Nitrosative Stress Biomarkers in the Non-Stimulated and Stimulated Saliva, as well as Gingival Crevicular Fluid of Patients with Periodontitis: Review and Clinical Study




Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Sample Collection
2.3. Clinical Examination
2.4. Redox Assays
2.5. Statistical Analysis
3. Results
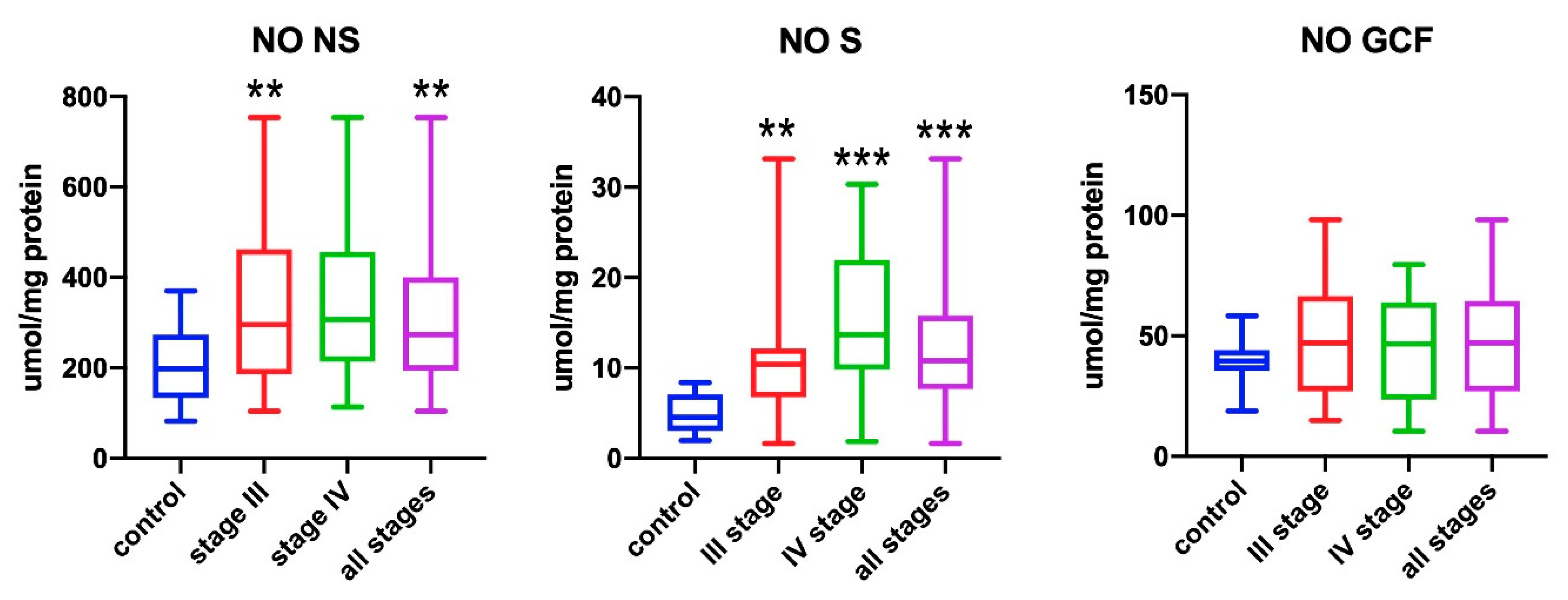
3.1. Nitric Oxide (NO)
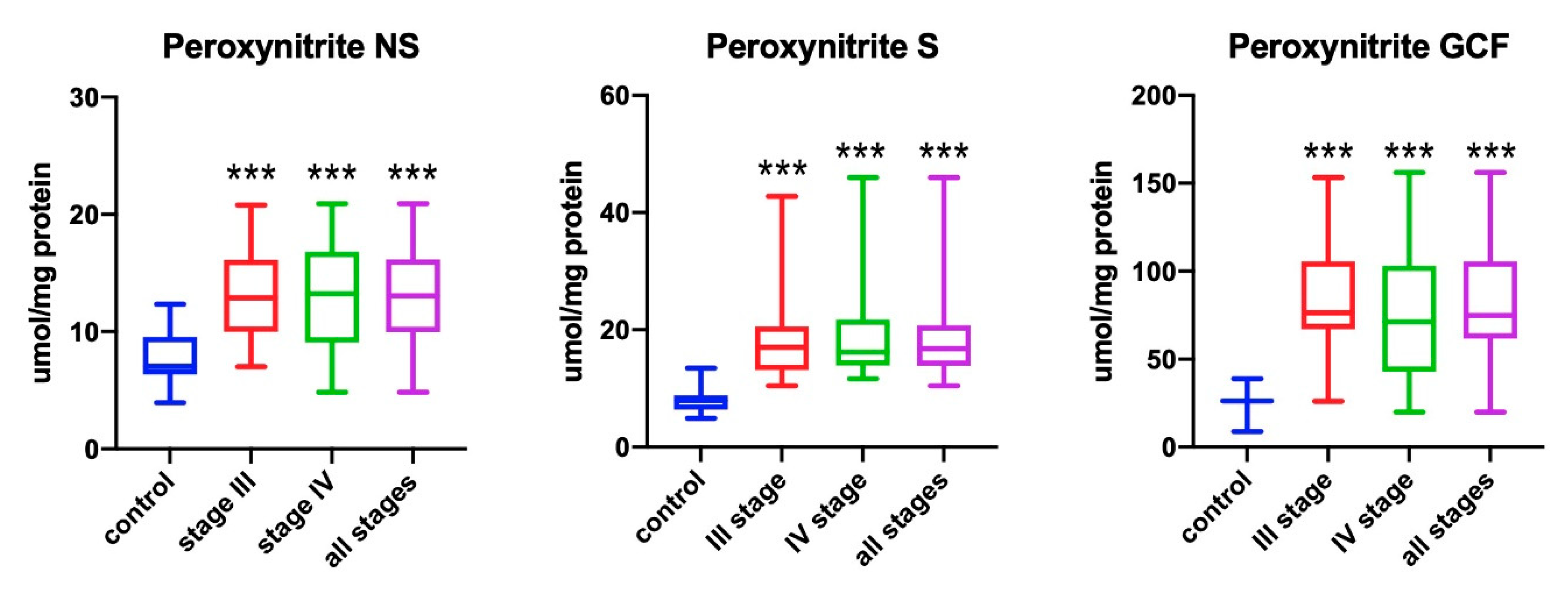
3.2. Peroxynitrite
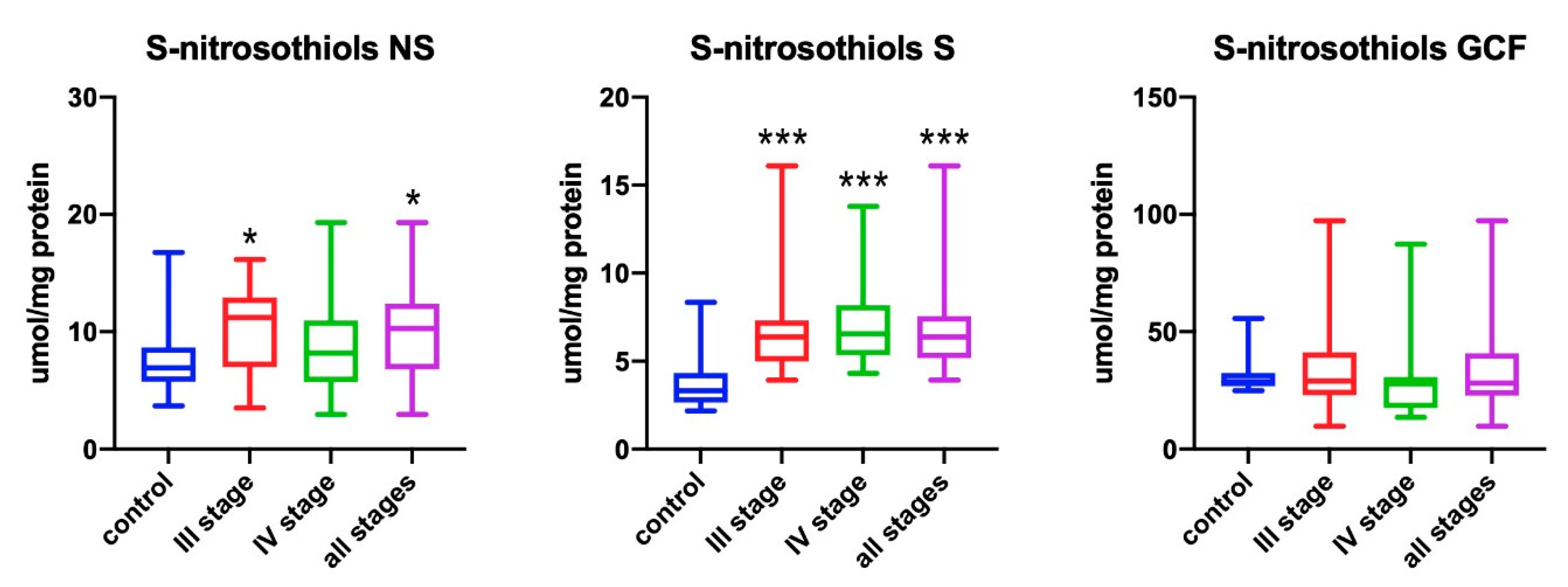
3.3. S-Nitrosothiols
3.4. Correlations
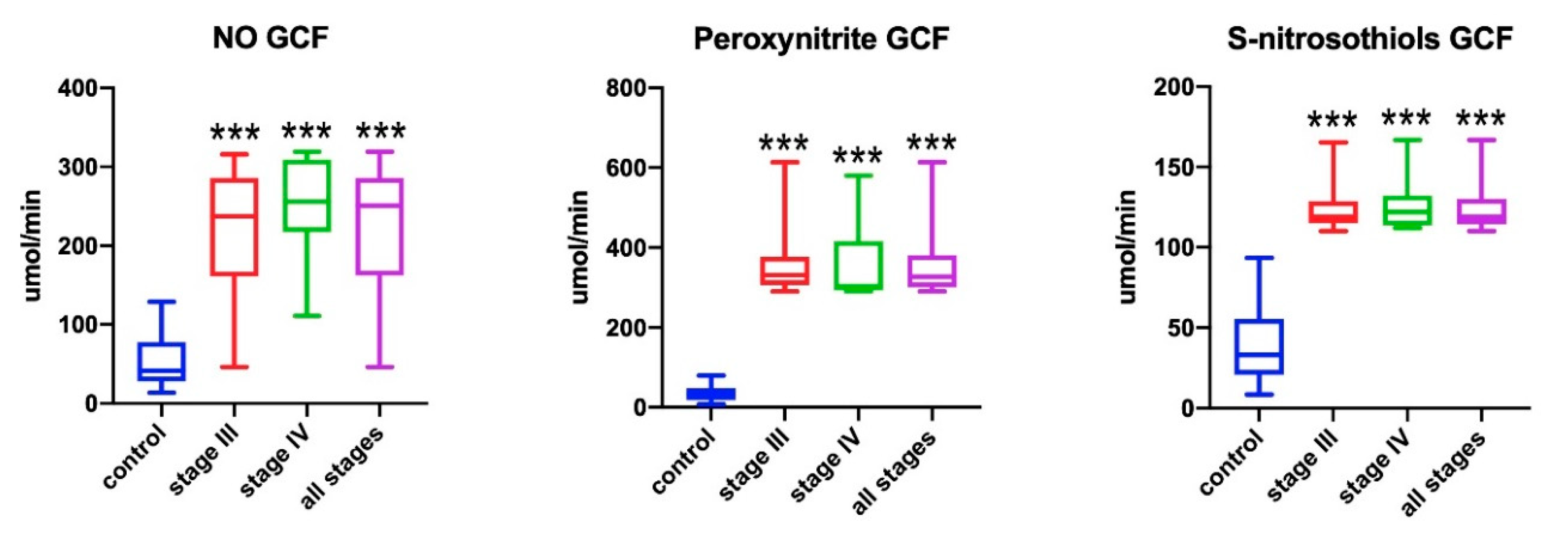
3.5. GCF Biomarkers
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Tonetti, M.S.; Greenwell, H.; Kornman, K.S. Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J. Periodontol. 2018, 89, S159–S172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hopkins, R.; Li, Y.R. Essentials of Free Radical Biology and Medicine; Cell Med Press AIMSCI, Inc.: Chicago, IL, USA, 2017. [Google Scholar]
- Kwon, N.S.; Nathan, C.F.; Gilker, C.; Griffith, O.W.; Matthews, D.E.; Stuehr, D.J. L-Citrulline production from L-arginine by macrophage nitric oxide synthase. The ureido oxygen derives from dioxygen. J. Biol. Chem. 1990, 265, 13442–13445. [Google Scholar] [PubMed]
- Özmeriç, N.; Elgün, S.; Uraz, A. Salivary arginase in patients with adult periodontitis. Clin. Oral Investig. 2000, 4, 21–24. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Huang, X.; He, F. Mechanism and role of nitric oxide signaling in periodontitis. Exp. Ther. Med. 2019, 18, 3929–3935. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parwani, S.R.; Chitnis, P.J.; Parwani, R.N. Salivary nitric oxide levels in inflammatory periodontal disease -A case-control and interventional study. Int. J. Dent. Hyg. 2012, 10, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Aurer, A.; Aleksić, J.; Ivić-Kardum, M.; Aurer, J.; Čulo, F. Nitric Oxide synthesis is decreased in periodontitis. J. Clin. Periodontol. 2001, 28, 565–568. [Google Scholar] [CrossRef] [PubMed]
