
A Study of Varicella Seroprevalence in a Pediatric and Adolescent Population in Florence (Italy). Natural Infection and Vaccination-Acquired Immunization

 ,
,  ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subject Enrolment and Sera Collection
2.2. Anamnestic and Vaccination Status
2.3. Serological Analysis
- Anti-varicella/IgG negative ΔA < 0.100 (cut-off);
- Anti-varicella/IgG positive ΔA > 0.200;
- Anti-varicella/IgG equivocal 0.100 ≤ ΔA ≤ 0.200.
2.4. Statistical Analysis
3. Data Analysis
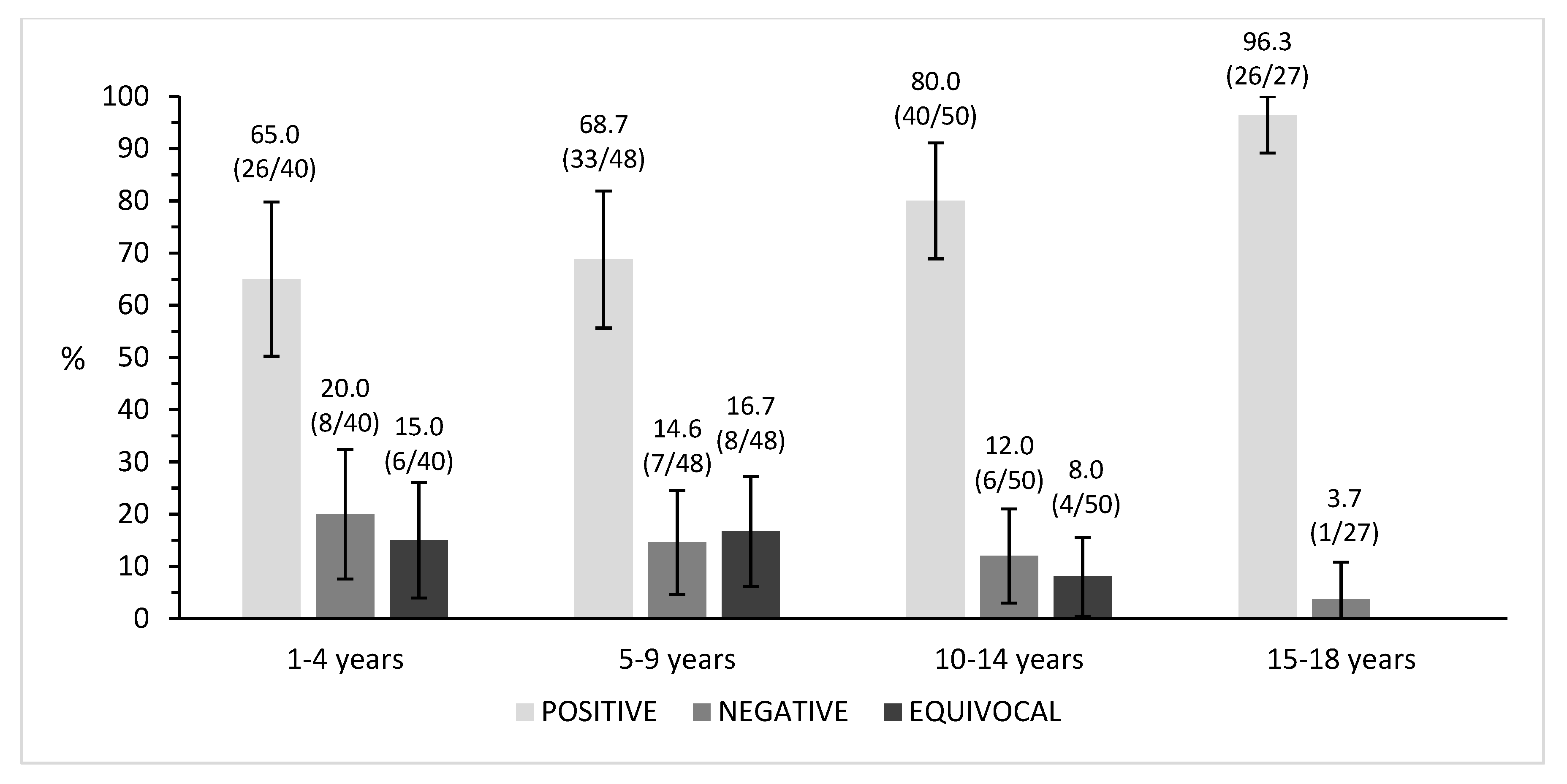
3.1. Varicella Seroprevalence Analysis
3.2. Varicella Disease Notification and Subjects’ Anamnestic Recall of the Disease
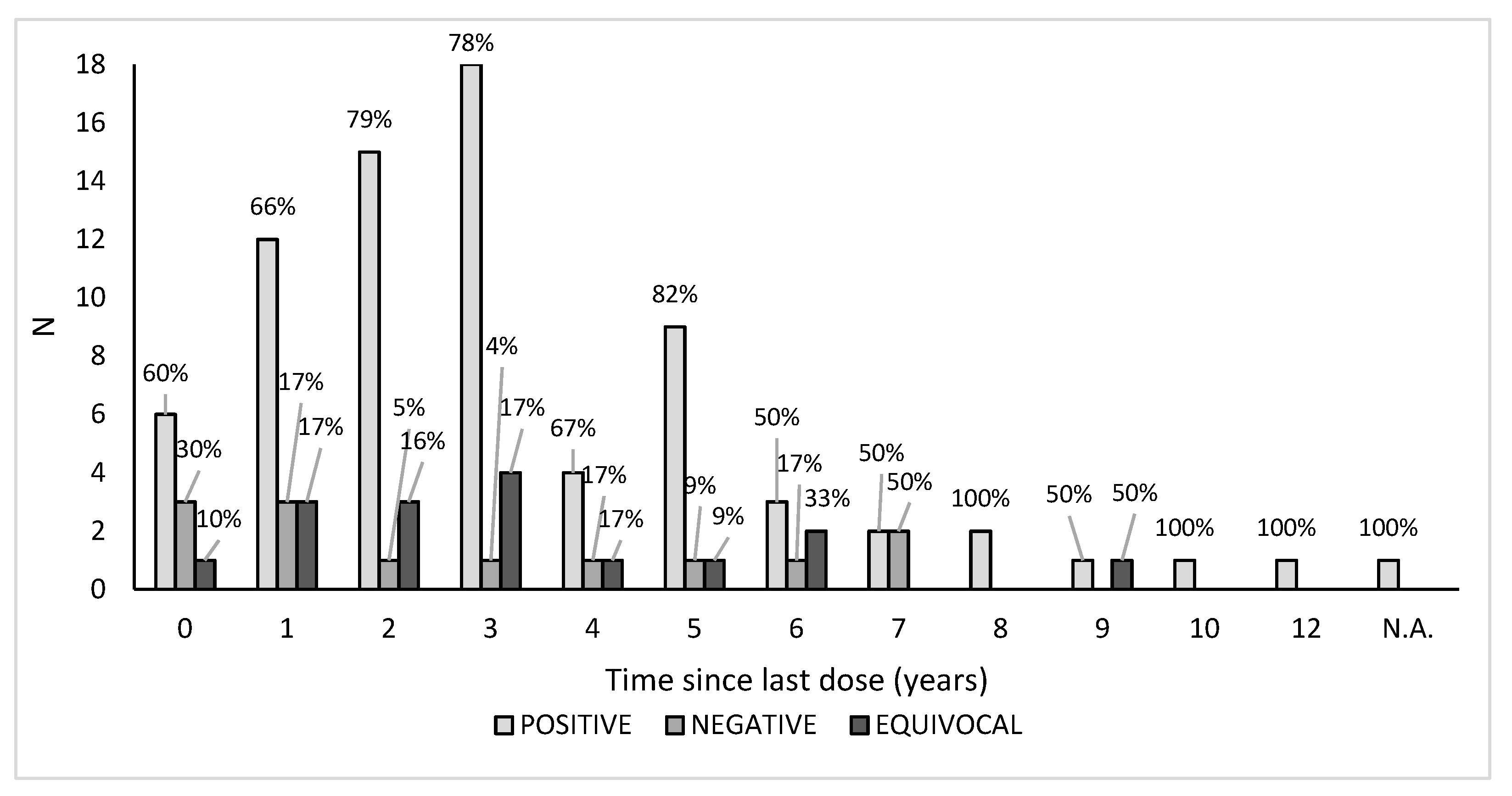
3.3. Vaccination Status against Varicella and Seroprevalence Assessment
