Low-Osmolality Carbohydrate–Electrolyte Solution Ingestion Avoid Fluid Loss and Oxidative Stress after Exhaustive Endurance Exercise

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. LCS
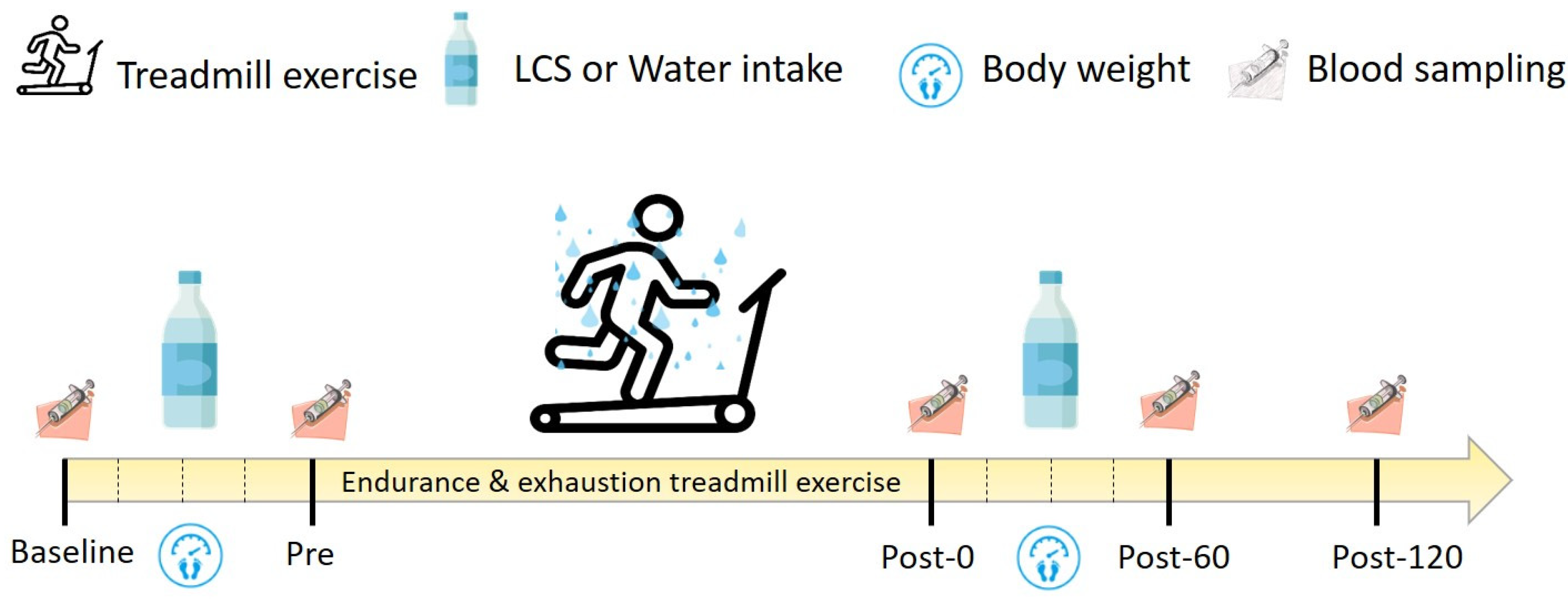
2.3. Experimental Design
2.4. Maximal Oxygen Consumption Assessment and Exercise Intensity
2.5. Biochemical Variables
2.6. Oxidative Stress Evaluation
2.7. Statistics
3. Results
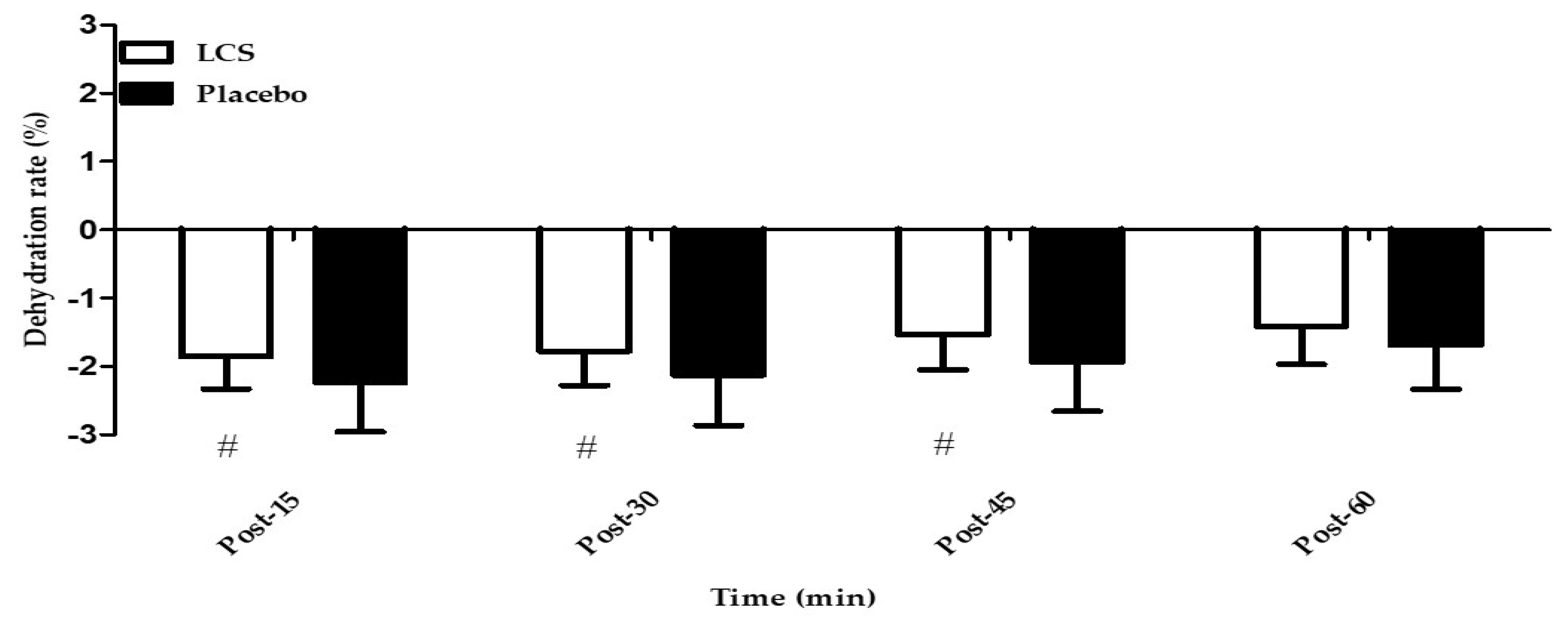
3.1. Effects of LCS on EEE-Induced Dehydration
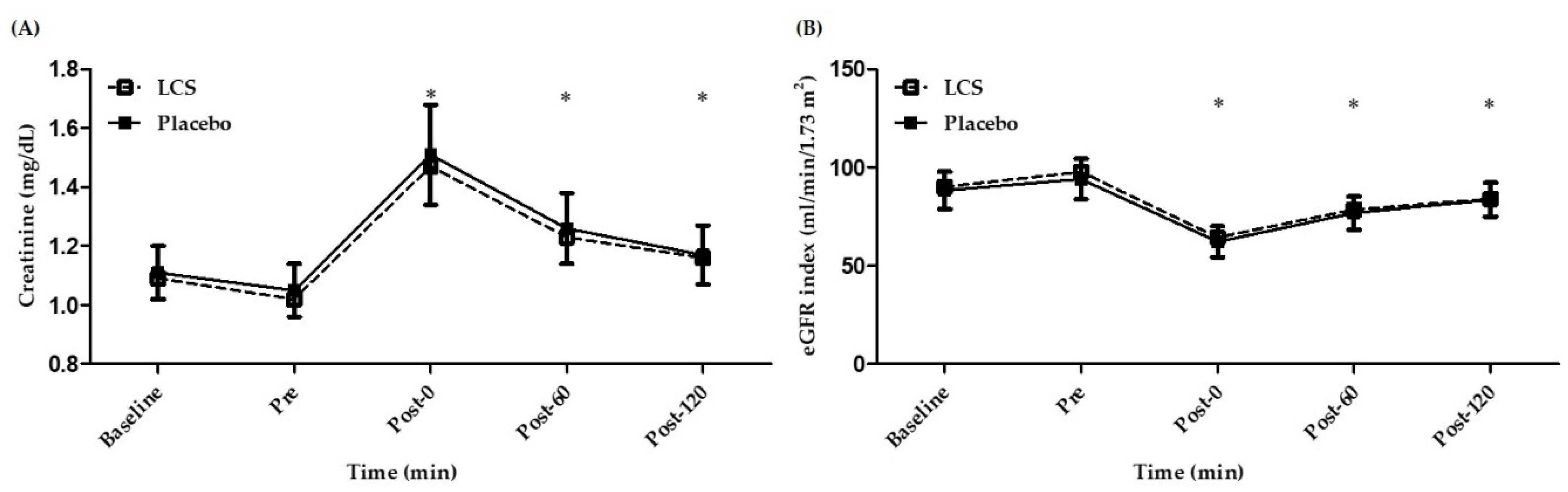
3.2. Effects of LCS on Renal Function During EEE
3.3. Effects of LCS on Electrolytes and Osmolality
3.4. Effects of LCS on Oxidative Stress, Antioxidative Capacity, and Inflammation During EEE
3.5. Effects of LCS on Aerobic Capacity
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Riebl, S.K.; Davy, B.M. The hydration equation: Update on water balance and cognitive performance. ACSMs. Health Fit. J. 2013, 17, 21–28. [Google Scholar]
- Thomas, D.T.; Erdman, K.A.; Burke, L.M. American college of sports medicine joint position statement. Nutrition and athletic performance. Med. Sci. Sports Exerc. 2016, 48, 543–568. [Google Scholar]
- Chen, J.; Wan, C.M.; Gong, S.T.; Fang, F.; Sun, M.; Qian, Y.; Huang, Y.; Wang, B.X.; Xu, C.D.; Ye, L.Y.; et al. Chinese clinical practice guidelines for acute infectious diarrhea in children. World J. Pediatr. 2018, 14, 429–436. [Google Scholar] [CrossRef]
- Atia, A.N.; Buchman, A.L. Oral rehydration solutions in non-cholera diarrhea: A review. Am. J. Gastroenterol. 2009, 104, 2596–2604. [Google Scholar] [CrossRef]
- Hew-Butler, T.; Loi, V.; Pani, A.; Rosner, M.H. Exercise-associated hyponatremia: 2017 Update. Front. Med. 2017, 4, 370. [Google Scholar] [CrossRef] [Green Version]
- Kamaruddin, H.K.; Ooi, C.H.; Mündel, T.; Aziz, A.R.; Che Muhamed, A.M. The ergogenic potency of carbohydrate mouth rinse on endurance running performance of dehydrated athletes. Eur. J. Appl. Physiol. 2019, 119, 1711–1723. [Google Scholar] [CrossRef]