- Papapanou, P.N.; Sanz, M.; Buduneli, N.; Dietrich, T.; Feres, M.; Fine, D.H.; Flemmig, T.F.; Garcia, R.; Giannobile, W.V.; Graziani, F.; et al. Periodontitis: Consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Clin. Periodontol. 2018, 45, S162–S170. [Google Scholar] [CrossRef]
- O’Leary, T.J.; Drake, R.B.; Naylor, J.E. The Plaque Control Record. J. Periodontol. 1972, 43, 38. [Google Scholar] [CrossRef]
- Choromańska, M.; Klimiuk, A.; Kostecka-Sochoń, P.; Wilczyńska, K.; Kwiatkowski, M.; Okuniewska, N.; Waszkiewicz, N.; Zalewska, A.; Maciejczyk, M. Antioxidant defence, oxidative stress and oxidative damage in saliva, plasma and erythrocytes of dementia patients. Can salivary AGE be a marker of dementia? Int. J. Mol. Sci. 2017, 18, 2205. [Google Scholar] [CrossRef] [Green Version]
- Maciejczyk, M.; Szulimowska, J.; Taranta-Janusz, K.; Werbel, K.; Wasilewska, A.; Zalewska, A. Salivary FRAP as a marker of chronic kidney disease progression in children. Antioxidants 2019, 8, 409. [Google Scholar] [CrossRef] [Green Version]
- Sawczuk, B.; Maciejczyk, M.; Siemieniuk, S.; Posmyk, R.; Zalewska, A. Car Salivary Gland Function, Antioxidant Defence and Oxidative Damage in the Saliva of Patients with Breast Cancer: Does the BRCA1 Mutation Disturb the Salivary Redox Profile? Cancers (Basel) 2019, 11, 1501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fejfer, K.; Buczko, P.; Niczyporuk, M.; Ładny, J.R.; Hady, H.R.; Knaś, M.; Waszkiel, D.; Klimiuk, A.; Zalewska, A.; Maciejczyk, M. Oxidative Modification of Biomolecules in the Nonstimulated and Stimulated Saliva of Patients with Morbid Obesity Treated with Bariatric Surgery. Biomed. Res. Int. 2017, 2017, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klimiuk, A.; Maciejczyk, M.; Choromańska, M.; Fejfer, K.; Waszkiewicz, N.; Zalewska, A. Salivary Redox Biomarkers in Different Stages of Dementia Severity. J. Clin. Med. 2019, 8, 840. [Google Scholar] [CrossRef] [Green Version]