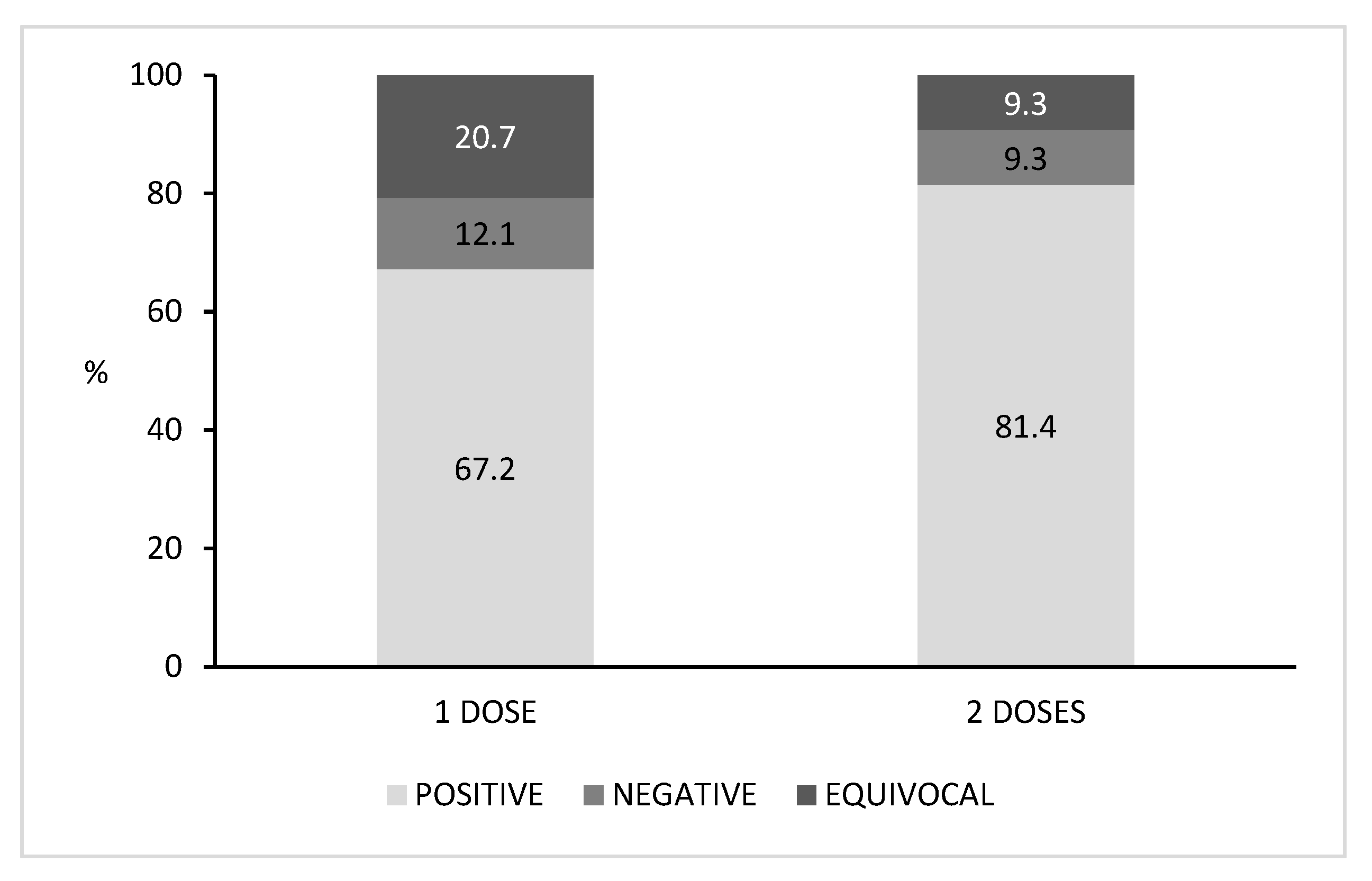
3.4. Seroprevalence Distribution Related to the Number of Vaccine Doses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Varicella-Vaccine-Preventable Diseases 2010. Available online: https://www.who.int/immunization/monitoring_surveillance/burden/vpd/WHO_SurveillanceVaccinePreventable_22_Varicella_R2.pdf?ua=1 (accessed on 19 January 2021).
- Best, J.M.; Reef, S. The Immunological Basis for Immunization Series-Varicella-zoster virus. Immunol. Basis Immun. Ser. Modul. 11 Rubella 2008, Module 11, 1–24. [Google Scholar]
- CDC. Prevention for Varicella—Recommendations of the Advisory Committee on Immunization Practices (ACIP). Available online: https://www.cdc.gov/mmwr/preview/mmwrhtml/rr5604a1.htm (accessed on 8 February 2021).
