Associations between Coenzyme Q10 Status, Oxidative Stress, and Muscle Strength and Endurance in Patients with Osteoarthritis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Study Design
2.2. Data Collection and Biochemical Analysis
2.3. Oxidative Stress and Antioxidant Capacity Measurements
2.4. Coenzyme Q10 Status Measurement
2.5. Muscle Strength and Endurance Assessments
2.6. Statistical Analysis
3. Results
3.1. Subjects’ Characteristics
3.2. The Coenzyme Q10 Status, Oxidative Stress, and Antioxidant Capacity of the Subjects
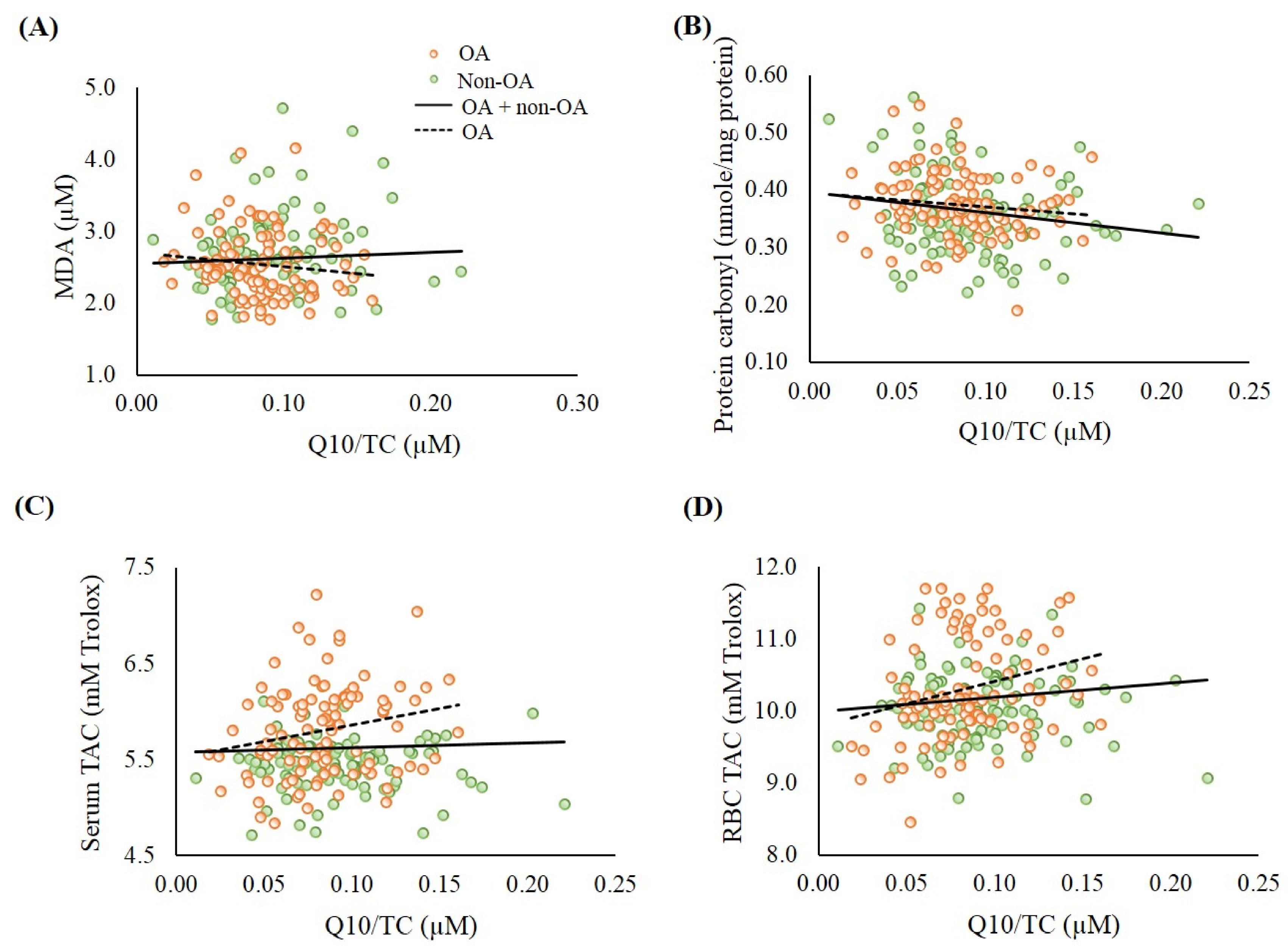
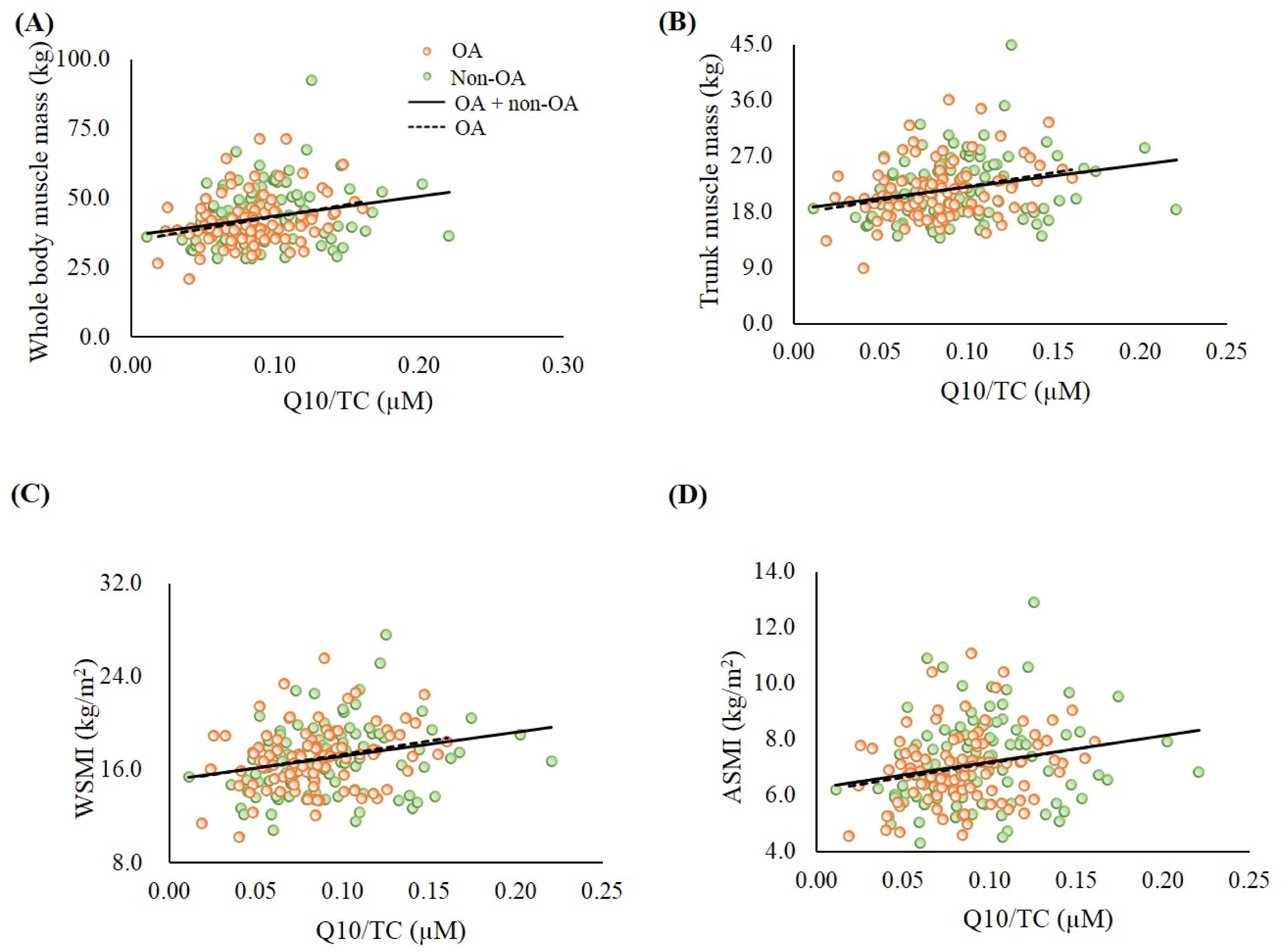
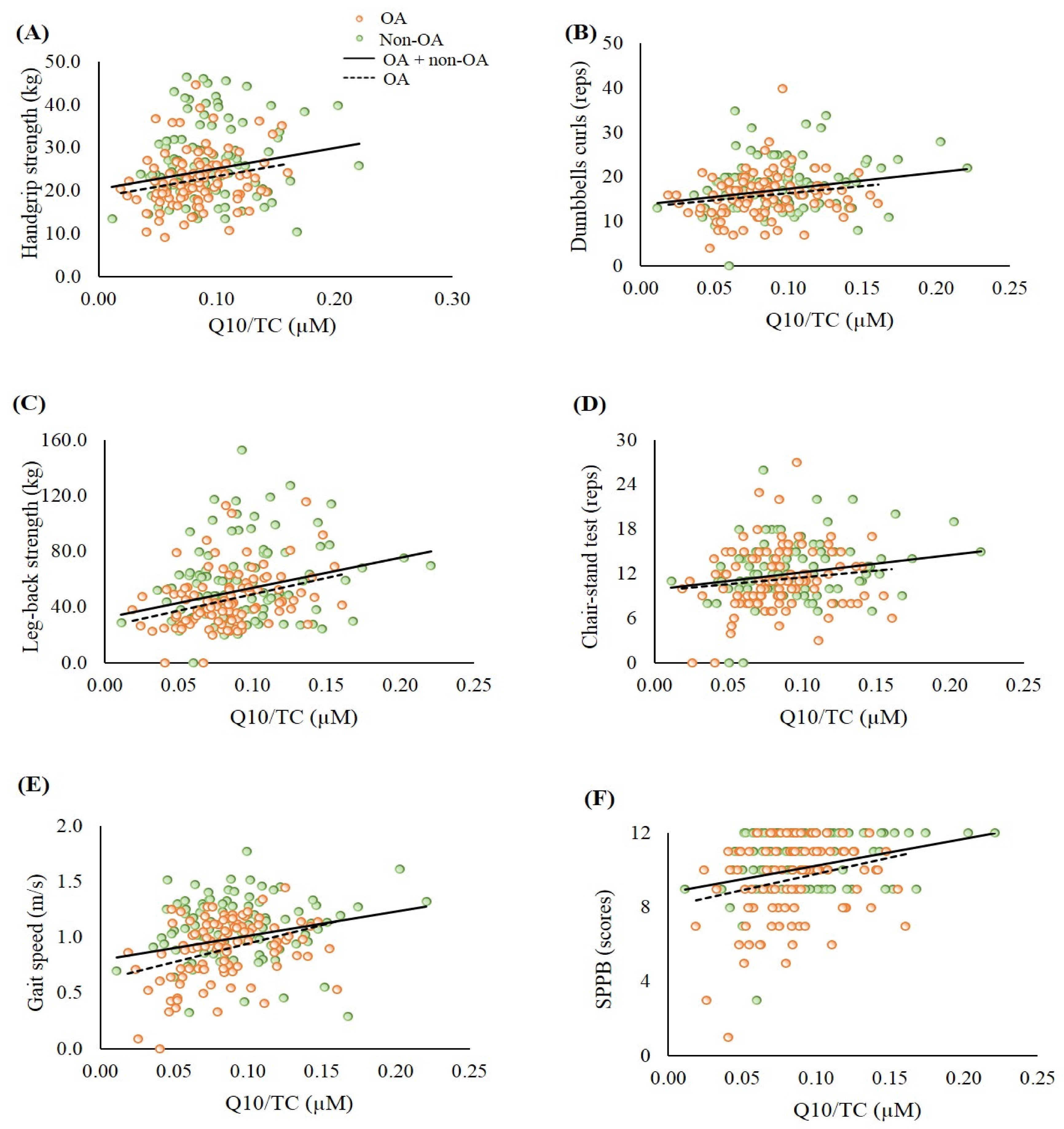
3.3. The Correlations between Coenzyme Q10 Status, Oxidative Stress, Antioxidant Capacity, Muscle Mass, and Muscle Strength and Endurance
3.4. The Correlations between Oxidative Stress and Antioxidant Capacity, Muscle Mass, Muscle Strength, and Muscle Endurance
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| ASMI | appendicular skeletal muscle mass index |
| BMI | body mass index |
| BUN | blood urea nitrogen |
| GOT | glutamic oxaloacetic transaminase |
| GPT | glutamic pyruvic transaminase |
| HPLC | high-performance liquid chromatography |
| Hs-CRP | high-sensitivity C-reactive protein |
| K/L | Kellgren and Lawrence |
| MDA | Malondialdehyde |
| OA | Osteoarthritis |
| RBC | red blood cell |
| ROS | reactive oxygen species |
| SPPB | short physical performance battery |
| TAC | Total antioxidant capacity |
| TC | total cholesterol |
| WSMI | whole skeletal muscle mass index |
References
- Thijssen, E.; van Caam, A.; van der Kraan, P.M. Obesity and osteoarthritis, more than just wear and tear: Pivotal roles for inflamed adipose tissue and dyslipidaemia in obesity-induced osteoarthritis. Rheumatology 2015, 54, 588–600. [Google Scholar] [CrossRef] [Green Version]
- Rai, M.F.; Sandell, L.J. Inflammatory mediators: Tracing links between obesity and osteoarthritis. Crit. Rev. Eukaryot. Gene Expr. 2011, 21, 131–142. [Google Scholar] [CrossRef]
- Lepetsos, P.; Papavassiliou, A.G. ROS/oxidative stress signaling in osteoarthritis. Biochim. Biophys. Acta 2016, 1862, 576–591. [Google Scholar] [CrossRef]