- Skutnik-Radziszewska, A.; Maciejczyk, M.; Fejfer, K.; Krahel, J.; Flisiak, I.; Kołodziej, U.; Zalewska, A. Salivary Antioxidants and Oxidative Stress in Psoriatic Patients: Can Salivary Total Oxidant Status and Oxidative Status Index Be a Plaque Psoriasis Biomarker? Oxid. Med. Cell. Longev. 2020, 2020, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Maciejczyk, M.; Szulimowska, J.; Skutnik, A.; Taranta-Janusz, K.; Wasilewska, A.; Wiśniewska, N.; Zalewska, A. Salivary Biomarkers of Oxidative Stress in Children with Chronic Kidney Disease. J. Clin. Med. 2018, 7, 209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lange, D.E.; Plagmann, H.C.; Eenboom, A.; Promesberger, A. Klinische Bewertungsverahren zur Objektivierung der Mundhygiene. Dtsch. Zahnarztl. Z. 1977, 32, 44–47. [Google Scholar] [PubMed]
- Ainamo, J.; Bay, I. Problems and proposals for recording gingivitis and plaque. Int. Dent. J. 1975, 25, 229–235. [Google Scholar]
- Newbrun, E. Indices to Measure Gingival Bleeding. J. Periodontol. 1996, 67, 555–561. [Google Scholar] [CrossRef]
- Taso, E.; Stefanovic, V.; Stevanovic, I.; Vojvodic, D.; Topic, A.; Petkovic-Curcin, A.; Obradovic-Djuricic, K.; Markovic, A.; Djukic, M.; Vujanovic, D. Influence of dental restorations on oxidative stress in gingival crevicular fluid. Oxid. Med. Cell. Longev. 2018, 2018, 1–17. [Google Scholar] [CrossRef]
- Grisham, M.B.; Johnson, G.G.; Lancaster, J.R. Quantitation of nitrate and nitrite in extracellular fluids. In Methods in Enzymology; Academic Press: Cambridge, MA, USA, 1996; Volume 268, pp. 237–246. [Google Scholar]
- Wink, D.A.; Kim, S.; Coffin, D.; Cook, J.C.; Vodovotz, Y.; Chistodoulou, D.; Jourd’heuil, D.; Grisham, M.B. Detection of S-nitrosothiols by fluorometric and colorimetric methods. In Methods in Enzymology; Academic Press: Cambridge, MA, USA, 1999; Volume 301, pp. 201–211. [Google Scholar]
- Wassall, R.R.; Preshaw, P.M. Clinical and technical considerations in the analysis of gingival crevicular fluid. Periodontology 2000 2016, 70, 65–79. [Google Scholar] [CrossRef]
- Menaka, K.; Ramesh, A.; Thomas, B.; Kumari, N.S. Estimation of nitric oxide as an inflammatory marker in periodontitis. J. Indian Soc. Periodontol. 2009, 13, 75. [Google Scholar] [CrossRef] [PubMed]
