
Vaccination Status of Mothers and Children from the ‘Mamma & Bambino’ Cohort

 ,
,  ,
, 
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Collection
2.3. Statistical Analyses
3. Results
3.1. Characteristics of Study Population
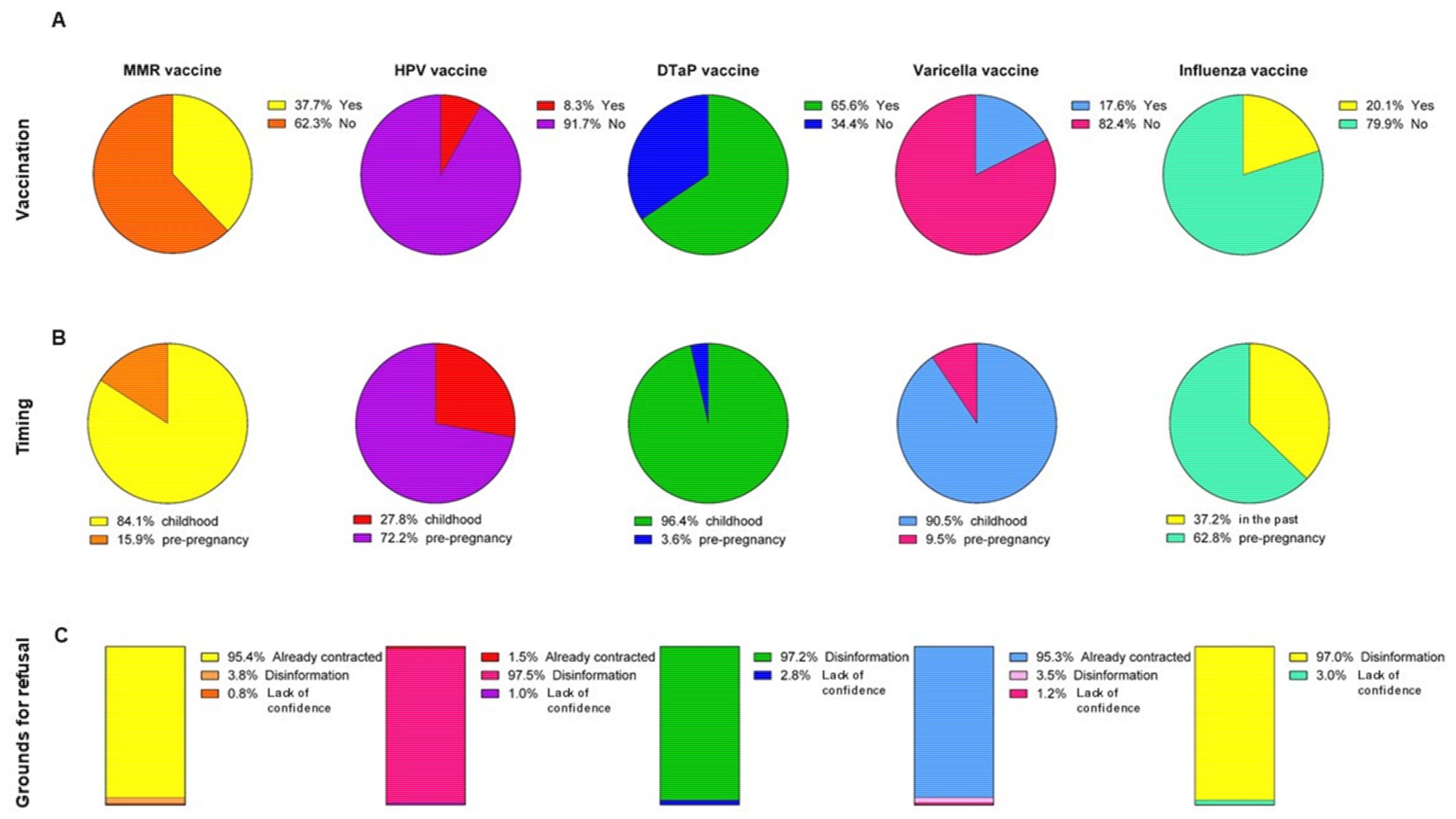
3.2. Vaccination Choice among Women
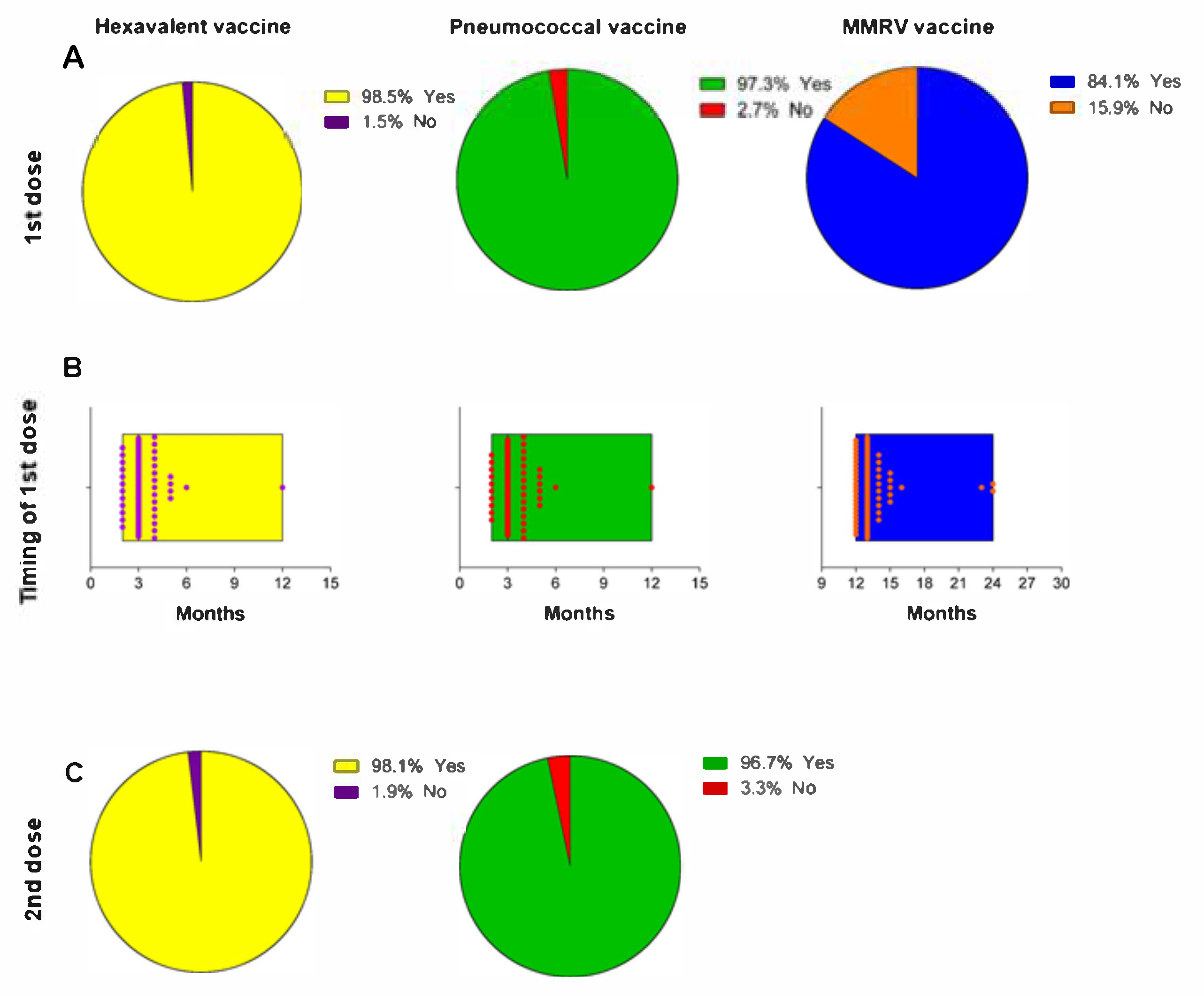
