
COVID-19 Vaccine Hesitancy among Parents of Children with Chronic Liver Diseases

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Setting
2.2. Population, Sample Size, and Sampling Technique
2.3. Data Collection Questionnaire
2.4. Ethical Considerations
2.5. Statistical Data Analysis
3. Results
3.1. Parents’ Characteristics
3.2. Characteristics of Children
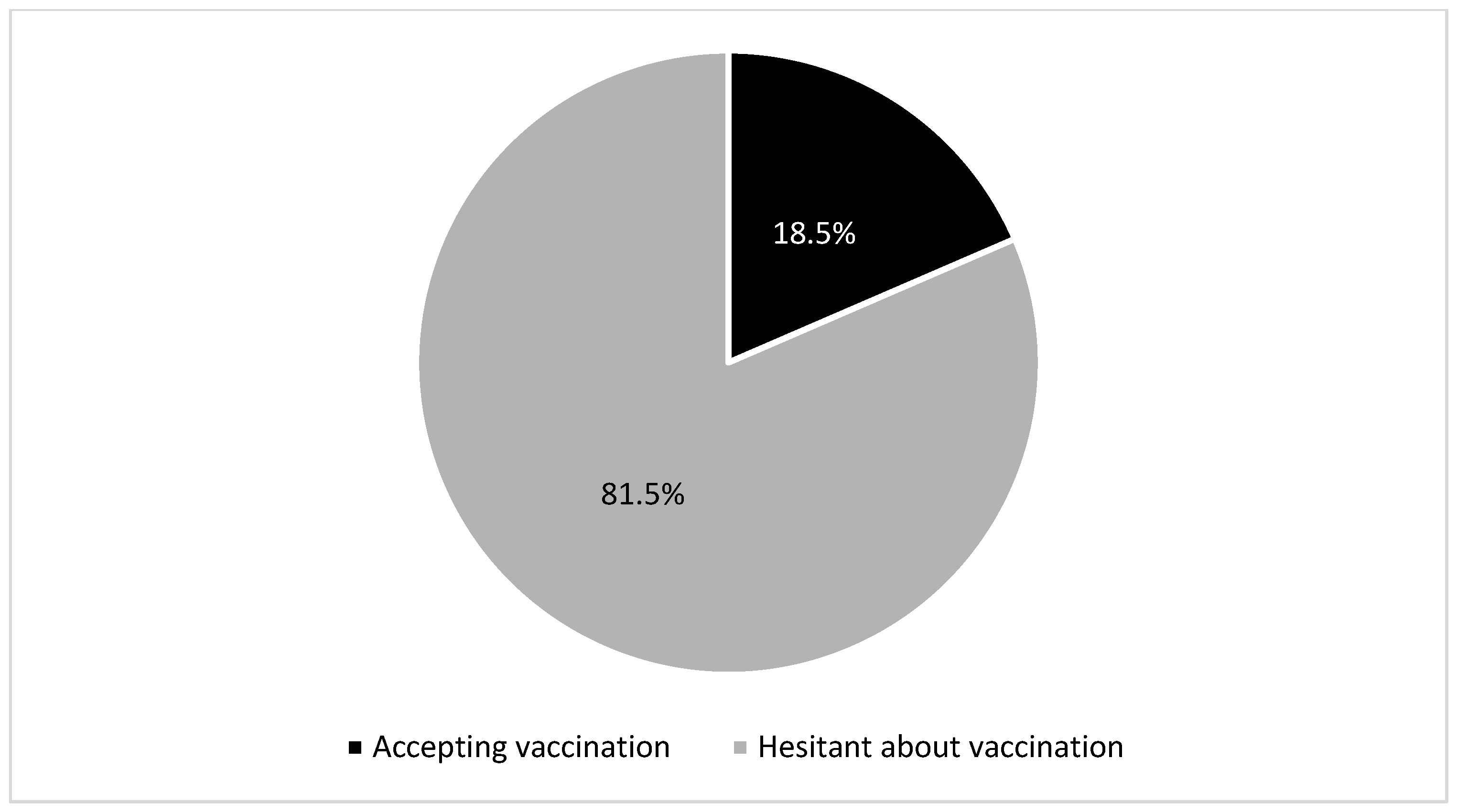
3.3. Proportion of Parents Hesitant about COVID-19 Vaccination
3.4. Parents’ and Children’s Characteristics Affecting COVID-19 VH
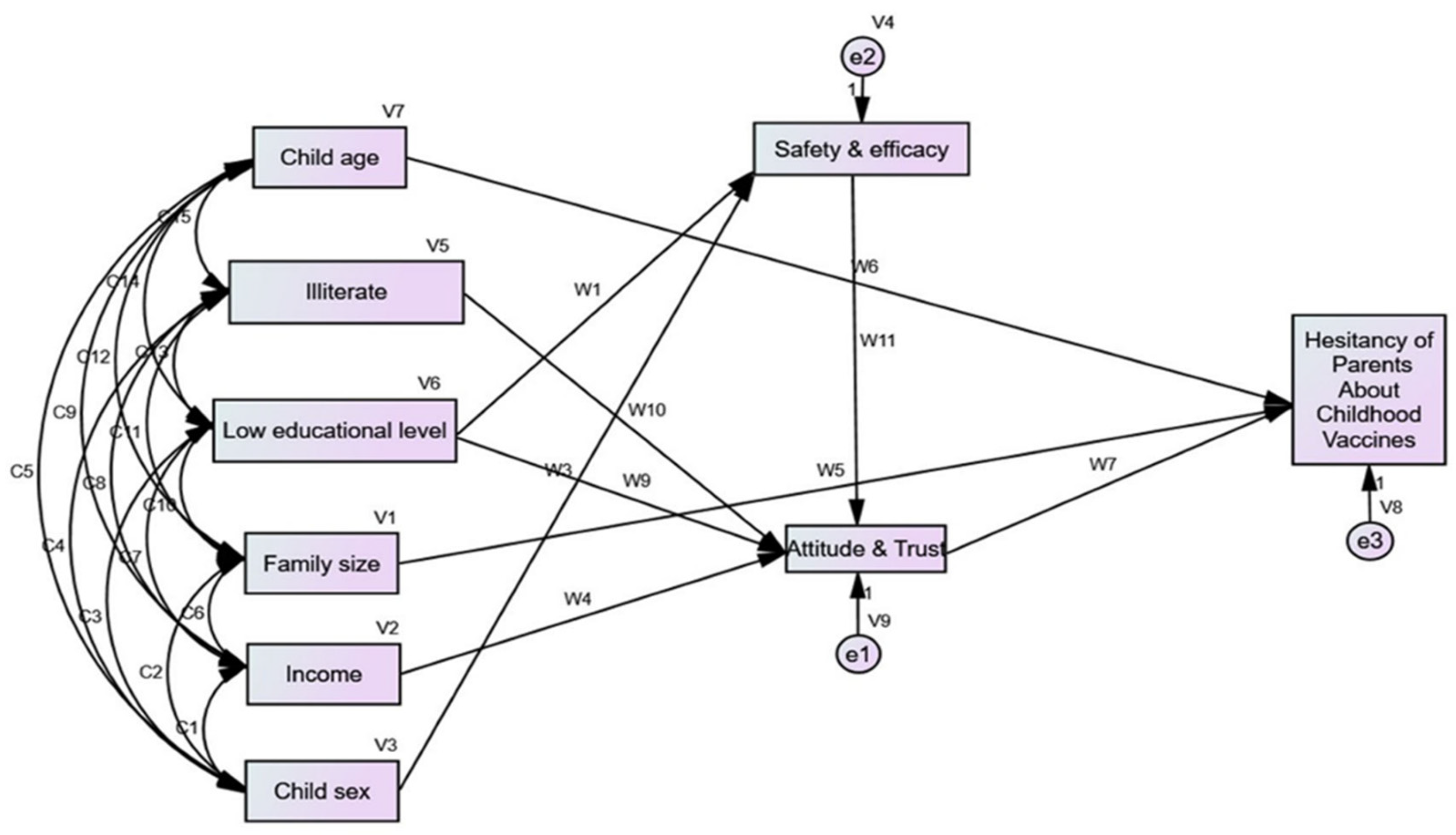
3.5. Structural Equation Model
3.6. Discriminant Analysis
4. Discussion
4.1. Vaccination Hesitancy
4.2. Determinants of Vaccination Hesitancy
4.3. Trust and Attitude
4.4. Safety and Efficacy
4.5. Limitations and Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| COVID-19 | Coronavirus disease 2019 |
| SARS-CoV-2 | Acute respiratory syndrome coronavirus 2 |
| WHO | World Health Organization |
| CLD | Chronic liver diseases |
| CDC | The Centers for Disease and Control |
| VH | Vaccine hesitancy |
| RMSR | Root mean square residual |
| GFI | The goodness of fit index |
| CFI | Comparative fit index |
| RMSEA | Root mean square error of approximation |
| VIF | Variance inflation factor |
References
- World Health Organization. WHO Coronavirus Disease (COVID-19) Dashboard with Vaccination Data. 2022. Available online: https://covid19.who.int/%0Ahttps://covid19.who.int/%0Ahttps://covid19.who.int/region/searo/country/bd (accessed on 4 November 2022).