- Dhotre, P.S.; Suryakar, A.N.; Bhogade, R.B. Oxidative stress in periodontitis: A critical link to cardiovascular disease. Biomed. Res. 2011, 22, 178–182. [Google Scholar]
- Mani Sundar, N.; Krishnan, V.; Krishnaraj, S.; Hemalatha, V.T.; Alam, M.N. Comparison of the salivary and the serum nitric oxide levels in chronic and aggressive periodontitis: A biochemical study. J. Clin. Diagn. Res. 2013, 7, 1223–1227. [Google Scholar] [CrossRef] [PubMed]
- Andrukhov, O.; Haririan, H.; Bertl, K.; Rausch, W.D.; Bantleon, H.P.; Moritz, A.; Rausch-Fan, X. Nitric oxide production, systemic inflammation and lipid metabolism in periodontitis patients: Possible gender aspect. J. Clin. Periodontol. 2013, 40, 916–923. [Google Scholar] [CrossRef]
- Wadhwa, D.; Bey, A.; Hasija, M.; Moin, S.; Kumar, A.; Aman, S.; Sharma, V.K. Determination of levels of nitric oxide in smoker and nonsmoker patients with chronic periodontitis. J. Periodontal Implant Sci. 2013, 43, 215–220. [Google Scholar] [CrossRef]
- Poorsattar Bejeh-Mir, A.; Parsian, H.; Akbari Khoram, M.; Ghasemi, N.; Bijani, A.; Khosravi-Samani, M. Diagnostic Role of Salivary and GCF Nitrite, Nitrate and Nitric Oxide to Distinguish Healthy Periodontium from Gingivitis and Periodontitis. Int. J. Mol. Cell. Med. 2014, 3, 138–145. [Google Scholar]
- Wattamwar, P.P.; Kolte, R.A.; Kolte, A.P.; Shah, K.K. Influence of interventional nonsurgical periodontal treatment on levels of salivary and serum nitric oxide in smokers and nonsmokers with chronic periodontitis. J. Indian Soc. Periodontol. 2016, 20, 592–596. [Google Scholar]
- Dhotre, P.S.; Bhogade, R.B.; Shaikh, A.K. Nitric oxide levels in periodontitis with relation to obesity. Int. J. Clin. Biochem. Res. 2016, 3, 50. [Google Scholar] [CrossRef]
- Chen, M.; Cai, W.; Zhao, S.; Shi, L.; Chen, Y.; Li, X.; Sun, X.; Mao, Y.; He, B.; Hou, Y.; et al. Oxidative stress-related biomarkers in saliva and gingival crevicular fluid associated with chronic periodontitis: A systematic review and meta-analysis. J. Clin. Periodontol. 2019, 46, 608–622. [Google Scholar] [CrossRef]