- Altay, M.A.; Ertürk, C.; Bilge, A.; Yaptı, M.; Levent, A.; Aksoy, N. Evaluation of prolidase activity and oxidative status in patients with knee osteoarthritis: Relationships with radiographic severity and clinical parameters. Rheumatol. Int. 2015, 35, 1725–1731. [Google Scholar] [CrossRef]
- Altindag, O.; Erel, O.; Aksoy, N.; Selek, S.; Celik, H.; Karaoglanoglu, M. Increased oxidative stress and its relation with collagen metabolism in knee osteoarthritis. Rheumatol. Int. 2007, 27, 339–344. [Google Scholar] [CrossRef]
- Howard, C.; Ferrucci, L.; Sun, K.; Fried, L.P.; Walston, J.; Varadhan, R.; Guralnik, J.M.; Semba, R.D. Oxidative protein damage is associated with poor grip strength among older women living in the community. J. Appl. Physiol. 2007, 103, 17–20. [Google Scholar] [CrossRef] [Green Version]
- Semba, R.D.; Ferrucci, L.; Sun, K.; Walston, J.; Varadhan, R.; Guralnik, J.M.; Fried, L.P. Oxidative stress and severe walking disability among older women. Am. J. Med. 2007, 120, 1084–1089. [Google Scholar] [CrossRef] [Green Version]
- Kemmler, W.; Teschler, M.; Goisser, S.; Bebenek, M.; von Stengel, S.; Bollheimer, L.C.; Sieber, C.C.; Freiberger, E. Prevalence of sarcopenia in Germany and the corresponding effect of osteoarthritis in females 70 years and older living in the community: Results of the FORMoSA study. Clin. Interv. Aging 2015, 10, 1565–1573. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El-barbary, A.M.; Khalek, M.A.A.; Elsalawy, A.M.; Hazaa, S.M. Assessment of lipid peroxidation and antioxidant status in rheumatoid arthritis and osteoarthritis patients. Egypt. Rheumatol. 2011, 33, 179–185. [Google Scholar] [CrossRef] [Green Version]
- Molyneux, S.L.; Young, J.M.; Florkowski, C.M.; Lever, M.; George, P.M. Coenzyme Q10: Is there a clinical role and a case for measurement? Clin. Biochem. Rev. 2008, 29, 71–82. Available online: https://pubmed.ncbi.nlm.nih.gov/18787645/ (accessed on 30 October 2020). [PubMed]
- Crane, F.L. Biochemical functions of coenzyme Q10. J. Am. Coll. Nutr. 2001, 20, 591–598. [Google Scholar] [CrossRef] [PubMed]