- UNICEF. COVID-19 Confirmed Cases and Deaths-UNICEF DATA. 2022. Available online: https://data.unicef.org/resources/covid-19-confirmed-cases-and-deaths-dashboard/ (accessed on 29 June 2022).
- American Academy of Pediatrics. Children and COVID-19: State-Level Data Report. 2022. Available online: https://www.aap.org/en/pages/2019-novel-coronavirus-covid-19-infections/children-and-covid-19-state-level-data-report/ (accessed on 24 October 2022).
- World Health Organization. Egypt: WHO Coronavirus Disease (COVID-19) Dashboard with Vaccination Data. 2022. Available online: https://covid19.who.int/region/emro/country/eg (accessed on 4 November 2022).
- UNICEF. COVID-19 in Egypt Key Highlights; UNICEF: New York, NY, USA, 2020; Volume 2019, pp. 1–8. Available online: https://covid19 (accessed on 30 June 2022).
- Ghazy, R.M.; Taha, S.H.N.; Elhadi, Y.A.M. Letter from Egypt. Respirology 2022, 27, 242–244. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Coronavirus Disease (COVID-19): Vaccines. 2022. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/question-and-answers-hub/q-a-detail/coronavirus-disease-(covid-19)-vaccines?adgroupsurvey=%7Badgroupsurvey%7D&gclid=CjwKCAjwqJSaBhBUEiwAg5W9pzyjMoMQEaNbYdBThNPdFTaaHFpiHXnEHa3v6diy7PyIl9kok5E (accessed on 11 October 2022).
- World Health Organization. Interim Statement on COVID-19 Vaccination for Children and Adolescents. 2021. Available online: https://www.who.int/news/item/24-11-2021-interim-statement-on-covid-19-vaccination-for-children-and-adolescents (accessed on 28 August 2022).
- UNICEF. Child Mortality and COVID-19. 2022. Available online: https://data.unicef.org/topic/child-survival/covid-19/ (accessed on 11 October 2022).
- Kompaniyets, L.; Agathis, N.T.; Nelson, J.M.; Preston, L.E.; Ko, J.Y.; Belay, B.; Pennington, A.F.; Danielson, M.L.; Desisto, C.L.; Chevinsky, J.R.; et al. Underlying medical conditions associated with severe COVID-19 illness among children. JAMA Netw. Open 2021, 4, e2111182. [Google Scholar] [CrossRef] [PubMed]
- Evliyaoğlu, O. Children with chronic disease and COVID-19 Kronik hastalığı olan çocuklar ve COVID-19. Turk. Arch. Pediatr. 2020, 55, 93–94. [Google Scholar] [CrossRef]
- Center for Diseases Prevention and Control. “COVID-19 Vaccines for Children and Teens,” Centers for Disease Control and Prevention. 2022. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/recommendations/children-teens.html (accessed on 29 August 2022).
