
Understanding the Influence of Individual and Systemic Factors on Vaccination Take-Up in European Citizens Aged 55 or Older


Abstract
:1. Introduction
2. Methods
2.1. Data
2.2. Variables
2.3. Statistical Analysis
3. Results
3.1. Descriptive Results
3.2. Explanatory Factors of Vaccination Up-Take
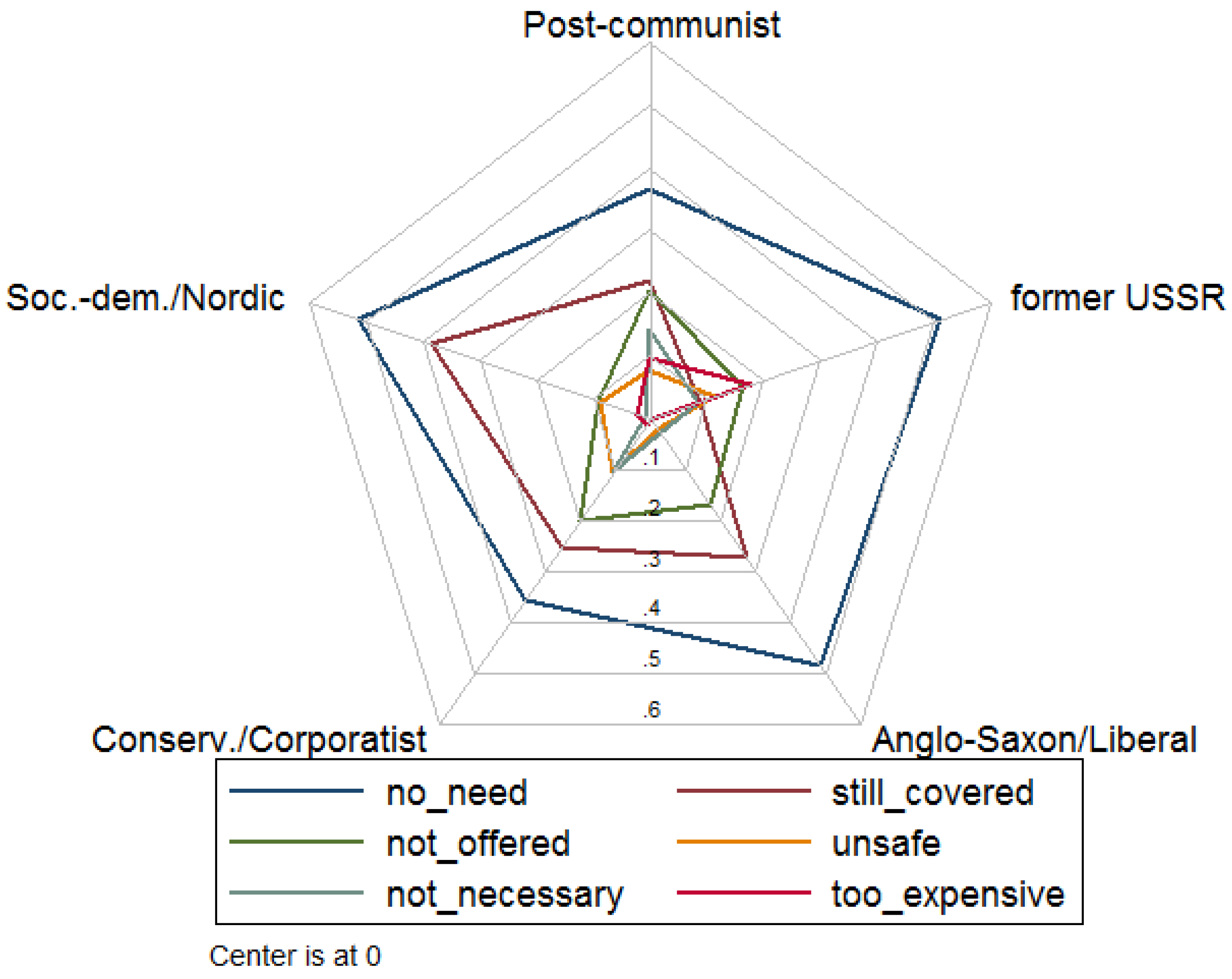
3.3. Reasons for no Vaccination
3.4. Information on Vaccination and Attitude on Vaccination Programs
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- European Centre for Disease Prevention and Control (ECDC). Let’s Talk about Protection; ECDC: Stockholm, Sweden, 2016. [Google Scholar]
- WHO. Ten Threats to Global Health in 2019; WHO: Geneva, Switzerland, 2019. [Google Scholar]
- European Centre for Disease Prevention and Control (ECDC). Vaccine Scheduler; ECDC: Stockholm, Sweden, 2020. [Google Scholar]
- Yaqub, O.; Castle-Clarke, S.; Sevdalis, N.; Chataway, J. Attitudes to vaccination: A critical review. Soc. Sci. Med. 2014, 112, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Machado, A.; Mazagatos, C.; Dijkstra, F.; Kislaya, I.; Gherasim, A.; McDonald, S.A.; Kissling, E.; Valenciano, M.; Meijer, A.; Hooiveld, M.; et al. Impact of influenza vaccination programmes among the elderly population on primary care, Portugal, Spain and The Netherlands: 2015/16 to 2017/18 influenza seasons. Eurosurveillance 2019, 24, 1900268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Centre for Disease Prevention and Control (ECDC). Let’s Talk about Hesitancy: Enhancing Confidence in Vaccination and Uptake; ECDC: Stockholm, Sweden, 2016. [Google Scholar]
- Ciabattini, A.; Nardini, C.; Santoro, F.; Garagnani, P.; Franceschi, C.; Medaglini, D. Vaccination in the elderly: The challenge of immune changes with aging. Semin. Immunol. 2018, 40, 83–94. [Google Scholar] [CrossRef]
