
Evaluation of Immunogenicity and Safety of Vero Cell-Derived Inactivated COVID-19 Vaccine in Older Patients with Hypertension and Diabetes Mellitus

 ,
, 
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Participants
2.2. Study Vaccine
2.3. Immunogenicity and Safety Evaluation
2.4. Blood Pressure and Blood Glucose Measurement
2.5. Statistical Analysis
2.6. Patient and Public Involvement
3. Results
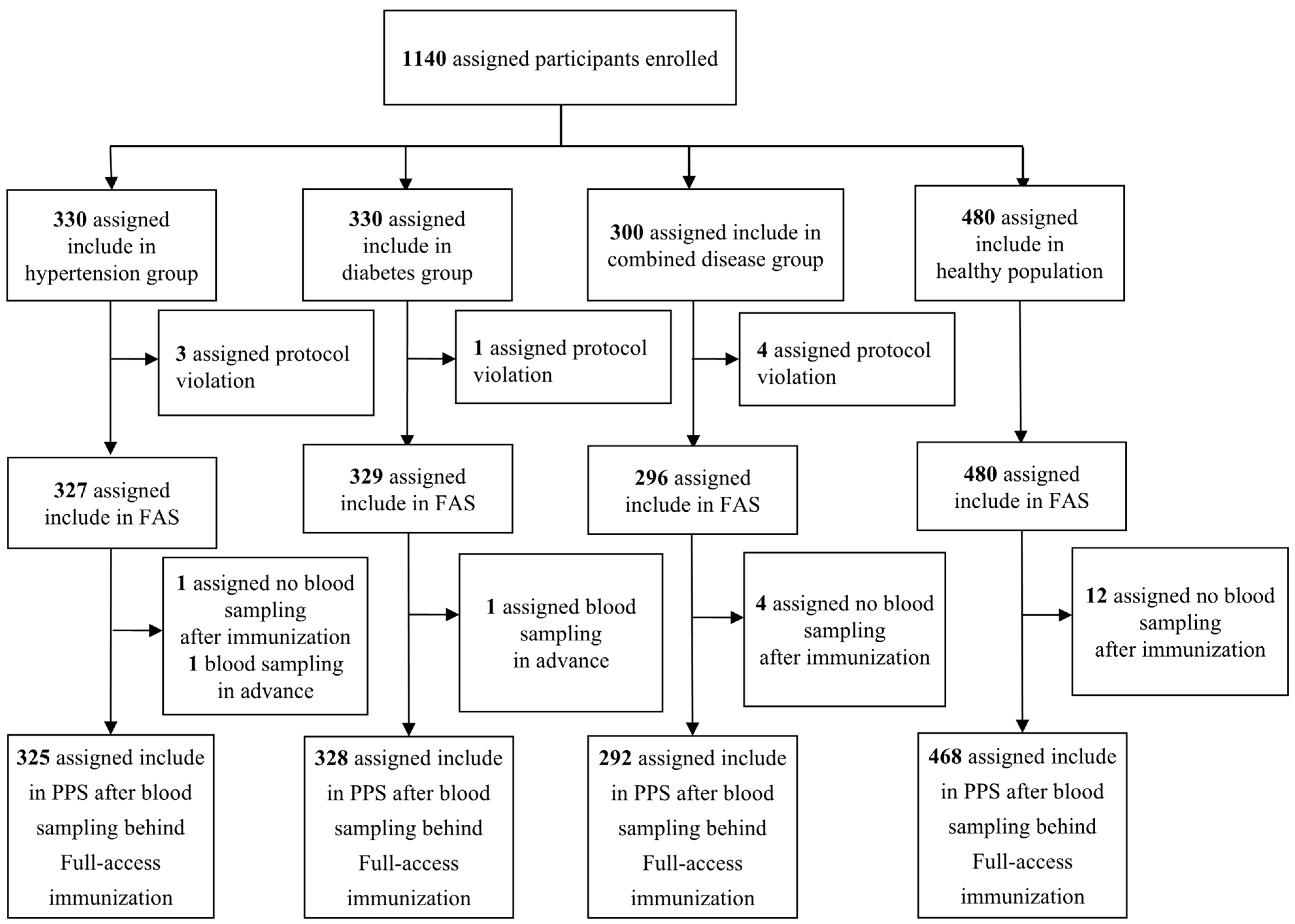
3.1. Study Population
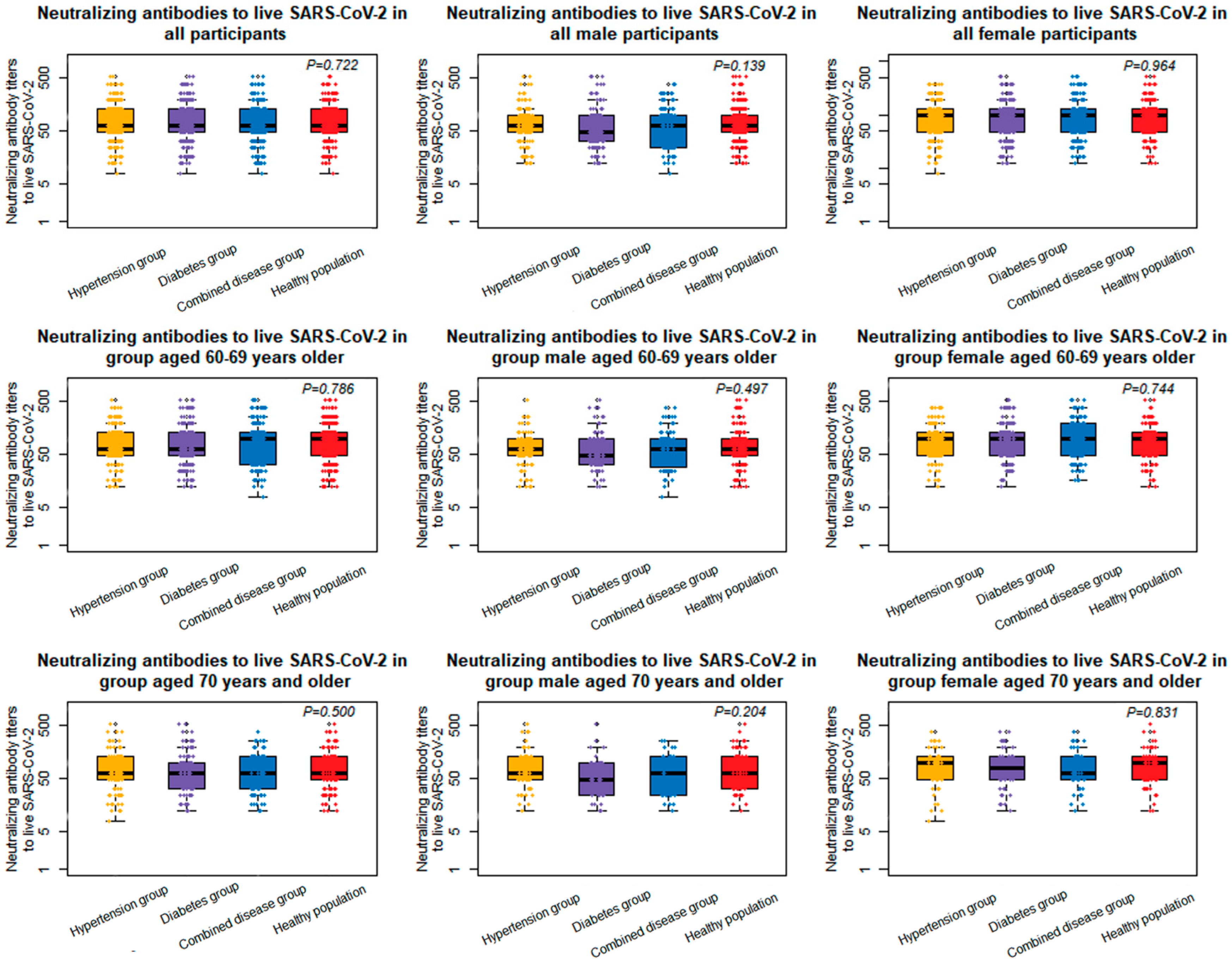
3.2. Immunogenicity of the Vaccine
3.3. Safety of the Vaccine
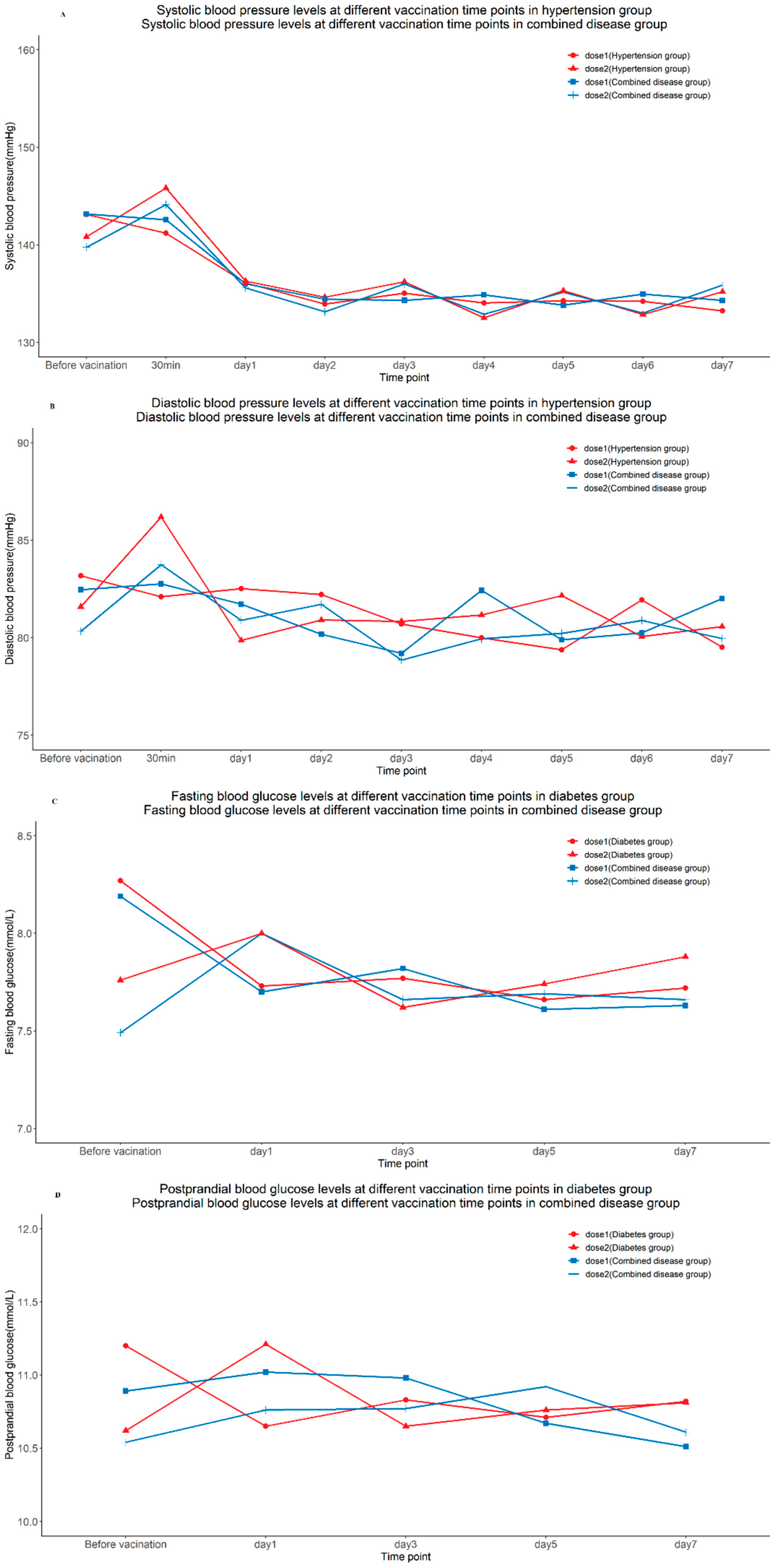
3.4. Analysis of Blood Pressure and Blood Glucose Levels
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Available online: https://covid19.who.int (accessed on 23 May 2022).
- Liu, W.; Tao, Z.W.; Wang, L.; Yuan, M.L.; Liu, K.; Zhou, L.; Wei, S.; Deng, Y.; Liu, J.; Liu, H.G.; et al. Analysis of factors associated with disease outcomes in hospitalized patients with 2019 novel coronavirus disease. Chin. Med. J. 2020, 133, 1032–1038. [Google Scholar] [CrossRef] [PubMed]