- Sauerbrei, A.; Wutzler, P. The congenital varicella syndrome. J. Perinatol. 2000, 20, 548–554. [Google Scholar] [CrossRef]
- Gershon, A.A.; Breuer, J.; Cohen, J.I.; Cohrs, R.J.; Gershon, M.D.; Gilden, D.; Grose, C.; Hambleton, S.; Kennedy, P.G.E.; Oxman, M.N.; et al. Varicella zoster virus infection. Nat. Rev. Dis. Prim. 2015, 1, 1–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takahashi, M.; Otsuka, T.; Okuno, Y.; Asano, Y.; Yazaki, T.; Isomura, S. Live vaccine used to prevent the spread of varicella in children in hospital. Lancet 1974, 304, 1288–1290. [Google Scholar] [CrossRef]
- Marin, M.; Güris, D.; Chaves, S.S.; Schmid, S.; Seward, J.F. Prevention of varicella: Recommendations of the Advisory Committee on Immunization Practices (ACIP). In Morbidity and Mortality Weekly Report; CDC: Atlanta, GA, USA, 2007. [Google Scholar]
- Kauffmann, F.; Bechini, A.; Bonanni, P.; Casabona, G.; Wutzler, P. Varicella Vaccination in Italy and Germany—Different Routes to Success: A Systematic Review. Expert Rev. Vaccines 2020, 19, 843–869. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. ECDC Guidance—Varicella Vaccination in the European Union; ECDC: Solna, Sweden, 2015; ISBN 9789291936199/9789291936199. Available online: https://www.ecdc.europa.eu/sites/default/files/media/en/publications/Publications/Varicella-Guidance-2015.pdf (accessed on 19 January 2021).
- European Centre for Disease Prevention and Control. Vaccine Scheduler. Available online: https://vaccine-schedule.ecdc.europa.eu/Scheduler/ByDisease?SelectedDiseaseId=48&SelectedCountryIdByDisease=-1%3E (accessed on 10 January 2021).