- Deshayes, T.A.; Jeker, D.; Goulet, E.D.B. Impact of pre-exercise hypohydration on aerobic exercise performance, peak oxygen consumption and oxygen consumption at lactate threshold: A systematic review with meta-analysis. Sports Med. 2020, 50, 581–596. [Google Scholar] [CrossRef] [PubMed]
- Sawka, M.N.; Burke, L.M.; Eichner, E.R.; Maughan, R.J.; Montain, S.J.; Stachenfeld, N.S. American college of sports medicine position stand. Exercise & fluid replacement. Med. Sci. Sports Exerc. 2007, 39, 377–390. [Google Scholar] [PubMed] [Green Version]
- Adams, W.M.; Vandermark, L.W.; Belval, L.N.; Casa, D.J. The utility of thirst as a measure of hydration status following exercise-induced dehydration. Nutrients 2019, 11, 2689. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faraco, G.; Wijasa, T.S.; Park, L.; Moore, J.; Anrather, J.; Ladecola, C. Water deprivation induces neurovascular and cognitive dysfunction through vasopressin-induced oxidative stress. J. Cereb. Blood Flow Metab. 2014, 34, 852–860. [Google Scholar] [CrossRef] [Green Version]
- Tan, B.L.; Norhaizan, M.E.; Liew, W.P.; Sulaiman Rahman, H. Antioxidant and oxidative stress: A mutual interplay in age-related diseases. Front. Pharmacol. 2018, 9, 1162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nieman, D.C.; Valacchi, G.; Wentz, L.M.; Ferrara, F.; Pecorelli, A.; Woodby, B.; Sakaguchi, C.A.; Simonson, A. Mixed flavonoid supplementation attenuates postexercise plasma levels of 4-hydroxynonenal and protein carbonyls in endurance athletes. Int. J. Sport Nutr. Exerc. Metab. 2019, 21, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Akbari-Fakhrabadi, M.; Najafi, M.; Mortazavian, S.; Rasouli, M.; Memari, A.H.; Shidfar, F. Effect of saffron (Crocus sativus L.) and endurance training on mitochondrial biogenesis, endurance capacity, inflammation, antioxidant, and metabolic biomarkers in Wistar rats. J. Food Biochem. 2019, 43, e12946. [Google Scholar] [CrossRef] [PubMed]
- Sousa, C.V.; Aguiar, S.S.; Deus, L.; Barbosa, L.P.; Dos Santos, P.A.; Neves, R.V.P.; Maciel, L.A.; Moraes, M.R.; Moreira, S.R.; Campbell, C.S.G.; et al. Faster and healthier: Relationship between telomere and performance in master athletes. Int. J. Sports Med. 2020, in press. [Google Scholar] [CrossRef]
