya, A.; Kaswabuli, S.; Zawedde, J.; Andama, A.; Byanyima, P.; Sanyu, I.; Sessolo, A.; Seremba, E.; et al. Effect of anti-retroviral therapy on oxidative stress in hospitalized HIV-infected adults with and without TB. Afr. Health Sci. 2018, 18, 512–522. [Google Scholar] [CrossRef] [Green Version]
- Ceccarelli, M.; Condorelli, F.; VenanziRullo, E.; Pellicanò, G.F. Editorial—Improving access and adherence to screening tests for cancers: A new, though old, challenge in the HIV epidemics. World Cancer Res. J. 2018, 5, e1030. [Google Scholar]
- Ceccarelli, M.; VenanziRullo, E.; Facciolà, A.; Madeddu, G.; Cacopardo, B.; Taibi, R.; D’Aleo, F.; Pinzone, M.R.; Picerno, I.; Di Rosa, M.; et al. Head and neck squamous cell carcinoma and its correlation with human papillomavirus in people living with HIV: A systematic review. Oncotarget 2018, 9, 17171–17180. [Google Scholar] [CrossRef] [PubMed]
- Ceccarelli, M.; Venanzi Rullo, E.; Vaccaro, M.; Facciolà, A.; D’Aleo, F.; Paolucci, I.A.; Cannavò, S.P.; Cacopardo, B.; Pinzone, M.R.; Pellicanò, G.F.; et al. HIV-associatedpsoriasis: Epidemiology, pathogenesis, and management. Dermatol. Ther. 2019, 32, e12806. [Google Scholar] [CrossRef] [PubMed]
- Ceccarelli, M.; Venanzi Rullo, E.; Marino, M.A.; D’Aleo, F.; Pellicanò, G.F.; D’Andrea, F.; Marino, A.; Cacopardo, B.; Celesia, B.M.; La Rocca, G.; et al. Non-AIDS defining cancers: A comprehensive update on diagnosis and management. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 3849–3875. [Google Scholar]
- Ceccarelli, M.; Facciolà, A.; Taibi, R.; Pellicanò, G.F.; Nunnari, G.; VenanziRullo, E. The treatment of Kaposi’s sarcoma: Present and future options, a review of the literature. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 7488–7497. [Google Scholar]
- D’Aleo, F.; Ceccarelli, M.; VenanziRullo, E.; Facciolà, A.; D’Andrea, F.; Micali, C.; Coco, M.; Pinzone, M.R.; Focà, E.; Condorelli, F.; et al. Anal cancer in people living with HIV: The importance of the screening and of early diagnosis. World Cancer Res. J. 2019, 6, e1319. [Google Scholar]
- D’Andrea, F.; Ceccarelli, M.; Facciolà, A.; Nunnari, G.; Pellicanò, G.F.; VenanziRullo, E. Breast cancer in women living with HIV. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 1158–1164. [Google Scholar]
- D’Andrea, F.; Ceccarelli, M.; VenanziRullo, E.; Facciolà, A.; D’Aleo, F.; Cacopardo, B.; Iacobello, C.; Costa, A.; Altavilla, G.; Pellicanò, G.F.; et al. Cancer screening in HIV-infected patients: Early diagnosis in a high-risk population. World Cancer Res. J. 2018, 5, e1130. [Google Scholar]
- D’Andrea, F.; Pellicanò, G.F.; Venanzi Rullo, E.; D’Aleo, F.; Facciolà, A.; Micali, C.; Coco, M.; Visalli, G.; Picerno, I.; Condorelli, F.; et al. Cervical cancer in women living with HIV: A review of the literature. World Cancer Res. J. 2019, 6, e1224. [Google Scholar]
- Pinzone, M.R.; Ceccarelli, M.; VenanziRullo, E.; Maresca, M.; Bruno, R.; Condorelli, F.; Di Rosa, M.; Madeddu, G.; Focà, E.; Calcagno, A.; et al. Circulating angiopoietin-like protein 2 levels are associated with decreased renal function in HIV+ subjects on cART: A potential marker of kidney disease. Biomed. Rep. 2019, 10, 140–144. [Google Scholar]
- D’Andrea, F.; VenanziRullo, E.; Facciolà, A.; Di Rosa, M.; Condorelli, F.; Marino, A.; Cacopardo, B.; Pellicanò, G.F.; Nunnari, G.; Ceccarelli, M. Epstein Barr Virus related cancer in people living with HIV: A review of the literature. World Cancer Res. J. 2020, 7, e1512. [Google Scholar]