- McLaughlin, J.M.; McGinnis, J.J.; Tan, L.; Mercatante, A.; Fortuna, J. Estimated Human and Economic Burden of Four Major Adult Vaccine-Preventable Diseases in the United States, 2013. J. Prim. Prev. 2015, 36, 259–273. [Google Scholar] [CrossRef] [Green Version]
- de Gomensoro, E.; Del Giudice, G.; Doherty, T.M. Challenges in adult vaccination. Ann. Med. 2018, 50, 181–192. [Google Scholar] [CrossRef] [PubMed]
- European Commission. Special Eurobarometer 488: Europeans’ Attitudes towards Vaccination. 2019. Available online: https://dataeuropaeu/euodp/en/data/dataset/S2223_91_2_488_ENG (accessed on 6 June 2020).
- Andersen, R.; Davidson, P. Improving access to care in America: Individual and contextual indicators. In Changing the US Health Care System: Key Issues in Health Services Policy and Management; Wiley: Hoboken, NJ, USA, 2014; Volume 2007. [Google Scholar]
- Miyachi, T.; Takita, M.; Senoo, Y.; Yamamoto, K. Lower trust in national government links to no history of vaccination. Lancet 2020, 395, 31–32. [Google Scholar] [CrossRef] [Green Version]
- D’Ancona, F.; D’Amario, C.; Maraglino, F.; Rezza, G.; Iannazzo, S. The law on compulsory vaccination in Italy: An update 2 years after the introduction. Eurosurveillance 2019, 24, 1900371. [Google Scholar] [CrossRef] [Green Version]
- Schmitz, H.; Wübker, A. What determines influenza vaccination take-up of elderly Europeans? Health Econ. 2011, 20, 1281–1297. [Google Scholar] [CrossRef] [PubMed]
- Esping-Andersen, G. The Three Worlds of Welfare Capitalism; Polity Press: Cambridge, UK, 1990. [Google Scholar]
- Fenger, M. Welfare regimes in Central and Eastern Europe: Incorporating post-communist countries in a welfare regime typology. Contemp. Issues Ideas Soc. Sci. 2007, 3, 1–30. [Google Scholar]
- ECDC. Seasonal Influenza Vaccination and Antiviral Use in EU/EEA Member States. 2018. Available online: https://wwwecdceuropaeu/sites/default/files/documents/seasonal-influenza-antiviral-use-2018pdf (accessed on 29 October 2020).