- O’Neal, E.K.; Wingo, J.E.; Richardson, M.T.; Leeper, J.D.; Neggers, Y.H.; Bishop, P.A. Half-marathon and full-marathon runners’ hydration practices and perceptions. J. Athl. Train. 2011, 46, 581–591. [Google Scholar] [CrossRef] [Green Version]
- Knechtle, B.; Chlíbková, D.; Papadopoulou, S.; Mantzorou, M.; Rosemann, T.; Nikolaidis, P.T. Exercise-associated hyponatremia in endurance and ultra-endurance performance-aspects of sex, race location, ambient temperature, sports discipline, and length of performance: A narrative review. Medicina 2019, 55, 537. [Google Scholar] [CrossRef] [Green Version]
- Noakes, T.D. Drinking guidelines for exercise: What evidence is there that athletes should drink “as much as tolerable”, “to replace the weight lost during exercise” or “adlibitum”? J. Sports Sci. 2007, 25, 781–796. [Google Scholar] [CrossRef]
- Evans, G.H.; James, L.J.; Shirreffs, S.M.; Maughan, R.J. Optimizing the restoration and maintenance of fluid balance after exercise-induced dehydration. J. Appl. Physiol. 2017, 122, 945–951. [Google Scholar] [CrossRef]
- Ho, C.F.; Shih, C.Y.; Chan, K.H.; Wang, T.Y. Effect of uphill high-intensity interval training on aerobic capacity and power of lower extremity in basketball players. Sports Exerc. Res. 2012, 14, 476–482. [Google Scholar]
- Lee, S.C.; Lim, L.M.; Chang, E.E.; Chiu, Y.W.; Hwang, S.J.; Chen, H.C. Effect of differences in serum creatinine estimation methodologies on estimated glomerular filtration rate. Singap. Med. J. 2019, 60, 468–473. [Google Scholar] [CrossRef] [Green Version]
- Goulet, E.D. Dehydration and endurance performance in competitive athletes. Nutr. Rev. 2012, 70, S132–S136. [Google Scholar] [CrossRef] [PubMed]
- Casa, D.J.; Armstrong, L.E.; Hillman, S.K.; Montain, S.J.; Reiff, R.V.; Rich, B.S.; Roberts, W.O.; Stone, J.A. National athletic trainers’ association position statement: Fluid replacement for athletes. J. Athl. Train. 2000, 35, 212–224. [Google Scholar] [PubMed]
- Rosner, M.H. Exercise-associated hyponatremia. Trans. Am. Clin. Climatol. Assoc. 2019, 130, 76–87. [Google Scholar] [PubMed]