- Quinzii, C.M.; Emmanuele, V.; Hirano, M. Clinical presentations of coenzyme q10 deficiency syndrome. Mol. Syndromol. 2014, 5, 141–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niklowitz, P.; Onur, S.; Fischer, A.; Laudes, M.; Palussen, M.; Menke, T.; Döring, F. Coenzyme Q10 serum concentration and redox status in European adults: Influence of age, sex, and lipoprotein concentration. J. Clin. Biochem. Nutr. 2016, 58, 240–245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alam, M.A.; Rahman, M.M. Mitochondrial dysfunction in obesity: Potential benefit and mechanism of Co-enzyme Q10 supplementation in metabolic syndrome. J. Diabetes Metab. Disord. 2014, 13, 60. [Google Scholar] [CrossRef] [Green Version]
- Kumar, A.; Kaur, H.; Devi, P.; Mohan, V. Role of coenzyme Q10 (CoQ10) in cardiac disease, hypertension and Meniere-like syndrome. Pharmacol. Ther. 2009, 124, 259–268. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez-Mariscal, F.M.; Arenas-de Larriva, A.P.; Limia-Perez, L.; Romero-Cabrera, J.L.; Yubero-Serrano, E.M.; López-Miranda, J. Coenzyme Q10 Supplementation for the Reduction of Oxidative Stress: Clinical Implications in the Treatment of Chronic Diseases. Int. J. Mol. Sci. 2020, 21, 7870. [Google Scholar] [CrossRef]
- Shen, Q.; Pierce, J.D. Supplementation of Coenzyme Q10 among Patients with Type 2 Diabetes Mellitus. Healthcare 2015, 3, 296–309. [Google Scholar] [CrossRef]
- Kellgren, J.H.; Lawrence, J.S. Radiological assessment of osteo-arthrosis. Ann. Rheum. Dis. 1957, 16, 494–502. [Google Scholar] [CrossRef] [Green Version]
- Tatum, V.L.; Changchit, C.; Chow, C.K. Measurement of malondialdehyde by high performance liquid chromatography with fluorescence detection. Lipids 1990, 25, 226–229. [Google Scholar] [CrossRef]
- Levine, R.L.; Garland, D.; Oliver, C.N.; Amici, A.; Climent, I.; Lenz, A.G.; Ahn, B.W.; Shaltiel, S.; Stadtman, E.R. Determination of carbonyl content in oxidatively modified proteins. Methods Enzymol. 1990, 186, 464–478. [Google Scholar] [CrossRef]
- Re, R.; Pellegrini, N.; Proteggente, A.; Pannala, A.; Yang, M.; Rice-Evans, C. Antioxidant activity applying an improved ABTS radical cation decolorization assay. Free Radic. Biol. Med. 1999, 26, 1231–1237. [Google Scholar] [CrossRef]
- Littarru, G.P.; Mosca, F.; Fattorini, D.; Bompadre, S. Method to Assay Coenzyme Q10 in Blood Plasma or Blood Serum. U.S. Patent 7303921, 2007. Available online: https://patentimages.storage.googleapis.com/pdfs/6aadab0bc819eac3443b/US7303921.pdf (accessed on 8 November 2010).
