
Does Anybody Want an Injectable Rotavirus Vaccine, and Why? Understanding the Public Health Value Proposition of Next-Generation Rotavirus Vaccines

 , ,
, ,
Abstract
:1. Introduction
2. The Multiple Theoretical Advantages of Next-Generation Rotavirus Vaccines
3. Methods
4. Results
4.1. The Tangible Need to Prioritize among iNGRV Use Cases
4.2. Focus on Infant Vaccination, Rather Than Booster
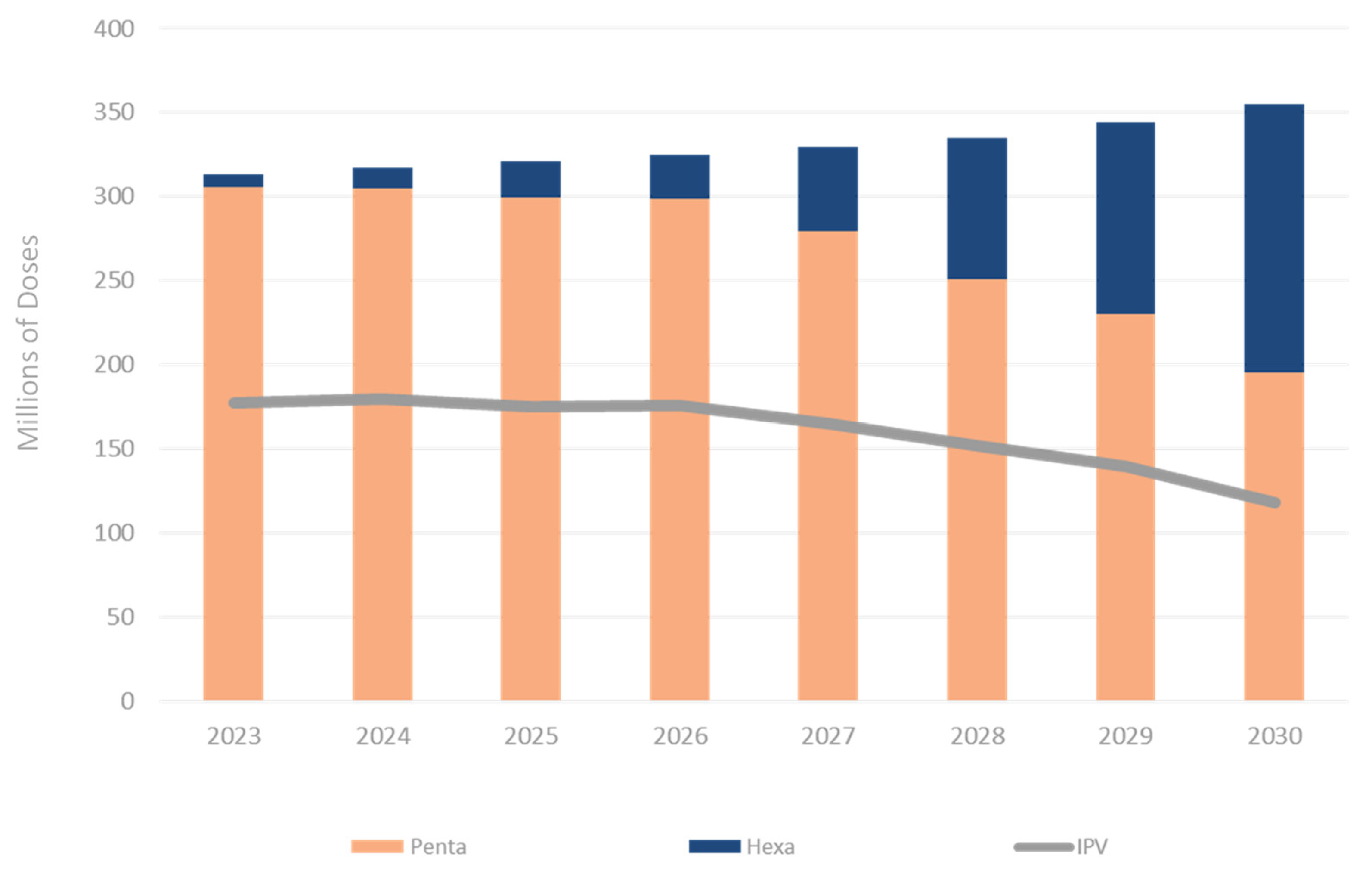
4.3. iNGRV Combination Vaccine Scenarios Should Focus on Potential Combinations with DTP-Hib-HepB and DTP-Hib-HepB-IPV, Not with IPV
4.4. Potential Impact and Cost-Effectiveness of Different Use Cases of iNGRV
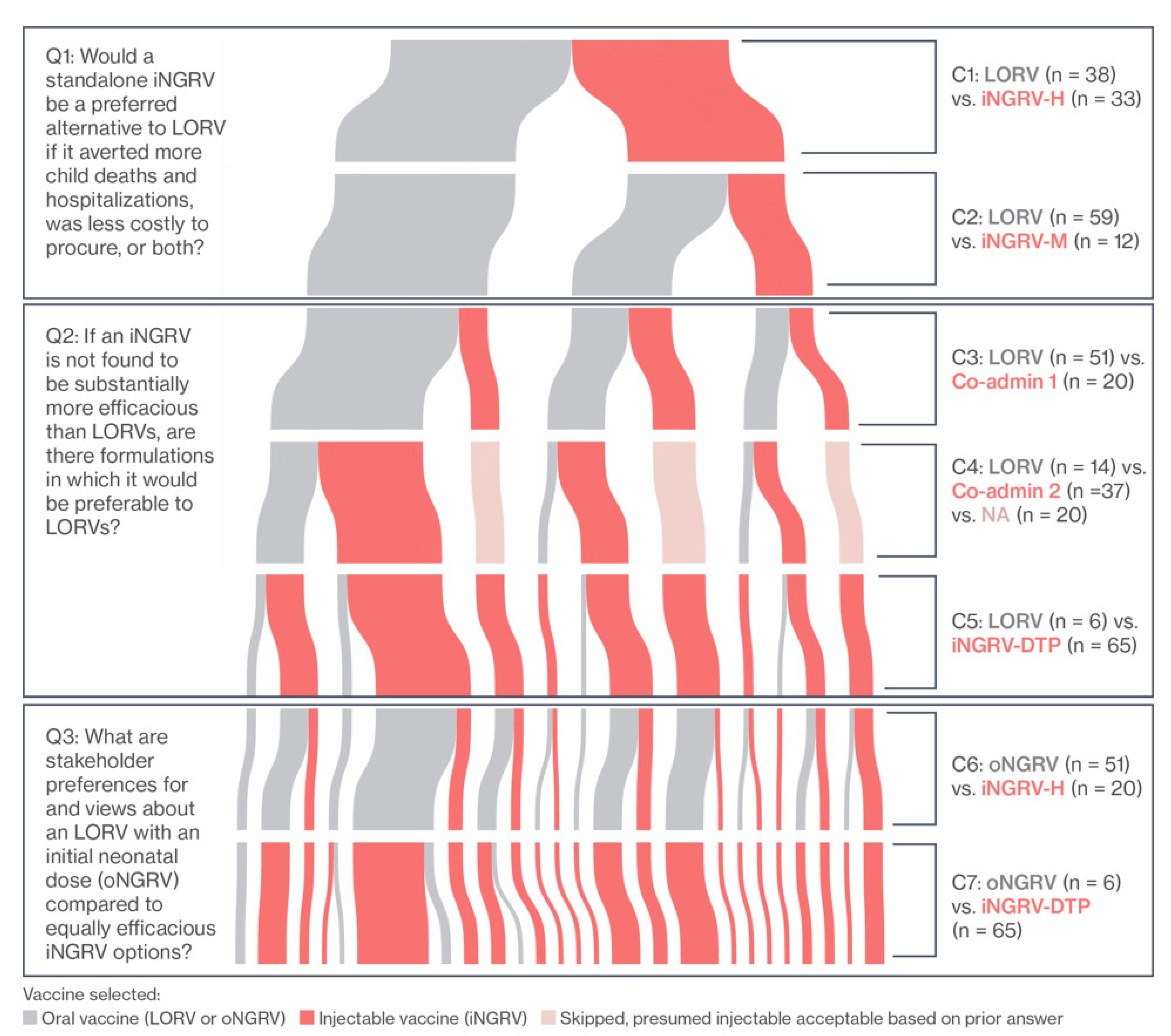
4.5. Product Preferences among Country Stakeholders in LMICs
4.6. High-Level Findings from National Stakeholder Interviews
4.7. High-Level Findings from Healthcare Provider Interviews
5. Projected Demand for iNGRVs
6. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kaslow, D.C.; Black, S.; Bloom, D.E.; Datla, M.; Salisbury, D.; Rappuoli, R. Vaccine candidates for poor nations are going to waste. Nature 2018, 564, 337–339. [Google Scholar] [CrossRef]
- Gessner, B.D.; Kaslow, D.; Louis, J.; Neuzil, K.; O’Brien, K.L.; Picot, V.; Pang, T.; Parashar, U.D.; Saadatian-Elahi, M.; Nelson, C.B. Estimating the full public health value of vaccination. Vaccine 2017, 35, 6255–6263. [Google Scholar] [CrossRef]
- Hutubessy, R.C.; Lauer, J.A.; Giersing, B.; Sim, S.Y.; Jit, M.; Kaslow, D.; Botwright, S. The Full Value of Vaccine Assessments (FVVA): A Framework to Assess and Communicate the Value of Vaccines for Investment and Introduction Decision Making. SSRN 2021. [Google Scholar] [CrossRef]