- D’Andrea, F.; Venanzi Rullo, E.; Marino, A.; Moscatt, V.; Celesia, B.M.; Cacopardo, B.; Condorelli, F.; La Rocca, G.; Di Rosa, M.; Pellicanò, G.F.; et al. Hepatitis B virus infection and hepatocellular carcinoma in PLWH: Epidemiology, pathogenesis and treatment. World Cancer Res. J. 2020, 7, e1537. [Google Scholar]
- D’Aleo, F.; Ceccarelli, M.; Venanzi Rullo, E.; Facciolà, A.; Di Rosa, M.; Pinzone, M.R.; Condorelli, F.; Visalli, G.; Picerno, I.; Berretta, M.; et al. Hepatitis C-related hepatocellular carcinoma: Diagnostic and therapeutic management in HIV-patients. Eur. Rev. Med. Pharmacol. Sci. 2017, 21, 5859–5867. [Google Scholar] [PubMed]
- D’Aleo, F.; Venanzi Rullo, E.; Ceccarelli, M.; Facciolà, A.; Condorelli, F.; Pinzone, M.R.; Cacopardo, B.; Di Rosa, M.; Nunnari, G.; Pellicanò, G.F. HIV and colorectal cancer. New insights and review of the literature. World Cancer Res. J. 2018, 5, e1122. [Google Scholar]
- Facciolà, A.; VenanziRullo, E.; Ceccarelli, M.; D’Aleo, F.; D’Andrea, F.; Visalli, G.; Pinzone, M.R.; Picerno, I.; Cacopardo, B.; Condorelli, F.; et al. Hodgkin’s lymphoma in people living with HIV: Epidemiology and clinical management. World Cancer Res. J. 2019, 6, e1295. [Google Scholar]
- Facciolà, A.; Venanzi Rullo, E.; Ceccarelli, M.; D’Aleo, F.; Di Rosa, M.; Pinzone, M.R.; Condorelli, F.; Visalli, G.; Picerno, I.; Fisichella, R.; et al. Kaposi’s sarcoma in HIV-infected patients in the era of new antiretrovirals. Eur. Rev. Med. Pharmacol. Sci. 2017, 21, 5868–5879. [Google Scholar]
- Facciolà, A.; Venanzi Rullo, E.; Ceccarelli, M.; D’Andrea, F.; Coco, M.; Micali, C.; Cacopardo, B.; Marino, A.; Cannavò, S.P.; Di Rosa, M.; et al. Malignant melanoma in HIV: Epidemiology, pathogenesis, and management. Dermatol. Ther. 2020, 33, e13180. [Google Scholar] [CrossRef]
- D’Aleo, F.; Cama, B.A.V.; Paolucci, I.A.; Venanzi Rullo, E.; Condorelli, F.; Facciolà, A.; Di Francia, R.; Savasta, A.; Pinzone, M.R.; Picerno, I.; et al. New and old assumptions on lung cancer in People Living with HIV. World Cancer Res. 2018, 5, e1036. [Google Scholar]
- Facciolà, A.; Ceccarelli, M.; Venanzi Rullo, E.; D’Aleo, F.; Condorelli, F.; Visalli, G.; Cacopardo, B.; Pinzone, M.R.; Di Rosa, M.; Nunnari, G.; et al. Prostate cancer in HIV-positive patients—A review of the literature. World Cancer Res. J. 2018, 5, e1136. [Google Scholar]
- Schwenger, K.J.P.; Arendt, B.M.; Smieja, M.; Ma, D.W.L.; Smaill, F.; Allard, J.P. Relationships between Atherosclerosis and Plasma Antioxidant Micronutrients or Red Blood Cell Polyunsaturated Fatty Acids in People Living with HIV. Nutrients 2019, 11, 1292. [Google Scholar] [CrossRef] [Green Version]
- Makinde, O.; Rotimi, K.; Ikumawoyi, V.; Adeyemo, T.; Olayemi, S. Effect of vitamin A and ASC supplementation on oxidative stress in HIV and HIV-TB co-infection at Lagos University Teaching Hospital (LUTH) Nigeria. Afr. Health Sci. 2017, 17, 308–314. [Google Scholar] [CrossRef] [PubMed]
- Bordes, C.; Leguelinel-Blache, G.; Lavigne, J.P.; Mauboussin, J.M.; Laureillard, D.; Faure, H.; Rouanet, I.; Sotto, A.; Loubet, P. Interactions between antiretroviral therapy and complementary and alternative medicine: A narrative review. Clin. Microbiol. Infect. 2020, in press. [Google Scholar] [CrossRef] [PubMed]