- Gardner, W.; States, D.; Bagley, N. The Coronavirus and the Risks to the Elderly in Long-Term Care. J. Aging Soc. Policy 2020, 32, 310–315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rabinowich, L.; Grupper, A.; Baruch, R.; Ben-Yehoyada, M.; Halperin, T.; Turner, D.; Katchman, E.; Levi, S.; Houri, I.; Lubezky, N.; et al. Low immunogenicity to SARS-CoV-2 vaccination among liver transplant recipients. J. Hepatol. 2021, 75, 435–438. [Google Scholar] [CrossRef] [PubMed]
- Sanders, J.S.F.; Bemelman, F.J.; Messchendorp, A.L.; Baan, C.C.; van Baarle, D.; van Binnendijk, R.; Diavatopoulos, D.A.; Frölke, S.C.; Geers, D.; GeurtsvanKessel, C.H.; et al. The RECOVAC Immune-response Study: The Immunogenicity, Tolerability, and Safety of COVID-19 Vaccination in Patients with Chronic Kidney Disease, on Dialysis, or Living with a Kidney Transplant. Transplantation 2021, 106, 821–834. [Google Scholar] [CrossRef]
- Wang, J.; Hou, Z.; Liu, J.; Gu, Y.; Wu, Y.; Chen, Z.; Ji, J.; Diao, S.; Qiu, Y.; Zou, S.; et al. Safety and immunogenicity of COVID-19 vaccination in patients with non-alcoholic fatty liver disease (CHESS2101): A multicenter study. J. Hepatol. 2021, 75, 439–441. [Google Scholar] [CrossRef]
- Shem-Tov, N.; Yerushalmi, R.; Danylesko, I.; Litachevsky, V.; Levy, I.; Olmer, L.; Lusitg, Y.; Avigdor, A.; Nagler, A.; Shimoni, A.; et al. Immunogenicity and safety of the BNT162b2 mRNA COVID-19 vaccine in haematopoietic stem cell transplantation recipients. Br. J. Haematol. 2021, 196, 884–891. [Google Scholar] [CrossRef]
- Ostchega, Y.; Fryar, C.D.; Nwankwo, T.; Nguyen, D.T. Hypertension Prevalence among Adults Aged 18 and over: United States, 2017–2018. NCHS Data Brief. 2020, 364, 1–8. [Google Scholar]
- National Diabetes Statistics Report 2020. Available online: https://www.cdc.gov/diabetes/pdfs/data/statistics/national-diabetes-statistics-report.pdf (accessed on 23 December 2021).