3.3. Vaccination Status of Children
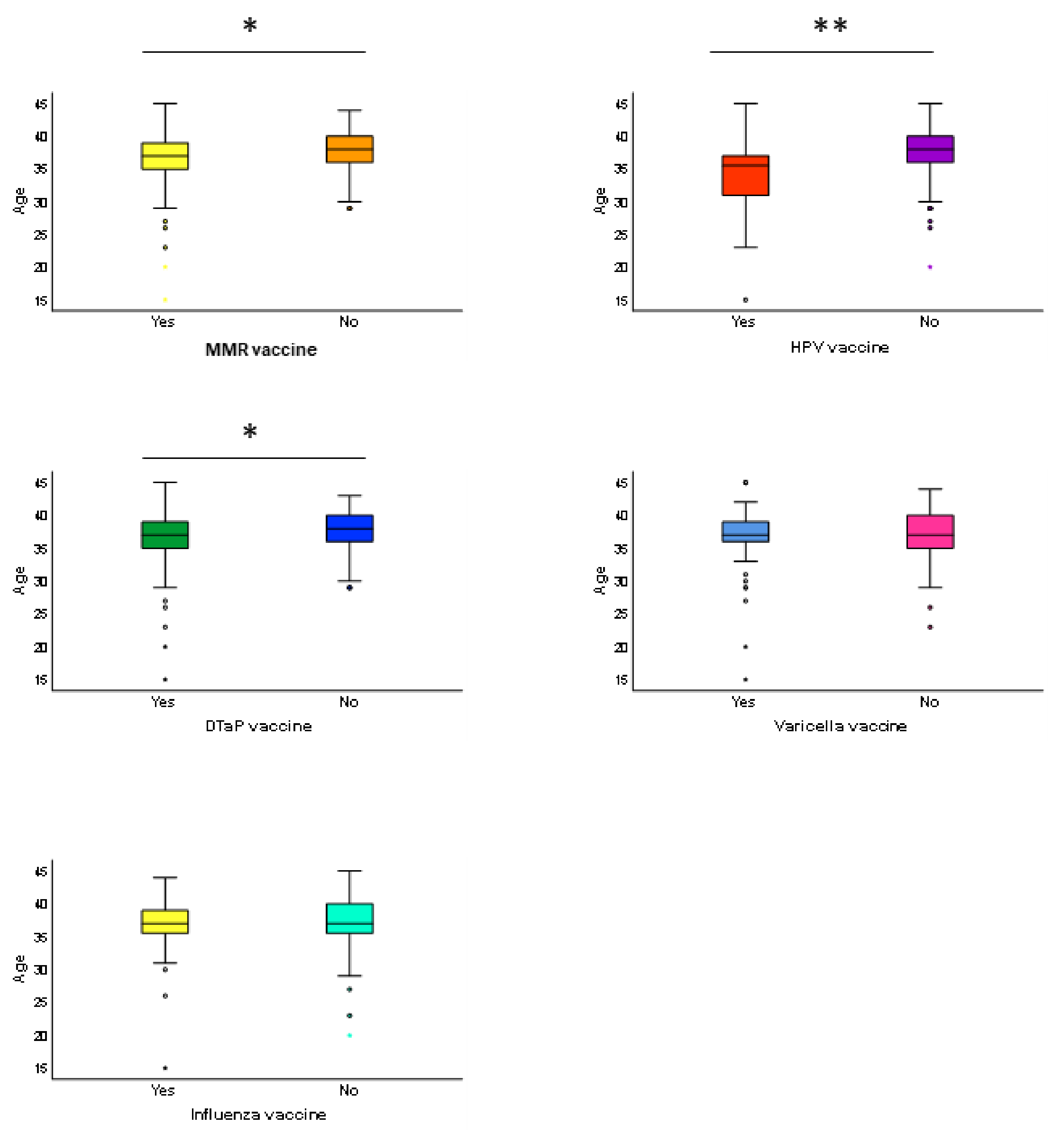
3.4. Association between Age and Vaccination Choice
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ammon, A.; Prats Monné, X. Vaccines, trust and European public health. Euro. Surveill. 2018, 23. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Imunization Agenda 2030: A global strategy to leave no one behind. 2020. Available online: https://www.who.int/immunization/immunization_agenda_2030/en/. (accessed on 15 January 2021).
- World Health Organization. Global vaccine action plan 2011–2020. 2013. Available online: https://www.who.int/immunization/global_vaccine_action_plan/en/. (accessed on 15 January 2021).