- Madill, J.; Arendt, B.M.; Aghdassi, E.; Therapondos, G.; Lilly, L.; Chow, C.W.; Guindi, M.; Allard, J.P. Hepatic Lipid Peroxidation and Antioxidant Micronutrients in Hepatitis Virus C Liver Recipients with and Without Disease Recurrence. Transplant. Proc. 2009, 41, 3800–3805. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez, J.A.; Nespereira, B.; Pérez-Ilzarbe, M.; Eguinoa, E.; Páramo, J.A. Vitamins C and E prevent endothelial VEGF and VEGFR-2 overexpression induced by porcine hypercholesterolemic LDL. Cardiovasc. Res. 2005, 65, 665–673. [Google Scholar] [CrossRef] [Green Version]
- Gonçalves, D.; Lima, C.; Ferreira, P.; Costa, P.; Costa, A.; Figueiredo, W.; Cesar, T. Orange juice as dietary source of antioxidants for patients with hepatitis C under antiviral therapy. Food Nutr. Res. 2017, 61, 1296675. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.-C.; Yin, M.-C. Vitamins B depletion, lower iron status and decreased antioxidative defense in patients with chronic hepatitis C treated by pegylated interferon alfa and ribavirin. Clin. Nutr. 2009, 28, 34–38. [Google Scholar] [CrossRef] [PubMed]
- Loguercio, C.; Cuomo, A.; Tuccillo, C.; Gazzerro, P.; Cioffi, M.; Molinari, A.M.; Del Vecchio Blanco, C. Liver p53 expression in patients with HCV-related chronich epatitis. J. Viral Hepat. 2003, 10, 266–270. [Google Scholar] [CrossRef] [PubMed]
- Lee, V.; Goyal, A.; Hsu, C.C.; Jacobson, J.S.; Rodriguez, R.D.; Siegel, A.B. Dietary Supplement Use Among Patients with Hepatocellular Carcinoma. Integr. Cancer Ther. 2014, 14, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Adams, K.K.; Baker, W.L.; Sobieraj, D.M. Myth Busters: Dietary Supplements and COVID-19. Ann. Pharmacother. 2020, 54, 820–826. [Google Scholar] [CrossRef]
- Kakodkar, P.; Kaka, N.; Baig, M.N. A Comprehensive Literature Review on the Clinical Presentation, and Management of the Pandemic Coronavirus Disease 2019 (COVID-19). Cureus 2020, 12, e7560. [Google Scholar] [CrossRef] [Green Version]
- Hemilä, H.; Chalker, E. ASC as a Possible Therapy for COVID-19. Infect. Chemother. 2020, 52, 222–223. [Google Scholar] [CrossRef] [PubMed]
- Moser, M.A.; Chun, O.K. ASC and Heart Health: A Review Based on Findings from Epidemiologic Studies. Int. J. Mol. Sci. 2016, 17, 1328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Khudairy, L.; Flowers, N.; Wheelhouse, R.; Ghannam, O.; Hartley, L.; Stranges, S.; Rees, K. ASC supplementation for the primary prevention of cardiovascular disease. Cochrane Database Syst. Rev. 2017, 3, CD011114. [Google Scholar] [PubMed] [Green Version]
- Ashor, A.W.; Lara, J.; Mathers, J.C.; Siervo, M. Effect of ASC on endothelial function in health and disease: A systematic review and meta-analysis of randomised controlled trials. Atherosclerosis 2014, 235, 9–20. [Google Scholar] [CrossRef] [PubMed]
- Martín-Calvo, N.; Martínez-González, M.Á. ASC Intake is Inversely Associated with Cardiovascular Mortality in a Cohort of Spanish Graduates: The SUN Project. Nutrients 2017, 9, 954. [Google Scholar] [CrossRef] [Green Version]
- Sabri, M.; Ghaffari, G.; Hashemipour, M.; Mostofizadeh, N.; Koushki, A.M. Effect of long-term ASC intake on vascular endothelial function in diabetic children and adolescents: A pilot study. J. Res. Med. Sci. 2016, 21, 119. [Google Scholar]
- Fouladvand, F.; Falahi, E.; Asbaghi, O.; Abbasnezhad, A. Effect of Vitamins C and E Co-Supplementation on Serum C-Reactive Protein Level: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Prev. Nutr. Food Sci. 2020, 25, 1–8. [Google Scholar] [CrossRef]
- Guan, Y.; Dai, P.; Wang, H. Effects of ASC supplementation on essential hypertension: A systematic review and meta-analysis. Medicine (Baltimore) 2020, 99, e19274. [Google Scholar] [CrossRef]