- Archer, R.A.; Kapoor, R.; Isaranuwatchai, W.; Teerawattananon, Y.; Giersing, B.; Botwright, S.; Luttjeboer, J.; Hutubessy, R.C.W. ‘It takes two to tango’: Bridging the gap between country need and vaccine product innovation. PLoS ONE 2020, 15, e0233950. [Google Scholar] [CrossRef]
- World Health Organization. WHO Full Public Health Value Proposition (FPHVP) for Vaccines (DRAFT template). Available online: https://www.who.int/immunization/sage/meetings/2018/april/3_WHO_FPHVPTableofContents_SAGE_Apr2018.pdf (accessed on 31 October 2021).
- GBD Diarrhoeal Diseases Collaborators. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of diarrhoea in 195 countries: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Infect. Dis. 2018, 18, 1211–1228. [Google Scholar] [CrossRef] [Green Version]
- Kotloff, K.L.; Nataro, J.P.; Blackwelder, W.C.; Nasrin, D.; Farag, T.H.; Panchalingam, S.; Wu, Y.; Sow, S.O.; Sur, D.; Breiman, R.F.; et al. Burden and aetiology of diarrhoeal disease in infants and young children in developing countries (the Global Enteric Multicenter Study, GEMS): A prospective, case-control study. Lancet 2013, 382, 209–222. [Google Scholar] [CrossRef]
- Cates, J.E.; Tate, J.E.; Parashar, U. Rotavirus vaccines: Progress and new developments. Expert Opin. Biol. Ther. 2021, 1–10. [Google Scholar] [CrossRef]
- Fix, A.; Kirkwood, C.D.; Steele, D.; Flores, J. Next-generation rotavirus vaccine developers meeting: Summary of a meeting sponsored by PATH and the Bill & Melinda Gates Foundation (19–20 June 2019, Geneva). Vaccine 2020, 38, 8247–8254. [Google Scholar] [CrossRef]
- Groome, M.J.; Fairlie, L.; Morrison, J.; Fix, A.; Koen, A.; Masenya, M.; Jose, L.; Madhi, S.A.; Page, N.; McNeal, M.; et al. Safety and immunogenicity of a parenteral trivalent P2-VP8 subunit rotavirus vaccine: A multisite, randomised, double-blind, placebo-controlled trial. Lancet Infect. Dis. 2020, 20, 851–863. [Google Scholar] [CrossRef]