- Loiacono, M.M.; Mahmud, S.M.; Chit, A.; van Aalst, R.; Kwong, J.C.; Mitsakakis, N.; Skinner, L.; Thommes, E.; Bricout, H.; Grootendorst, P. Patient and practice level factors associated with seasonal influenza vaccine uptake among at-risk adults in England, 2011 to 2016: An age-stratified retrospective cohort study. Vaccine X 2020, 4, 100054. [Google Scholar] [CrossRef] [PubMed]
- Sato, A.P.S.; Antunes, J.L.F.; Lima-Costa, M.F.F.; de Andrade, F.B. Influenza vaccine uptake among older adults in Brazil: Socioeconomic equality and the role of preventive policies and public services. J. Infect. Public Health 2020, 13, 211–215. [Google Scholar] [CrossRef]
- Burns, V.E.; Ring, C.; Carroll, D. Factors influencing influenza vaccination uptake in an elderly, community-based sample. Vaccine 2005, 23, 3604–3608. [Google Scholar] [CrossRef] [PubMed]
- Bertoldo, G.; Pesce, A.; Pepe, A.; Pelullo, C.P.; Di Giuseppe, G.; The Collaborative Working Group. Seasonal influenza: Knowledge, attitude and vaccine uptake among adults with chronic conditions in Italy. PLoS ONE 2019, 14, e0215978. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagata, J.M.; Hernández-Ramos, I.; Kurup, A.S.; Albrecht, D.; Vivas-Torrealba, C.; Franco-Paredes, C. Social determinants of health and seasonal influenza vaccination in adults ≥65 years: A systematic review of qualitative and quantitative data. BMC Public Health 2013, 13, 388. [Google Scholar] [CrossRef] [Green Version]
- Altpeter, E.; Wymann, M.N.; Richard, J.-L.; Mäusezahl-Feuz, M. Marked increase in measles vaccination coverage among young adults in Switzerland: A campaign or cohort effect? Int. J. Public Health 2018, 63, 589–599. [Google Scholar] [CrossRef] [Green Version]
- Rey, D.; Fressard, L.; Cortaredona, S.; Bocquier, A.; Gautier, A.; Peretti-Watel, P.; Verger, P. Vaccine hesitancy in the French population in 2016, and its association with vaccine uptake and perceived vaccine risk–benefit balance. Eurosurveillance 2018, 23, 17-00816. [Google Scholar] [CrossRef] [Green Version]
- Fall, E.; Izaute, M.; Chakroun-Baggioni, N. How can the health belief model and self-determination theory predict both influenza vaccination and vaccination intention ? A longitudinal study among university students. Psychol. Health 2018, 33, 746–764. [Google Scholar] [CrossRef]
- Alhalaseh, L.; Fayoumi, H.; Khalil, B. The Health Belief Model in predicting healthcare workers’ intention for influenza vaccine uptake in Jordan. Vaccine 2020, 38, 7372–7378. [Google Scholar] [CrossRef]
- Rosenstock, I.M. Historical Origins of the Health Belief Model. Health Educ. Monogr. 1974, 2, 328–335. [Google Scholar] [CrossRef]
- Janz, N.K.; Becker, M.H. The Health Belief Model: A Decade Later. Health Educ. Q. 1984, 11, 1–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bertoncello, C.; Ferro, A.; Fonzo, M.; Zanovello, S.; Napoletano, G.; Russo, F.; Baldo, V.; Cocchio, S. Socioeconomic Determinants in Vaccine Hesitancy and Vaccine Refusal in Italy. Vaccines 2020, 8, 276. [Google Scholar] [CrossRef]