- Lu, J.; Lu, Y.; Wang, X.; Li, X.; Linderman, G.C.; Wu, C.; Cheng, X.; Mu, L.; Zhang, H.; Liu, J.; et al. Prevalence, awareness, treatment, and control of hypertension in China: Data from 1·7 million adults in a population-based screening study (China PEACE Million Persons Project). Lancet 2017, 390, 2549–2558. [Google Scholar] [CrossRef]
- Chinese Diabetes Society. Guideline for the prevention and treatment of type 2 diabetes mellitus in China (2020 edition). Chin. J. Diabetes Mellit. 2021, 13, 315–409. [Google Scholar]
- Yu, Q.; Lin, S.; Wu, J. Hypertension Prevalence Rates among Urban and Rural Older Adults of China, 1991–2015: A Standardization and Decomposition Analysis. Front. Public Health 2021, 9, 713730. [Google Scholar] [CrossRef]
- Zhao, C.; Wong, L.; Zhu, Q.; Yang, H. Prevalence and correlates of chronic diseases in an elderly population: A community-based survey in Haikou. PLoS ONE 2018, 13, e0199006. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xia, S.; Zhang, Y.; Wang, Y.; Wang, H.; Yang, Y.; Gao, G.F.; Tan, W.; Wu, G.; Xu, M.; Lou, Z.; et al. Safety and immunogenicity of an inactivated SARS-CoV-2 vaccine, BBIBP-CorV: A randomised, double-blind, placebo-controlled, phase 1/2 trial. Lancet Infect. Dis. 2021, 21, 39–51. [Google Scholar] [CrossRef]
- Wu, Z.; Hu, Y.; Xu, M.; Chen, Z.; Yang, W.; Jiang, Z.; Li, M.; Jin, H.; Cui, G.; Chen, P.; et al. Safety, tolerability, and immunogenicity of an inactivated SARS-CoV-2 vaccine (CoronaVac) in healthy adults aged 60 years and older: A randomised, double-blind, placebo-controlled, phase 1/2 clinical trial. Lancet Infect. Dis. 2021, 21, 803–812. [Google Scholar] [CrossRef]
- Walsh, E.E.; Frenck, R.W., Jr.; Falsey, A.R.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Neuzil, K.; Mulligan, M.J.; Bailey, R.; et al. Safety and Immunogenicity of Two RNA-Based Covid-19 Vaccine Candidates. N. Engl. J. Med. 2020, 383, 2439–2450. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Yang, J.; Wang, L.; Wu, Q.; Wu, Z.; Zheng, W.; Wang, L.; Lu, W.; Deng, X.; Peng, C.; et al. A booster dose is immunogenic and will be needed for older adults who have completed two doses vaccination with CoronaVac: A randomised, double-blind, placebo-controlled, phase 1/2 clinical trial. MedRxiv 2021, 8, 21261544. [Google Scholar]
- Bubar, K.M.; Reinholt, K.; Kissler, S.M.; Lipsitch, M.; Cobey, S.; Grad, Y.H.; Larremore, D.B. Model-informed COVID-19 vaccine prioritization strategies by age and serostatus. Science 2021, 371, 916–921. [Google Scholar] [CrossRef]
- He, Q.; Mao, Q.; Zhang, J.; Bian, L.; Gao, F.; Wang, J.; Xu, M.; Liang, Z. COVID-19 Vaccines: Current Understanding on Immunogenicity, Safety, and Further Considerations. Front. Immunol. 2021, 12, 669339. [Google Scholar] [CrossRef]
- Team CC-R. Severe Outcomes Among Patients with Coronavirus Disease 2019 (COVID-19)—United States, 12 February–16 March 2020. Morb. Mortal. Wkly. Rep. 2020, 69, 343–346. [Google Scholar] [CrossRef] [PubMed]
- Chakraborty, C.; Sharma, A.R.; Bhattacharya, M.; Agoramoorthy, G.; Lee, S.S. Asian-Origin Approved COVID-19 Vaccines and Current Status of COVID-19 Vaccination Program in Asia: A Critical Analysis. Vaccines 2021, 9, 600. [Google Scholar] [CrossRef]
