
Knowledge, Attitudes and Perceptions of COVID-19 Vaccination among Healthcare Workers of an Inner-City Hospital in New York

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Settings and Survey Participants
2.2. Survey Description
2.3. Model Fit and Structural Equation Modeling
2.4. Regression
2.5. Univariate Analysis
3. Results
3.1. Characteristics of the Study Cohort
3.2. Univariate and Descriptive Analysis
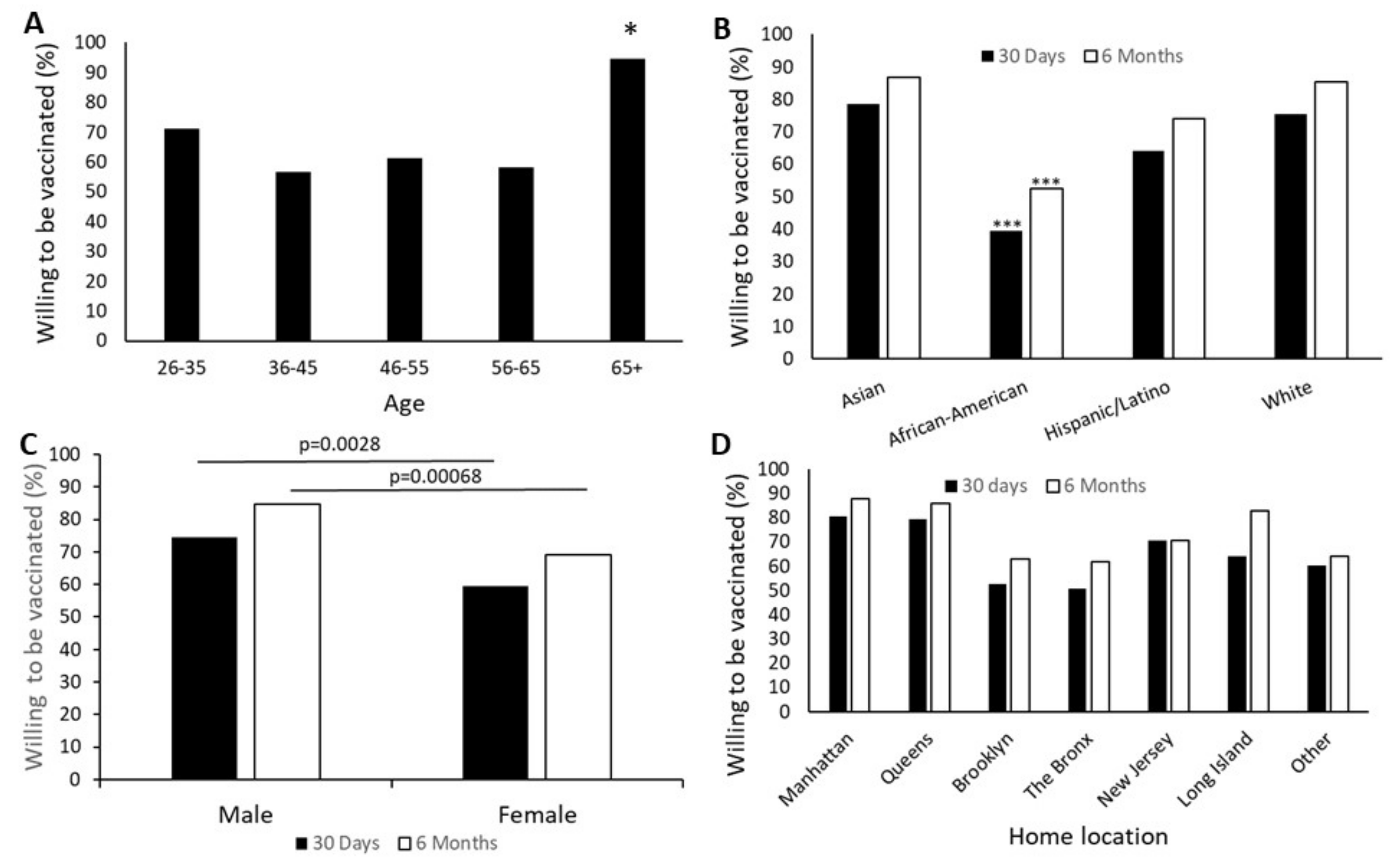
3.2.1. Demographic Factors
