
Who Should Get COVID-19 Vaccine First? A Survey to Evaluate Hospital Workers’ Opinion





Abstract
:1. Introduction
2. Materials and Methods
- Collecting the personal data of the participants (age; sex and working position) that could be relevant in terms of correlation with the other answers provided;
- Assessing the preferences of the participants with regard to the order of access to COVID-19 vaccination for different categories of the general population and of HCWs;
- Collecting the arguments given by the participants for assigning a priority in access to HCWs, law enforcement and essential services workers. The answers to some questions have been designed to be easily classified as arguments corresponding to a criterion of risk, utility or desert or to a melded criterion (utility, risk and desert) [10,11,12,13,14];
- Assessing participants’ opinion on mandatory vaccination for HCWs;
- Assessing the need for a consistent, transparent and detailed order of priority at a national level.
3. Results
3.1. Characteristics of the Participants
3.2. Priority Ranking
3.3. Prioritization Criteria
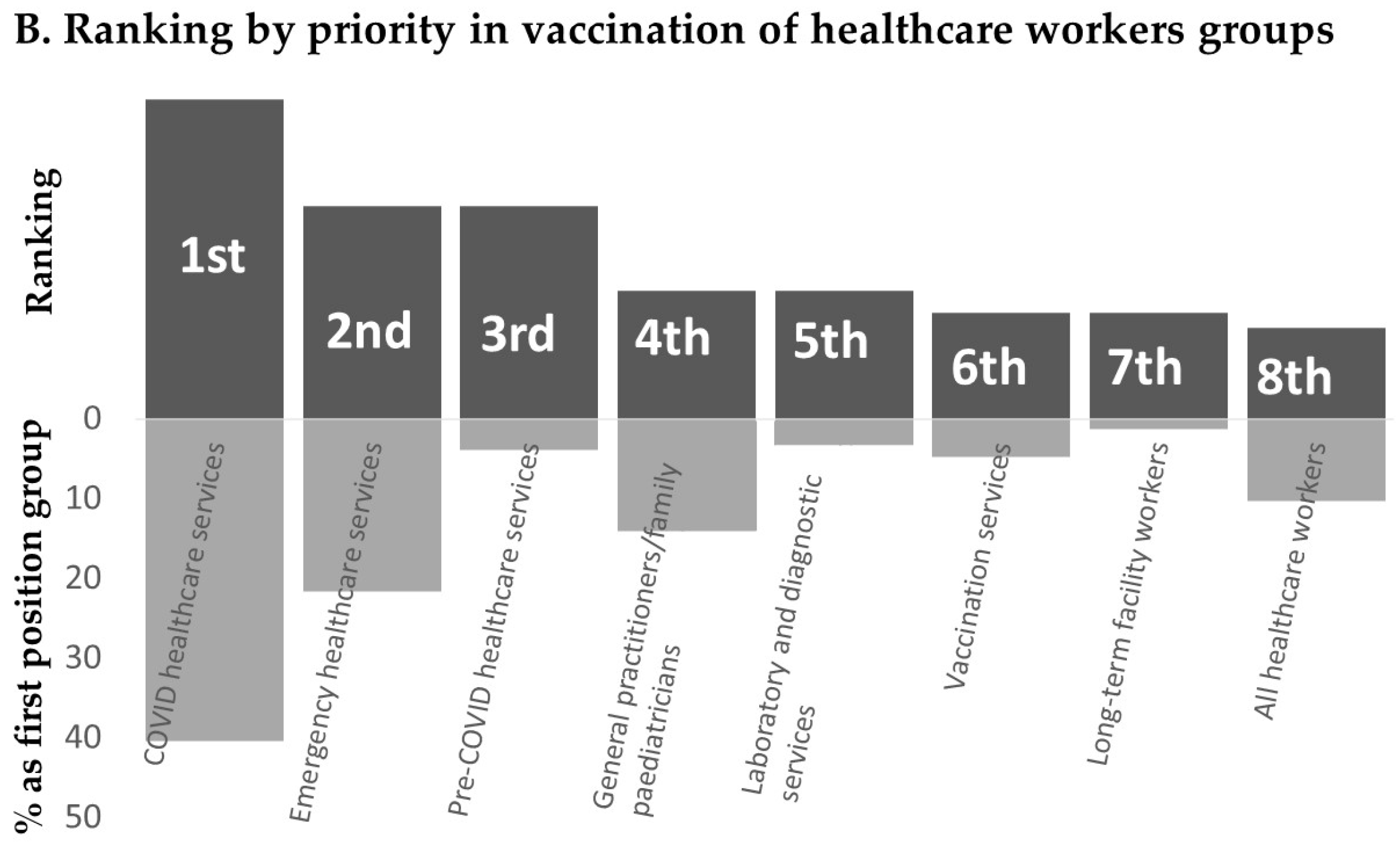
3.4. Vaccination Strategy Suggested for Healthcare Workers
4. Discussion
- HCWs are at increased risk of transmitting the infection to susceptible and vulnerable patients in health and social care settings (risk of transmitting infection to others);
- HCWs have a greater probability of being in settings where COVID-19 is circulating and exposed to a sufficient dose of the virus to become infected (risk of acquiring infection).