- Center for Diseases Prevention and Control. Pfizer-BioNTech COVID-19 Vaccine Overview and Safety. 2022. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/different-vaccines/Pfizer-BioNTech.html (accessed on 29 August 2022).
- Center for Diseases Prevention and Control. Moderna COVID19 Vaccine Overview and Safty. 2022. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/different-vaccines/Moderna.html (accessed on 29 August 2022).
- Center for Diseases Prevention and Control. Novavax COVID-19, Adjuvanted Vaccine: Overview and Safety. 2022. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/novavax.html (accessed on 29 August 2022).
- Ahram Online. Egypt to Vaccinate 12–15 Years Old Children against Coronavirus: Cabinet. 2022. Available online: https://english.ahram.org.eg/News/443448.aspx (accessed on 11 October 2022).
- Sharma, A.; Nagalli, S. Chronic Liver Disease; StatPearls Publishing: Orlando, FL, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK554597/ (accessed on 14 October 2022).
- Abdullatif, H.; Elakel, W.; Baroudy, S.; El-Karaksy, H.; Mogahed, E.A. COVID-19 pandemic in Egyptian children with liver diseases: Incidence and impact on health care service delivery in a low/middle income country. Arab J. Gastroenterol. 2022, 23, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Institute for Health Metrics and Evaluation (IHME). Global Burden of Disease Study 2019 (GBD 2019) Results. 2020. Available online: https://vizhub.healthdata.org/gbd-results/ (accessed on 23 October 2022).
- Rozek, L.S.; Jones, P.; Menon, A.; Hicken, A.; Apsley, S.; King, E.J. Understanding vaccine hesitancy in the context of COVID-19: The role of trust and confidence in a seventeen-country survey. Int. J. Public Health 2021, 66, 636255. [Google Scholar] [CrossRef]
- World Health Organization. Behavioural Considerations for Acceptance and Uptake of COVID-19 Vaccines; World Health Organization: Geneva, Switzerland, 2020; p. 18. Available online: https://apps.who.int/iris/bitstream/handle/10665/337335/9789240016927-eng.pdf (accessed on 20 June 2022).
- Alfieri, N.L.; Kusma, J.D.; Heard-Garris, N.; Davis, M.M.; Golbeck, E.; Barrera, L.; Macy, M.L. Parental COVID-19 vaccine hesitancy for children: Vulnerability in an urban hotspot. BMC Public Health 2021, 21, 1662. [Google Scholar] [CrossRef]
- Abdou, M.S.; Kheirallah, K.A.; Aly, M.O.; Ramadan, A.; Elhadi, Y.A.M.; Elbarazi, I.; Deghidy, E.A.; El Saeh, H.M.; Salem, K.M.; Ghazy, R.M. The coronavirus disease 2019 (COVID-19) vaccination psychological antecedent assessment using the Arabic 5c validated tool: An online survey in 13 Arab countries. PLoS ONE 2021, 16, e0260321. [Google Scholar] [CrossRef]
- Shaaban, R.; Ghazy, R.M.; Elsherif, F.; Ali, N.; Yakoub, Y.; Aly, M.; Elmakhzangy, R.; Abdou, M.S.; McKinna, B.; Elzorkany, A.M.; et al. COVID-19 vaccine acceptance among social media users: A content analysis, multi-continent study. Int. J. Environ. Res. Public Health 2022, 19, 5737. [Google Scholar] [CrossRef]