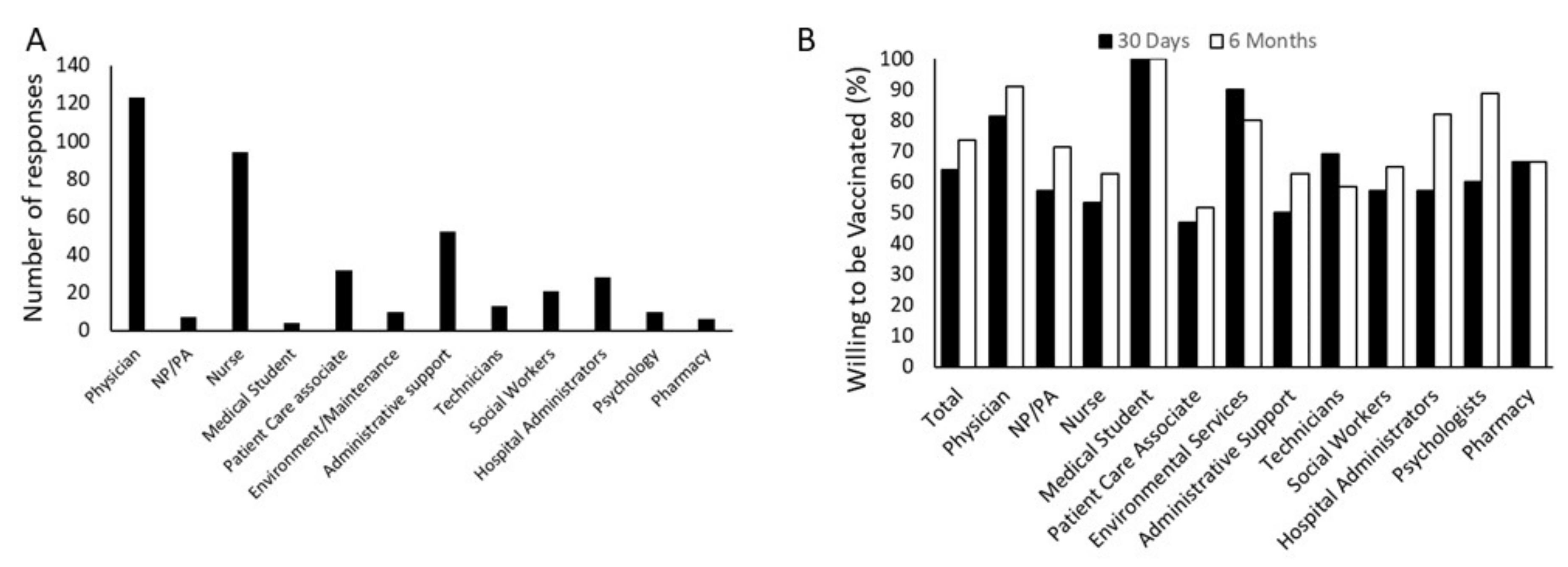
3.2.2. Participant Role and Attitude towards COVID-19 Vaccination
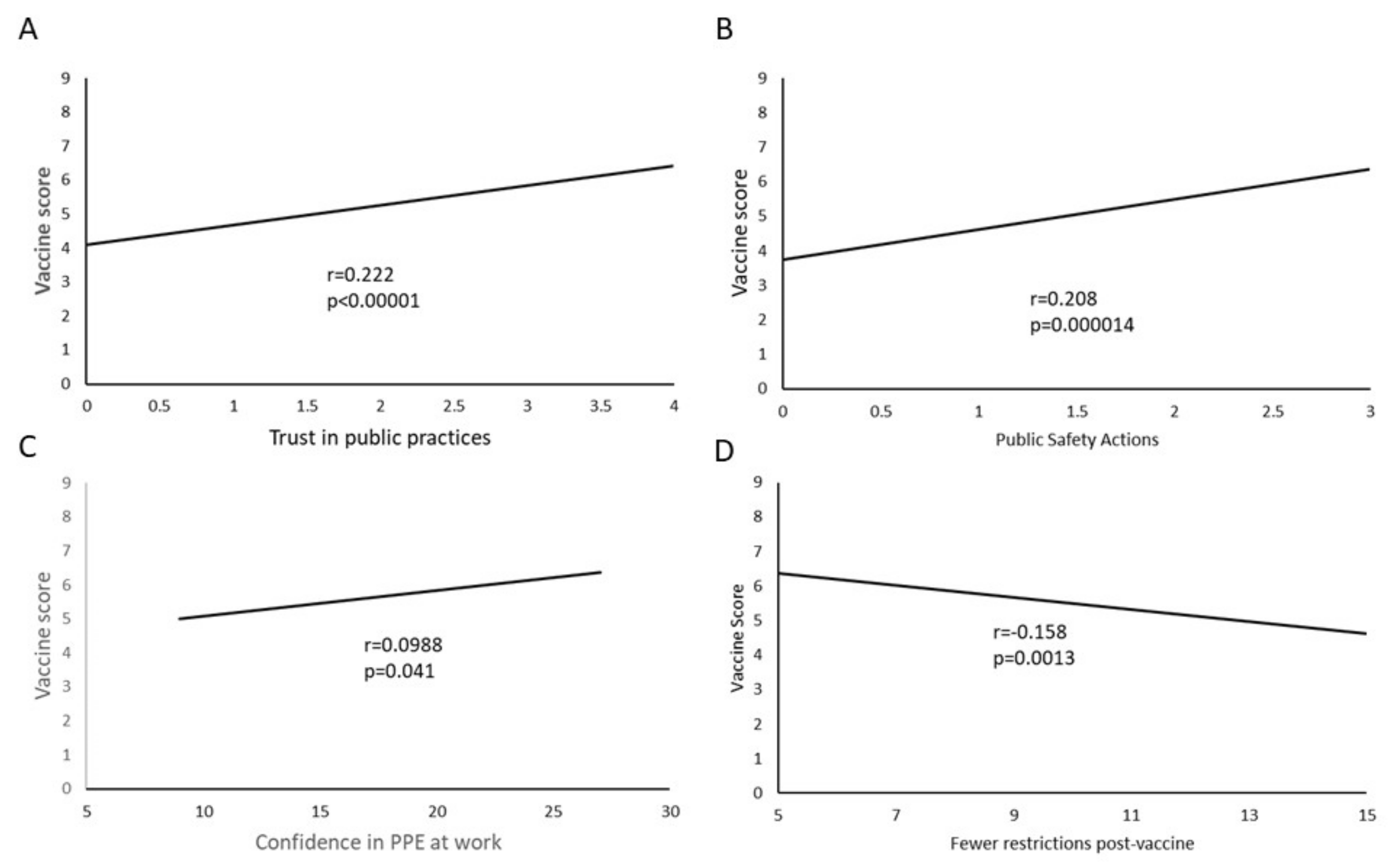
3.2.3. PPE, Preventive Practices and Attitude towards COVID-19 Vaccination
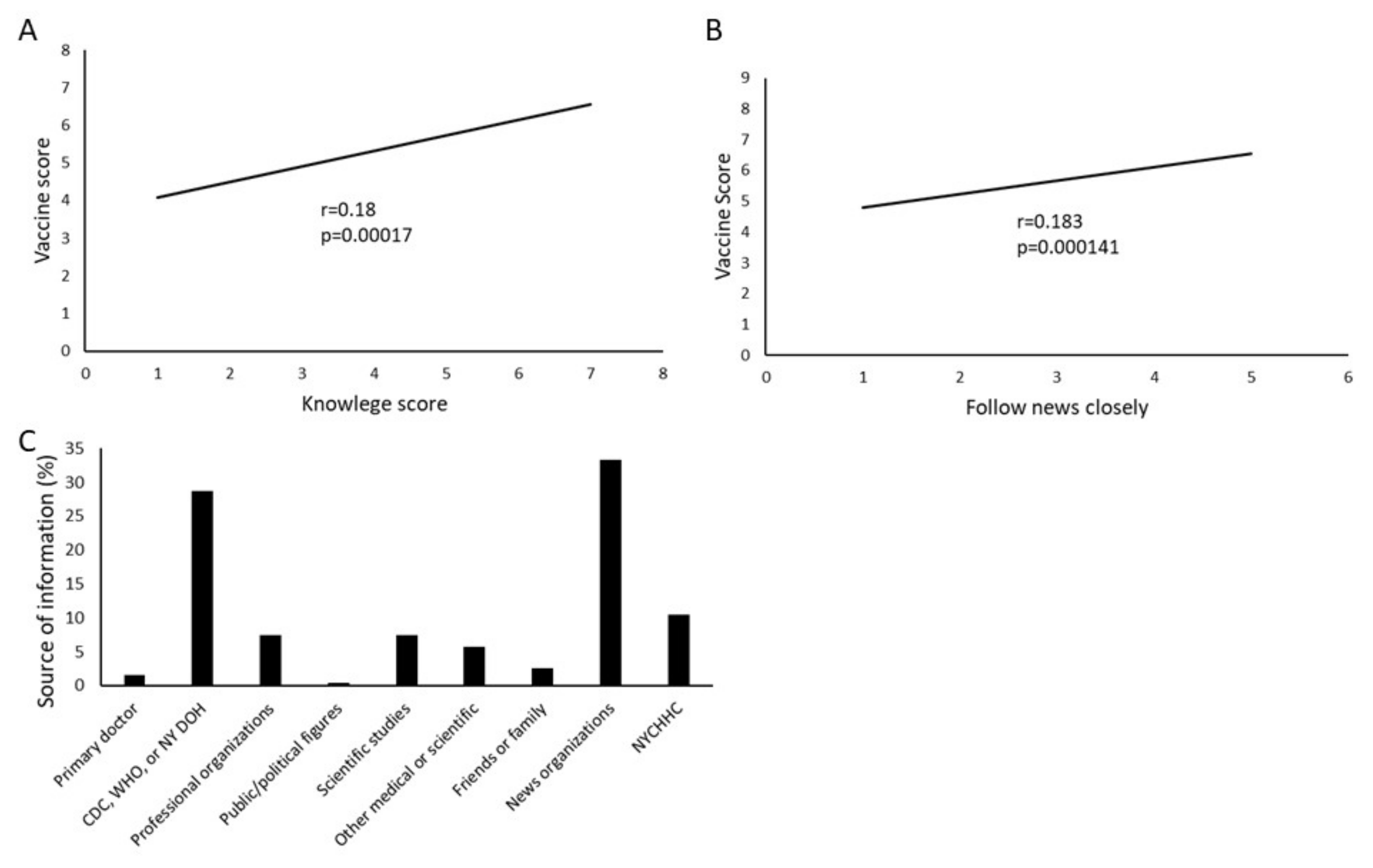
3.2.4. Information and Attitude towards COVID-19 Vaccination
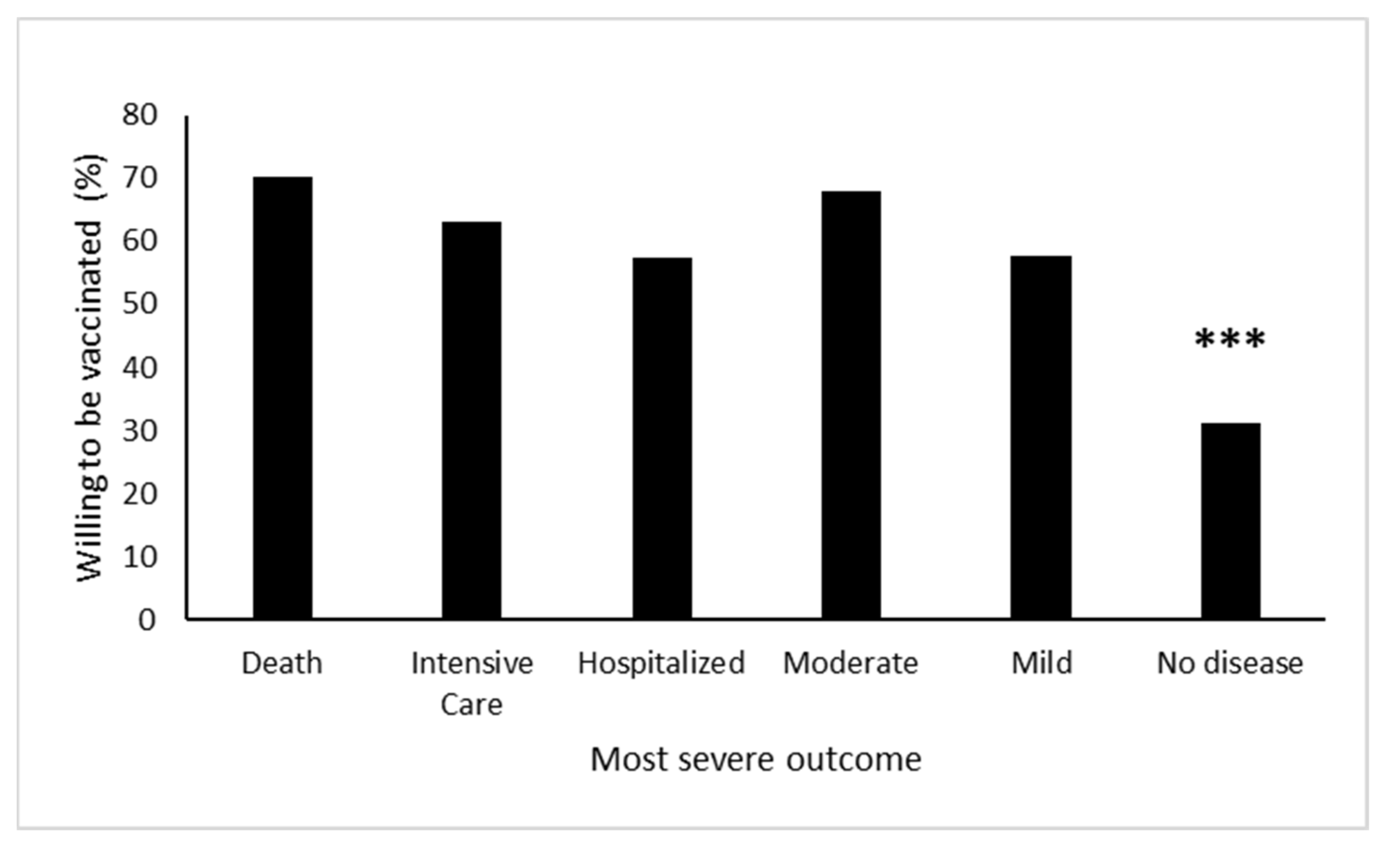
3.2.5. Personal Experience and Attitude towards COVID-19 Vaccination
3.3. Modeling and Multivariate Analysis
3.3.1. Statistical Results of CFA and SEM