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ministero della Salute; Presidenza del Consiglio dei Ministri; Istituto Superiore di Sanità; Agenzia Nazionale per i Servizi Sanitari Regionali; Agenzia Italiana del Farmaco. Vaccinazione anti-SARS-CoV-2/COVID-19. Piano Strategico. Available online: http://www.salute.gov.it/imgs/C_17_pubblicazioni_2986_allegato.pdf (accessed on 20 January 2021).
- Department of Health and Social Care. UK COVID-19 Vaccines Delivery Plan. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/951928/uk-covid-19-vaccines-delivery-plan-final.pdf (accessed on 28 January 2021).
- The Centers for Disease Control and Prevention. The COVID-19 Vaccination Program Interim Operational Guidance for Jurisdictions Playbook. Available online: https://www.cdc.gov/vaccines/imz-managers/downloads/COVID-19-Vaccination-Program-Interim_Playbook.pdf (accessed on 28 January 2021).
- European Centre for Disease Prevention and Control. Overview of COVID-19 Vaccination Strategies and Vaccine Deployment Plans in the EU/EEA and the UK. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/Overview-of-EU_EEA-UK-vaccination-deployment-plans.pdf (accessed on 28 January 2021).
- Emanuel, E.J.; Persad, G.; Upshur, R.; Thome, B.; Parker, M.; Glickman, A.; Zhang, C.; Boyle, C.; Smith, M.; Phillips, J.P. Fair Allocation of Scarce Medical Resources in the Time of Covid-19. N. Engl. J. Med. 2020, 382, 2049–2055. [Google Scholar] [CrossRef]
- Center for Health Security. Interim Framework for COVID-19 Vaccine Allocation and Distribution in the United States. Available online: https://www.centerforhealthsecurity.org/our-work/pubs_archive/pubs-pdfs/2020/200819-vaccine-allocation.pdf (accessed on 20 January 2021).
- WHO SAGE Values Framework for the Allocation and Prioritization of COVID-19 Vaccination. Available online: WHO-2019-nCoV-SAGE_Framework-Allocation_and_prioritization-2020.1-eng.pdf (accessed on 20 January 2021).
- Ethical Challenges in the Middle Tier of Covid-19 Vaccine Allocation: Guidance for Organizational Decision-Making. Available online: https://www.thehastingscenter.org/wp-content/uploads/COVID-guidelines-supplement-vaccines-2.pdf (accessed on 20 January 2021).
- Anelli (Fnomceo): Preoccupa la Variabilità tra Regioni, Ancora Troppi i Medici non Vaccinati. Available online: http://www.quotidianosanita.it/studi-e-analisi/articolo.php?approfondimento_id=15723 (accessed on 28 January 2021).
- Konow, J. Which Is the Fairest One of All? A Positive Analysis of Justice Theories. J. Econ. Lit. 2003, 41, 1188–1239. [Google Scholar] [CrossRef] [Green Version]
- Cushman, F.; Young, L.; Hauder, M. The role of conscious reasoning and intuition in moral judgment: Testing three principles of harm. Psychol. Sci. 2006, 17, 1082–1089. [Google Scholar] [CrossRef] [PubMed]
- Faravelli, M. How context matters: A survey based experiment on distributive justice. J. Public Econ. 2007, 91, 1399–1422. [Google Scholar] [CrossRef] [Green Version]
- Fallucchi, F.; Faravelli, M.; Quercia, S. Fair allocation of scarce medical resources in the time of COVID-19: What do people think? J. Med. Ethics. 2021, 47, 3–6. [Google Scholar] [CrossRef] [PubMed]
- Arora, C.; Savulescu, J.; Maslen, H.; Selgelid, M.; Wilkinson, D. The Intensive Care Lifeboat: A survey of lay attitudes to rationing dilemmas in neonatal intensive care. BMC Med. Ethics. 2016, 17, 69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2002; Available online: https://www.R-project.org (accessed on 28 January 2021).