- Bines, J. Investigating barriers to the protective efficacy provided by rotavirus vaccines in African infants. PLoS Med. 2021, 18, e1003721. [Google Scholar] [CrossRef]
- Lee, B. Update on rotavirus vaccine underperformance in low- to middle-income countries and next-generation vaccines. Hum. Vaccines Immunother. 2021, 17, 1787–1802. [Google Scholar] [CrossRef]
- Steele, A.; Victor, J.; Carey, M.; Tate, J.; Atherly, D.; Pecenka, C.; Diaz, Z.; Parashar, U.; Kirkwood, C. Experiences with rotavirus vaccines: Can we improve rotavirus vaccine impact in developing countries? Hum. Vaccines Immunother. 2019, 15, 1215–1227. [Google Scholar] [CrossRef] [Green Version]
- Bines, J.E.; At Thobari, J.; Satria, C.D.; Handley, A.; Watts, E.; Cowley, D.; Nirwati, H.; Ackland, J.; Standish, J.; Justice, F.; et al. Human Neonatal Rotavirus Vaccine (RV3-BB) to Target Rotavirus from Birth. N. Engl. J. Med. 2018, 378, 719–730. [Google Scholar] [CrossRef]
- Jiang, B.; Patel, M.; Glass, R. Polio endgame: Lessons for the global rotavirus vaccination program. Vaccine 2019, 37, 3040–3049. [Google Scholar] [CrossRef] [PubMed]
- Clark, A.; van Zandvoort, K.; Flasche, S.; Sanderson, C.; Bines, J.; Tate, J.; Parashar, U.; Jit, M. Efficacy of live oral rotavirus vaccines by duration of follow-up: A meta-regression of randomised controlled trials. Lancet Infect. Dis. 2019, 19, 17–727. [Google Scholar] [CrossRef] [Green Version]
- Jonesteller, C.; Burnett, E.; Yen, C.; Tate, J.; Parashar, U. Effectiveness of Rotavirus Vaccination: A Systematic Review of the First Decade of Global Postlicensure Data, 2006–2016. Clin. Infect. Dis. 2017, 65, 840–850. [Google Scholar] [CrossRef]