- Ozer, L.; Elgun, S.; Ozdemir, B.; Pervane, B.; Ozmeric, N. Arginine–Nitric Oxide–Polyamine Metabolism in Periodontal Disease. J. Periodontol. 2011, 82, 320–328. [Google Scholar] [CrossRef]
- Mazurek-Mochol, M.; Kozak, M.; Sawczuk, M.; Maciejewska, A.; Malinowski, D.; Safranow, K.; Pawlik, A. NOS3 gene rs1799983 and rs2070744 polymorphisms in patients with periodontal disease. Folia Biol. 2018, 64, 59–64. [Google Scholar]
- Topcu, A.O.; Akalin, F.A.; Sahbazoglu, K.B.; Yamalik, N.; Kilinc, K.; Karabulut, E.; Tözüm, T.F. Nitrite and Nitrate Levels of Gingival Crevicular Fluid and Saliva in Subjects with Gingivitis and Chronic Periodontitis. J. Oral Maxillofac. Res. 2014, 5, e5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meschiari, C.A.; Zuardi, L.R.; Gomes, V.A.; Costa de Almeida, G.R.; Novaes, A.B.; Gerlach, R.F.; Marcaccini, A.M. Salivary, blood and plasma nitrite concentrations in periodontal patients and healthy individuals before and after periodontal treatment. Clin. Chim. Acta 2015, 444, 293–296. [Google Scholar] [CrossRef] [PubMed]
- Scarel-Caminaga, R.; Cera, F.; Pigossi, S.; Finoti, L.; Kim, Y.; Viana, A.; Secolin, R.; Montenegro, M.; Tanus-Santos, J.; Orrico, S.; et al. Inducible Nitric Oxide Synthase Polymorphisms and Nitric Oxide Levels in Individuals with Chronic Periodontitis. Int. J. Mol. Sci. 2017, 18, 1128. [Google Scholar] [CrossRef] [Green Version]
- Maciejczyk, M.; Zalewska, A.; Gerreth, A.K. Salivary Redox Biomarkers in Selected Neurodegenerative Diseases. J. Clin. Med. 2020, 9, 497. [Google Scholar] [CrossRef] [Green Version]
- Klimiuk, A.; Zalewska, A.; Sawicki, R.; Knapp, M.; Maciejczyk, M. Salivary Oxidative Stress Increases with the Progression of Chronic Heart Failure. J. Clin. Med. 2020, 9, 769. [Google Scholar] [CrossRef] [Green Version]
- Żukowski, P.; Maciejczyk, M.; Waszkiel, D. Sources of free radicals and oxidative stress in the oral cavity. Arch. Oral Biol. 2018, 92, 8–17. [Google Scholar] [CrossRef]