- Zeng, G.; Wu, Q.; Pan, H.; Li, M.; Yang, J.; Wang, L.; Wu, Z.; Jiang, D.; Deng, X.; Chu, K.; et al. Immunogenicity and safety of a third dose of CoronaVac, and immune persistence of a two-dose schedule, in healthy adults: Interim results from two single-centre, double-blind, randomised, placebo-controlled phase 2 clinical trials. Lancet Infect. Dis. 2021, 22, 483–495. [Google Scholar] [CrossRef]
- Mbaeyi, S.; Oliver, S.E.; Collins, J.P.; Godfrey, M.; Goswami, N.D.; Hadler, S.C.; Jones, J.; Moline, H.; Moulia, D.; Reddy, S.; et al. The Advisory Committee on Immunization Practices′ Interim Recommendations for Additional Primary and Booster Doses of COVID-19 Vaccines—United States, 2021. Morb. Mortal. Wkly. Rep. 2021, 70, 1545–1552. [Google Scholar] [CrossRef] [PubMed]
- WHO. Interim Recommendations for Use of the Inactivated COVID-19 Vaccine, CoronaVac, Developed by Sinovac. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-vaccines-SAGE_recommendation-Sinovac-CoronaVac-2021.1 (accessed on 23 December 2021).
- WHO. Interim Recommendations for Use of the Inactivated COVID-19 Vaccine BIBP Developed by China National Biotec Group (CNBG), Sinopharm. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-vaccines-SAGE-recommendation-BIBP (accessed on 23 December 2021).
- Al Kaabi, N.; Zhang, Y.; Xia, S.; Yang, Y.; Al Qahtani, M.M.; Abdulrazzaq, N.; Al Nusair, M.; Hassany, M.; Jawad, J.S.; Abdalla, J.; et al. Effect of 2 Inactivated SARS-CoV-2 Vaccines on Symptomatic COVID-19 Infection in Adults: A Randomized Clinical Trial. JAMA 2021, 326, 35–45. [Google Scholar] [CrossRef] [PubMed]
- See, I.; Su, J.R.; Lale, A.; Woo, E.J.; Guh, A.Y.; Shimabukuro, T.T.; Streiff, M.B.; Rao, A.K.; Wheeler, A.P.; Beavers, S.F.; et al. US Case Reports of Cerebral Venous Sinus Thrombosis with Thrombocytopenia after Ad26.COV2.S Vaccination, 2 March to 21 April 2021. JAMA 2021, 325, 2448–2456. [Google Scholar] [CrossRef]
- Van Kammen, M.S.; De Sousa, D.A.; Poli, S.; Cordonnier, C.; Heldner, M.R.; Van De Munckhof, A.; Krzywicka, K.; Van Haaps, T. Characteristics and Outcomes of Patients with Cerebral Venous Sinus Thrombosis in SARS-CoV-2 Vaccine-Induced Immune Thrombotic Thrombocytopenia. JAMA Neurol. 2021, 78, 1314–1323. [Google Scholar] [CrossRef] [PubMed]
- Finsterer, J. Neurological side effects of SARS-CoV-2 vaccinations. Acta Neurol. Scand. 2022, 145, 5–9. [Google Scholar] [CrossRef] [PubMed]
- Abu-Rumeileh, S.; Abdelhak, A.; Foschi, M.; Tumani, H.; Otto, M. Guillain-Barre syndrome spectrum associated with COVID-19: An up-to-date systematic review of 73 cases. J. Neurol. 2021, 268, 1133–1170. [Google Scholar] [CrossRef]
- Wan, E.Y.F.; Chui, C.S.L.; Lai, F.T.T.; Chan, E.W.Y.; Li, X.; Yan, V.K.C.; Gao, L.; Yu, Q.; Lam, I.C.H.; Chun, R.K.C.; et al. Bell’s palsy following vaccination with mRNA (BNT162b2) and inactivated (CoronaVac) SARS-CoV-2 vaccines: A case series and nested case-control study. Lancet Infect. Dis. 2022, 22, 64–72. [Google Scholar] [CrossRef]