- Wilkinson, I.B.; Megson, I.L.; MacCallum, H.; Sogo, N.; Cockcroft, J.R.; Webb, D.J. Oral ASC reduces arterial stiffness and platelet aggregation in humans. J. Cardiovasc. Pharmacol. 1999, 34, 690–693. [Google Scholar] [CrossRef]
- Ellulu, M.S.; Rahmat, A.; Patimah, I.; Khaza’ai, H.; Abed, Y. Effect of ASC on inflammation and metabolic markers in hypertensive and/or diabetic obese adults: A randomized controlled trial. Drug Des. Dev. Ther. 2015, 9, 3405–3412. [Google Scholar] [CrossRef] [Green Version]
- Thosar, S.S.; Bielko, S.L.; Wiggins, C.C.; Klaunig, J.E.; Mather, K.J.; Wallace, J.P. Antioxidant ASC prevents decline in endothelial function during sitting. Med. Sci. Monit. 2015, 21, 1015–1021. [Google Scholar] [PubMed] [Green Version]
- Siavash, M.; Amini, M. ASC may have similar beneficial effects to Gemfibrozil on serum high-density lipoprotein-cholesterol in type 2 diabetic patients. J. Res. Pharm. Pract. 2014, 3, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Juraschek, S.P.; Guallar, E.; Appel, L.J.; Miller, E.R., 3rd. Effects of ASC supplementation on blood pressure: A meta-analysis of randomized controlled trials. Am. J. Clin. Nutr. 2012, 95, 1079–1088. [Google Scholar] [CrossRef] [PubMed]
- Barbarisi, M.; Barbarisi, A.; De Sena, G.; Armenia, E.; Aurilio, C.; Libutti, M.; Iaffaioli, R.V.; Botti, G.; Maurea, N.; Quagliariello, V. Boswellic acid has anti-inflammatory effects and enhances the anticancer activities of Temozolomide and Afatinib, an irreversible ErbB family blocker, in human glioblastoma cells. Phytother. Res. 2019, 33, 1670–1682. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.S.; de Mattos, A.B.; Shao, D.; Li, T.; Nabben, M.; Kim, M.; Wang, W.; Tian, R.; Kolwicz, S.C., Jr. Preservation of myocardial fatty acid oxidation prevents diastolic dysfunction in mice subjected to angiotensin II infusion. J. Mol. Cell Cardiol. 2016, 100, 64–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, N.; Jiang, W.; Wang, Y.; Wu, Y.; Chen, H.; Zhao, X. Plasma levels of free fatty acid differ in patients with left ventricular preserved, mid-range, and reduced ejection fraction. BMC Cardiovasc. Disord. 2018, 18, 104. [Google Scholar] [CrossRef]
- Quagliariello, V.; Passariello, M.; Coppola, C.; Rea, D.; Barbieri, A.; Scherillo, M.; Monti, M.G.; Iaffaioli, R.V.; De Laurentiis, M.; Ascierto, P.A.; et al. Cardiotoxicity and pro-inflammatory effects of the immune checkpoint inhibitor Pembrolizumab associated to Trastuzumab. Int. J. Cardiol. 2019, 292, 171–179. [Google Scholar] [CrossRef]
- Hillstrom, R.J.; Yacapin-Ammons, A.K.; Lynch, S.M. ASC inhibits lipid oxidation in human HDL. J. Nutr. 2003, 133, 3047–3051. [Google Scholar] [CrossRef] [Green Version]
- Li, X.; Huang, J.; May, J.M. Ascorbic acid spares alpha-tocopherol and decreases lipid peroxidation in neuronal cells. Biochem. Biophys. Res. Commun. 2003, 305, 656–661. [Google Scholar] [CrossRef]
- Strongman, H.; Gadd, S.; Matthews, A.; Mansfield, K.; Stanway, S.; Lyon, A.; dos-Santos-Silva, I.; Smeeth, L.; Bhaskaran, K. Medium and long-term risks of specific cardiovascular diseases in survivors of 20 adult cancers: A population-based cohort study using multiple linked UK electronic health records databases. Lancet 2019, 394, 1041–1054. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Drug | Interactions |
|---|---|
| Amphetamine | Combination with ASC can reduce serum 2,5-dimethoxy-4-ethylamphetamine and 4-bromo-2,5-dimethoxyamphetamine concentrations. |