- Chen, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Chou, M.Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307.e2. [Google Scholar] [CrossRef]
- Guralnik, J.M.; Simonsick, E.M.; Ferrucci, L.; Glynn, R.J.; Berkman, L.F.; Blazer, D.G.; Scherr, P.A.; Wallace, R.B. A short physical performance battery assessing lower extremity function: Association with self-reported disability and prediction of mortality and nursing home admission. J. Gerontol. 1994, 49, M85–M94. [Google Scholar] [CrossRef] [PubMed]
- Godziuk, K.; Prado, C.M.; Woodhouse, L.J.; Forhan, M. The impact of sarcopenic obesity on knee and hip osteoarthritis: A scoping review. BMC Musculoskelet. Disord. 2018, 19, 271. [Google Scholar] [CrossRef] [PubMed]
- Roubenoff, R. Sarcopenia and its implications for the elderly. Eur. J. Clin. Nutr. 2000, 54 (Suppl. 3), S40–S47. [Google Scholar] [CrossRef]
- Hernández-Camacho, J.D.; Bernier, M.; López-Lluch, G.; Navas, P. Coenzyme Q10 Supplementation in Aging and Disease. Front. Physiol. 2018, 9, 44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chin, K.Y.; Ima-Nirwana, S. The Role of Vitamin E in Preventing and Treating Osteoarthritis—A Review of the Current Evidence. Front. Pharmacol. 2018, 9, 946. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suantawee, T.; Tantavisut, S.; Adisakwattana, S.; Tanavalee, A.; Yuktanandana, P.; Anomasiri, W.; Deepaisarnsakul, B.; Honsawek, S. Oxidative stress, vitamin E, and antioxidant capacity in knee osteoarthritis. J. Clin. Diagn. Res. 2013, 7, 1855–1859. [Google Scholar] [CrossRef] [PubMed]
- Surapaneni, K.M.; Venkataramana, G. Status of lipid peroxidation, glutathione, ascorbic acid, vitamin E and antioxidant enzymes in patients with osteoarthritis. Indian J. Med. Sci. 2007, 61, 9–14. [Google Scholar] [CrossRef] [Green Version]
- Maneesh, M.; Jayalekshmi, H.; Suma, T.; Chatterjee, S.; Chakrabarti, A.; Singh, T.A. Evidence for oxidative stress in osteoarthritis. Indian J. Clin. Biochem. 2005, 20, 129–130. [Google Scholar] [CrossRef] [Green Version]
- Tetik, S.; Ahmad, S.; Alturfan, A.A.; Fresko, I.; Disbudak, M.; Sahin, Y.; Aksoy, H.; Yardimci, K.T. Determination of oxidant stress in plasma of rheumatoid arthritis and primary osteoarthritis patients. Indian J. Biochem. Biophys. 2010, 47, 353–358. Available online: https://pubmed.ncbi.nlm.nih.gov/21355418/ (accessed on 30 October 2020). [PubMed]
- Wen, L.; Shin, M.H.; Kang, J.H.; Yim, Y.R.; Kim, J.E.; Lee, J.W.; Lee, K.E.; Park, D.J.; Kim, T.J.; Kweon, S.S.; et al. Association between grip strength and hand and knee radiographic osteoarthritis in Korean adults: Data from the Dong-gu study. PLoS ONE 2017, 12, e0185343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pestronk, A.; Keeling, R.; Choksi, R. Sarcopenia, age, atrophy, and myopathy: Mitochondrial oxidative enzyme activities. Muscle Nerve 2017, 56, 122–128. [Google Scholar] [CrossRef]
- Dwivedi, S.; Singh, S.; Jaiswal, G. Lipid-peroxidation and Antioxidant Status in Osteoarthritis and Rheumatoid Arthritis Patients. Int. J. Contemp. Med. Res. 2016, 3, 1738–1741. Available online: https://www.ijcmr.com/uploads/7/7/4/6/77464738/_ijcmr_654_jne_2.pdf (accessed on 30 October 2020).