- National Institutes of Health. Mixed Schedule Study of Live Oral Rotavirus Vaccines and Trivalent P2-VP8 Subunit Rotavirus Vaccine. Available online: https://clinicaltrials.gov/ct2/show/NCT04344054 (accessed on 4 October 2021).
- Glass, R.I.; Tate, J.E.; Jiang, B.; Parashar, U. The Rotavirus Vaccine Story: From Discovery to the Eventual Control of Rotavirus Disease. J. Infect. Dis. 2021, 224, S331–S342. [Google Scholar] [CrossRef]
- Burnett, E.; Lopman, B.A.; Parashar, U.D. Potential for a booster dose of rotavirus vaccine to further reduce diarrhea mortality. Vaccine 2017, 35, 7198–7203. [Google Scholar] [CrossRef]
- Rogawski, E.T.; Platts-Mills, J.A.; Colgate, E.R.; Haque, R.; Zaman, K.; Petri, W.A.; Kirkpatrick, B.D. Quantifying the Impact of Natural Immunity on Rotavirus Vaccine Efficacy Estimates: A Clinical Trial in Dhaka, Bangladesh (PROVIDE) and a Simulation Study. J. Infect. Dis. 2018, 217, 861–868. [Google Scholar] [CrossRef] [Green Version]
- Lopman, B.A.; Pitzer, V.E. Waxing Understanding of Waning Immunity. J. Infect. Dis. 2018, 217, 851–853. [Google Scholar] [CrossRef]
- World Health Organization. Weekly Epidemiological Record—GPEI. Available online: https://polioeradication.org/library/ (accessed on 31 October 2021).
- Gavi. Combined Supply and Procurement Roadmap, Penta-IPV-Hexa-Roadmap-Public-Summary. Available online: https://www.gavi.org/our-alliance/market-shaping/supply-and-procurement-roadmaps (accessed on 31 October 2021).
- Linksbridge. The Global Vaccine Market: Overview of Asset (Version 5.3). Available online: https://4550bf57-cdn.agilitycms.cloud/help-guides/Introduction%20to%20GVMM.pdf (accessed on 31 October 2021).