- Lazarus, J.V.; Ratzan, S.C.; Palayew, A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Kimball, S.; El-Mohandes, A. A global survey of potential acceptance of a COVID-19 vaccine. Nat. Med. 2020, 1–4. [Google Scholar] [CrossRef]
- Kreps, S.; Prasad, S.; Brownstein, J.S.; Hswen, Y.; Garibaldi, B.T.; Zhang, B.; Kriner, D.L. Factors Associated with US Adults’ Likelihood of Accepting COVID-19 Vaccination. JAMA Netw. Open 2020, 3, e2025594. [Google Scholar] [CrossRef] [PubMed]
- Rosenbaum, L. Facing Covid-19 in Italy—Ethics, Logistics, and Therapeutics on the Epidemic’s Front Line. N. Engl. J. Med. 2020, 382, 1873–1875. [Google Scholar] [CrossRef] [PubMed]
- Craxì, L.; Vergano, M. Beneficence and Equity: How the Covid-19 Pandemic Exposed Our Weaknesses in Italy. Available online: https://blogs.bmj.com/bmj/2020/05/22/beneficence-and-equity-how-the-covid-19-pandemic-exposed-our-weaknesses-in-italy/ (accessed on 28 January 2021).
- Craxì, L.; Vergano, M.; Savulescu, J.; Wilkinson, D. Rationing in a Pandemic: Lessons from Italy. Asian Bioeth. Rev. 2020, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Independent Report. Joint Committee on Vaccination and Immunisation: Advice on Priority Groups for COVID-19 Vaccination, 30 December 2020 (Updated 6 January 2021). Available online: https://www.gov.uk/government/publications/priority-groups-for-coronavirus-covid-19-vaccination-advice-from-the-jcvi-30-december-2020/joint-committee-on-vaccination-and-immunisation-advice-on-priority-groups-for-covid-19-vaccination-30-december-2020 (accessed on 20 January 2021).
- Dooling, K.; Marin, M.; Wallace, M.; McClung, N.; Chamberland, M.; Lee, G.M.; Talbot, H.K.; Romero, J.R.; Bell, B.P.; Oliver, S.E. The Advisory Committee on Immunization Practices’ Updated Interim Recommendation for Allocation of COVID-19 Vaccine—United States, December 2020. MMWR Morb. Mortal. Wkly. Rep. 2021, 69, 1657–1660. [Google Scholar] [CrossRef] [PubMed]
- National Academies of Sciences, Engineering, and Medicine; Health and Medicine Division; Board on Population Health and Public Health Practice; Board on Health Sciences Policy; Committee on Equitable Allocation of Vaccine for the Novel Coronavirus; Kahn, B.; Brown, L.; Foege, W. (Eds.) Framework for Equitable Allocation of COVID-19 Vaccine; National Academies Press (US): Washington, DC, USA, 2020. Available online: https://www.ncbi.nlm.nih.gov/books/NBK562672/ (accessed on 28 January 2021). [CrossRef]
- European Medicines Agency Comirnaty Assessment Report. Available online: https://www.ema.europa.eu/en/documents/assessment-report/comirnaty-epar-public-assessment-report_en.pdf (accessed on 28 January 2021).
- European Medicines Agency COVID-19 Moderna Vaccine EU Product Information. Available online: https://www.ema.europa.eu/en/documents/product-information/covid-19-vaccine-moderna-product-information_en.pdf (accessed on 28 January 2021).