| Aluminum hydroxide (anti-Anti-glutamic acid decarboxylase remedies) | ASC can enhance aluminum hydroxide absorption, resulting in increased serum concentrations and potentially increasing the severity of adverse effects. |
| Bleomycin | Combination with ASC can reduce drug efficacy. |
| Bortezomib | Combination with ASC can reduce drug efficacy. |
| Chlorpropamide | ASC can reduce the chlorpropamide excretion rate, potentially raising its serum levels. |
| Conjugated estrogens | They can reduce ASC concentrations. |
| Cyclosporine | Combination with ASC can reduce drug serum concentrations. |
| Deferoxamine | Combination with ASC can increase the risk/severity of cardiovascular impairment. |
| Dienestrol | It can reduce ASC serum levels. |
| Diethylpropion | Combination with ASC can reduce drug serum concentrations. |
| Diethylstilbestrol | It can reduce ASC serum levels. |
| Doxycycline | Combination with ASC can reduce drug efficacy. |
| Erythromycin | Combination with ASC can reduce drug efficacy. |
| Esterified estrogens | It can reduce ASC serum levels. |
| Estradiol | It can reduce ASC serum levels. |
| Estradiol acetate | It can reduce ASC serum levels. |
| Estradiol benzoate | It can reduce ASC serum levels. |
| Estriol | It can reduce ASC serum levels. |
| Estrone | It can reduce ASC serum levels. |
| Ethinylestradiol | It can reduce ASC serum levels. |
| Gepefrine | Combination with ASC can reduce drug serum concentrations. |
| Iofetamine I-123 | It can reduce ASC serum levels. |
| Kanamycin | Combination with ASC can reduce drug efficacy. |
| Lincomycin | Combination with ASC can reduce drug efficacy. |
| Methamphetamine | It can reduce ASC serum levels. |
| Promestriene | It can reduce ASC serum levels. |
| Quinestrol | It can reduce ASC serum levels. |
| Streptomycin | Combination with ASC can reduce drug efficacy. |
| Synthetic conjugated estrogens, A | It can reduce ASC serum levels. |
| Synthetic conjugated estrogens, B | It can reduce ASC serum levels. |
| Tibolone | It can reduce ASC serum levels. |
| Zeranol | It can reduce ASC serum levels. |
| Member Genes | Gene(s) | Epigenetic Functions | Phenotype Affected Functions |
|---|---|---|---|
| JMJCs, Jumonj C-domain-containing histone demethylases | Histone demethylase (HDAM) | Fe(II) 2-oxoglutarate-dependent ASC | Loss of H3 and H4 demethylation. Influence on oncosuppressor gene transcription and gene replication. Abnormal spermatogenesis [49]. Embryonic cardiomyopathy [50,51]. |
| TET, ten-eleven translocation | TET1, TET2, TET3 | Conversion of 5-methyl-cytosine (5mC) to 5-hydroxymethyl-cytosine (5hmC) | TET1 and TET2 reduction in 5hmC is implicated in the development of several types of lymphoid and myeloid acute leukemias. TET2 mutations are also associated with myeloid leukemias and myeloproliferative disorders [52]. |
| ABH, alkylation repair homolog | H2A demethylase | Fe(II) 2-oxoglutarate-dependent ASC | H2A selective demethylase enzyme. Placental defects [52]. |
| FTO, fat mass and obesity-associated gene | Methylase | Addition of 3 methyl groups to single-stranded DNA | Reduced expression due to the FTO rs9939609 polymorphism is associated with child obesity [49,53]. |
| Dio3 deiodinase, iodothyronine type IIIDlk1 delta-like 1 homolog | Dio3–Dlk1 gene cluster | H3 acetylation and Lys4 demethylation | Embryonic stem cell development. Reprogramming in the absence of ASC induces hypermethylation of the imprinted Dlk1–Dio3 locus [54,55]. |
| Source | Ascorbic Acid Content (mg/100 g of Product) |
|---|---|