- Elbarazi, I.; Yacoub, M.; Reyad, O.A.; Abdou, M.S.; Elhadi, Y.A.M.; Kheirallah, K.A.; Ababneh, B.F.; Hamada, B.A.; El Saeh, H.M.; Ali, N.; et al. Exploring enablers and barriers toward COVID-19 vaccine acceptance among Arabs: A qualitative study. Int. J. Disaster Risk Reduct. 2022, 82, 103304. [Google Scholar] [CrossRef]
- ElHafeez, S.A.; Elbarazi, I.; Shaaban, R.; ElMakhzangy, R.; Aly, M.O.; Alnagar, A.; Yacoub, M.; El Saeh, H.M.; Eltaweel, N.; Alqutub, S.T.; et al. Arabic validation and cross-cultural adaptation of the 5C scale for assessment of COVID-19 vaccines psychological antecedents. PLoS ONE 2021, 16, e0254595. [Google Scholar] [CrossRef]
- Ghazy, R.M.; Abdou, M.S.; Awaidy, S.; Sallam, M.; Elbarazi, I.; Youssef, N.; Fiidow, O.A.; Mehdad, S.; Hussein, M.F.; Adam, M.F.; et al. Acceptance of COVID-19 vaccine booster doses using the health belief model: A cross-sectional study in low-middle- and high-income countries of the East Mediterranean region. Int. J. Environ. Res. Public Health 2022, 19, 12136. [Google Scholar] [CrossRef]
- Abdelmoneim, S.A.; Sallam, M.; Hafez, D.M.; Elrewany, E.; Mousli, H.M.; Hammad, E.M.; Elkhadry, S.W.; Adam, M.F.; Ghobashy, A.A.; Naguib, M.; et al. COVID-19 vaccine booster dose acceptance: Systematic review and meta-analysis. Trop. Med. Infect. Dis. 2022, 7, 252901278. [Google Scholar] [CrossRef]
- Drouin, O.; Fontaine, P.; Arnaud, Y.; Montmarquette, C.; Prud’homme, A.; Borgès, R.; Silva, D. Parental decision and intent towards COVID-19 vaccination in children with asthma: An econometric analysis. BMC Public Health 2021, 22, 1547. [Google Scholar] [CrossRef]
- OpenEpi-Toolkit Shell for Developing New Applications. Available online: http://www.openepi.com/SampleSize/SSPropor.htm (accessed on 15 April 2022).
- Elsayed, D.A.; Raad, E.B.; Bekhit, S.A.; Sallam, M.; Ibrahim, N.M.; Soliman, S.; Abdullah, R.; Farag, S.; Ghazy, R.M. Validation and cultural adaptation of the parent attitudes about childhood vaccines (PACV) questionnaire in Arabic language widely spoken in a region with a high prevalence of COVID-19 vaccine hesitancy. Trop. Med. Infect. Dis. 2022, 7, 234. [Google Scholar] [CrossRef]
- Opel, D.J.; Taylor, J.A.; Mangione-Smith, R.; Solomon, C.; Zhao, C.; Catz, S.; Martin, D. Validity and reliability of a survey to identify vaccine-hesitant parents. Vaccine 2011, 29, 6598–6605. [Google Scholar] [CrossRef]
- Alenezi, S.; Alarabi, M.; Al-Eyadhy, A.; Aljamaan, F.; Elbarazi, I.; Saddik, B.; Alhasan, K.; Assiri, R.; Bassrawi, R.; Alshahrani, F.; et al. Parental perceptions and the 5C psychological antecedents of COVID-19 vaccination during the first month of omicron variant surge: A large-scale cross-sectional survey in Saudi Arabia. Front. Pediatr. 2022, 10, 1386. [Google Scholar] [CrossRef]
- Orbea, M.; Cunningham, R.; Mary Healy, C.; Boom, J.A.; Bocchini, C. 1172. SARS-CoV-2 vaccine hesitancy in caregivers of hospitalized children. Open Forum Infect. Dis. 2021, 8 (Suppl. 1), S677. [Google Scholar] [CrossRef]
- Derdemezis, C.; Markozannes, G.; Rontogianni, M.O.; Trigki, M.; Kanellopoulou, A.; Papamichail, D.; Aretouli, E.; Ntzani, E.; Tsilidis, K.K. Parental hesitancy towards the established childhood vaccination programmes in the COVID-19 era: Assessing the drivers of a challenging public health concern. Vaccines 2022, 10, 814. [Google Scholar] [CrossRef]