- World Health Organization. Imunization, Vaccines and Biologicals: vaccines and diseases. 2020. Available online: https://www.who.int/immunization/diseases/en/. (accessed on 15 January 2021).
- Bandyopadhyay, A.S.; Garon, J.; Seib, K.; Orenstein, W.A. Polio vaccination: past, present and future. Future Microbiol. 2015, 10, 791–808. [Google Scholar] [CrossRef] [Green Version]
- Thèves, C.; Crubézy, E.; Biagini, P. History of Smallpox and Its Spread in Human Populations. Microbiol. Spectr. 2016, 4. [Google Scholar] [CrossRef]
- Barchitta, M.; Quattrocchi, A.; Maugeri, A.; La Rosa, M.C.; La Mastra, C.; Sessa, L.; Cananzi, P.; Murolo, G.; Oteri, A.; Basile, G.; et al. Antibiotic Consumption and Resistance during a 3-Year Period in Sicily, Southern Italy. Int. J. Environ. Res. Public Health 2019, 16. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Strategic Advisory Group of Experts on Imunization. Assessment report of the global vaccine action plan. 2017. Available online: https://www.who.int/immunization/web_2017_sage_gvap_assessment_report_en.pdf. (accessed on 15 January 2021).
- Barchitta, M.; Basile, G.; Lopalco, P.L.; Agodi, A. Vaccine-preventable diseases and vaccination among Italian healthcare workers: a review of current literature. Future Microbiol. 2019, 14, 15–19. [Google Scholar] [CrossRef]
- Tavoschi, L.; Quattrone, F.; Agodi, A.; Lopalco, P.L. Risk of transmission of vaccine-preventable diseases in healthcare settings. Future Microbiol. 2019, 14, 9–14. [Google Scholar] [CrossRef]
- Odone, A.; Fara, G.M.; Giammaco, G.; Blangiardi, F.; Signorelli, C. The future of immunization policies in Italy and in the European Union: The Declaration of Erice. Hum. Vaccin. Immunother. 2015, 11, 1268–1271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sheikh, S.; Biundo, E.; Courcier, S.; Damm, O.; Launay, O.; Maes, E.; Marcos, C.; Matthews, S.; Meijer, C.; Poscia, A.; et al. A report on the status of vaccination in Europe. Vaccine 2018, 36, 4979–4992. [Google Scholar] [CrossRef] [PubMed]
- Signorelli, C.; Odone, A.; Pezzetti, F.; Spagnoli, F.; Visciarelli, S.; Ferrari, A.; Camia, P.; Latini, C.; Ciorba, V.; Agodi, A.; et al. Human Papillomavirus infection and vaccination: knowledge and attitudes of Italian general practitioners. Epidemiol. Prev. 2014, 38, 88–92. [Google Scholar] [PubMed]
- Haralambieva, I.H.; Ovsyannikova, I.G.; Kennedy, R.B.; Goergen, K.M.; Grill, D.E.; Chen, M.H.; Hao, L.; Icenogle, J.; Poland, G.A. Rubella virus-specific humoral immune responses and their interrelationships before and after a third dose of measles-mumps-rubella vaccine in women of childbearing age. Vaccine 2020, 38, 1249–1257. [Google Scholar] [CrossRef]
- Zacharis, K.; Messini, C.I.; Anifandis, G.; Koukoulis, G.; Satra, M.; Daponte, A. Human Papilloma Virus (HPV) and Fertilization: A Mini Review. Medicina (Kaunas) 2018, 54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baxter, R.; Bartlett, J.; Fireman, B.; Lewis, E.; Klein, N.P. Effectiveness of Vaccination During Pregnancy to Prevent Infant Pertussis. Pediatrics 2017, 139. [Google Scholar] [CrossRef] [Green Version]