- Mathieu, P.; Gautier, A.; Raude, J.; Goronflot, T.; Launay, T.; Debin, M.; Guerrisi, C.; Turbelin, C.; Hanslik, T.; Jestin, C.; et al. Population perception of mandatory childhood vaccination programme before its implementation, France, 2017. Eurosurveillance 2019, 24, 1900053. [Google Scholar] [CrossRef] [PubMed]
- Endrich, M.M.; Blank, P.R.; Szucs, T.D. Influenza vaccination uptake and socioeconomic determinants in 11 European countries. Vaccine 2009, 27, 4018–4024. [Google Scholar] [CrossRef]
- Fedson, D.S.; Hannoun, C.; Leese, J.; Sprenger, M.J.; Hampson, A.W.; Bro-Jørgensen, K.; Ahlbom, A.M.; Nøkleby, H.; Valle, M.; Olafsson, O.; et al. Influenza vaccination in 18 developed countries, 1980–1992. Vaccine 1995, 13, 623–627. [Google Scholar] [CrossRef]
- Kunze, U.; Groman, E.; Böhm, G.; Kunze, M. Influenza vaccination in Austria, 1982–2003. Wien. Med. Wochenschr. 2007, 157, 98–101. [Google Scholar] [CrossRef]
- McHugh, S.M.; Browne, J.; O’Neill, C.; Kearney, P.M. The influence of partial public reimbursement on vaccination uptake in the older population: A cross-sectional study. BMC Public Health 2015, 15, 83. [Google Scholar] [CrossRef] [Green Version]
- Blank, P.; Schwenkglenks, M.; Szucs, T.D. The impact of European vaccination policies on seasonal influenza vaccination coverage rates in the elderly. Hum. Vaccines Immunother. 2012, 8, 328–335. [Google Scholar] [CrossRef]
- Shemesh, A.A.; Rasooly, I.; Horowitz, P.; Lemberger, J.; Ben-Moshe, Y.; Kachal, J.; Danziger, J.; Clarfield, A.M.; Rosenberg, E. Health behaviors and their determinants in multiethnic, active Israeli seniors. Arch. Gerontol. Geriatr. 2008, 47, 63–77. [Google Scholar] [CrossRef]
- Farmanara, N.; Sherrard, L.; Dubé, È.; Gilbert, N.L. Determinants of non-vaccination against seasonal influenza in Canadian adults: Findings from the 2015–2016 Influenza Immunization Coverage Survey. Can. J. Public Health 2018, 109, 369–378. [Google Scholar] [CrossRef] [PubMed]
- Bödeker, B.; Remschmidt, C.; Schmich, P.; Wichmann, O. Why are older adults and individuals with underlying chronic diseases in Germany not vaccinated against flu? A population-based study. BMC Public Health 2015, 15, 618. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Age | Flu Vaccination | |||||||
|---|---|---|---|---|---|---|---|---|
| 55–59 | 60–64 | 65–69 | 70–74 | 75+ | not rec. | rec. | All | |
| Conservative/Corporatist | 0.53 | |||||||
| Austria | 0.43 | 0.43 | 0.44 | 0.48 | 0.61 | - | 0.48 | 0.48 |
| Belgium *** | 0.45 | 0.47 | 0.48 | 0.71 | 0.64 | 0.46 | 0.60 | 0.55 |
| Cyprus *** | 0.26 | 0.13 | 0.29 | 0.40 | 0.57 | 0.19 | 0.42 | 0.33 |
| France *** | 0.41 | 0.50 | 0.50 | 0.66 | 0.70 | 0.46 | 0.61 | 0.55 |
| Germany | 0.62 | 0.64 | 0.70 | 0.65 | 0.70 | 0.62 | 0.68 | 0.67 |
| Greece | 0.25 | 0.26 | 0.52 | 0.62 | 0.76 | 0.25 | 0.56 | 0.51 |
| Italy | 0.26 | 0.28 | 0.27 | 0.44 | 0.30 | 0.27 | 0.33 | 0.31 |