| Acerola | 1300 |
| Apple | 2–10 |
| Apricot | 7–10 |
| Avocado | 15–20 |
| Banana | 10–30 |
| Blackberry | 15 |
| Broccoli | 113 |
| Broccoli (cooked) | 90 |
| Brussels sprouts | 87–109 |
| Cabbage (raw) | 46–47 |
| Cauliflower | 64–78 |
| Cauliflower(cooked) | 55 |
| Carrot | 6 |
| Cranberry | 12 |
| Cherry | 5–8 |
| Blackcurrant | 200–210 |
| Redcurrant | 40 |
| Damson | 3 |
| Gooseberry | 40 |
| Gourd | 8 |
| Passion fruit | 25 |
| Grapefruit | 40 |
| Guava | 230–300 |
| Horseradish | 120 |
| Kale | 186 |
| Kale (cooked) | 62 |
| Kiwi | 60 |
| Lemon | 50 |
| Lettuce | 15 |
| Lime | 25 |
| Loganberry | 30 |
| Lychee | 45 |
| Melon | 10–35 |
| Orange | 50 |
| Orange (juice) | 50 |
| Tangerine | 30 |
| Peach | 7–31 |
| Peach (canned) | 6 |
| Pepper (green) | 128 |
| Plum | 3 |
| Pea | 25 |
| Pear | 3–4 |
| Pineapple | 12–25 |
| Pineapple (canned) | 12 |
| Pomegranate | 6 |
| Potato (new) | 30 |
| Potato (Oct., Nov.) | 20 |
| Potato (Dec.) | 15 |
| Potato (Jan., Feb.) | 10 |
| Potato (Mar.–May) | 8 |
| Potato (boiled) | 16 |
| Quince | 15 |
| Raspberry | 25 |
| Rosehip | 1000 |
| Spinach | 51 |
| Spinach (cooked) | 28 |
| Strawberry | 59–60 |
| Tomato | 20–25 |
| Tomato (juice) | 16 |
| Watercress | 68–79 |
| Study | Type of Cancer | Administration | Outcomes |
|---|---|---|---|
| Padayatty, S. [110] | Advanced cancers | Intravenous administration | Increased survival |
| Hoffer, L et al. [119] | Advanced cancer or hematologic malignancy | Intravenous administration | Adverse events and toxicity were minimal |
| Vollbracht, C. et al. [120] | 125 breast cancer patients | Intravenous administration | Significant reduction incomplaints induced by the disease and chemo-/radiotherapy, in particular, nausea, loss of appetite, fatigue, depression, sleep disorders, dizziness and hemorrhagic diathesis. |
| Takahashi, H. et al. [121] | Advanced cancer patients | High-dose intravenous administration | Improved Quality of Life (QoL) in cancer patients |
| Stephenson, C. et al. [122] | Advanced cancer patients | High-dose intravenous administration | Ascorbic acid administered i.v. at 1 g/min for 4 consecutive days/week for 4 weeks produced up to 49 mM ascorbic acid in patient’s blood and was well tolerated. The recommended dose for future studies is 70–80 g/m2 |
| Monti, D. et al. [123] | Metastatic pancreatic cancer | Intravenous administration | The initial safety data do not reveal increased toxicity with the addition of ascorbic acid to gemcitabine and erlotinib in pancreatic cancer patients. |
| Welsh, J. et al. [124] | Metastatic and node-positive pancreatic cancer | Intravenous administration | Data suggest pharmacologic ascorbate administered concurrently with gemcitabine is well-tolerated. Initial data from this small sampling suggest some efficacy. |
| Hoffer, L. et al. [125] | Advanced cancer patients | High-dose intravenous administration | ASC was safe and generally well tolerated. The pre- and post-chemotherapy pharmacokinetic profiles suggested that tissue uptake of ASC increases after chemotherapy, with no increase in urinary oxalic acid excretion. |
| Nielsen, T. et al. [126] | Castration-resistant prostate cancer patients | Intravenous administration | Treatment with ASC did not result in disease remission. |
| Polireddy, K. et al. [128] | Pancreatic cancer patients | High-dose intravenous administration | Treatment with ASC was safe in patients and showed the possibility to prolong patient survival. There was no interference with gemcitabine pharmacokinetics by ASC administration. |