- Nunes, M.C.; Cutland, C.L.; Jones, S.; Downs, S.; Weinberg, A.; Ortiz, J.R.; Neuzil, K.M.; Simões, E.A.F.; Klugman, K.P.; Madhi, S.A. Efficacy of Maternal Influenza Vaccination Against All-Cause Lower Respiratory Tract Infection Hospitalizations in Young Infants: Results From a Randomized Controlled Trial. Clin. Infect. Dis. 2017, 65, 1066–1071. [Google Scholar] [CrossRef]
- Skoff, T.H.; Blain, A.E.; Watt, J.; Scherzinger, K.; McMahon, M.; Zansky, S.M.; Kudish, K.; Cieslak, P.R.; Lewis, M.; Shang, N.; et al. Impact of the US Maternal Tetanus, Diphtheria, and Acellular Pertussis Vaccination Program on Preventing Pertussis in Infants. Clin. Infect. Dis. 2017, 65, 1977–1983. [Google Scholar] [CrossRef] [Green Version]
- Zerbo, O.; Modaressi, S.; Chan, B.; Goddard, K.; Lewis, N.; Bok, K.; Fireman, B.; Klein, N.P.; Baxter, R. No association between influenza vaccination during pregnancy and adverse birth outcomes. Vaccine 2017, 35, 3186–3190. [Google Scholar] [CrossRef] [PubMed]
- D’Alessandro, A.; Napolitano, F.; D’Ambrosio, A.; Angelillo, I.F. Vaccination knowledge and acceptability among pregnant women in Italy. Hum. Vaccin. Immunother. 2018, 14, 1573–1579. [Google Scholar] [CrossRef] [Green Version]
- Blanchard-Rohner, G.; Eberhardt, C. Review of maternal immunisation during pregnancy: focus on pertussis and influenza. Swiss Med. Wkly. 2017, 147, w14526. [Google Scholar] [CrossRef] [PubMed]
- Piano Nazionale Prevenzione Vaccinale. Available online: http://www.salute.gov.it/imgs/C_17_pubblicazioni_2571_allegato.pdf (accessed on 15 January 2021).
- Laenen, J.; Roelants, M.; Devlieger, R.; Vandermeulen, C. Influenza and pertussis vaccination coverage in pregnant women. Vaccine 2015, 33, 2125–2131. [Google Scholar] [CrossRef]
- Ding, H.; Kahn, K.E.; Black, C.L.; O’Halloran, A.; Lu, P.J.; Williams, W.W. Influenza Vaccination Coverage Among Pregnant Women in the U.S., 2012–2015. Am. J. Prev. Med. 2019, 56, 477–486. [Google Scholar] [CrossRef]
- Delamater, P.L.; Leslie, T.F.; Yang, Y.T. Change in Medical Exemptions from Immunization in California After Elimination of Personal Belief Exemptions. JAMA 2017, 318, 863–864. [Google Scholar] [CrossRef]
- Ricciardi, W.; Boccia, S.; Siliquini, R. Moving towards compulsory vaccination: the Italian experience. Eur. J. Public Health 2018, 28, 2–3. [Google Scholar] [CrossRef] [PubMed]
- Ward, J.K.; Colgrove, J.; Verger, P. Why France is making eight new vaccines mandatory. Vaccine 2018, 36, 1801–1803. [Google Scholar] [CrossRef]
- Signorelli, C.; Odone, A.; Cella, P.; Iannazzo, S. Childhood vaccine coverage in Italy after the new law on mandatory immunization. Ann. Ig. 2018, 30, 1–10. [Google Scholar] [CrossRef]
- Rezza, G. Mandatory vaccination for infants and children: the Italian experience. Pathog. Glob. Health 2019, 113, 291–296. [Google Scholar] [CrossRef] [Green Version]
- MacDonald, N.E.; Harmon, S.; Dube, E.; Steenbeek, A.; Crowcroft, N.; Opel, D.J.; Faour, D.; Leask, J.; Butler, R. Mandatory infant & childhood immunization: Rationales, issues and knowledge gaps. Vaccine 2018, 36, 5811–5818. [Google Scholar] [CrossRef] [PubMed]
- European Center for Disease Prevention and Control. Let’s talk about hesitancy. In Enhancing confidence in vaccination and uptake 2016; ECDC: Stockholm, Sweden; Available online: https://www.ecdc.europa.eu/sites/portal/files/media/en/publications/Publications/lets-talk-about-hesitancy-vaccination-guide.pdf. (accessed on 15 January 2021).