- Ennaceur, S.; Al-Mohaithef, M. Parents’ willingness to vaccinate children against COVID-19 in Saudi Arabia: A cross-sectional study. Vaccines 2022, 10, 156. [Google Scholar] [CrossRef]
- Galanis, P.; Vraka, I.; Siskou, O.; Konstantakopoulou, O.; Katsiroumpa, A.; Kaitelidou, D. Uptake of COVID-19 vaccines among pregnant women: A systematic review and meta-analysis. Vaccines 2022, 10, 766. [Google Scholar] [CrossRef]
- Giambi, C.; Fabiani, M.; D’Ancona, F.; Ferrara, L.; Fiacchini, D.; Gallo, T.; Martinelli, D.; Pascucci, M.G.; Prato, R.; Filia, A.; et al. Parental vaccine hesitancy in Italy—Results from a national survey. Vaccine 2018, 36, 779–787. [Google Scholar] [CrossRef] [PubMed]
- Irvine, K.M.; Ratnasekera, I.; Powell, E.E.; Hume, D.A. Casuses and consequences of innate immune dysfucntion in cirrhosis. Front. Immunol. 2019, 10, 293. [Google Scholar] [CrossRef] [PubMed]
- Marjot, T.; Moon, A.M.; Cook, J.A.; Abd-Elsalam, S.; Aloman, C.; Armstrong, M.J.; Pose, E.; Brenner, E.J.; Cargill, T.; Catana, M.A.; et al. Outcomes following SARS-CoV-2 infection in patients with chronic liver disease: An international registry study. J. Hepatol. 2021, 74, 567–577. [Google Scholar] [CrossRef] [PubMed]
- Thuluvath, P.J.; Robarts, P.; Chauhan, M. Analysis of antibody responses after COVID-19 vaccination in liver transplant recipients and those with chronic liver diseases. J. Hepatol. 2021, 75, 1434–1439. [Google Scholar] [CrossRef] [PubMed]
- Ge, J.; Digitale, J.C.; Pletcher, M.J.; Lai, J.C.; The N3C Consortium. Breakthrough SARS-CoV-2 infection outcomes in vaccinated patients with chronic liver disease and cirrhosis: A national COVID cohort collaborative study. Hepatology 2022, 161, 1487–1501.e5. [Google Scholar] [CrossRef]
- ElSayed, D.A.; Bou Raad, E.; Bekhit, S.A.; Sallam, M.; Ibrahim, N.M.; Soliman, S.; Abdullah, R.; Farag, S.; Ghazy, R.M. Validation and Cultural Adaptation of the Parent Attitudes about Childhood Vaccines (PACV) Questionnaire in Arabic Language Widely Spoken in a Region with a High Prevalence of COVID-19 Vaccine Hesitancy. Trop. Med. Infect. Dis. 2022, 7, 234. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Category | N (%) |
|---|---|---|
| Gender | Female | 118 (68.2%) |
| Male | 55 (31.8%) | |
| Age | <40 years | 70 (40.5%) |
| ≥40 years | 103 (59.5%) | |
| Relation to the child | Father | 48 (27.7%) |
| Mother | 118 (68.2%) | |
| Others | 5 (3.5%) | |
| Level of education | Illiterate | 25 (14.5%) |
| Low educated 1 | 56 (32.4%) | |
| Medium to high educated 2 | 92 (53.2%) | |
| Workplace | Not employed | 107 (61.8%) |
| Government | 47 (27.2%) | |
| Private | 19 (11.0%) | |
| Work sector | Health | 6 (3.5%) |
| Non-Health | 167 (96.5%) | |
| Health insurance | No | 123 (71.1%) |
| Private | 6 (3.5%) | |
| Governmental | 44 (25.4%) | |
| Income | Not enough, on a loan and cannot pay back | 4 (2.3%) |
| Not enough, on a loan but can pay back | 14 (8.1%) | |