- Shibli, R.; Barnett, O.; Abu-Full, Z.; Gronich, N.; Najjar-Debbiny, R.; Doweck, I.; Rennert, G.; Saliba, W. Association between vaccination with the BNT162b2 mRNA COVID-19 vaccine and Bell′s palsy: A population-based study. Lancet Reg. Health Eur. 2021, 11, 100236. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Hypertension Group | Diabetes Group | Combined Disease Group | Healthy Population | p |
|---|---|---|---|---|---|
| Age | 0.279 * | ||||
| Mean ± SD | 68.79 ± 5.34 | 68.02 ± 4.62 | 68.33 ± 5.42 | 68.3 ± 5.09 | |
| Median | 68.18 | 67.42 | 67.55 | 67.4 | |
| Min, Max | 60.01, 96.46 | 60.31, 83.36 | 60.07, 96.4 | 60.11, 87.31 | |
| Gender | 0.001 ** | ||||
| Male | 157 (48.31%) | 137 (41.77%) | 118 (40.41%) | 249 (53.21%) | |
| Female | 168 (51.69%) | 191 (58.23%) | 174 (59.59%) | 219 (46.79%) |
| Hypertension Group (327 Assigned) | Diabetes Group (329 Assigned) | Combined Disease Group (296 Assigned) | Healthy Population (480 Assigned) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Adverse Events | Case Times | No. of Cases | Incidence Rate | Case Times | No. of Cases | Incidence Rate | Case Times | No. of Cases | Incidence Rate | Case Times | No. of Cases | Incidence Rate | Statistical Method | Statistic | p |
| Total | 59 | 39 | 11.93 | 92 | 47 | 14.29 | 80 | 37 | 12.50 | 80 | 45 | 9.38 | Chi-Square Test | 4.828 | 0.1849 |
| Solicited event | 43 | 35 | 10.70 | 76 | 43 | 13.07 | 62 | 30 | 10.14 | 64 | 37 | 7.71 | Chi-Square Test | 6.336 | 0.0964 |
| Local adverse events | 13 | 13 | 3.98 | 21 | 18 | 5.47 | 15 | 12 | 4.05 | 24 | 20 | 4.17 | Chi-Square Test | 1.184 | 0.7569 |
| Soreness | 11 | 11 | 3.36 | 15 | 13 | 3.95 | 9 | 8 | 2.70 | 23 | 19 | 3.96 | Chi-Square Test | 1.038 | 0.7919 |
| Swelling | 0 | 0 | 0.00 | 5 | 5 | 1.52 | 3 | 2 | 0.68 | 0 | 0 | 0.00 | Fisher’s Exact Test | - | 0.0044 |
| Pruritus | 1 | 1 | 0.31 | 1 | 1 | 0.30 | 2 | 2 | 0.68 | 1 | 1 | 0.21 | Fisher’s Exact Test | - | 0.8262 |
| Rash | 1 | 1 | 0.31 | 0 | 0 | 0.00 | 0 | 0 | 0.00 | 0 | 0 | 0.00 | Fisher’s Exact Test | - | 0.4351 |
| Hardness | 0 | 0 | 0.00 | 0 | 0 | 0.00 | 1 | 1 | 0.34 | 0 | 0 | 0.00 | Fisher’s Exact Test | - | 0.2067 |
| Systemic adverse events | 30 | 24 | 7.34 | 55 | 31 | 9.42 | 47 | 21 | 7.09 | 40 | 21 | 4.38 | Chi-Square Test | 8.243 | 0.0413 |
| Dizziness | 14 | 12 | 3.67 | 23 | 17 | 5.17 | 8 | 7 | 2.36 | 13 | 10 | 2.08 | Chi-Square Test | 6.915 | 0.0746 |
| Fatigue/lethargy | 7 | 7 | 2.14 | 9 | 9 | 2.74 | 10 | 8 | 2.70 | 8 | 8 | 1.67 | Chi-Square Test | 1.397 | 0.7063 |
| Headache | 1 | 1 | 0.31 | 7 | 7 | 2.13 | 7 | 6 | 2.03 | 3 | 3 | 0.63 | Fisher’s Exact Test | - | 0.0474 |
| Chest tightness | 1 | 1 | 0.31 | 5 | 4 | 1.22 | 4 | 4 | 1.35 | 1 | 1 | 0.21 | Fisher’s Exact Test | - | 0.1187 |
| Nausea | 1 | 1 | 0.31 | 3 | 3 | 0.91 | 4 | 4 | 1.35 | 1 | 1 | 0.21 | Fisher’s Exact Test | - | 0.1607 |
| Non-injection site pruritus | 1 | 1 | 0.31 | 1 | 1 | 0.30 | 2 | 2 | 0.68 | 3 | 2 | 0.42 | Fisher’s Exact Test | - | 0.8498 |
| Muscle pain | 2 | 2 | 0.61 | 1 | 1 | 0.30 | 0 | 0 | 0.00 | 4 | 3 | 0.63 | Fisher’s Exact Test | - | 0.6524 |
| Cough | 0 | 0 | 0.00 | 2 | 2 | 0.61 | 3 | 3 | 1.01 | 2 | 2 | 0.42 | Fisher’s Exact Test | - | 0.2892 |