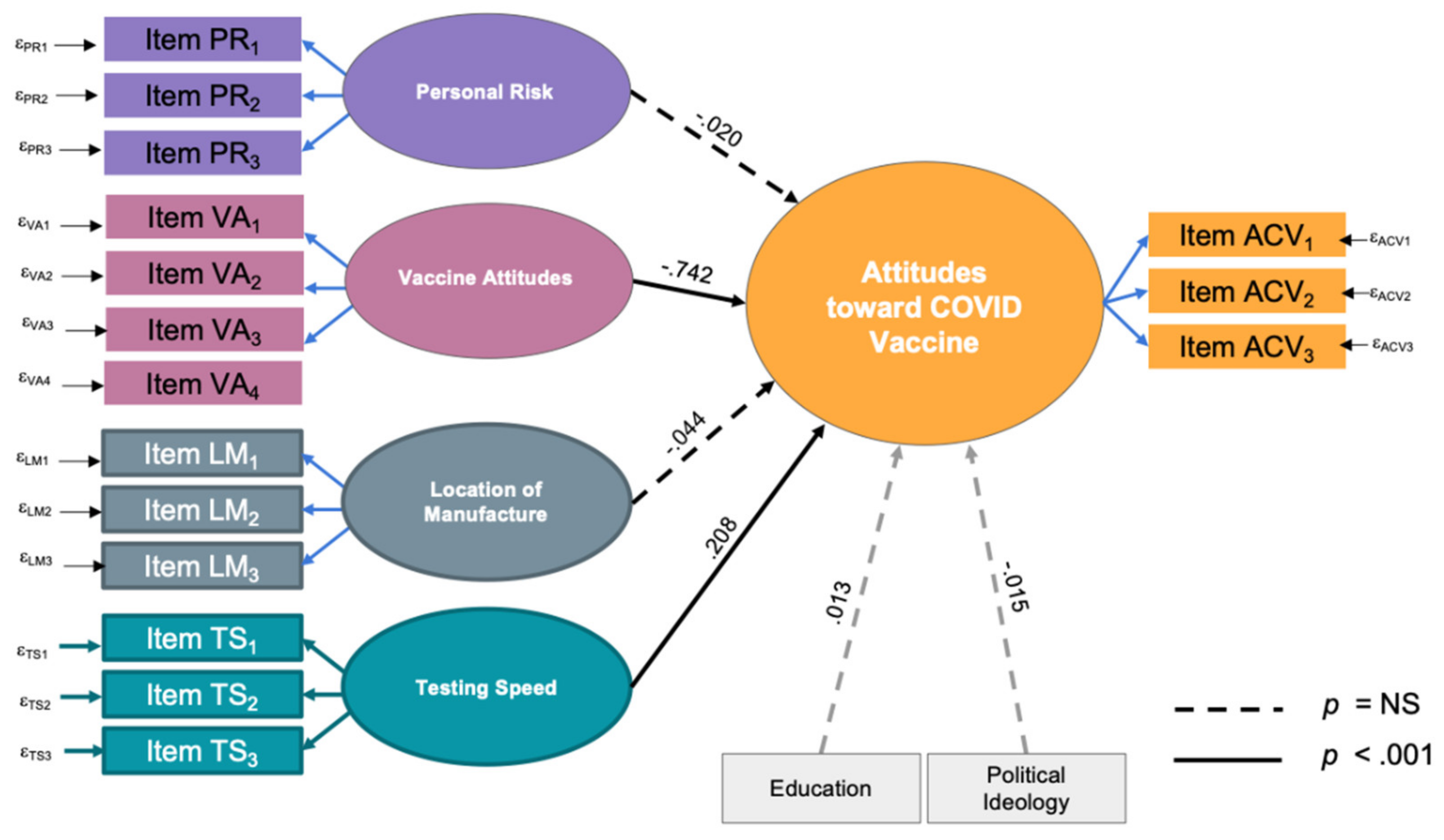
3.3.2. Structural Equation Model (SEM)
3.3.3. Regression Analysis
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- COVID-19 Map—Johns Hopkins Coronavirus Resource Center. Available online: https://coronavirus.jhu.edu/map.html (accessed on 27 February 2021).
- WHO. Draft Landscape and Tracker of COVID-19 Candidate Vaccines. Available online: https://www.who.int/publications/m/item/draft-landscape-of-covid-19-candidate-vaccines (accessed on 27 February 2021).
- Ten Threats to Global Health in 2019. Available online: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019 (accessed on 3 March 2021).
- Johnson, D.K.; Mello, E.J.; Walker, T.D.; Hood, S.J.; Jensen, J.L.; Poole, B.D. Combating Vaccine Hesitancy with Vaccine-Preventable Disease Familiarization: An Interview and Curriculum Intervention for College Students. Vaccines 2019, 7, 39. [Google Scholar] [CrossRef]
- Funk, C.; Tyson, A. Intent to Get a COVID-19 Vaccine Rises to 60% as Confidence in Research and Development Process Increases. Pew Research Center. 3 December 2020. Available online: https://www.pewresearch.org/science/2020/12/03/intent-to-get-a-covid-19-vaccine-rises-to-60-as-confidence-in-research-and-development-process-increases/ (accessed on 16 May 2021).
- Brenan, M. Willingness to Get COVID-19 Vaccine Ticks Up to 63% in U.S. Gallup. 8 December 2020. Available online: https://news.gallup.com/poll/327425/willingness-covid-vaccine-ticks.aspx (accessed on 27 February 2021).