- Spoulou, V.; Alain, S.; Gabutti, G.; Giaquinto, C.; Liese, J.; Martinon-Torres, F.; Vesikari, T. Implementing universal varicella vaccination in europe: The path forward. Pediatr. Infect. Dis. J. 2019, 38, 181–188. [Google Scholar] [CrossRef] [PubMed]
- García, F.J.Á.; Ortega, M.J.C.; Aldeán, J.Á.; Garcés-Sánchez, M.; Sánchez, N.G.; Llanos, E.G.; Merino, Á.H.; de Arce, A.I.; Moína, M.M.; Melián, A.M.; et al. Immunisation Schedule of the Spanish Association of Paediatrics: 2020 Recommendations. An. Pediatría 2020, 92, 52.e1–52.e10. [Google Scholar] [CrossRef]
- Bonanni, P.; Breuer, J.; Gershon, A.; Gershon, M.; Hryniewicz, W.; Papaevangelou, V.; Rentier, B.; Rümke, H.; Sadzot-Delvaux, C.; Senterre, J.; et al. Varicella vaccination in Europe—Taking the practical approach. BMC Med. 2009, 7, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bechini, A.; Boccalini, S.; Baldo, V.; Cocchio, S.; Castiglia, P.; Gallo, T.; Giuffrida, S.; Locuratolo, F.; Tafuri, S.; Martinelli, D.; et al. Impact of universal vaccination against varicella in Italy. Hum. Vaccin. Immunother. 2015, 11, 63–71. [Google Scholar] [CrossRef] [Green Version]
- Ministero della Salute. Piano Nazionale Prevenzione Vaccinale 2017–2019. Available online: http://www.salute.gov.it/imgs/C_17_pubblicazioni_2571_allegato.pdf (accessed on 10 December 2020).
- Ministero della Salute. Direzione Generale della Prevenzione Sanitaria. Ufficio 5—Prevenzione delle Malattie Trasmissibili e Profilassi Internazionale. (Unpublished Data).
- ARS Toscana. La Sorveglianza Epidemiologica delle Malattie Infettive in Toscana. 2019. Available online: https://www.ars.toscana.it/images/pubblicazioni/Rapporti/2019/Rapporto_malattie_infettive.pdf (accessed on 10 December 2020).
- Ciofi Degli Atti, M.L.; Rota, M.C.; Mandolini, D.; Bella, A.; Gabutti, G.; Crovari, P.; Salmaso, S. Assessment of varicella underreporting in Italy. Epidemiol. Infect. 2002, 128, 479–484. [Google Scholar] [CrossRef]
- Zanella, B.; Boccalini, S.; Bonito, B.; Del Riccio, M.; Tiscione, E.; Bonanni, P.; Dhs, W.G.; Aoumeyer, W.G.; Ausltc, W.G.; Bechini, A.; et al. Increasing Measles Seroprevalence in a Sample of Pediatric and Adolescent Population of Tuscany (Italy): A Vaccination Campaign Success. Vaccines 2020, 8, 512. [Google Scholar] [CrossRef] [PubMed]
- Zanella, B.; Boccalini, S.; Bonito, B.; Del Riccio, M.; Manzi, F.; Tiscione, E.; Bonanni, P.; Bianchi, J.; Biondi, I.; Chellini, M.; et al. Rubella seroprevalence boost in the pediatric and adolescent population of florence (Italy) as a preventive strategy for congenital rubella syndrome (CRS). Vaccines 2020, 8, 599. [Google Scholar] [CrossRef]
- Zanella, B.; Bechini, A.; Boccalini, S.; Sartor, G.; Tiscione, E.; Bonanni, P. Hepatitis B Seroprevalence in the Pediatric and Adolescent Population of Florence (Italy): An Update 27 Years after the Implementation of Universal Vaccination. Vaccines 2020, 8, 156. [Google Scholar] [CrossRef] [Green Version]
- GeoDemo Istat. Popolazione Residente al 1° Gennaio 2017 nella Provincia di Firenze. Available online: http://demo.istat.it/pop2017/index.html (accessed on 10 December 2020).