- Paździor, M.; Kiełczykowska, M.; Kurzepa, J.; Luchowska-Kocot, D.; Kocot, J.; Musik, I. The Oxidative Stress in Knee Osteoarthritis Patients. An Attempt of Evaluation of Possible Compensatory Effects Occurring in the Disease Development. Medicina 2019, 55, 150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fischer, A.; Onur, S.; Niklowitz, P.; Menke, T.; Laudes, M.; Rimbach, G.; Döring, F. Coenzyme Q10 Status as a Determinant of Muscular Strength in Two Independent Cohorts. PLoS ONE 2016, 11, e0167124. [Google Scholar] [CrossRef] [PubMed]
- Del Pozo-Cruz, J.; Rodríguez-Bies, E.; Navas-Enamorado, I.; Del Pozo-Cruz, B.; Navas, P.; López-Lluch, G. Relationship between functional capacity and body mass index with plasma coenzyme Q10 and oxidative damage in community-dwelling elderly-people. Exp. Gerontol. 2014, 52, 46–54. [Google Scholar] [CrossRef] [PubMed]
- Farnaghi, S.; Prasadam, I.; Cai, G.; Friis, T.; Du, Z.; Crawford, R.; Mao, X.; Xiao, Y. Protective effects of mitochondria-targeted antioxidants and statins on cholesterol-induced osteoarthritis. FASEB J. 2017, 31, 356–367. [Google Scholar] [CrossRef] [Green Version]
- Berenbaum, F. Osteoarthritis as an inflammatory disease (osteoarthritis is not osteoarthrosis!). Osteoarthr. Cartil. 2013, 21, 16–21. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.; Hong, Y.S.; Jeong, J.H.; Yang, E.J.; Jhun, J.Y.; Park, M.K.; Jung, Y.O.; Min, J.K.; Kim, H.Y.; Park, S.H.; et al. Coenzyme Q10 ameliorates pain and cartilage degradation in a rat model of osteoarthritis by regulating nitric oxide and inflammatory cytokines. PLoS ONE 2013, 8, e69362. [Google Scholar] [CrossRef] [Green Version]
- Coelho-Junior, H.J.; Picca, A.; Calvani, R.; Uchida, M.C.; Marzetti, E. If my muscle could talk: Myokines as a biomarker of frailty. Exp. Gerontol. 2019, 127, 110715. [Google Scholar] [CrossRef] [PubMed]
- Planella-Farrugia, C.; Comas, F.; Sabater-Masdeu, M.; Moreno, M.; Moreno-Navarrete, J.M.; Rovira, O.; Ricart, W.; Fernández-Real, J.M. Circulating Irisin and Myostatin as Markers of Muscle Strength and Physical Condition in Elderly Subjects. Front. Physiol. 2019, 10, 871. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | OA (N = 100) | Non-OA (N = 100) | p Value 2 | |||
|---|---|---|---|---|---|---|
| Age (y) | 69.5 ± 9.4 (71.0) 1 | 60.5 ± 9.6 (60.0) | <0.01 | |||
| BMI (kg/m2) | 25.3 ± 3.8 (25.6) | 24.3 ± 4.3 (24.2) | 0.10 | |||
| Albumin (g/L) | 45.0 ± 2.7 (45.0) | 45.2 ± 3.1 (45.0) | 0.31 | |||
| BUN (mmol/L) | 6.0 ± 2.4 (5.4) | 5.1 ± 2.1 (4.6) | <0.01 | |||
| Creatinine (µmol/L) | 76.0 ± 23.9 (71.6) | 74.3 ± 23.9 (71.6) | 0.58 | |||
| GOT (U/L) | 24.0 ± 5.0 (23.0) | 27.1 ± 10.9 (25.0) | 0.06 | |||
| GPT (U/L) | 20.9 ± 7.9 (19.0) | 27.3 ± 20.7 (22.0) | <0.01 | |||
| hs-CRP (mg/L) | 2.4 ± 7.2 (1.2) | 2.2 ± 3.8 (1.0) | 0.36 | |||
| Male (n = 27) | Female (n = 73) | p Value 3 | Male (n = 40) | Female (n = 60) | p Value 3 | |
| Muscle mass | ||||||
| Whole body muscle mass (kg) | 50.5 ± 9.0 (49.5) | 38.6 ± 6.4 (38.6) | <0.01 | 51.5 ± 10.6 (50.9) | 38.3 ± 7.4 (36.8) | <0.01 |
| Trunk muscle mass (kg) | 25.4 ± 4.6 (24.9) | 19.9 ± 3.5 (19.5) | <0.01 | 25.5 ± 5.2 (25.6) | 19.3 ± 3.6 (18.7) | <0.01 |
| WSMI (kg/m2) | 18.6 ± 2.8 (18.9) | 16.3 ± 2.3 (16.4) | <0.01 | 18.6 ± 2.9 (18.6) | 15.8 ± 2.5 (15.7)) | <0.01 |
| ASMI (kg/m2) | 7.9 ± 1.3 (7.9) | 6.6 ± 1.0 (6.7) | <0.01 | 8.1 ± 1.5 (8.1) | 6.6 ± 1.3 (6.4) | <0.01 |
| Muscle strength and endurance | ||||||
| Handgrip strength (kg) | 29.3 ± 6.7 (28.7) † | 20.2 ± 4.4 (20.1) | <0.01 | 35.1 ± 7.2 (35.5) | 21.2 ± 4.6 (21.5) | <0.01 |
| Dumbbells curls (reps) | 16.8 ± 6.5 (17.0) † | 15.5 ± 4.3 (15.0) | 0.18 | 21.2 ± 6.1 (20.0) | 16.1 ± 4.4 (16.0) | <0.01 |