- Szilagyi, P.G.; Thomas, K.; Shah, M.D.; Vizueta, N.; Cui, Y.; Vangala, S.; Kapteyn, A. National Trends in the US Public’s Likelihood of Getting a COVID-19 Vaccine—April 1 to December 8, 2020. JAMA J. Am. Med. Assoc. 2021, 325, 396–398. [Google Scholar] [CrossRef] [PubMed]
- Omer, S.B.; Yildirim, I.; Forman, H.P. Herd Immunity and Implications for SARS-CoV-2 Control. J. Am. Med. Assoc. 2020, 324, 2095–2096. [Google Scholar] [CrossRef] [PubMed]
- Fontanet, A.; Cauchemez, S. COVID-19 herd immunity: Where are we? Nat. Rev. Immunol. 2020, 20, 583–584. [Google Scholar] [CrossRef]
- Kreps, S.; Prasad, S.; Brownstein, J.S.; Hswen, Y.; Garibaldi, B.T.; Zhang, B.; Kriner, D.L. Factors Associated with US Adults’ Likelihood of Accepting COVID-19 Vaccination. J. Am. Med. Assoc. Netw. Open 2020, 3, e2025594. [Google Scholar] [CrossRef] [PubMed]
- Detoc, M.; Bruel, S.; Frappe, P.; Tardy, B.; Botelho-Nevers, E.; Gagneux-Brunon, A. Intention to participate in a COVID-19 vaccine clinical trial and to get vaccinated against COVID-19 in France during the pandemic. Vaccine 2020, 38, 7002–7006. [Google Scholar] [CrossRef] [PubMed]
- Williams, L.; Gallant, A.J.; Rasmussen, S.; Nicholls, L.A.B.; Cogan, N.; Deakin, K.; Young, D.; Flowers, P. Towards intervention development to increase the uptake of COVID-19 vaccination among those at high risk: Outlining evidence-based and theoretically informed future intervention content. Br. J. Health Psychol. 2020, 25, 1039–1054. [Google Scholar] [CrossRef]
- Pogue, K.; Jensen, J.L.; Stancil, C.K.; Ferguson, D.G.; Hughes, S.J.; Mello, E.J.; Burgess, R.; Berges, B.K.; Quaye, A.; Poole, B.D. Influences on Attitudes Regarding Potential COVID-19 Vaccination in the United States. Vaccines 2020, 8, 582. [Google Scholar] [CrossRef]
- Wang, K.; Wong, E.L.Y.; Ho, K.F.; Cheung, A.W.L.; Chan, E.Y.Y.; Yeoh, E.K.; Wong, S.Y.S. Intention of nurses to accept coronavirus disease 2019 vaccination and change of intention to accept seasonal influenza vaccination during the coronavirus disease 2019 pandemic: A cross-sectional survey. Vaccine 2020, 38, 7049–7056. [Google Scholar] [CrossRef] [PubMed]
- Shekhar, R.; Sheikh, A.B.; Upadhyay, S.; Singh, M.; Kottewar, S.; Mir, H.; Barrett, E.; Pal, S. COVID-19 Vaccine Acceptance among Health Care Workers in the United States. Vaccines 2021, 9, 119. [Google Scholar] [CrossRef]
- Fisher, K.A.; Bloomstone, S.J.; Walder, J.; Crawford, S.; Fouayzi, H.; Mazor, K.M. Attitudes Toward a Potential SARS-CoV-2 Vaccine: A Survey of U.S. Adults. Ann. Intern. Med. 2020, 173, 964–973. [Google Scholar] [CrossRef]
- NYC Health. COVID-19: Latest Data. Available online: https://www1.nyc.gov/site/doh/covid/covid-19-data.page#epicurve (accessed on 1 March 2021).
- COVID-19 Vaccine. Hospital Worker Vaccinations. Available online: https://covid19vaccine.health.ny.gov/hospital-worker-vaccinations (accessed on 2 March 2021).
- Dubé, E.; Laberge, C.; Guay, M.; Bramadat, P.; Roy, R.; Bettinger, J. Vaccine hesitancy: An overview. Hum. Vaccines Immunother. 2013, 9, 1763–1773. [Google Scholar] [CrossRef] [PubMed]
- Dubé, E.; Gagnon, D.; Nickels, E.; Jeram, S.; Schuster, M. Mapping vaccine hesitancy-Country-specific characteristics of a global phenomenon. Vaccine 2014, 32, 6649–6654. [Google Scholar] [CrossRef]
- Schwarzinger, M.; Watson, V.; Arwidson, P.; Alla, F.; Luchini, S. COVID-19 vaccine hesitancy in a representative working-age population in France: A survey experiment based on vaccine characteristics. Lancet Public Health 2021, 6, e210–e221. [Google Scholar] [CrossRef]
- U.S. Bureau of Labor Statistics. In Employed Persons by Detailed Industry and Age. Available online: https://www.bls.gov/cps/cpsaat18b.htm (accessed on 10 May 2021).