- World Health Organization. International Clinical Trials Registry Platform: ICTRP Search Portal. Available online: https://www.who.int/clinical-trials-registry-platform/the-ictrp-search-portal (accessed on 15 October 2021).
- Debellut, F.; Pecenka, C.; Clark, A.; Hausdorff, W.P. Potential impact and cost-effectiveness of injectable next-generation rotavirus vaccines in 137 LMICs: A modelling study. Hum. Vacc. Imm. 2022, in press.
- National Institutes of Health. A Trial to Assess the Safety, Immunogenicity and Efficacy of a Trivalent Rotavirus P2-VP8 Subunit Vaccine in Prevention of Severe Rotavirus Gastroenteritis in Healthy Infants in Africa and India. Available online: https://clinicaltrials.gov/ct2/show/NCT04010448 (accessed on 4 October 2021).
- Clark, A.; Black, R.; Tate, J.; Roose, A.; Kotloff, K.; Lam, D.; Blackwelder, W.; Parashar, U.; Lanata, C.; Kang, G.; et al. Estimating global, regional and national rotavirus deaths in children aged <5 years: Current approaches, new analyses and proposed improvements. PLoS ONE 2017, 12, e0183392. [Google Scholar] [CrossRef]
- Price, J.; Mooney, J.; Bain, C.; Bawa, J.T.; Gurley, N.; Kumar, A.; Liyanage, G.; Mkisi, R.E.; Odero, C.; Seck, K.; et al. National Stakeholder Preferences for Next-Generation Rotavirus Vaccines: Results from a Six-Country Study. Vaccine 2021, 40, 370–379. [Google Scholar] [CrossRef]
- Mooney, J.; Price, J.; Bain, C.; Bawa, J.; Gurley, N.; Kumar, A.; Liyanage, G.; Mkisi, R.E.; Seck, K.; Simpson, E.; et al. Health Provider Perspectives on Delivering Next Generation Rotavirus Vaccines in Five LMICs. PLoS ONE, 2022; submitted. [Google Scholar]
- Rubinstein, R.; Kroese, D. Simulation and the Monte Carlo Method, 3rd ed.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2017. [Google Scholar]
- Dalberg Advisors. Validated inference of adoption likelihood—Oral Rotavirus Vaccine. Available online: https://www.vial-health.com (accessed on 31 October 2021).
- Pitzer, V.E.; Bennett, A.; Bar-Zeev, N.; Jere, K.C.; Lopman, B.A.; Lewnard, J.A.; Parashar, U.D.; Cunliffe, N.A. Evaluating strategies to improve rotavirus vaccine impact during the second year of life in Malawi. Sci. Transl. Med. 2019, 11, 505. [Google Scholar] [CrossRef]
- Kardani, K.; Bolhassani, A.; Shahbazi, S. Prime-boost vaccine strategy against viral infections: Mechanisms and benefits. Vaccine 2016, 34, 413–423. [Google Scholar] [CrossRef]
- Sim, S.Y.; Jit, M.; Constenla, D.; Peters, D.H.; Hutubessy, R.C.W. A Scoping Review of Investment Cases for Vaccines and Immunization Programs. Value in Health. J. Int. Soc. Pharm. Outcomes Res. 2019, 22, 942–952. [Google Scholar] [CrossRef]
- Donadel, M.; Paneroa, M.S.; Ametewee, L.; Shefer, A.M. National decision-making for the introduction of new vaccines: A systematic review, 2010–2020. Vaccine 2021, 39, 1897–1909. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Comparisons with National Stakeholders | Comparisons with Healthcare Providers | ||||||
|---|---|---|---|---|---|---|---|
| C1 | LORV | vs. | iNGRV-H | C1a | LORV | vs. | iNGRV |
| C2 | LORV | vs. | iNGRV-M | C2a | oNGRV | vs. | iNGRV |
| C3 | LORV | vs. | Co-admin 1 | C3a | LORV | vs. | oNGRV |
| C4 | LORV | vs. | Co-admin 2 | ||||
| C5 | LORV | vs. | iNGRV-DTP | ||||
| C6 | oNGRV | vs. | iNGRV-H | ||||