- Magee, P.J.; Gallagher, A.M.; McCormack, J.M. High Prevalence of dehydration and inadequate nutritional knowledge among university and club level athletes. Int. J. Sport Nutr. Exerc. Metab. 2017, 27, 158–168. [Google Scholar] [CrossRef] [PubMed]
- Jahic, D.; Begic, E. Exercise-associated muscle cramp-doubts about the cause. Mater. Sociomed. 2018, 30, 67–69. [Google Scholar] [CrossRef] [Green Version]
- Lau, W.Y.; Kato, H.; Nosaka, K. Water intake after dehydration makes muscles more susceptible to cramp but electrolytes reverse that effect. BMJ Open Sport Exerc. Med. 2019, 5, e000478. [Google Scholar] [CrossRef] [Green Version]
- Miller, K.C. Plasma potassium concentration and content changes after banana ingestion in exercised men. J. Athl. Train. 2012, 47, 648–654. [Google Scholar] [CrossRef] [Green Version]
- Lippi, G.; Schena, F.; Salvagno, G.L.; Tarperi, C.; Montagnana, M.; Gelati, M.; Banfi, G.; Guidi, G.C. Acute variation of estimated glomerular filtration rate following a half-marathon run. Int. J. Sports Med. 2008, 29, 948–951. [Google Scholar] [CrossRef]
- Bongers, C.; Alsady, M.; Nijenhuis, T.; Tulp, A.; Eijsvogels, T.; Deen, P.; Hopman, M. Impact of acute versus prolonged exercise and dehydration on kidney function and injury. Physiol. Rep. 2018, 6, e13734. [Google Scholar] [CrossRef]
- Lipman, G.S.; Shea, K.; Christensen, M.; Phillips, C.; Burns, P.; Higbee, R.; Koskenoja, V.; Eifling, K.; Krabak, B.J. Ibuprofen versus placebo effect on acute kidney injury in ultramarathons: A randomised controlled trial. Emerg. Med. J. 2017, 34, 637–642. [Google Scholar] [CrossRef] [Green Version]
- Belli, T.; Macedo, D.V.; de Araújo, G.G.; Dos Reis, I.G.M.; Scariot, P.P.M.; Lazarim, F.L.; Nunes, L.A.S.; Brenzikofer, R.; Gobatto, C.A. Mountain ultramarathon induces early increases of muscle damage, inflammation, and risk for acute renal injury. Front. Physiol. 2018, 9, 1368. [Google Scholar] [CrossRef] [PubMed]