| Luxembourg | 0.61 | 0.54 | 0.72 | 0.59 | 0.69 | 0.56 | 0.67 | 0.63 |
| Malta | 0.34 | 0.51 | 0.60 | 0.55 | 0.70 | - | 0.54 | 0.54 |
| Netherlands ** | 0.46 | 0.58 | 0.59 | 0.54 | 0.57 | 0.46 | 0.57 | 0.55 |
| Portugal ** | 0.55 | 0.59 | 0.71 | 0.66 | 0.69 | 0.57 | 0.69 | 0.64 |
| Spain *** | 0.31 | 0.38 | 0.55 | 0.60 | 0.74 | 0.35 | 0.65 | 0.54 |
| Social-democrat/Nordic | 0.64 | |||||||
| Denmark ** | 0.44 | 0.48 | 0.57 | 0.59 | 0.59 | 0.46 | 0.58 | 0.54 |
| Finland | 0.70 | 0.64 | 0.70 | 0.78 | 0.68 | 0.67 | 0.71 | 0.69 |
| Sweden *** | 0.47 | 0.57 | 0.73 | 0.75 | 0.77 | 0.52 | 0.76 | 0.67 |
| Anglo-Saxon/Liberal | 0.57 | |||||||
| Ireland *** | 0.34 | 0.47 | 0.62 | 0.64 | 0.60 | 0.40 | 0.62 | 0.53 |
| United Kingdom *** | 0.31 | 0.43 | 0.60 | 0.67 | 0.74 | 0.37 | 0.69 | 0.57 |
| Post-communist | 0.23 | |||||||
| Bulgaria | 0.18 | 0.15 | 0.12 | 0.15 | 0.16 | 0.17 | 0.14 | 0.15 |
| Croatia | 0.29 | 0.20 | 0.28 | 0.42 | 0.40 | 0.24 | 0.35 | 0.31 |
| Czech Republic | 0.46 | 0.36 | 0.47 | 0.42 | 0.44 | 0.41 | 0.44 | 0.43 |
| Hungary ** | 0.14 | 0.21 | 0.20 | 0.29 | 0.38 | 0.14 | 0.26 | 0.23 |
| Poland | 0.20 | 0.13 | 0.16 | 0.18 | 0.15 | - | 0.16 | 0.16 |
| Romania ** | 0.08 | 0.22 | 0.20 | 0.24 | 0.30 | 0.15 | 0.24 | 0.20 |
| Slovakia | 0.38 | 0.33 | 0.35 | 0.39 | 0.40 | 0.38 | 0.37 | 0.37 |
| Slovenia * | 0.32 | 0.26 | 0.35 | 0.42 | 0.38 | 0.29 | 0.37 | 0.34 |
| Former USSR | 0.28 | |||||||
| Estonia | 0.36 | 0.21 | 0.29 | 0.25 | 0.30 | 0.28 | 0.29 | 0.29 |
| Latvia ** | 0.43 | 0.43 | 0.34 | 0.29 | - | 0.43 | 0.31 | 0.36 |
| Lithuania | 0.20 | 0.18 | 0.26 | 0.28 | 0.24 | 0.23 | - | 0.23 |
| Total | 0.38 | 0.40 | 0.46 | 0.54 | 0.60 | 0.39 | 0.51 | 0.48 |
| Mean | Std. Dev. | Min | Max | |
|---|---|---|---|---|
| Vaccinated | 0.462 | 0.499 | 0 | 1 |
| Predisposing factors (Andersen’s model of health care utilization) | ||||
| Medium vaccination knowledge | 0.448 | 0.497 | 0 | 1 |
| High vaccination knowledge | 0.432 | 0.495 | 0 | 1 |
| Female | 0.546 | 0.498 | 0 | 1 |
| Age | 67.968 | 8.469 | 55 | 98 |
| Single household | 0.328 | 0.470 | 0 | 1 |
| Welfare system | ||||
| post-communist | 0.252 | 0.434 | 0 | 1 |
| former USSR | 0.127 | 0.333 | 0 | 1 |
| Anglo-Saxon/Liberal | 0.072 | 0.258 | 0 | 1 |
| Conservative/Corporatist | 0.410 | 0.492 | 0 | 1 |
| Social-democrat/Nordic | 0.139 | 0.346 | 0 | 1 |
| Country of Residence | ||||
| Austria | 0.027 | 0.161 | 0 | 1 |
| Belgium | 0.037 | 0.188 | 0 | 1 |
| Bulgaria | 0.034 | 0.181 | 0 | 1 |
| Croatia | 0.024 | 0.153 | 0 | 1 |
| Cyprus | 0.020 | 0.139 | 0 | 1 |
| Czech Republic | 0.028 | 0.165 | 0 | 1 |
| Denmark | 0.042 | 0.201 | 0 | 1 |
| Estonia | 0.046 | 0.209 | 0 | 1 |
| Finland | 0.048 | 0.215 | 0 | 1 |
| France | 0.039 | 0.193 | 0 | 1 |
| Germany | 0.060 | 0.238 | 0 | 1 |
| Greece | 0.036 | 0.186 | 0 | 1 |
| Hungary | 0.034 | 0.180 | 0 | 1 |
| Ireland | 0.031 | 0.172 | 0 | 1 |
| Italy | 0.031 | 0.172 | 0 | 1 |
| Latvia | 0.037 | 0.188 | 0 | 1 |
| Lithuania | 0.045 | 0.207 | 0 | 1 |