| C7 | oNGRV | vs. | iNGRV-DTP | ||||
| Primary Theoretical Advantage of iNGRV over LORVs | Clinical Endpoint Needed | Chemistry, Manufacturing, and Controls (CMC) Implications | Recommending Body/Market Implications |
|---|---|---|---|
| Higher vaccine efficacy in high-morbidity settings | Demonstrate NGRV’s vaccine efficacy (VE) superiority to LORV. | n/a | Strong selling point to WHO/Strategic Advisory Group of Experts (SAGE) and low-income, high-morbidity settings but perhaps not to lower morbidity middle income countries (MICs). |
| Lower Cost of Goods (COGs)/dose | Demonstrate VE non-inferiority to LORV. | Focus on technologies to minimize COGs. | If prices lower than LORV, an NGRV would be attractive to Gavi and LMICs supporting their own vaccine costs. Not clear if low-income countries currently supported by Gavi would see this as a sufficiently compelling reason to choose NGRV over LORVs, nor whether lower COGs would translate into prices sufficiently low enough to attract MICs that have not yet introduced rotavirus vaccine. |
| Co-administration with LORVs or as a boost to counteract reduced vaccine impact over time | No need to demonstrate VE after primary series but must show enhanced VE compared to LORV alone upon co-administration or boost. | n/a | COGs advantage over LORVs lost; unclear if preventing incremental late disease sufficiently impactful to affect global recommendations or national uptake. |
| Can be combined with DTP-containing vaccines or IPV | Demonstrate VE non-inferiority to LORV, plus immunological non-inferiority in the combination form and non-interference with other antigens. | Major investment needed; physicochemical compatibility efforts prioritized; need to reduce iNGRV dosage volume and potentially interfering excipients. | Delayed time to market compared to a standalone product, but if only one manufacturer is successful might allow it to dominate DTP-containing combination vaccine field. |
| No vaccine-induced intussusception | Demonstrate VE non-inferiority to LORV. (Impossible to demonstrate lack of heightened risk of intussusception pre-licensure.) | n/a | Unclear if vaccine-induced intussusception observed primarily in low-mortality countries is a barrier to uptake of LORVs in other settings. |
| Region | Linear Waning | Logarithmic Waning |
|---|---|---|
| Deaths occurring annually despite high oral rotavirus vaccine coverage, without a booster. | ||
| Africa | 62,466 | 62,382 |
| Southeast Asia | 28,507 | 27,838 |
| Deaths preventable by 12-month booster increasing vaccine efficacy by 50% | ||
| Africa | 2658 (4.3%) * | 4035 (6.5%) * |
| Southeast Asia | 2153 (7.6%) * | 3269 (11.7%) * |
| Study Site | LORV Efficacy Waning (% Decrease between Reported 1st and 2nd Year Vaccine Efficacies *) | How Much Higher Second Year Efficacy Should Be (Excludes from Efficacy Calculations Unvaccinated Children Likely Naturally Immunized by Mildly Symptomatic Rotavirus Infections) * | Percentage of “Waning” that Appears Artifactual ** |
|---|---|---|---|
| South Africa | 36.9% | 5.8% | 16% |
| Ghana | 35.1% | 10% | 28% |
| Bangladesh | 42.2% | 15.5% | 37% |
| Mali | 23.7% | 14.8% | 62% * |
| Malawi | 31.8% | 18% | 57% * |
| Average | 33.9% | 12.8% | 40% * |