- Radak, Z.; Zhao, Z.; Koltai, E.; Ohno, H.; Atalay, M. Oxygen consumption and usage during physical exercise: The balance between oxidative stress and ROS-dependent adaptive signaling. Antioxid. Redox Signal. 2013, 18, 1208–1246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kawamura, T.; Muraoka, I. Exercise-induced oxidative stress and the effects of antioxidant intake from a physiological viewpoint. Antioxidants 2018, 7, 119. [Google Scholar] [CrossRef] [Green Version]
- Vezzoli, A.; Dellanoce, C.; Mrakic-Sposta, S.; Montorsi, M.; Moretti, S.; Tonini, A.; Pratali, L.; Accinni, R. Oxidative stress assessment in response to ultraendurance exercise: Thiols redox status and ROS production according to duration of a competitive race. Oxid. Med. Cell. Longev. 2016, 2016, 6439037. [Google Scholar] [CrossRef] [Green Version]
- Kenefick, R.W. Drinking strategies: Planned drinking versus drinking to thirst. Sports Med. 2018, 48, 31–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheuvront, S.N.; Kenefick, R.W. Dehydration: Physiology, assessment, and performance effects. Compr. Physiol. 2014, 4, 257–285. [Google Scholar] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Parameters | Baseline | Pre | Post-0 | Post-60 | Post-120 |
|---|---|---|---|---|---|
| Na+ (mmol/L) | |||||
| LCS | 140.25 ± 0.75 (0.54%) | 140.50 ± 0.67 * (0.48%) | 143.50 ± 1.83 *,‡ (1.28%) | 141.67 ± 1.44 *,‡,+ (1.01%) | 141.25 ± 1.77 *,+ (1.25%) |
| Placebo | 140.50 ± 1.68 (1.19%) | 140.58 ± 1.17 (0.82%) | 143.92 ± 1.88 *,‡ (1.31%) | 141.17 ± 1.27 ‡,+ (0.90%) | 140.75 ± 1.42 +,† (1.01%) |
| Cl− (mmol/L) | |||||
| LCS | 102.17 ± 1.64 (1.61%) | 102.92 ± 1.98 * (1.92%) | 104.50 ± 1.68 *,‡,# (1.61%) | 103.00 ± 1.76 + (1.71%) | 102.67 ± 1.50 + (1.46%) |
| Placebo | 103.25 ± 1.48 (1.44%) | 103.83 ± 1.40 (1.35%) | 105.92 ± 1.31 *,‡ (1.24%) | 103.42 ± 1.68 + (1.62%) | 103.33 ± 1.92 + (1.86%) |
| K+ (mmol/L) | |||||
| LCS | 3.97 ± 0.28 (6.99%) | 4.07 ± 0.27 * (6.66%) | 4.26 ± 0.35 * (8.28%) | 4.70 ± 0.49 *,‡,+ (10.38%) | 4.50 ± 0.35 *,‡,† (7.70%) |
| Placebo | 4.08 ± 0.26 (6.34%) | 4.17 ± 0.30 (7.19%) | 4.30 ± 0.37 * (8.53%) | 4.63 ± 0.40 *,‡,+ (8.65%) | 4.33 ± 0.43 † (9.91%) |
| O (mOsm/L) | |||||