| Enough | 133 (76.9%) | |
| Enough and saving | 22 (12.7%) | |
| Older adults living in the same home | No | 111 (64.2%) |
| Yes | 62 (35.8%) | |
| Family size | 2–3 | 6 (3.5%) |
| 4–5 | 100 (57.8%) | |
| >5 | 67 (38.7%) | |
| Previous COVID-19 infection | No | 120 (69.4%) |
| Not Sure | 7 (4.0%) | |
| Yes | 46 (26.6%) | |
| COVID-19 vaccine status | Does not want to take the vaccine | 36 (20.8%) |
| Took the first dose and is awaiting the second | 22 (12.7%) | |
| Took the first dose but does not want to take the second dose | 7 (4.0%) | |
| Took the first and second doses and is awaiting the booster dose | 79 (45.7%) | |
| Took the first and second doses but did not want to take the booster dose | 4 (2.3%) | |
| Took the three doses | 18 (10.4%) | |
| Wants to take the vaccine, but it is not scheduled yet | 7 (4.0%) | |
| Chronically diseased parents | Yes | 26 (15.0%) |
| Variable | N (%) | |
|---|---|---|
| Sex | Female | 112 (64.7%) |
| Male | 61 (35.3%) | |
| Age | Mean ± SD | 12.77 ± 3.6 |
| Previous COVID-19 infection | No | 159 (91.9%) |
| Not sure | 5 (2.9%) | |
| Yes | 9 (3%) | |
| The child received the scheduled vaccine | Yes | 168 (97.1%) |
| The child received the influenza vaccine last 2 years | Yes | 8 (4.6%) |
| Parents’ intentions to allow COVID-19 vaccination | Already took the COVID vaccine | 32 (18.5%) |
| Hesitant | 141 (81.5%) | |
| Variable | Category | Parents’ Intention | Chi-Square Test | df | p. | ||
|---|---|---|---|---|---|---|---|
| Accepting Vaccination | Hesitant | ||||||
| Gender | Female | 16 (13.6%) | 102 (86.4%) | 6.003 | 1 | 0.014 * | |
| Male | 16 (29.1%) | 39 (70.9%) | |||||
| Age | <40 years | 5 (7.1%) | 65 (92.9%) | 10.054 | 1 | 0.002 * | |
| >40 years | 27 (26.2%) | 76 (73.8%) | |||||
| Relation to the child | Father | 16 (33.3%) | 32 (66.7%) | 10.797 | 1 | 0.001 * | |
| Mother | 14 (11.8%) | 105 (88.2%) | |||||
| Workplace | Not employed | 12 (11.2%) | 95 (88.8%) | 10.147 | 2 | 0.006 * | |
| Government | 15 (31.9%) | 32 (68.1%) | |||||
| Private | 5 (26.3%) | 14 (73.7%) | |||||
| Health insurance | No | 15 (12.2%) | 108 (87.8%) | 11.567 # | 2 | 0.003 * | |
| Private | 1 (16.7%) | 5 (83.3%) | |||||
| Governmental | 16 (36.4%) | 28 (63.6%) | |||||
| Older adults living in the same home | No | 18 (16.2%) | 93 (83.8%) | 1.069 | 1 | 0.301 | |
| Yes | 14 (22.6%) | 48 (77.4%) | |||||
| Previous COVID-19 infection | No | 17 (14.2%) | 103 (85.8%) | 2 | 0.05 | ||
| Not Sure | 3 (42.9%) | 4 (57.1%) | 6.006 | ||||
| Yes | 12 (26.1%) | 34 (73.9%) | |||||
| COVID-19 vaccine status | Does not want to take the vaccine | 1 (2.8%) | 35 (97.2%) | 12.448 # | 6 | 0.033 * | |
| Took the first dose and is awaiting the second | 6 (27.3%) | 16 (72.7%) | |||||
| Took the first dose but does not want to take the second dose | 1 (14.3%) | 6 (85.7%) | |||||
| Took the first and second doses and is awaiting the booster dose | 20 (25.3%) | 59 (74.7%) | |||||
| Parents’ characteristics | Took the first and second but does not want to take the booster dose | - | 4 (100%) | ||||
| Took the three doses | 4 (22.2%) | 14 (77.8%) | |||||