- Istat. Natalità e Fecondità della Popolazione Residente | Anno 2018; Volume 444. Available online: https://www.istat.it/it/files/2019/11/Report_natalit%C3%A0_anno2018_def.pdf (accessed on 20 January 2021).
- Fornaro, P.; Gandini, F.; Marin, M.; Pedrazzi, C.; Piccoli, P.; Tognetti, D.; Assael, B.M.; Lucioni, C.; Mazzi, S. Epidemiology and cost analysis of varicella in Italy: Results of a sentinel study in the pediatric practice. Italian Sentinel Group on Pediatric Infectious Diseases. Pediatr. Infect. Dis. J. 1999, 18, 414–419. [Google Scholar] [CrossRef] [PubMed]
- Holmes, C.N. Predictive value of a history of varicella infection. Can. Fam. Physician 2005, 51, 60–65. [Google Scholar]
- Regione Toscana. Antivaricella. Available online: https://www.regione.toscana.it/-/antivaricella (accessed on 10 December 2020).
- Michalik, D.E.; Steinberg, S.P.; LaRussa, P.S.; Edwards, K.M.; Wright, P.F.; Arvin, A.M.; Gans, H.A.; Gershon, A.A. Primary vaccine failure after 1 dose of varicella vaccine in healthy children. J. Infect. Dis. 2008, 197, 944–949. [Google Scholar] [CrossRef]
- Lopez, A.S.; Guris, D.; Zimmerman, L.; Gladden, L.; Moore, T.; Haselow, D.T.; Loparev, V.N.; Schmid, D.S.; Jumaan, A.O.; Snow, S.L. One dose of varicella vaccine does not prevent school outbreaks: Is it time for a second dose? Pediatrics 2006, 117, e1070–e1077. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galil, K.; Fair, E.; Mountcastle, N.; Britz, P.; Seward, J. Younger age at vaccination may increase risk of varicella vaccine failure. J. Infect. Dis. 2002, 186, 102–105. [Google Scholar] [CrossRef]
- Izurieta, H.S.; Strebel, P.M.; Blake, P.A. Postlicensure effectiveness of varicella vaccine during an outbreak in a child care center. J. Am. Med. Assoc. 1997, 278, 1495–1499. [Google Scholar] [CrossRef]
- CDC. Prevention of Varicella. In Morbidity and Mortality Weekly Report; CDC: Atlanta, GA, USA, 2007; Volume 56, pp. 1–55. [Google Scholar]
- Kuter, B.; Matthews, H.; Shinefield, H.; Black, S.; Dennehy, P.; Watson, B.; Reisinger, K.; Kim, L.L.; Lupinacci, L.; Hartzel, J.; et al. Ten year follow-up of healthy children who received one or two injections of varicella vaccine. Pediatr. Res. 2004, 23, 132–137. [Google Scholar] [CrossRef]
- Watson, B.; Rothstein, E.; Bernstein, H.; Arbeter, A.; Arvin, A.; Chartrand, S.; Clements, D.; Kumar, M.L.; Reisinger, K.; Blatter, M.; et al. Safety and cellular and humoral immune responses of a booster dose of varicella vaccine 6 years after primary immunization. J. Infect. Dis. 1995, 172, 217–219. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Anti-VZV Seroprevalence | |||
|---|---|---|---|
| Group | Positive % (n/N) | Negative % (n/N) | Equivocal % (n/N) |
| Male | 75.9 (66/87) | 14.9 (13/87) | 9.2 (8/87) |
| Female | 75.6 (59/78) | 11.5 (9/78) | 12.8 (10/78) |
| Italian | 75.8 (113/149) | 12.8 (19/149) | 11.4 (17/149) |
| Non-Italian | 75.0 (12/16) | 18.8 (3/16) | 6.3 (1/16) |