- Lahner, E.; Dilaghi, E.; Prestigiacomo, C.; Alessio, G.; Marcellini, L.; Simmaco, M.; Santino, I.; Orsi, G.B.; Anibaldi, P.; Marcolongo, A.; et al. Prevalence of Sars-Cov-2 Infection in Health Workers (HWs) and Diagnostic Test Performance: The Experience of a Teaching Hospital in Central Italy. Int. J. Environ. Res. Public Health 2020, 17, 4417. [Google Scholar] [CrossRef] [PubMed]
- Bandyopadhyay, S.; Baticulon, R.E.; Kadhum, M.; Alser, M.; Ojuka, D.K.; Badereddin, Y.; Kamath, A.; Parepalli, S.A.; Brown, G.; Iharchane, S.; et al. Infection and mortality of healthcare workers worldwide from COVID-19: A systematic review. BMJ Glob. Health 2020, 5, e003097, PMCID:PMC7722361. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, L.H.; Drew, D.A.; Graham, M.S.; Joshi, A.D.; Guo, C.G.; Ma, W.; Mehta, R.S.; Warner, E.T.; Sikavi, D.R.; Lo, C.-H.; et al. Risk of COVID-19 among front-line health-care workers and the general community: A prospective cohort study. Lancet Pub Health 2020, 5, e475–e483. [Google Scholar] [CrossRef]
- CDC. Centers for Disease Control and Prevention. Scientific Evidence for Conditions that Increase Risk of Severe Illness. 2020. Available online: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/evidence-table.html (accessed on 28 January 2021).
- Kambhampati, A.K.; O’Halloran, A.C.; Whitaker, M.; Magill, S.S.; Chea, N.; Chai, S.J.; Kirley, P.D.; Herlihy, R.K.; Kawasaki, B.; Meek, J.; et al. COVID-19-Associated Hospitalizations Among Health Care Personnel-COVID-NET, 13 States, March 1–May 31, 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1576–1583. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | |
|---|---|
| Sex, n (%) | |
| - Male | 240 (51.6) |
| - Female | 225 (48.4) |
| Age, median (IQR) | 51 (41.0–59.0) |
| Age group, n (%) | |
| - 18 to 39 | 105 (22.6) |
| - 40 to 49 | 107 (23.0) |
| - 50 to 59 | 139 (29.9) |
| - 59 or more | 114 (24.5) |
| Working position, n (%) | |
| - Physician | 212 (45.6) |
| - Nurse | 120 (25.8) |
| - Healthcare technician | 41 (8.8) |
| - Administrative/others | 92 (19.8) |
| Preferred vaccination strategy for healthcare workers | |
| - Mandatory | 200 (43) |
| - Mandatory if enforced by the healthcare facility | 29 (6.2) |
| - Recommended | 191 (41.1) |
| - Fostered with financial incentives | 14 (3.0) |
| - Voluntary | 31 (6.7) |
| Transparency in management of COVID-19 vaccination priority strategy | |
| - Yes | 395 (85.0) |
| - No | 26 (6.0) |
| - I do not know | 44 (9.5) |
| COVID-19 vaccination priority for HCWs, n (%) | 444 (95.5) |
| COVID-19 vaccination priority for essential services, n (%) | 428 (92.0) |
| COVID-19 vaccination priority for law enforcement, n (%) | 428 (92.0) |
| No Priority, N (%) | Melded, N (%) | Risk, N (%) | Desert, N (%) | Utility, N (%) | p-Value | |
|---|---|---|---|---|---|---|
| Priority for healthcare workers | 21 (4.5) | 187 (40.3) | 115 (24.7) | 96 (20.6) | 46 (9.9) | <0.001 b <0.001 c |
| Priority for essential services | 37 (8.0) | 129 (27.7) | 72 (15.5) | 109 (23.4) | 118 (25.4) | <0.001 a <0.001 c |
| Priority for law enforcement | 37 (8.0) | 139 (29.9) | 69 (14.8) | 122 (26.2) | 98 (21.1) | <0.001 a <0.001 b |
| Priority for 2 or more groups | 28 (6.0) | 110 (23.6) | 46 (9.9) | 67 (14.4) | 66 (14.2) | - |