| Zhao, H. et al. [129] | Patients with acute myeloid leukemia | Intravenous administration | Patients who received ASC + DCAG (decitabine with cytarabine, aclarubicin hydrochloride, and granulocyte colony-stimulating factor) regimen had a higher complete remission (CR) rate than those who received the DCAG regimen (79.92% vs. 44.11%; p = 0.004) after one cycle of chemotherapy. The median overall survival (OS) was better in the ASC-DCAG group compared with the DCAG group (15.3 months vs. 9.3 months, p = 0.039). |
| Lv, H. et al. [130] | Hepatocellular carcinoma | Intravenous administration | Administration of ASC improved disease-free survival (DFS) in hepatocellular carcinoma patients (adjusted HR = 0.622, 95% CI = 0.487 to 0.795, p < 0.001) |
| Wang, F. et al. [131] | Metastatic colorectal cancer or gastric cancer | Intravenous administration | The favorable safety profile and preliminary efficacy of ASC plus mFOLFOX6/FOLFIRI support further evaluation of this combination in patients with metastatic colorectal cancer or gastric cancer |
| Fritz, H. et al. [132] | Cancer patients | Intravenous administration | Good safety profile and potentially important antitumor activity. ASC administration may improve the quality of life and symptom severity of patients with cancer, and several cases of cancer remission have been reported. |
| Jacobs, C. et al. [133] | Cancer patients | Intravenous administration | No high-quality evidence to suggest that ASC supplementation in cancer patients either enhances the antitumor effects of chemotherapy or reduces its toxicity. |
| Nauman, G. et al. [135] | Cancer patients | Intravenous administration | An 8.75 month increase in progression-free survival (PFS) and an improved trend in overall survival (OS) in the ASC-treated arm were seen |
| Study | Type of Patients | Administration | Outcomes |
|---|---|---|---|
| Carr, A.C. [139] | Infection diseases | Not applicable (N.A) | Low levels of ASC were proportional to infection disease severity |
| Tan, S.H.S. et al. [140] | Acute and chronic viral infectious | Intravenous administration | Protective effects with improvement of oxidative damage |
| Musisi, E. et al. [142] | HIV-infected subjects | N.A | High oxidative stress in hospitalized HIV-infected adults; ASC (p < 0.0001) and albumin (p < 0.01) were lower in HIV-patients relative to controls. |
| Ceccarelli, M. et al. [143] | Advanced cancer patients | High-dose intravenous administration | Improved QoL in cancer patients |
| Ceccarelli, M. et al. [144] | Advanced cancer patients | High-dose intravenous administration | Ascorbic acid administered i.v. at 1 g/min for 4 consecutive days/week for 4 weeks produced up to 49 mM ascorbic acid in patient’s blood and was well tolerated. The recommended dose for future studies is 70–80 g/m2 |
| Ceccarelli, M. et al. [145] | Metastatic pancreatic cancer | Intravenous administration | The initial safety data do not reveal increased toxicity with the addition of ascorbic acid to gemcitabine and erlotinib in pancreatic cancer patients. |
| Ceccarelli, M. et al. [146] | Metastatic and node-positive pancreatic cancer | Intravenous administration | Data suggest pharmacologic ascorbate administered concurrently with gemcitabine is well-tolerated. Initial data from this small sampling suggest some efficacy. |
| Makinde, O. et al. [163] | Patients with HIV | Oral administration | Exogenous antioxidant supplementation with ACS did not increase the antioxidant status in patients with HIV |