- Dubé, E.; Laberge, C.; Guay, M.; Bramadat, P.; Roy, R.; Bettinger, J. Vaccine hesitancy: an overview. Hum. Vaccin. Immunother. 2013, 9, 1763–1773. [Google Scholar] [CrossRef] [PubMed]
- Glatman-Freedman, A.; Nichols, K. The effect of social determinants on immunization programs. Hum. Vaccin. Immunother. 2012, 8, 293–301. [Google Scholar] [CrossRef] [Green Version]
- Maugeri, A.; Barchitta, M.; Agrifoglio, O.; Favara, G.; La Mastra, C.; La Rosa, M.C.; Magnano San Lio, R.; Panella, M.; Cianci, A.; Agodi, A. The impact of social determinants and lifestyles on dietary patterns during pregnancy: evidence from the “Mamma & Bambino” study. Ann. Ig. 2019, 31, 81–89. [Google Scholar] [CrossRef]
- Barchitta, M.; Maugeri, A.; La Rosa, M.C.; Magnano San Lio, R.; Favara, G.; Panella, M.; Cianci, A.; Agodi, A. Single Nucleotide Polymorphisms in Vitamin D Receptor Gene Affect Birth Weight and the Risk of Preterm Birth: Results From the “Mamma & Bambino” Cohort and A Meta-Analysis. Nutrients 2018, 10. [Google Scholar] [CrossRef] [Green Version]
- Duclos, P. National Immunization Technical Advisory Groups (NITAGs): guidance for their establishment and strengthening. Vaccine 2010, 28. [Google Scholar] [CrossRef] [PubMed]
- Takla, A.; Wichmann, O.; Carrillo-Santisteve, P.; Cotter, S.; Levy-Bruhl, D.; Paradowska-Stankiewicz, I.; Valentiner-Branth, P.; D’Ancona, F.; Group, V.I.N.S. Characteristics and practices of National Immunisation Technical Advisory Groups in Europe and potential for collaboration, April 2014. Euro. Surveill. 2015, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Commission. Vaccination. Available online: https://ec.europa.eu/health/vaccination/overview_en. (accessed on 15 January 2021).
- The Lancet. Addressing decreasing vaccine coverage in the EU. Lancet 2018, 391, 1638. [Google Scholar] [CrossRef]
- Italian Ministry of Health. Vaccinazioni raccomandate per le donne in età fertile e in gravidanza, Novembre 2018. Available online: http://www.trovanorme.salute.gov.it/norme/renderNormsanPdfanno=2018&codLeg=66751&parte=1%20&serie=null. (accessed on 15 January 2021).
- Chamberlain, A.T.; Seib, K.; Ault, K.A.; Orenstein, W.A.; Frew, P.M.; Malik, F.; Cortés, M.; Cota, P.; Whitney, E.A.; Flowers, L.C.; et al. Factors Associated with Intention to Receive Influenza and Tetanus, Diphtheria, and Acellular Pertussis (Tdap) Vaccines during Pregnancy: A Focus on Vaccine Hesitancy and Perceptions of Disease Severity and Vaccine Safety. PLoS Curr. 2015, 7. [Google Scholar] [CrossRef]
- Donaldson, B.; Jain, P.; Holder, B.S.; Lindsey, B.; Regan, L.; Kampmann, B. What determines uptake of pertussis vaccine in pregnancy? A cross sectional survey in an ethnically diverse population of pregnant women in London. Vaccine 2015, 33, 5822–5828. [Google Scholar] [CrossRef] [Green Version]
- Healy, C.M.; Rench, M.A.; Montesinos, D.P.; Ng, N.; Swaim, L.S. Knowledge and attitiudes of pregnant women and their providers towards recommendations for immunization during pregnancy. Vaccine 2015, 33, 5445–5451. [Google Scholar] [CrossRef] [PubMed]
- Ditsungnoen, D.; Greenbaum, A.; Praphasiri, P.; Dawood, F.S.; Thompson, M.G.; Yoocharoen, P.; Lindblade, K.A.; Olsen, S.J.; Muangchana, C. Knowledge, attitudes and beliefs related to seasonal influenza vaccine among pregnant women in Thailand. Vaccine 2016, 34, 2141–2146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacDougall, D.M.; Halperin, B.A.; Langley, J.M.; McNeil, S.A.; MacKinnon-Cameron, D.; Li, L.; Halperin, S.A. Knowledge, attitudes, beliefs, and behaviors of pregnant women approached to participate in a Tdap maternal immunization randomized, controlled trial. Hum. Vaccin. Immunother. 2016, 12, 879–885. [Google Scholar] [CrossRef] [Green Version]