| LCS | 291.33 ± 2.10 (0.72%) | 289.67 ± 2.50 * (0.86%) | 299.58 ± 5.92 *, ‡ (1.97%) | 292.92 ± 3.87 ‡,+ (1.32%) | 292.17 ± 4.34 + (1.49%) |
| Placebo | 291.92 ± 3.15 (1.08%) | 290.33 ± 2.15 * (0.74%) | 301.00 ± 5.36 *,‡ (1.78%) | 291.75 ± 2.30 + (0.79%) | 290.25 ± 2.45 +,† (0.85%) |
| Parameters | Pre-U | Post-U |
|---|---|---|
| Na+ (mmol/L) | ||
| LCS | 41.71 ± 14.95 (35.84%) | 62.00 ± 47.22 (76.17%) |
| Placebo | 56.86 ± 24.35 (42.83%) | 60.29 ± 43.64 (72.39%) |
| Cl− (mmol/L) | ||
| LCS | 43.00 ± 12.94 (30.08%) | 63.43 ± 46.60 (73.46%) |
| Placebo | 61.43 ± 30.03 (48.89%) | 59.14 ± 37.03 (62.61%) |
| K− (mmol/L) | ||
| LCS | 10.54 ± 6.31 (59.83%) | 33.33 ± 13.96 * (41.87%) |
| Placebo | 15.60 ± 7.12 (45.63%) | 28.79 ± 16.01 (55.61%) |
| O (mOsm/L) | ||
| LCS | 294.43 ± 141.49 # (48.06%) | 350.10 ± 212.31 (60.64%) |
| Placebo | 349.43 ± 127.07 (36.36%) | 361.00 ± 230.49 (63.85) |
| Parameters | Baseline | Pre | Post-0 | Post-60 | Post-120 |
|---|---|---|---|---|---|
| TBARS (µM) | |||||
| LCS | 2.73 ± 0.52 (18.97%) | 2.79 ± 0.50 (17.89%) | 2.95 ± 0.70 (23.81%) | 2.68 ± 0.57 (21.40%) | 2.89 ± 0.54 (18.74%) |
| Placebo | 2.73 ± 0.44 (16.01%) | 2.85 ± 0.61 (21.46%) | 2.93 ± 0.49 (16.66%) | 2.88 ± 0.66 (22.97%) | 2.97 ± 0.60 (20.23%) |
| PC (nmol carbonyl/mg protein) | |||||
| LCS | 3.02 ± 0.58 (19.11%) | 2.87 ± 0.37 (13.05%) | 2.72 ± 0.31 *,# (11.52%) | 2.89 ± 0.52 (18.12%) | 2.77 ± 0.31 * (11.04%) |
| Placebo | 3.08 ± 0.67 (21.83%) | 3.01 ± 0.50 (16.54%) | 2.89 ± 0.43 (14.80%) | 2.89 ± 0.46 (15.93%) | 3.03 ± 0.98 (32.30%) |
| GPx (U) | |||||
| LCS | 1076.30 ± 180.54 (16.77%) | 1249.87 ± 195.95 (15.68%) | 1239.71 ± 275.29 (22.21%) | 1226.17 ± 256.26 (20.90%) | 1289.97 ± 214.49 (16.63%) |
| Placebo | 1270.44 ± 237.65 (18.71%) | 1313.28 ± 295.39 (22.49%) | 1364.84 ± 301.27 (22.07%) | 1347.40 ± 251.12 (18.64%) | 1274.61 ± 290.00 (22.75%) |
| SOD (U/mL) | |||||
| LCS | 5.18 ± 0.80 (15.45%) | 5.43 ± 0.56 (10.27%) | 6.15 ± 0.89 *,‡ (14.49%) | 5.94 ± 0.89 *,‡ (14.93%) | 6.02 ± 1.00 *,‡ (16.63%) |
| Placebo | 5.34 ± 0.51 (9.47%) | 5.40 ± 0.63 (11.65%) | 5.78 ± 0.78 (13.47%) | 5.95 ± 1.30 (21.82%) | 5.60 ± 0.56 (9.96%) |