| Wants to take the vaccine, but it is not scheduled yet | - | 7 (100%) | |||||
| Chronic diseased parents | No | 21 (14.3%) | 126 (85.7%) | 11.507 | 1 | 0.001 * | |
| Yes | 11 (42.3%) | 15 (57.7%) | |||||
| Child age | Mean ± SD | 16.34 ± 1.4 | 11.90 ± 3.473 | 11.41 $ | 0.001 * | ||
| Child sex | Female | 22 (19.6%) | 90 (80.4%) | 0.277 | 1 | 0.599 | |
| Male | 10 (16.4%) | 51 (83.6%) | |||||
| Children’s characteristics | Child with a previous COVID-19 infection | No | 23 (14.5%) | 136 (85.5%) | 16.884 # | 2 | 0.0001 * |
| Not sure | 3 (60.0%) | 2 (40.0%) | |||||
| Yes | 6 (66.7%) | 3 (33.3%) | |||||
| Parents’ Attitudes about Childhood Vaccines (PACV) | Behavior | Median (IQR) | 0 (0–0) | 0 (0–0) | 0.83 $$ | 0.407 | |
| Safety and efficacy | Median (IQR) | 7 (6.25–7) | 7 (7–7) | 0.754 $$ | 0.451 | ||
| Attitude and trust | Median (IQR) | 1 (0.25–2) | 2 (1–3.5) | 2.145 $$ | 0.032 * | ||
| Total PACV Score ## | Median (IQR) | 26.67 (23.3–33.3) | 30 (26.67–33.33) | 2.424 $$ | 0.015 * | ||
| Variable | Total Effect and Direction | Direct Effect and Direction | Indirect Effect and Direction |
|---|---|---|---|
| Child age | −0.049 | −0.049 | 0 |
| Level illiterate | −0.018 | 0 | −0.018 |
| Level low | −0.014 | 0 | −0.014 |
| Family size | −0.053 | −0.053 | 0 |
| Income | −0.048 | 0 | −0.048 |
| Child sex | −0.004 | 0 | −0.004 |
| Safety and efficacy | 0.004 | 0 | 0.004 |
| Attitude trust | 0.030 | 0.030 | 0 |
| Parents’ Hesitancy about Vaccines | Accepting Vaccination Mean ± SD | Hesitant Mean ± SD | Wilks’ Lambda | Function | p. |
|---|---|---|---|---|---|
| Safety and efficacy | 6.0 ± 2.39 | 6.41 ± 2.01 | 0.98 | −0.036 | 0.092 |
| Attitude and trust | 1.56 ± 1.41 | 2.34 ± 1.88 | 0.96 | −0.317 | 0.028 |
| Child age | 16.34 ± 1.41 | 11.96 ± 3.47 | 0.78 | 0.904 | 0.000 |
| Family size | 5.50 ± 0.67 | 5.07 ± 0.87 | 0.96 | 0.259 | 0.009 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Elkhadry, S.W.; Salem, T.A.E.H.; Elshabrawy, A.; Goda, S.S.; Bahwashy, H.A.A.; Youssef, N.; Hussein, M.; Ghazy, R.M. COVID-19 Vaccine Hesitancy among Parents of Children with Chronic Liver Diseases. Vaccines 2022, 10, 2094. https://doi.org/10.3390/vaccines10122094
Elkhadry SW, Salem TAEH, Elshabrawy A, Goda SS, Bahwashy HAA, Youssef N, Hussein M, Ghazy RM. COVID-19 Vaccine Hesitancy among Parents of Children with Chronic Liver Diseases. Vaccines. 2022; 10(12):2094. https://doi.org/10.3390/vaccines10122094
Chicago/Turabian StyleElkhadry, Sally Waheed, Tahany Abd El Hameed Salem, Abdelhamid Elshabrawy, Shymaa Sami Goda, Howyda Ali Al Bahwashy, Naglaa Youssef, Mai Hussein, and Ramy Mohamed Ghazy. 2022. "COVID-19 Vaccine Hesitancy among Parents of Children with Chronic Liver Diseases" Vaccines 10, no. 12: 2094. https://doi.org/10.3390/vaccines10122094
APA StyleElkhadry, S. W., Salem, T. A. E. H., Elshabrawy, A., Goda, S. S., Bahwashy, H. A. A., Youssef, N., Hussein, M., & Ghazy, R. M. (2022). COVID-19 Vaccine Hesitancy among Parents of Children with Chronic Liver Diseases. Vaccines, 10(12), 2094. https://doi.org/10.3390/vaccines10122094