| Arthralgia | 1 | 1 | 0.31 | 0 | 0 | 0.00 | 3 | 2 | 0.68 | 1 | 1 | 0.21 | Fisher’s Exact Test | - | 0.4899 |
| Fever | 1 | 1 | 0.31 | 0 | 0 | 0.00 | 3 | 3 | 1.01 | 0 | 0 | 0.00 | Fisher’s Exact Test | - | 0.0152 |
| Diarrhoea | 0 | 0 | 0.00 | 1 | 1 | 0.30 | 2 | 2 | 0.68 | 0 | 0 | 0.00 | Fisher’s Exact Test | - | 0.0913 |
| Anorexia | 0 | 0 | 0.00 | 1 | 1 | 0.30 | 0 | 0 | 0.00 | 2 | 2 | 0.42 | Fisher’s Exact Test | - | 0.7034 |
| Constipation | 0 | 0 | 0.00 | 0 | 0 | 0.00 | 1 | 1 | 0.34 | 1 | 1 | 0.21 | Fisher’s Exact Test | - | 0.6927 |
| Vomiting | 1 | 1 | 0.31 | 0 | 0 | 0.00 | 0 | 0 | 0.00 | 1 | 1 | 0.21 | Fisher’s Exact Test | - | 0.8459 |
| Skin mucosal abnormalities | 0 | 0 | 0.00 | 2 | 2 | 0.61 | 0 | 0 | 0.00 | 0 | 0 | 0.00 | Fisher’s Exact Test | - | 0.1473 |
| Hypertension Group (327 Assigned) | Diabetes Group (329 Assigned) | Combined Disease Group (296 Assigned) | Healthy Population (480 Assigned) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Adverse Events | Level 1 | Level 2 | Level 3 | Level 1 | Level 2 | Level 3 | Level 1 | Level 2 | Level 3 | Level 1 | Level 2 | Level 3 | KW_p |
| Total | 45 (13.76) | 9 (2.75) | 6 (1.83) | 46 (13.98) | 18 (5.47) | 4 (1.22) | 31 (10.47) | 16 (5.41) | 6 (2.03) | 53 (11.04) | 23 (4.79) | 5 (1.04) | 0.6145 |
| Solicitation event | 36 (11.01) | 2 (0.61) | 1 (0.31) | 38 (11.55) | 8 (2.43) | 1 (0.30) | 22 (7.43) | 7 (2.36) | 3 (1.01) | 37 (7.71) | 4 (0.83) | 0 (0.00) | 0.0728 |
| Local adverse events | 13 (3.98) | 0 (0.00) | 0 (0.00) | 18(5.47) | 1 (0.30) | 0 (0.00) | 11 (3.72) | 2 (0.68) | 0 (0.00) | 20 (4.17) | 0 (0.00) | 0 (0.00) | 0.6638 |
| Soreness | 11 (3.36) | 0 (0.00) | 0 (0.00) | 13(3.95) | 0 (0.00) | 0 (0.00) | 7 (2.36) | 1 (0.34) | 0 (0.00) | 19 (3.96) | 0 (0.00) | 0 (0.00) | 0.7968 |
| Swelling | 0 (0.00) | 0 (0.00) | 0 (0.00) | 4(1.22) | 1 (0.30) | 0 (0.00) | 1 (0.34) | 1 (0.34) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0.0100 |
| Pruritus | 1 (0.31) | 0 (0.00) | 0 (0.00) | 1(0.30) | 0 (0.00) | 0 (0.00) | 2 (0.68) | 0 (0.00) | 0 (0.00) | 1 (0.21) | 0 (0.00) | 0 (0.00) | 0.7490 |
| Rash | 1 (0.31) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0.3368 |
| Hardness | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 1 (0.34) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0.2795 |
| Systemic adverse events | 28 (8.56) | 4 (1.22) | 1 (0.31) | 41 (12.46) | 10 (3.04) | 3 (0.91) | 34 (11.49) | 6 (2.03) | 8 (2.70) | 35 (7.29) | 5 (1.04) | 0 (0.00) | 0.0003 |
| Dizziness | 12 (3.67) | 1 (0.31) | 0 (0.00) | 17 (5.17) | 2 (0.61) | 0 (0.00) | 6 (2.03) | 1 (0.34) | 0 (0.00) | 12 (2.50) | 0 (0.00) | 0 (0.00) | 0.0528 |
| Fatigue/lethargy | 7 (2.14) | 0 (0.00) | 0 (0.00) | 7 (2.13) | 1 (0.30) | 1 (0.30) | 5 (1.69) | 1 (0.34) | 2 (0.68) | 8 (1.67) | 1 (0.21) | 0 (0.00) | 0.8160 |
| Headache | 3 (0.92) | 0 (0.00) | 0 (0.00) | 4 (1.22) | 2 (0.61) | 1 (0.30) | 6 (2.03) | 0 (0.00) | 1 (0.34) | 3 (0.63) | 0 (0.00) | 0 (0.00) | 0.1146 |
| Cough | 1 (0.31) | 1 (0.31) | 0 (0.00) | 1 (0.30) | 1 (0.30) | 0 (0.00) | 3 (1.01) | 1 (0.34) | 1 (0.34) | 1 (0.21) | 1 (0.21) | 0 (0.00) | 0.2323 |