- Isola, G.; Polizzi, A.; Muraglie, S.; Leonardi, R.; Lo Giudice, A. Assessment of Vitamin C and Antioxidant Profiles in Saliva and Serum in Patients with Periodontitis and Ischemic Heart Disease. Nutrients 2019, 11, 2956. [Google Scholar] [CrossRef] [Green Version]
- Isola, G.; Matarese, G.; Williams, R.C.; Siciliano, V.I.; Alibrandi, A.; Cordasco, G.; Ramaglia, L. The effects of a desiccant agent in the treatment of chronic periodontitis: A randomized, controlled clinical trial. Clin. Oral Investig. 2018, 22, 791–800. [Google Scholar] [CrossRef]
- Toczewska, J.; Konopka, T. Activity of enzymatic antioxidants in periodontitis: A systematic overview of the literature. Dent. Med. Probl. 2019, 56, 419–426. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control | Stage III | Stage IV | All Stages | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Median | Min | Max | Mean | SD | Median | Min | Max | Mean | SD | Median | Min | Max | Mean | SD | Median | Min | Max | ||
| age | 40.3 | 9.58 | 39 | 20 | 55 | 43.3 | 8.99 | 45 | 20 | 55 | 44 | 8.03 | 45 | 29 | 55 | 43.6 | 8.56 | 45 | 20 | 55 | |
| sex | women | 17 (57%) | 17 (47%) | 13 (54%) | 30 (50%) | ||||||||||||||||
| men | 13 (43%) | 19 (53%) | 11 (46%) | 30 (50%) | |||||||||||||||||
| non-stimulated saliva flow (mL/min) | 0.42 | 0.19 | 0.4 | 0.2 | 1 | 0.41 | 0.22 | 0.375 | 0.1 | 1 | 0.5 | 0.3 | 0.45 | 0.1 | 1.3 | 0.45 | 0.26 | 0.4 | 0.1 | 1.3 | |
| stimulated saliva flow (mL/min) | 1.74 | 0.75 | 1.55 | 0.4 | 3.4 | 1.43 | 0.66 | 1.4 | 0.3 | 3 | 1.47 | 0.67 | 1.4 | 0.6 | 3 | 1.45 | 0.66 | 1.4 | 0.3 | 3 | |
| protein in non-stimulated saliva (µg/mL) | 633.13 | 189.88 | 624.16 | 300.45 | 1101 | 865.87 | 237.05 | 824.55 | 481.23 | 1387 | 898.13 | 451.84 | 839.62 | 23.48 | 1847.1 | 879.15 | 338.4 | 827.95 | 23.48 | 1847.1 | |
| protein in stimulated saliva (µg/mL) | 592.16 | 160.87 | 599.74 | 235.74 | 946.29 | 594.85 | 179.63 | 626.28 | 28.91 | 926.41 | 554.59 | 217.35 | 634.78 | 42.74 | 811.92 | 577.99 | 193.06 | 634.78 | 28.91 | 926.41 | |
| protein in gingival fluid (µg/mL) | 39.23 | 21.56 | 31.22 | 8.44 | 91.66 | 132.30 | 69.83 | 130.43 | 36.8 | 336.97 | 178.78 | 109.71 | 134.24 | 45.5 | 445.64 | 151.82 | 90.75 | 131.13 | 36.8 | 445.64 | |