| Luxembourg | 0.017 | 0.129 | 0 | 1 |
| Malta | 0.024 | 0.153 | 0 | 1 |
| Netherlands | 0.052 | 0.223 | 0 | 1 |
| Poland | 0.033 | 0.178 | 0 | 1 |
| Portugal | 0.036 | 0.186 | 0 | 1 |
| Romania | 0.026 | 0.160 | 0 | 1 |
| Slovakia | 0.036 | 0.187 | 0 | 1 |
| Slovenia | 0.038 | 0.191 | 0 | 1 |
| Spain | 0.033 | 0.178 | 0 | 1 |
| Sweden | 0.048 | 0.214 | 0 | 1 |
| United Kingdom | 0.041 | 0.198 | 0 | 1 |
| Enabling factors (Andersen’s model of health care utilization) | ||||
| Education | ||||
| Low (<age 15) | 0.249 | 0.432 | 0 | 1 |
| Medium (age 16–19) | 0.438 | 0.496 | 0 | 1 |
| High (age 20+) | 0.313 | 0.464 | 0 | 1 |
| Retired | 0.671 | 0.470 | 0 | 1 |
| Working | 0.265 | 0.442 | 0 | 1 |
| Financial hardship | 0.272 | 0.445 | 0 | 1 |
| Flu vaccination recommended but not covered | 0.124 | 0.329 | 0 | 1 |
| Need factor (Andersen’s model of health care utilization) | ||||
| Flu vaccination recommended | 0.667 | 0.471 | 0 | 1 |
| (1) | (2) | (3) | (4) | (5) | |
|---|---|---|---|---|---|
| Dependent variable: | LPM | LPM | LPM | LPM | Probit |
| vaccinated within the last 5 years | (robust std. err.) | (clustered std. err.) | (w/o BU, CZ) | (w/o AT, MT, PL) | (marginal effects) |
| Flu vacc. recommended | 0.059 *** | 0.059 ** | 0.056 *** | 0.057 *** | 0.050 *** |
| (0.016) | (0.024) | (0.017) | (0.018) | (0.016) | |
| Flu vacc. not covered | −0.097 *** | −0.097 *** | −0.082 *** | −0.097 *** | −0.086 *** |
| (0.025) | (0.027) | (0.031) | (0.025) | (0.030) | |
| Medium vacc. knowledge | 0.149 *** | 0.149 *** | 0.154 *** | 0.151 *** | 0.164 *** |
| (0.012) | (0.018) | (0.013) | (0.013) | (0.014) | |
| High vacc. knowledge | 0.258 *** | 0.258 *** | 0.263 *** | 0.264 *** | 0.269 *** |
| (0.013) | (0.020) | (0.013) | (0.013) | (0.014) | |
| Female | 0.002 | 0.002 | −0.001 | −0.001 | 0.004 |
| (0.008) | (0.010) | (0.009) | (0.009) | (0.008) | |
| Age | −0.200 *** | −0.200 ** | −0.190 *** | −0.187 ** | −0.197 *** |
| (0.071) | (0.074) | (0.073) | (0.074) | (0.071) | |
| Age2/100 | 0.290 *** | 0.290 ** | 0.278 *** | 0.273 *** | 0.286 *** |
| (0.099) | (0.105) | (0.102) | (0.103) | (0.099) | |
| Age3/10,000 | −0.135 *** | −0.135 ** | −0.130 *** | −0.128 *** | −0.134 *** |
| (0.046) | (0.049) | (0.047) | (0.047) | (0.046) | |
| Single household | −0.031 *** | −0.031 *** | −0.031 *** | −0.027 *** | −0.031 *** |
| (0.009) | (0.010) | (0.010) | (0.010) | (0.009) | |
| Low education | −0.024 ** | −0.024 | −0.028 ** | −0.028 ** | −0.024 ** |
| (0.011) | (0.015) | (0.012) | (0.012) | (0.011) | |
| High education | 0.031 ** | 0.031 * | 0.026 ** | 0.025 * | 0.031 ** |
| (0.013) | (0.018) | (0.013) | (0.013) | (0.013) | |
| Retired | 0.054 *** | 0.054 *** | 0.057 *** | 0.058 *** | 0.055 *** |
| (0.018) | (0.016) | (0.019) | (0.020) | (0.019) | |
| Working | 0.049 *** | 0.049 ** | 0.048 ** | 0.053 *** | 0.051 *** |
| (0.019) | (0.018) | (0.019) | (0.020) | (0.019) | |
| Financial hardship | −0.042 *** | −0.042 *** | −0.042 *** | −0.037 *** | −0.045 *** |