- Murphy, J.; Vallières, F.; Bentall, R.P.; Shevlin, M.; McBride, O.; Hartman, T.K.; McKay, R.; Bennett, K.; Mason, L.; Gibson-Miller, J.; et al. Psychological characteristics associated with COVID-19 vaccine hesitancy and resistance in Ireland and the United Kingdom. Nat. Commun. 2021, 12, 1–15. [Google Scholar] [CrossRef]
- Adhikari, E.H.; Spong, C.Y. COVID-19 Vaccination in Pregnant and Lactating Women. J. Am. Med. Assoc. 2021, 325, 1039–1040. [Google Scholar] [CrossRef] [PubMed]
- Closson, T. Stark Disparities in Vaccine Rollout by ZIP Code. The New York Times. 17 February 2021. Available online: https://www.nytimes.com/2021/02/17/nyregion/vaccine-rollout-neighborhood-numbers.html (accessed on 16 May 2021).
- McClendon, S.; Proctor, K. New Survey of 13K U.S. Nurses: Findings Indicate Urgent Need to Educate Nurses about COVID-19 Vaccines. Available online: https://www.nursingworld.org/news/news-releases/2020/new-survey-of-13k-u.s.-nurses-findings-indicate-urgent-need-to-educate-nurses-about-covid-19-vaccines/ (accessed on 27 February 2021).
- Kwok, K.O.; Li, K.K.; Wei, W.I.; Tang, A.; Wong, S.Y.S.; Lee, S.S. Influenza vaccine uptake, COVID-19 vaccination intention and vaccine hesitancy among nurses: A survey. Int. J. Nurs. Stud. 2021, 114, 103854. [Google Scholar] [CrossRef] [PubMed]
- Hogan, C.; Atta, M.; Anderson, P.; Stead, T.; Solomon, M.; Banerjee, P.; Sleigh, B.; Shivdat, J.; McAdams, A.W.; Ganti, L. Knowledge and attitudes of us adults regarding COVID-19. Int. J. Emerg. Med. 2020, 13, 53. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Data | Number | Percentage of Total Responses |
|---|---|---|
| Age (n = 428) | ||
| 18–25 | 4 | 0.93% |
| 26–35 | 125 | 29.21% |
| 36–45 | 106 | 24.77% |
| 46–55 | 88 | 20.56% |
| 55–65 | 86 | 20.09% |
| >65 | 19 | 4.44% |
| Gender (n = 428) | ||
| Male | 137 | 32.01% |
| Female | 279 | 65.19% |
| Prefer to self-describe | 3 | 0.70% |
| Prefer not to answer | 9 | 2.10% |
| Race (n = 428) | ||
| White | 102 | 23.83% |
| Latinx | 123 | 28.74% |
| African American | 82 | 19.16% |
| Asian | 84 | 19.63% |
| Native American | 3 | 0.70% |
| Native Hawaiian or Pacific Islander | 2 | 0.47% |
| Prefer not to answer | 17 | 3.97% |
| Other | 15 | 3.50% |
| Marital Status (n = 428) | ||
| Single | 176 | 41.12% |
| Married | 220 | 51.40% |
| Divorced | 26 | 6.07% |
| Widow/widower | 6 | 1.40% |
| Number of Children (n = 428) | ||
| 0 | 171 | 39.95% |
| 1 | 73 | 17.06% |
| 2 | 112 | 26.17% |
| more than 2 | 72 | 16.82% |
| Level of Education (n = 428) | ||
| Not finished high school | 2 | 0.47% |
| Finished high school | 15 | 3.50% |
| Some college | 49 | 11.45% |
| Associates degree | 31 | 7.24% |
| Bachelor’s degree | 113 | 26.40% |
| Master’s degree | 74 | 17.29% |
| Doctoral degree | 144 | 33.64% |
| Primary Role at Work (n = 428) | ||
| Physician | 122 | 28.50% |
| Nurses | 94 | 21.96% |
| Administrative/clerical staff | 65 | 15.19% |
| Patient Care associates | 27 | 6.31% |
| Social worker | 20 | 4.67% |
| Other | 100 | 23.36% |
| Location of Work (n = 672) | ||
| Administrative offices | 75 | 11.16% |
| Ambulatory care | 135 | 20.09% |
| Emergency Department | 130 | 19.35% |
| Medical and Surgical Inpatient Units | 127 | 18.90% |
| Intensive Care Units | 84 | 12.50% |
| Operating Rooms | 31 | 4.61% |
| Other | 90 | 13.39% |
| Residence Borough (n = 428) | ||
| The Bronx | 150 | 35.05% |
| Manhattan | 82 | 19.16% |
| Queens | 49 | 11.45% |
| Brooklyn | 19 | 4.44% |
| Staten Island | 1 | 0.23% |
| Long Island NY | 14 | 3.27% |
| Connecticut | 2 | 0.47% |
| New Jersey | 41 | 9.58% |
| Prefer not to answer | 2 | 0.47% |
| Other | 68 | 15.89% |
| RMSEA | CFI | TLI | SRMR | Chi-Square Test | |||
|---|---|---|---|---|---|---|---|
| χ2 | df | p-Value | |||||
| Full Measurement Model | 0.067 | 0.913 | 0.882 | 0.076 | 2086.86 | 120 | <0.001 |
| Latent Variable and Associated Items (Factor Loading Indicated a) | |||||||
| Personal Risk | |||||||