| Vaccine(s) | Averted RVGE Cases | Averted RVGE Hospitalizations | Averted RVGE Deaths | Additional IS Deaths | Averted DALYs (Discounted) | Vaccine Program Costs | Averted Healthcare Costs | Net Cost | Cost-Effectiveness Ratio |
|---|---|---|---|---|---|---|---|---|---|
| iNGRV-DTP | 322,134,000 | 13,053,000 | 754,000 | 0 | 19,643,000 | 1,393,077,000 | 2,716,684,000 | −1,323,607,000 | Cost-saving |
| iNGRV-DTP-M | 256,731,000 | 10,424,000 | 573,000 | 0 | 14,991,000 | 1,393,077,000 | 2,332,835,000 | −939,759,000 | Cost-saving |
| iNGRV | 322,134,000 | 13,053,000 | 754,000 | 0 | 19,643,000 | 8,250,914,000 | 2,716,684,000 | 5,534,230,000 | 282 |
| iNGRV-M | 256,731,000 | 10,424,000 | 573,000 | 0 | 14,991,000 | 8,250,914,000 | 2,332,835,000 | 5,918,079,000 | 395 |
| oNGRV or oNGRV-H | 288,677,000 328,462,000 | 11,713,000 13,316,000 | 636,000 748,000 | 470 | 16,650,000 19,510,000 | 9,440,011,000 | 2,580,877,000 2,812,059,000 | 6,627,952,000 6,859,134,000 | 340 412 |
| ROTAVAC ROTASIIL | 251,184,000 | 10,198,000 | 556,000 | 1530 | 14,524,000 | 9,375,359,000 10,403,578,000 | 2,294,338,000 | 7,081,020,000 8,109,240,000 | 488 558 |
| iNGRV-DTP with oNGRV, ROTAVAC, or ROTASIIL | 322,134,000–328,462,000 | 13,053,000–13,316,000 | 748,000–754,000 | 470–1530 | 19,510,000–19,604,000 | 10,833,088,000– 11,796,655,000 | 2,714,128,000– 2,812,059,000 | 8,021,029,000–9,082,527,000 | 411–463 |
| iNGRV with oNGRV, ROTAVAC, or ROTASIIL | 322,134,000–328,462,000 | 13,053,000–13,316,000 | 748,000–754,000 | 470–1530 | 19,510,000–19,604,000 | 17,690,925,000– 18,654,492,000 | 2,714,128,000–2,812,059,000 | 14,878,866,000–15,940,364,000 | 763–813 |
| ROTARIX | 251,184,000 | 10,198,000 | 556,000 | 1530 | 14,524,000 | 24,075,203,000 | 2,294,338,000 | 21,780,865,000 | 1500 |
| iNGRV-DTP or iNGRV with ROTARIX | 322,134,000 | 13,053,000 | 754,000 | 1530 | 19,604,000 | 25,468,279,000 32,326,116,000 | 2,714,128,000 | 22,754,152,000 29,611,989,000 | 1161 1510 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hausdorff, W.P.; Price, J.; Debellut, F.; Mooney, J.; Torkelson, A.A.; Giorgadze, K.; Pecenka, C. Does Anybody Want an Injectable Rotavirus Vaccine, and Why? Understanding the Public Health Value Proposition of Next-Generation Rotavirus Vaccines. Vaccines 2022, 10, 149. https://doi.org/10.3390/vaccines10020149
Hausdorff WP, Price J, Debellut F, Mooney J, Torkelson AA, Giorgadze K, Pecenka C. Does Anybody Want an Injectable Rotavirus Vaccine, and Why? Understanding the Public Health Value Proposition of Next-Generation Rotavirus Vaccines. Vaccines. 2022; 10(2):149. https://doi.org/10.3390/vaccines10020149
Chicago/Turabian StyleHausdorff, William P., Jessica Price, Frédéric Debellut, Jessica Mooney, Andrew A. Torkelson, Khatuna Giorgadze, and Clint Pecenka. 2022. "Does Anybody Want an Injectable Rotavirus Vaccine, and Why? Understanding the Public Health Value Proposition of Next-Generation Rotavirus Vaccines" Vaccines 10, no. 2: 149. https://doi.org/10.3390/vaccines10020149
APA StyleHausdorff, W. P., Price, J., Debellut, F., Mooney, J., Torkelson, A. A., Giorgadze, K., & Pecenka, C. (2022). Does Anybody Want an Injectable Rotavirus Vaccine, and Why? Understanding the Public Health Value Proposition of Next-Generation Rotavirus Vaccines. Vaccines, 10(2), 149. https://doi.org/10.3390/vaccines10020149