| (0.011) | (0.011) | (0.011) | (0.011) | (0.011) | |
| former USSR | −0.060 * | −0.060 *** | −0.061 * | −0.060 * | −0.070 ** |
| (0.032) | (0.013) | (0.032) | (0.032) | (0.035) | |
| Anglo-Saxon/Liberal | 0.198 *** | 0.198 *** | 0.196 *** | 0.198 *** | 0.180 *** |
| (0.033) | (0.010) | (0.033) | (0.033) | (0.033) | |
| Conservative/Corporatist | 0.217 *** | 0.217 *** | 0.216 *** | 0.217 *** | 0.202 *** |
| (0.034) | (0.007) | (0.034) | (0.034) | (0.033) | |
| Social-democrat/Nordic | 0.247 *** | 0.247 *** | 0.247 *** | 0.250 *** | 0.227 *** |
| (0.032) | (0.012) | (0.033) | (0.033) | (0.033) | |
| Constant | 4.545 *** | 4.545 ** | 4.300 ** | 4.226 ** | |
| (1.671) | (1.734) | (1.729) | (1.743) | ||
| Observations | 12,803 | 12,803 | 12,012 | 11,736 | 12,803 |
| R-squared | 0.157 | 0.157 | 0.151 | 0.153 |
| Mean | Std. Dev. | |
|---|---|---|
| QC11: A vaccination program establishes what vaccines a person should receive and at what time in life (like a calendar), as recommended by a health authority. At which level do you think vaccination programs should be coordinated? | ||
| At international level | 0.334 | 0.472 |
| At European level | 0.265 | 0.441 |
| At national level | 0.406 | 0.491 |
| At regional or local level | 0.165 | 0.371 |
| There should be no vaccination programs, it is a personal choice | 0.085 | 0.278 |
| - post-communist | 0.098 | 0.298 |
| - former USSR | 0.152 | 0.359 |
| - Anglo-Saxon | 0.031 | 0.175 |
| - Conservative/Corporatist | 0.092 | 0.289 |
| - Social-democrat/Nordic | 0.048 | 0.214 |
| Don’t know | 0.055 | 0.228 |
| QC12: In the past six months, have you seen, read or heard any information on vaccination in the media? | ||
| No | 0.341 | 0.474 |
| Yes, on TV | 0.556 | 0.497 |
| Yes, on the radio | 0.148 | 0.355 |
| Yes, in newspapers or magazines | 0.197 | 0.398 |
| Yes, on online social networks | 0.037 | 0.188 |
| Yes, on other Internet sites | 0.044 | 0.206 |
| Other (SPONTANEOUS) | 0.013 | 0.113 |
| Don’t know | 0.014 | 0.118 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Anastasiou, O.E.; Heger, D. Understanding the Influence of Individual and Systemic Factors on Vaccination Take-Up in European Citizens Aged 55 or Older. Vaccines 2021, 9, 169. https://doi.org/10.3390/vaccines9020169
Anastasiou OE, Heger D. Understanding the Influence of Individual and Systemic Factors on Vaccination Take-Up in European Citizens Aged 55 or Older. Vaccines. 2021; 9(2):169. https://doi.org/10.3390/vaccines9020169
Chicago/Turabian StyleAnastasiou, Olympia E., and Dörte Heger. 2021. "Understanding the Influence of Individual and Systemic Factors on Vaccination Take-Up in European Citizens Aged 55 or Older" Vaccines 9, no. 2: 169. https://doi.org/10.3390/vaccines9020169
APA StyleAnastasiou, O. E., & Heger, D. (2021). Understanding the Influence of Individual and Systemic Factors on Vaccination Take-Up in European Citizens Aged 55 or Older. Vaccines, 9(2), 169. https://doi.org/10.3390/vaccines9020169