| number of teeth | 26.1 | 2.63 | 27.5 | 19 | 28 | 26.86 | 1.53 | 27.5 | 21 | 28 | 22.21 | 4 | 23 | 15 | 28 | 25 | 3.59 | 26 | 15 | 28 | |
| PI | 22.22 | 16.16 | 20.5 | 0 | 79 | 45.25 | 25.59 | 43 | 9 | 100 | 49.79 | 32.14 | 43.5 | 0 | 100 | 47.07 | 28.21 | 43.5 | 0 | 100 | |
| API | 36.87 | 16.27 | 32 | 7 | 68 | 64.06 | 21.26 | 65 | 29 | 100 | 77.54 | 23.41 | 86.5 | 22 | 100 | 69.45 | 23.14 | 72.5 | 22 | 100 | |
| BoP | 11.8 | 7.34 | 9.5 | 0.7 | 26 | 45.12 | 27.66 | 41 | 4 | 100 | 63.38 | 28.70 | 61 | 17 | 100 | 52.42 | 29.26 | 46.5 | 4 | 100 | |
| PD | 1.74 | 0.32 | 1.7 | 1.2 | 2.3 | 3.19 | 0.66 | 3.15 | 2.1 | 5.3 | 4 | 0.61 | 4.1 | 2.7 | 5.4 | 3.51 | 0.75 | 3.5 | 2.1 | 5.4 | |
| mean CAL > 0 | 2.26 | 1.17 | 2.1 | 1 | 5.2 | 4.74 | 1.4 | 4.65 | 2.4 | 8.1 | 6.1 | 1.75 | 6.05 | 3 | 10.1 | 5.29 | 1.68 | 5.4 | 2.4 | 10.1 | |
| Author, Year and Country | Fluid Method | Study Group Size and Age | p for Perio | Other Data |
|---|---|---|---|---|
| Aurer et al. [7], 2001, Croatia | NS saliva S saliva Griess reaction | AgP, 25 (19–35) CP, 25 (39–59) HP, 25 (21–42) | NS saliva ↓ NO p < 0.001 S saliva ↓ NO p < 0.05 | Decrease depends on periodontitis severity |
| Menaka et al. [24], 2009, India | Serum Griess reaction | CP, 30 (18–45) HP, 30 (18–45) | ↑ NO p = 0.000 | |
| Dhotre et al. [25], 2011, India | NS saliva Serum Cortas and Wakid method | P, 100 (mean 52.7) HP, 100 (mean 50.3) | Saliva ↑ NO p < 0.001 serum ↑ NO p < 0.001 | |
| Parwani et al. [6], 2012, India | NS saliva Griess reaction | CP, 30 (20–60) HP, 30 (20–60) | ↑ NO p = 0.000 | Positive correlation with PD |
| Sundar et al. [26], 2013, India | NS saliva Serum Griess reaction | AgP, 20 (25–35) CP, 20 (35–55) HP, 20 (25–55) | Saliva ↑ NO p < 0.001 serum ↑ NO p < 0.001 | Positive correlation for both with plaque, GI, PD, CAL, and concentration for saliva and serum |
| Andrukhov et al. [27], 2013, Austria | NS saliva (nitrite) Serum Griess reaction | Severe P, 89 (mean 34.3) HP, 54 (mean 42.2) | Saliva ↓ NO p < 0.01 serum ↓ NO p < 0.01 | No correlation between saliva and serum |