| Leg-back strength (kg) | 65.2 ± 23.8 (61.5) † | 38.3 ± 14.0 (38.5) | <0.01 | 80.0 ± 29.3 (79.3) | 42.7 ± 14.8 (44.0) | <0.01 |
| Chair-stand test (reps) | 11.5 ± 4.9 (11.0) † | 11.1 ± 4.0 (11.0) | 0.65 | 13.1 ± 3.8 (13.5) | 12.4 ± 4.0 (12.0) | 0.14 |
| Gait speed (m/s) | 0.9 ± 0.3 (1.0) † | 0.9 ± 0.3 (0.9) † | 0.26 | 1.2 ± 0.3 (1.3) | 1.0 ± 0.2 (1.0) | <0.01 |
| SPPB (scores) | 9.7 ± 2.1 (10.0) † | 9.5 ± 2.2 (10.0) † | 0.75 | 10.9 ± 1.4 (11.5) | 10.5 ± 1.5 (11.0) | 0.11 |
| Sarcopenia (n, %) 6 | 7 (25.9%) | 10 (13.7%) | 0.23 | 6 (15.0%) | 10 (16.7%) | 0.96 |
| Elderly 4 | Middle-age 4 | |||||
| OA (N = 74) | Non-OA (N = 33) | p Value 5 | OA (N = 26) | Non-OA (N = 67) | p Value 5 | |
| BMI (kg/m2) | 24.9 ± 3.7 (25.1) | 22.9 ± 4.0 (23.2) | 0.02 | 26.5 ± 3.8 (26.3) | 25.0 ± 4.2 (24.8) | 0.12 |
| Albumin (g/L) | 44.5 ± 2.3 (44.5) * | 43.4 ± 3.2 (44.0) * | 0.20 | 46.5 ± 3.4 (46.5) | 46.0 ± 2.6 (46.0) | 0.53 |
| BUN (mmol/L) | 6.2 ± 2.6 (5.4) | 6.1 ± 2.9 (5.4) * | 0.63 | 5.5 ± 1.5 (5.4) | 4.5 ± 1.2 (4.6) | <0.01 |
| Creatinine (µmol/L) | 77.8 ± 24.8 (72.5) | 84.9 ± 31.8 (81.3) * | 0.18 | 73.4 ± 19.4 (67.2) | 69.0 ± 16.8 (66.3) | 0.47 |
| GOT (U/L) | 24.1 ± 4.9 (23.0) | 29.8 ± 12.4 (27.0) * | <0.01 | 23.8 ± 5.3 (23.0) | 25.7 ± 9.9 (24.0) | 0.53 |
| GPT (U/L) | 19.9 ± 7.3 (18.0) * | 27.5 ± 19.5 (22.0) | 0.02 | 23.7 ± 8.9 (22.0) | 27.2 ± 21.4 (22.0) | 0.80 |
| hs-CRP (mg/L) | 2.9 ± 8.3 (1.3) * | 2.0 ± 2.3 (1.1) | 0.41 | 1.2 ± 1.0 (0.9) | 2.3 ± 4.4 (0.9) | 0.56 |
| Muscle mass | ||||||
| Whole body muscle mass (kg) | 40.1 ± 8.0 (38.7) * | 38.8 ± 8.3 (36.5) * | 0.24 | 46.7 ± 9.8 (45.1) | 45.9 ± 11.3 (45.7) | 0.75 |
| Trunk muscle mass (kg) | 20.5 ± 4.2 (19.9) * | 19.5 ± 3.9 (18.6) * | 0.17 | 23.9 ± 4.8 (23.2) | 23.0 ± 5.5 (23.2) | 0.46 |
| WSMI (kg/m2) | 16.5 ± 2.4 (16.4) * | 15.8 ± 2.5 (15.6) * | 0.19 | 18.2 ± 2.9 (17.8) | 17.4 ± 3.1 (17.6) | 0.26 |
| ASMI (kg/m2) | 6.8 ± 1.1 (6.7) * | 6.6 ± 1.4 (6.3) * | 0.25 | 7.6 ± 1.4 (7.2) | 7.5 ± 1.6 (7.4) | 0.79 |
| Muscle strength and endurance | ||||||
| Handgrip strength (kg) | 21.2 ± 5.5 (20.6) * | 23.1 ± 7.1 (23.9) * | 0.19 | 26.8 ± 7.5 (26.3) | 28.6 ± 9.2 (26.7) | 0.55 |
| Dumbbells curls (reps) | 14.9 ± 5.0 (15.0) * | 15.5 ± 5.2 (16.0) * | 0.49 | 18.3 ± 4.2 (18.0) | 19.5 ± 5.6 (19.0) | 0.57 |
| Leg-back strength (kg) | 41.4 ± 16.6 (38.8) * | 49.3 ± 25.8 (44.0) * | 0.21 | 57.5 ± 26.8 (53.3) | 61.7 ± 28.9 (58.5) | 0.61 |
| Chair-stand test (reps) | 10.5 ± 4.3 (10.0) * | 10.6 ± 3.6 (10.0) * | 0.67 | 13.2 ± 3.7 (13.5) | 13.7 ± 3.7 (14.0) | 0.64 |
| Gait speed (m/s) | 0.85 ± 0.29 (0.90) * | 0.96 ± 0.27 (1.02) * | 0.07 | 1.00 ± 0.21 (1.04) | 1.15 ± 0.25 (1.17) | 0.01 |
| SPPB (scores) | 9.1 ± 2.2 (9.0) * | 9.8 ± 1.7 (10.0) * | 0.14 | 10.8 ± 1.5 (11.0) | 11.1 ± 1.1 (11.0) | 0.48 |
| Sarcopenia (n, %) 6 | 14 (18.9%) | 9 (27.3%) | 0.47 | 3 (11.5%) | 7 (10.4%) | 1.00 |
| Male | ||||||
| Elderly 4 | Middle-Age 4 | |||||
| OA (N = 18) | Non-OA (N = 10) | p Value 5 | OA (N = 9) | Non-OA (N = 30) | p Value 5 | |
| Muscle mass | ||||||
| Whole body muscle mass (kg) | 48.3 ± 8.5 (47.0) | 46.8 ± 6.9 (45.8) | 0.63 | 54.8 ± 8.7 (53.7) | 53.0 ± 11.2 (53.2) | 0.56 |
| Trunk muscle mass (kg) | 24.4 ± 4.4 (23.6) | 23.6 ± 3.3 (23.9) | 0.60 | 27.5 ± 4.7 (26.9) | 26.2 ± 5.6 (26.0) | 0.52 |
| WSMI (kg/m2) | 17.7 ± 2.6 (17.7) * | 17.9 ± 2.4 (18.3) | 0.87 | 20.4 ± 2.5 (20.4) | 18.8 ± 3.1 (19.0) | 0.19 |
| ASMI (kg/m2) | 7.5 ± 1.3 (7.6) * | 7.6 ± 1.3 (7.5) | 0.92 | 8.7 ± 1.1 (8.7) | 8.3 ± 1.5 (8.2) | 0.19 |
| Muscle strength and endurance | ||||||
| Handgrip strength (kg) | 27.0 ± 5.5 (25.8) * | 30.5 ± 4.4 (29.8) * | 0.09 | 34.0 ± 6.8 (36.0) | 36.6 ± 7.3 (38.3) | 0.34 |