| CAT (nmol/min/mL) | |||||
| LCS | 1270.56 ± 246.95 (19.44%) | 1340.99 ± 266.67 (19.89%) | 2046.21 ± 381.98 *,‡,# (18.67%) | 1565.47 ± 367.23 *,‡,+ (23.46%) | 1677.25 ± 395.63 *,‡,+ (23.59%) |
| Placebo | 1337.18 ± 386.32 (28.89%) | 1471.97 ± 302.45 (20.55%) | 1820.37 ± 417.35 *,‡ (22.93%) | 1623.01 ± 443.46 (27.32%) | 1694.80 ± 419.63 *,‡ (24.76%) |
| CRP (mg/dL) | |||||
| LCS | 0.06 ± 0.06 (95.43%) | 0.06 ± 0.06 (97.85%) | 0.07 ± 0.06 *,‡ (96.28%) | 0.06 ± 0.06 + (94.18%) | 0.06 ± 0.06 + (96.68%) |
| Placebo | 0.08 ± 0.13 (165.62%) | 0.08 ± 0.13 (163.30%) | 0.09 ± 0.14 (159.70%) | 0.08 ± 0.13 (163.03%) | 0.08 ± 0.14 (162.88%) |
| Parameters | Exhaustion (min) | MHR (beats/min) | (mL/kg/min) |
|---|---|---|---|
| LCS | 63.13 ± 3.35 (5.30%) | 198.58 ± 9.97 (5.02%) | 52.33 ± 6.66 (12.72%) |
| Placebo | 63.28 ± 3.37 (5.33%) | 198.00 ± 9.49 (4.79%) | 53.11 ± 6.44 (12.13%) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, W.-C.; Tung, Y.-T.; Wu, M.-S.; Liu, M.-C.; Lin, T.-J.; Yang, M.-T. Low-Osmolality Carbohydrate–Electrolyte Solution Ingestion Avoid Fluid Loss and Oxidative Stress after Exhaustive Endurance Exercise. Antioxidants 2020, 9, 336. https://doi.org/10.3390/antiox9040336
Huang W-C, Tung Y-T, Wu M-S, Liu M-C, Lin T-J, Yang M-T. Low-Osmolality Carbohydrate–Electrolyte Solution Ingestion Avoid Fluid Loss and Oxidative Stress after Exhaustive Endurance Exercise. Antioxidants. 2020; 9(4):336. https://doi.org/10.3390/antiox9040336
Chicago/Turabian StyleHuang, Wen-Ching, Yu-Tang Tung, Mai-Szu Wu, Ming-Che Liu, Tsai-Jung Lin, and Ming-Ta Yang. 2020. "Low-Osmolality Carbohydrate–Electrolyte Solution Ingestion Avoid Fluid Loss and Oxidative Stress after Exhaustive Endurance Exercise" Antioxidants 9, no. 4: 336. https://doi.org/10.3390/antiox9040336
APA StyleHuang, W. -C., Tung, Y. -T., Wu, M. -S., Liu, M. -C., Lin, T. -J., & Yang, M. -T. (2020). Low-Osmolality Carbohydrate–Electrolyte Solution Ingestion Avoid Fluid Loss and Oxidative Stress after Exhaustive Endurance Exercise. Antioxidants, 9(4), 336. https://doi.org/10.3390/antiox9040336