| Wadhwa et al. [28], 2013, India | NS saliva Serum Griess reaction | CP, 20 (no data) HP, 20 (no data) | Saliva ↑ NO p < 0.05 serum ↑ NO p < 0.05 | |
| Poorsattar Bejeh- Mir [29], 2014, Iran | GCF NS saliva ELISA | P, 14 (mean 38.3) HP, 14 (mean 37.7) | GCF ↓ NO p < 0.001 saliva ↑ NO p = 0.007 | Sensitivity and specificity for NO in saliva in periodontitis is 0.93 and 0.96 |
| Wattamwar et al. [30], 2016, India | NS saliva Serum Griess reaction | CP, 20 (30–55) | saliva ↑ NO p < 0.001 versus serum | Significant correlation for both with plaque, GI, PD, CAL, and between saliva and serum |
| Own study | GCF NS saliva S saliva Griess reaction | P, 60 (20–55) HP, 30 (20–55) | GCF, n.s. serum ↑ NO p < 0.001 | In severe P in GCF positive correlation with interproximal CAL |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Toczewska, J.; Konopka, T.; Zalewska, A.; Maciejczyk, M. Nitrosative Stress Biomarkers in the Non-Stimulated and Stimulated Saliva, as well as Gingival Crevicular Fluid of Patients with Periodontitis: Review and Clinical Study. Antioxidants 2020, 9, 259. https://doi.org/10.3390/antiox9030259
Toczewska J, Konopka T, Zalewska A, Maciejczyk M. Nitrosative Stress Biomarkers in the Non-Stimulated and Stimulated Saliva, as well as Gingival Crevicular Fluid of Patients with Periodontitis: Review and Clinical Study. Antioxidants. 2020; 9(3):259. https://doi.org/10.3390/antiox9030259
Chicago/Turabian StyleToczewska, Joanna, Tomasz Konopka, Anna Zalewska, and Mateusz Maciejczyk. 2020. "Nitrosative Stress Biomarkers in the Non-Stimulated and Stimulated Saliva, as well as Gingival Crevicular Fluid of Patients with Periodontitis: Review and Clinical Study" Antioxidants 9, no. 3: 259. https://doi.org/10.3390/antiox9030259
APA StyleToczewska, J., Konopka, T., Zalewska, A., & Maciejczyk, M. (2020). Nitrosative Stress Biomarkers in the Non-Stimulated and Stimulated Saliva, as well as Gingival Crevicular Fluid of Patients with Periodontitis: Review and Clinical Study. Antioxidants, 9(3), 259. https://doi.org/10.3390/antiox9030259