| Overall | 75.8 (125/165) | 13.3 (22/165) | 10.9 (18/165) |
| Year of Birth | Age at the Time of Enrolment (Years) | Sex | Notification (Year) | Age at the Time of Disease Notification (Years) |
|---|---|---|---|---|
| 2000 | 17 | F | 2006 | 6 |
| 2002 | 16 | M | 2006 | 4 |
| 2002 | 15 | M | 2006 | 4 |
| 2004 | 14 | F | 2008 | 4 |
| 2006 | 11 | M | 2010 | 4 |
| 2007 | 10 | M | 2011 | 4 |
| 2012 | 5 | F | 2015 | 3 |
| Vaccination Status | Age Group (years) | Positive % (n/N) | Negative % (n/N) | Equivocal % (n/N) | Total % (n/N) |
|---|---|---|---|---|---|
| Vaccinated | 73.3 (74/101) | 10.9 (11/101) | 15.8 (16/101) | 61.2 (101/165) | |
| 1–4 | 74.3 (26/35) | 8.6 (3/35) | 17.1 (6/35) | 34.7 (35/101) | |
| 5–9 | 71.8 (28/39) | 12.8 (5/39) | 15.4 (6/39) | 38.6 (39/101) | |
| 10–14 | 65.0 (13/20) | 15.0 (3/20) | 20.0 (4/20) | 19.8 (20/101) | |
| 15–18 | 100.0 (7/7) | 0.0 (0/7) | 0.0 (0/7) | 6.9 (7/101) | |
| Unvaccinated | 79.7 (51/64) | 17.2 (11/64) | 3.1 (2/64) | 38.8 (64/165) | |
| 1–4 | 0.0 (0/5) | 100.0 (5/5) | 0.0 (0/5) | 7.8 (5/64) | |
| 5–9 | 55.6 (5/9) | 22.2 (2/9) | 22.2 (2/9) | 14.1 (9/64) | |
| 10–14 | 90.0 (27/30) | 10.0 (3/10) | 0.0 (0/29) | 46.9 (30/64) | |
| 15–18 | 95.0 (19/20) | 5.0 (1/20) | 0.0 (0/20) | 31.2 (20/64) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zanella, B.; Bechini, A.; Bonito, B.; Del Riccio, M.; Ninci, A.; Tiscione, E.; Working Group DHS; Working Group AOUMeyer; Working Group AUSLTC; Bonanni, P.; et al. A Study of Varicella Seroprevalence in a Pediatric and Adolescent Population in Florence (Italy). Natural Infection and Vaccination-Acquired Immunization. Vaccines 2021, 9, 152. https://doi.org/10.3390/vaccines9020152
Zanella B, Bechini A, Bonito B, Del Riccio M, Ninci A, Tiscione E, Working Group DHS, Working Group AOUMeyer, Working Group AUSLTC, Bonanni P, et al. A Study of Varicella Seroprevalence in a Pediatric and Adolescent Population in Florence (Italy). Natural Infection and Vaccination-Acquired Immunization. Vaccines. 2021; 9(2):152. https://doi.org/10.3390/vaccines9020152
Chicago/Turabian StyleZanella, Beatrice, Angela Bechini, Benedetta Bonito, Marco Del Riccio, Alessandra Ninci, Emilia Tiscione, Working Group DHS, Working Group AOUMeyer, Working Group AUSLTC, Paolo Bonanni, and et al. 2021. "A Study of Varicella Seroprevalence in a Pediatric and Adolescent Population in Florence (Italy). Natural Infection and Vaccination-Acquired Immunization" Vaccines 9, no. 2: 152. https://doi.org/10.3390/vaccines9020152
APA StyleZanella, B., Bechini, A., Bonito, B., Del Riccio, M., Ninci, A., Tiscione, E., Working Group DHS, Working Group AOUMeyer, Working Group AUSLTC, Bonanni, P., & Boccalini, S. (2021). A Study of Varicella Seroprevalence in a Pediatric and Adolescent Population in Florence (Italy). Natural Infection and Vaccination-Acquired Immunization. Vaccines, 9(2), 152. https://doi.org/10.3390/vaccines9020152