| Priority for 3 groups | 18 (3.9) | 100 (21.5) | 33 (7.1) | 59 (12.7) | 28 (6) | - |
| Melded N (%) | Risk N (%) | Desert N (%) | Utility N (%) | p-Value | |
|---|---|---|---|---|---|
| Priority for Healthcare Workers | |||||
| Sex | |||||
| - F | 101 (47.2) | 53 (24.8) | 41 (19.2) | 19 (8.9) | 0.19 |
| - M | 86 (37.4) | 62 (27) | 55 (23.9) | 27 (11.7) | |
| Age, median (IQR) | 51 (42–60) | 50 (41–59) | 51 (39–57) | 50 (40–59) | 0.73 |
| Healthcare profession | |||||
| - Physician | 89 (43.4) | 54 (26.3) | 39 (19) | 23 (11.2) | 0.42 |
| - Nurse | 45 (40.9) | 28 (25.5) | 29 (26.4) | 8 (7.3) | |
| - Healthcare technician | 13 (32.5) | 12 (30) | 7 (17.5) | 8 (20) | |
| - Administrative/others | 40 (44.9) | 21 (23.6) | 21 (23.6) | 7 (7.9) | |
| Priority for Essential Services | |||||
| Sex | |||||
| - F | 74 (35.7) | 36 (17.4) | 47 (22.7) | 50 (24.2) | 0.067 |
| - M | 55 (24.9) | 36 (16.3) | 62 (28.1) | 68 (30.8) | |
| Age, median (IQR) | 52 (43-61) | 49 (38-57) | 51 (41-58) | 50 (38-59) | 0.09 |
| Healthcare profession | |||||
| - Physician | 51 (25.5) | 34 (17) | 43 (21.5) | 72 (36) | 0.016 |
| - Nurse | 38 (35.8) | 21 (19.8) | 29 (27.4) | 18 (17) | |
| - Healthcare technician | 9 (24.3) | 6 (16.2) | 10 (27) | 12 (32.4) | |
| - Administrative/others | 31 (36.5) | 11 (12.9) | 27 (31.8) | 16 (18.8) | |
| Priority for Law Enforcement | |||||
| Sex | |||||
| - F | 78 (37.5) | 35 (16.8) | 55 (26.4) | 40 (19.2) | 0.10 |
| - M | 61 (27.7) | 34 (15.5) | 67 (30.5) | 58 (26.4) | |
| Age, median (IQR) | 52 (42–60) | 49 (40–58) | 51 (39–60) | 51 (42–59) | 0.27 |
| Healthcare profession | |||||
| - Physician | 53 (27.2) | 33 (16.9) | 55 (28.2) | 54 (27.7) | 0.043 |
| - Nurse | 45 (41.3) | 21 (19.3) | 29 (26.6) | 14 (12.8) | |
| - Healthcare technician | 8 (22.2) | 7 (19.4) | 11 (30.6) | 10 (27.8) | |
| - Administrative/others | 33 (37.5) | 8 (9.1) | 27 (30.7) | 20 (22.7) | |
| Mandatory (ref. Voluntary) | Other Strategies (ref. Voluntary) | |
|---|---|---|
| Sex | ||
| - M (ref. female) | 2.07 (0.96–4.44) | 0.91 (0.43–1.92) |
| Age, (per year increase) | 0.98 (0.94–1.01) | 0.97 (0.93–1) |
| Healthcare profession (ref. Administrative/others) | ||
| - Physician | 10.2 (2.7–39.1) a | 7.2 (1.9–27.3) a |
| - Nurse | 0.62 (0.25–1.53) | 0.83 (0.35–1.98) |
| - Healthcare technician | 4.45 (0.52–37.9) | 5.23 (0.63–43.4) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Craxì, L.; Casuccio, A.; Amodio, E.; Restivo, V. Who Should Get COVID-19 Vaccine First? A Survey to Evaluate Hospital Workers’ Opinion. Vaccines 2021, 9, 189. https://doi.org/10.3390/vaccines9030189
Craxì L, Casuccio A, Amodio E, Restivo V. Who Should Get COVID-19 Vaccine First? A Survey to Evaluate Hospital Workers’ Opinion. Vaccines. 2021; 9(3):189. https://doi.org/10.3390/vaccines9030189
Chicago/Turabian StyleCraxì, Lucia, Alessandra Casuccio, Emanuele Amodio, and Vincenzo Restivo. 2021. "Who Should Get COVID-19 Vaccine First? A Survey to Evaluate Hospital Workers’ Opinion" Vaccines 9, no. 3: 189. https://doi.org/10.3390/vaccines9030189
APA StyleCraxì, L., Casuccio, A., Amodio, E., & Restivo, V. (2021). Who Should Get COVID-19 Vaccine First? A Survey to Evaluate Hospital Workers’ Opinion. Vaccines, 9(3), 189. https://doi.org/10.3390/vaccines9030189