| Madill, J. et al. [164] | Patients with hepatitis virus C | N.A | Oxidative stress was independently associated with recurrence of hepatitis virus C infection. |
| Gonçalves, D. et al. [167] | Patients with hepatitis C under antiviral therapy | Oral administration of orange juice | The serum levels of total cholesterol, LDL-cholesterol, c-reacrive protein (CRP) and parameters of oxidative stress decreased in patients receiving orange juice. Moreover, alanine aminotransferase (AST) levels decreased significantly after oral administration of orange juice. |
| Adams, K.K. et al. [171] | Patients with COVID-19 | Intravenous administration | Large doses of ASC (10,000–20,000 mg/d) led to a shorter mean hospital length of stay compared with untreated patients with COVID-19 and no incidences of death |
| Study | Type of Patients | Administration | Outcomes |
|---|---|---|---|
| Ashor, A.W. et al. [176] | Patients with CVD | Oral administration | ASC reduces blood pressure and increases endothelial function in humans |
| Martín-Calvo, N. et al. [177] | Patients with CVD | Oral administration | Low ASC plasma levels increase the risk of CVD in men and women. ASC intake is inversely associated with cardiovascular mortality |
| Sabri, M. et al. [178] | Diabetic children and adolescents | Oral administration | Long-term ASC intake induced beneficial effects on vascular endothelial function, lipid profiles, and arterial stiffness |
| Martín-Calvo, N. et al. [180] | Patients with CVD | Oral administration | Reduction in arterial stiffness and enhanced endothelial function |
| Wilkinson, I.B. et al. [181] | Patients with CVD | Oral administration | Oral ASC reduces arterial stiffness and platelet aggregation |
| Thosar, S.S. et al. [183] | Patients with CVD | Oral administration | ASC prevents decline in endothelial function during sitting |
| Siavash, M. et al. [184] | Diabetic patients | Oral administration | ASC increases HDL cholesterol and reduces systolic and diastolic blood pressure |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Berretta, M.; Quagliariello, V.; Maurea, N.; Di Francia, R.; Sharifi, S.; Facchini, G.; Rinaldi, L.; Piezzo, M.; Manuela, C.; Nunnari, G.; et al. Multiple Effects of Ascorbic Acid against Chronic Diseases: Updated Evidence from Preclinical and Clinical Studies. Antioxidants 2020, 9, 1182. https://doi.org/10.3390/antiox9121182
Berretta M, Quagliariello V, Maurea N, Di Francia R, Sharifi S, Facchini G, Rinaldi L, Piezzo M, Manuela C, Nunnari G, et al. Multiple Effects of Ascorbic Acid against Chronic Diseases: Updated Evidence from Preclinical and Clinical Studies. Antioxidants. 2020; 9(12):1182. https://doi.org/10.3390/antiox9121182
Chicago/Turabian StyleBerretta, Massimiliano, Vincenzo Quagliariello, Nicola Maurea, Raffaele Di Francia, Saman Sharifi, Gaetano Facchini, Luca Rinaldi, Michela Piezzo, Ceccarelli Manuela, Giuseppe Nunnari, and et al. 2020. "Multiple Effects of Ascorbic Acid against Chronic Diseases: Updated Evidence from Preclinical and Clinical Studies" Antioxidants 9, no. 12: 1182. https://doi.org/10.3390/antiox9121182
APA StyleBerretta, M., Quagliariello, V., Maurea, N., Di Francia, R., Sharifi, S., Facchini, G., Rinaldi, L., Piezzo, M., Manuela, C., Nunnari, G., & Montopoli, M. (2020). Multiple Effects of Ascorbic Acid against Chronic Diseases: Updated Evidence from Preclinical and Clinical Studies. Antioxidants, 9(12), 1182. https://doi.org/10.3390/antiox9121182