| Dumbbells curls (reps) | 16.2 ± 7.6 (16.5) | 17.7 ± 3.9 (17.0) * | 0.41 | 18.0 ± 3.0 (18.0) | 22.4 ± 6.4 (22.0) | 0.06 |
| Leg-back strength (kg) | 57.7 ± 16.7 (57.8) | 79.8 ± 20.1 (78.0) | < 0.01 | 80.3 ± 29.5 (88.0) | 80.1 ± 32.1 (79.8) | 0.99 |
| Chair-stand test (reps) | 10.7 ± 5.6 (10.0) | 10.7 ± 2.5 (10.0) * | 0.77 | 13.1 ± 2.8 (13.0) | 13.9 ± 3.9 (14.0) | 0.34 |
| Gait speed (m/s) | 0.9 ± 0.4 (0.9) | 1.1 ± 0.3 (1.2) | 0.07 | 1.0 ± 0.2 (1.1) | 1.2 ± 0.3 (1.3) | 0.09 |
| SPPB (scores) | 9.1 ± 2.3 (10.0) | 10.1 ± 1.2 (10.0) * | 0.41 | 10.8 ± 1.1 (11.0) | 11.2 ± 1.3 (12.0) | 0.21 |
| Sarcopenia (n, %) 6 | 6 (33.3%) | 3 (30.0%) | 1.00 | 1 (11.1%) | 3 (10.0%) | 1.00 |
| Female | ||||||
| Elderly 4 | Middle-Age 4 | |||||
| OA (N = 56) | Non-OA (N = 23) | p Value 5 | OA (N = 17) | Non-OA (N = 37) | p Value 5 | |
| Muscle mass | ||||||
| Whole body muscle mass (kg) | 37.4 ± 5.6 (38.1) * | 35.3 ± 6.3 (34.2) * | 0.03 | 42.4 ± 7.4 (40.6) | 40.2 ± 7.4 (39.3) | 0.32 |
| Trunk muscle mass (kg) | 19.2 ± 3.2 (19.2) * | 17.7 ± 2.6 (17.4) * | 0.05 | 22.0 ± 3.7 (22.3) | 20.4 ± 3.7 (19.7) | 0.13 |
| WSMI (kg/m2) | 16.1 ± 2.2 (16.2) | 14.9 ± 2.0 (14.9) * | 0.03 | 17.1 ± 2.5 (17.2) | 16.3 ± 2.6 (16.2) | 0.29 |
| ASMI (kg/m2) | 6.5 ± 1.0 (6.6) | 6.2 ± 1.3 (6.0)* | 0.06 | 6.9 ± 1.2 (7.2) | 6.8 ± 1.2 (6.7) | 0.69 |
| Muscle strength and endurance | ||||||
| Handgrip strength (kg) | 19.3 ± 4.1 (19.4) * | 19.8 ± 5.5 (19.8) | 0.83 | 23.0 ± 4.5 (23.9) | 22.0 ± 3.8 (21.9) | 0.43 |
| Dumbbells curls (reps) | 14.5 ± 3.7 (15.0) * | 14.5 ± 5.4 (13.5) * | 0.95 | 18.5 ± 4.8 (18.0) | 17.1 ± 3.4 (17.0) | 0.25 |
| Leg-back strength (kg) | 36.2 ± 12.8 (34.8) * | 36.1 ± 14.0 (35.0) * | 0.92 | 45.4 ± 15.7 (48.5) | 46.7 ± 13.9 (48.0) | 0.76 |
| Chair-stand test (reps) | 10.4 ± 3.8 (10.0) * | 10.6 ± 4.0 (10.0) * | 0.79 | 13.2 ± 4.1 (14.0) | 13.5 ± 3.7 (13.0) | 0.93 |
| Gait speed (m/s) | 0.8 ± 0.3 (0.9) * | 0.9 ± 0.2 (1.0) * | 0.40 | 1.0 ± 0.2 (1.0) | 1.1 ± 0.2 (1.1) | 0.10 |
| SPPB (scores) | 9.1 ± 2.2 (9.0) * | 9.6 ± 1.9 (9.0) * | 0.25 | 10.8 ± 1.7 (11.0) | 11.0 ± 1.0 (11.0) | 0.85 |
| Sarcopenia (n, %) 6 | 8 (14.3%) | 6 (26.1%) | 0.33 | 2 (11.8%) | 4 (10.8%) | 1.00 |
| Elderly 2 | Middle-Age 2 | |||||
|---|---|---|---|---|---|---|
| OA (N = 74) | Non-OA (N = 33) | p Value 3 | OA (N = 26) | Non-OA (N = 67) | p Value 3 | |
| Coenzyme Q10 (µM) 1 | 0.41 ± 0.15 (0.41) | 0.47 ± 0.22 (0.46) | 0.18 | 0.44 ± 0.13 (0.42) | 0.47 ± 0.18 (0.43) | 0.44 |
| Coenzyme Q10/TC (µmol/mmol) | 0.08 ± 0.03 (0.08) | 0.10 ± 0.04 (0.09) | 0.06 | 0.09 ± 0.03 (0.09) | 0.09 ± 0.03 (0.09) | 0.99 |
| Oxidative stress | ||||||
| MDA (µM) | 2.6 ± 0.5 (2.5) | 2.7 ± 0.6 (2.6) | 0.29 | 2.5 ± 0.4 (2.5) | 2.7 ± 0.5 (2.7) | 0.09 |
| Protein carbonyl (nmole/mg protein) | 0.38 ± 0.06 (0.37) | 0.38 ± 0.07 (0.38) * | 0.96 | 0.36 ± 0.05 (0.37) | 0.34 ± 0.07 (0.33) | 0.02 |
| Antioxidant capacity | ||||||
| Serum TAC (mM Trolox) | 5.8 ± 0.5 (5.7) | 5.4 ± 0.3 (5.4) | <0.01 | 5.9 ± 0.4 (6.0) | 5.4 ± 0.3 (5.5) | <0.01 |
| RBC TAC (mM Trolox) | 10.2 ± 0.7 (10.1) * | 10.0 ± 0.5 (10.0) | 0.16 | 10.6 ± 0.7 (10.4) | 10.1 ± 0.5 (10.0) | <0.01 |
| Coenzyme Q10/TC (µmol/mmol) | ||||
|---|---|---|---|---|
| Elderly 2 | Middle-Age 2 | |||
| OA (N = 74) | Non-OA (N = 33) | OA (N = 26) | Non-OA (N = 67) | |
| Oxidative stress | ||||
| MDA (µM) | −0.21 1,# | 0.18 | −0.07 | 0.09 |
| Protein carbonyl (nmole/mg protein) | −0.12 | −0.27 | −0.08 | −0.11 |
| Antioxidant capacity | ||||
| Serum TAC (mM Trolox) | 0.20 † | −0.10 | 0.19 | −0.02 |
| RBC TAC (mM Trolox) | 0.26 * | −0.19 | 0.20 | 0.13 |
| Muscle mass | ||||