| How much of a problem is COVID-19 in America? b (−0.56) | |||||||
| Based on your own health, age and risk factors, what do you believe to be your risk level were you to get COVID-19? b (0.30) | |||||||
| Based on your overall experience with COVID-19 in both a professional and personal capacity, how serious would you say COVID-19? b (0.67) | |||||||
| Vaccine Attitudes | |||||||
| I am current on the vaccinations recommended by my primary care physician.c (0.39) | |||||||
| How important is it for you to get the flu vaccine every year? b (0.66) | |||||||
| Vaccines are important for the prevention of serious diseases.c (0.89) | |||||||
| My children are current on recommended vaccines (or, if I don’t have children, I would keep my children current on recommended vaccines).c (0.62) | |||||||
| Location of Manufacture | |||||||
| Development of a vaccine outside of the United States would reduce my likelihood of being vaccinated. c (1.18) | |||||||
| Development of a vaccine in China or Russia would reduce my likelihood of being vaccinated c (0.90) | |||||||
| Development of a vaccine in the United Kingdom would reduce my likelihood of being vaccinated c (1.30) | |||||||
| Testing Speed | |||||||
| I worry that the rushed pace of testing for the new COVID-19 vaccine will fail to detect potential side effects or dangers c (0.60) | |||||||
| I would accept a COVID-19 vaccine with full FDA approval but not one with an emergency use authorization c (0.51) | |||||||
| I would NOT accept a COVID-19 vaccine until the completion of its clinical trial and publication of results in a peer-reviewed journal such as JAMA, NEJM or the Lancet.c (0.81) | |||||||
| Likelihood of getting the COVID-19 vaccine | |||||||
| I am likely to get the COVID vaccine d (0.82) | |||||||
| Other people around me being vaccinated against COVID-19 will be helpful in controlling the pandemic c (−0.85) | |||||||
| A vaccine is important to end the COVID-19 pandemic c (−0.94) | |||||||
| Parameter | B | SE B | 95% Wald CI | Wald Chi-Square | df | p-Value | |
|---|---|---|---|---|---|---|---|
| LL | UL | ||||||
| (Intercept) | 3.17 | 0.104 | 2.97 | 3.38 | 924.28 | 1 | <0.001 |
| Vaccine Attitudes | −0.091 | 0.006 | −0.103 | −0.08 | 202.37 | 1 | <0.001 |
| Testing Speed | 0.014 | 0.005 | 0.004 | 0.024 | 7.30 | 1 | 0.007 |
| Personal Risk | −0.017 | 0.008 | −0.034 | −0.001 | 4.57 | 1 | 0.033 |
| Location of Manufacture | −0.007 | 0.005 | −0.017 | 0.003 | 1.95 | 1 | 0.163 |
| Education | 0.005 | 0.011 | −0.016 | 0.025 | .21 | 1 | 0.646 |
| Political Ideology | 0.013 | 0.014 | −0.014 | 0.040 | .92 | 1 | 0.338 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ciardi, F.; Menon, V.; Jensen, J.L.; Shariff, M.A.; Pillai, A.; Venugopal, U.; Kasubhai, M.; Dimitrov, V.; Kanna, B.; Poole, B.D. Knowledge, Attitudes and Perceptions of COVID-19 Vaccination among Healthcare Workers of an Inner-City Hospital in New York. Vaccines 2021, 9, 516. https://doi.org/10.3390/vaccines9050516
Ciardi F, Menon V, Jensen JL, Shariff MA, Pillai A, Venugopal U, Kasubhai M, Dimitrov V, Kanna B, Poole BD. Knowledge, Attitudes and Perceptions of COVID-19 Vaccination among Healthcare Workers of an Inner-City Hospital in New York. Vaccines. 2021; 9(5):516. https://doi.org/10.3390/vaccines9050516
Chicago/Turabian StyleCiardi, Federico, Vidya Menon, Jamie L. Jensen, Masood A Shariff, Anjana Pillai, Usha Venugopal, Moiz Kasubhai, Vihren Dimitrov, Balavenkatesh Kanna, and Brian D. Poole. 2021. "Knowledge, Attitudes and Perceptions of COVID-19 Vaccination among Healthcare Workers of an Inner-City Hospital in New York" Vaccines 9, no. 5: 516. https://doi.org/10.3390/vaccines9050516
APA StyleCiardi, F., Menon, V., Jensen, J. L., Shariff, M. A., Pillai, A., Venugopal, U., Kasubhai, M., Dimitrov, V., Kanna, B., & Poole, B. D. (2021). Knowledge, Attitudes and Perceptions of COVID-19 Vaccination among Healthcare Workers of an Inner-City Hospital in New York. Vaccines, 9(5), 516. https://doi.org/10.3390/vaccines9050516