- Larson, H.J.; Jarrett, C.; Eckersberger, E.; Smith, D.M.; Paterson, P. Understanding vaccine hesitancy around vaccines and vaccination from a global perspective: a systematic review of published literature, 2007–2012. Vaccine 2014, 32, 2150–2159. [Google Scholar] [CrossRef]
- McClure, C.C.; Cataldi, J.R.; O’Leary, S.T. Vaccine Hesitancy: Where We Are and Where We Are Going. Clin. Ther. 2017, 39, 1550–1562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Figueiredo, A.; Johnston, I.; Smith, D.M.; Larson, H.J.; Jones, N. Changing socioeconomic determinants of childhood vaccines: a global analysis over three decades. Lancet Glob. Health 2015, 3, S20. [Google Scholar] [CrossRef] [Green Version]
- Signorelli, C.; Odone, A.; Cella, P.; Iannazzo, S.; D’Ancona, F.; Guerra, R. Infant immunization coverage in Italy (2000–2016). Ann. Ist. Super. Sanita 2017, 53, 231–237. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Measles and Rubella Surveillance Data. Surveillance data from 2017-06 to 2017-11. Available online: https://www.who.int/immunization/monitoring_surveillance/burden/vpd/surveillance_type/active/measles_monthlydata/en/ (accessed on 15 January 2021).
- European Center for Disease Prevention and Control. Vaccine Scheduler. In Vaccine schedules in all countries of the European Union; ECDC: Stockholm, Sweden; Available online: https://vaccine-schedule.ecdc.europa.eu/. (accessed on 15 January 2021).
- European Commission; 12 September 2017. Available online: http://europa.eu/rapid/press-release_SPEECH-17-3165_en.htm (accessed on 15 January 2021).
- D’Ancona, F.; D’Amario, C.; Maraglino, F.; Rezza, G.; Ricciardi, W.; Iannazzo, S. Introduction of new and reinforcement of existing compulsory vaccinations in Italy: first evaluation of the impact on vaccination coverage in 2017. Euro. Surveill. 2018, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Ancona, F.; D’Amario, C.; Maraglino, F.; Rezza, G.; Iannazzo, S. The law on compulsory vaccination in Italy: an update 2 years after the introduction. Euro. Surveill. 2019, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- 2018. Available online: https://www.who.int/immunization/monitoring_surveillance/who-immuniz.pdf?ua=1. (accessed on 15 January 2021).



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barchitta, M.; Maugeri, A.; Magnano San Lio, R.; La Rosa, M.C.; La Mastra, C.; Favara, G.; Giunta, G.; Cianci, A.; Agodi, A. Vaccination Status of Mothers and Children from the ‘Mamma & Bambino’ Cohort. Vaccines 2021, 9, 168. https://doi.org/10.3390/vaccines9020168
Barchitta M, Maugeri A, Magnano San Lio R, La Rosa MC, La Mastra C, Favara G, Giunta G, Cianci A, Agodi A. Vaccination Status of Mothers and Children from the ‘Mamma & Bambino’ Cohort. Vaccines. 2021; 9(2):168. https://doi.org/10.3390/vaccines9020168
Chicago/Turabian StyleBarchitta, Martina, Andrea Maugeri, Roberta Magnano San Lio, Maria Clara La Rosa, Claudia La Mastra, Giuliana Favara, Giuliana Giunta, Antonio Cianci, and Antonella Agodi. 2021. "Vaccination Status of Mothers and Children from the ‘Mamma & Bambino’ Cohort" Vaccines 9, no. 2: 168. https://doi.org/10.3390/vaccines9020168
APA StyleBarchitta, M., Maugeri, A., Magnano San Lio, R., La Rosa, M. C., La Mastra, C., Favara, G., Giunta, G., Cianci, A., & Agodi, A. (2021). Vaccination Status of Mothers and Children from the ‘Mamma & Bambino’ Cohort. Vaccines, 9(2), 168. https://doi.org/10.3390/vaccines9020168