| Whole body muscle mass (kg) | 0.21 † | 0.15 | 0.20 | 0.30 * |
| Trunk muscle mass (kg) | 0.15 | 0.25 | 0.30 | 0.28 * |
| WSMI (kg/m2) | 0.22 # | 0.15 | 0.27 | 0.36 ** |
| ASMI (kg/m2) | 0.26 * | 0.08 | 0.10 | 0.38 ** |
| Muscle strength and endurance | ||||
| Handgrip strength (kg) | 0.19 | 0.04 | 0.17 | 0.18 |
| Dumbbells curls (reps) | 0.24 * | 0.24 | −0.01 | 0.20 |
| Leg-back strength (kg) | 0.29 * | 0.19 | 0.25 | 0.27 * |
| Chair-stand test (reps) | 0.03 | 0.33 ‡ | 0.17 | 0.12 |
| Gait speed (m/s) | 0.33 ** | 0.17 | 0.31 | 0.05 |
| SPPB (scores) | 0.16 | 0.28 | 0.12 | 0.15 |
| Oxidative Stress | Antioxidant Capacity | |||
|---|---|---|---|---|
| MDA (µM) | Protein Carbonyl (nmole/mg protein) | Serum TAC (mM Trolox) | RBC TAC (mM Trolox) | |
| OA + Non-OA (N = 200) | ||||
| Whole body muscle mass (kg) | 0.11 1 | −0.23 ** | 0.01 | 0.09 |
| Trunk muscle mass (kg) | 0.08 | −0.26 ** | 0.04 | 0.10 |
| WSMI (kg/m2) | 0.08 | −0.25 ** | 0.07 | 0.15 * |
| ASMI (kg/m2) | 0.13 | −0.22 ** | 0.04 | 0.10 |
| Handgrip strength (kg) | 0.13 | −0.07 | −0.13 | −0.03 |
| Dumbbells curls (reps) | −0.04 | −0.13 | −0.06 | −0.02 |
| Leg-back strength (kg) | 0.10 | −0.15 * | −0.03 | 0.04 |
| Chair-stand test (reps) | −0.01 | −0.13 | −0.03 | −0.00 |
| Gait speed (m/s) | 0.14 | −0.33 ** | 0.12 | 0.27 ** |
| SPPB (scores) | 0.01 | −0.26 ** | 0.01 | 0.11 |
| Elderly 2 OA + Non-OA (N = 107) | ||||
| Whole body muscle mass (kg) | 0.12 | −0.12 | 0.02 | 0.08 |
| Trunk muscle mass (kg) | 0.13 | −0.14 | 0.04 | 0.09 |
| WSMI (kg/m2) | 0.08 | −0.17 | 0.09 | 0.14 |
| ASMI (kg/m2) | 0.09 | −0.14 | 0.10 | 0.10 |
| Handgrip strength (kg) | 0.06 | 0.04 | −0.17 | −0.03 |
| Dumbbells curls (reps) | −0.03 | −0.02 | −0.06 | −0.00 |
| Leg-back strength (kg) | −0.00 | 0.01 | −0.04 | 0.09 |
| Chair-stand test (reps) | −0.03 | −0.04 | −0.05 | −0.02 |
| Gait speed (m/s) | 0.09 | −0.10 | 0.17 | 0.38 ** |
| SPPB (scores) | 0.00 | −0.10 | −0.02 | 0.08 |
| Middle-age 2 OA + Non-OA (N = 93) | ||||
| Whole body muscle mass (kg) | 0.08 | −0.23 * | 0.03 | 0.01 |
| Trunk muscle mass (kg) | 0.02 | −0.26 * | 0.08 | 0.05 |
| WSMI (kg/m2) | 0.07 | −0.23 * | 0.07 | 0.11 |
| ASMI (kg/m2) | 0.17 | −0.20 | −0.01 | 0.04 |
| Handgrip strength (kg) | 0.17 | 0.01 | −0.08 | −0.11 |
| Dumbbells curls (reps) | −0.12 | −0.08 | −0.08 | −0.12 |
| Leg-back strength (kg) | 0.21* | −0.17 | −0.03 | −0.09 |
| Chair-stand test (reps) | −0.04 | −0.02 | −0.01 | −0.10 |
| Gait speed (m/s) | 0.15 | −0.42 ** | 0.12 | 0.12 |
| SPPB (scores) | −0.04 | −0.23 * | 0.10 | 0.07 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, P.-S.; Yen, C.-H.; Huang, Y.-Y.; Chiu, C.-J.; Lin, P.-T. Associations between Coenzyme Q10 Status, Oxidative Stress, and Muscle Strength and Endurance in Patients with Osteoarthritis. Antioxidants 2020, 9, 1275. https://doi.org/10.3390/antiox9121275
Chang P-S, Yen C-H, Huang Y-Y, Chiu C-J, Lin P-T. Associations between Coenzyme Q10 Status, Oxidative Stress, and Muscle Strength and Endurance in Patients with Osteoarthritis. Antioxidants. 2020; 9(12):1275. https://doi.org/10.3390/antiox9121275
Chicago/Turabian StyleChang, Po-Sheng, Chi-Hua Yen, Yu-Yun Huang, Ching-Ju Chiu, and Ping-Ting Lin. 2020. "Associations between Coenzyme Q10 Status, Oxidative Stress, and Muscle Strength and Endurance in Patients with Osteoarthritis" Antioxidants 9, no. 12: 1275. https://doi.org/10.3390/antiox9121275
APA StyleChang, P. -S., Yen, C. -H., Huang, Y. -Y., Chiu, C. -J., & Lin, P. -T. (2020). Associations between Coenzyme Q10 Status, Oxidative Stress, and Muscle Strength and Endurance in Patients with Osteoarthritis. Antioxidants, 9(12), 1275. https://doi.org/10.3390/antiox9121275