| Nausea | 0 (0.00) | 1 (0.31) | 0 (0.00) | 3 (0.91) | 0 (0.00) | 1 (0.30) | 4 (1.35) | 0 (0.00) | 0 (0.00) | 1 (0.21) | 0 (0.00) | 0 (0.00) | 0.1408 |
| Chest tightness, | 1 (0.31) | 0 (.00) | 0 (0.00) | 4 (1.22) | 0 (0.00) | 0 (0.00) | 4 (1.35) | 0 (0.00) | 0 (0.00) | 1 (0.21) | 0 (0.00) | 0 (0.00) | 0.1401 |
| Muscle pain | 1 (0.31) | 0 (0.00) | 1 (0.31) | 2 (0.61) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 4 (0.83) | 0 (0.00) | 0 (0.00) | 0.5046 |
| Non-injection site pruritus | 1 (0.31) | 0 (0.00) | 0 (0.00) | 1 (0.30) | 0 (0.00) | 0 (0.00) | 2 (0.68) | 1 (0.34) | 0 (0.00) | 1 (0.21) | 1 (0.21) | 0 (0.00) | 0.5350 |
| Arthralgia | 0 (0.00) | 1 (0.31) | 0 (0.00) | 0 (0.00) | 1 (0.30) | 0 (0.00) | 2 (0.68) | 1 (0.34) | 0 (0.00) | 1 (0.21) | 1 (0.21) | 0 (0.00) | 0.5377 |
| Fever | 1 (0.31) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 1 (0.34) | 0 (0.00) | 2 (0.68) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0.0459 |
| Diarrhea | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 1 (0.30) | 0 (0.00) | 0 (0.00) | 1 (0.34) | 2 (0.68) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0.0461 |
| Skin mucosal abnormalities | 0 (0.00) | 0 (0.00) | 0 (0.00) | 2 (0.61) | 1 (0.30) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0.0180 |
| Anorexia | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 1 (0.30) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 2 (0.42) | 0 (0.00) | 0 (0.00) | 0.4880 |
| Constipation | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 1 (0.34) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 1 (0.21) | 0 (0.00) | 0.5912 |
| Vomiting | 1 (0.31) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 1 (0.21) | 0 (0.00) | 0 (0.00) | 0.6408 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, Y.; Chen, H.; Lv, J.; Huang, T.; Zhang, R.; Zhang, D.; Luo, L.; Wei, S.; Liu, X.; Zhang, S.; et al. Evaluation of Immunogenicity and Safety of Vero Cell-Derived Inactivated COVID-19 Vaccine in Older Patients with Hypertension and Diabetes Mellitus. Vaccines 2022, 10, 1020. https://doi.org/10.3390/vaccines10071020
Zhang Y, Chen H, Lv J, Huang T, Zhang R, Zhang D, Luo L, Wei S, Liu X, Zhang S, et al. Evaluation of Immunogenicity and Safety of Vero Cell-Derived Inactivated COVID-19 Vaccine in Older Patients with Hypertension and Diabetes Mellitus. Vaccines. 2022; 10(7):1020. https://doi.org/10.3390/vaccines10071020
Chicago/Turabian StyleZhang, Yuntao, Haiping Chen, Jun Lv, Tao Huang, Ruizhi Zhang, Dongjuan Zhang, Linyun Luo, Sheng Wei, Xiaoqin Liu, Shangxiao Zhang, and et al. 2022. "Evaluation of Immunogenicity and Safety of Vero Cell-Derived Inactivated COVID-19 Vaccine in Older Patients with Hypertension and Diabetes Mellitus" Vaccines 10, no. 7: 1020. https://doi.org/10.3390/vaccines10071020
APA StyleZhang, Y., Chen, H., Lv, J., Huang, T., Zhang, R., Zhang, D., Luo, L., Wei, S., Liu, X., Zhang, S., Mu, Q., Huang, R., Huang, J., Xiao, Y., Yang, Y., Han, Y., Gong, H., Guan, Q., Xie, F., ... Yang, X. (2022). Evaluation of Immunogenicity and Safety of Vero Cell-Derived Inactivated COVID-19 Vaccine in Older Patients with Hypertension and Diabetes Mellitus. Vaccines, 10(7), 1020. https://doi.org/10.3390/vaccines10071020