
The Costs of Introducing the Hepatitis B Birth Dose Vaccine into the National Immunization Programme in Senegal (NéoVac Study)

 , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Data Collection
2.3. Costs Analysis
2.3.1. Overview of the Costing Analysis
2.3.2. Costing Methods to Estimate Costs per Study Site
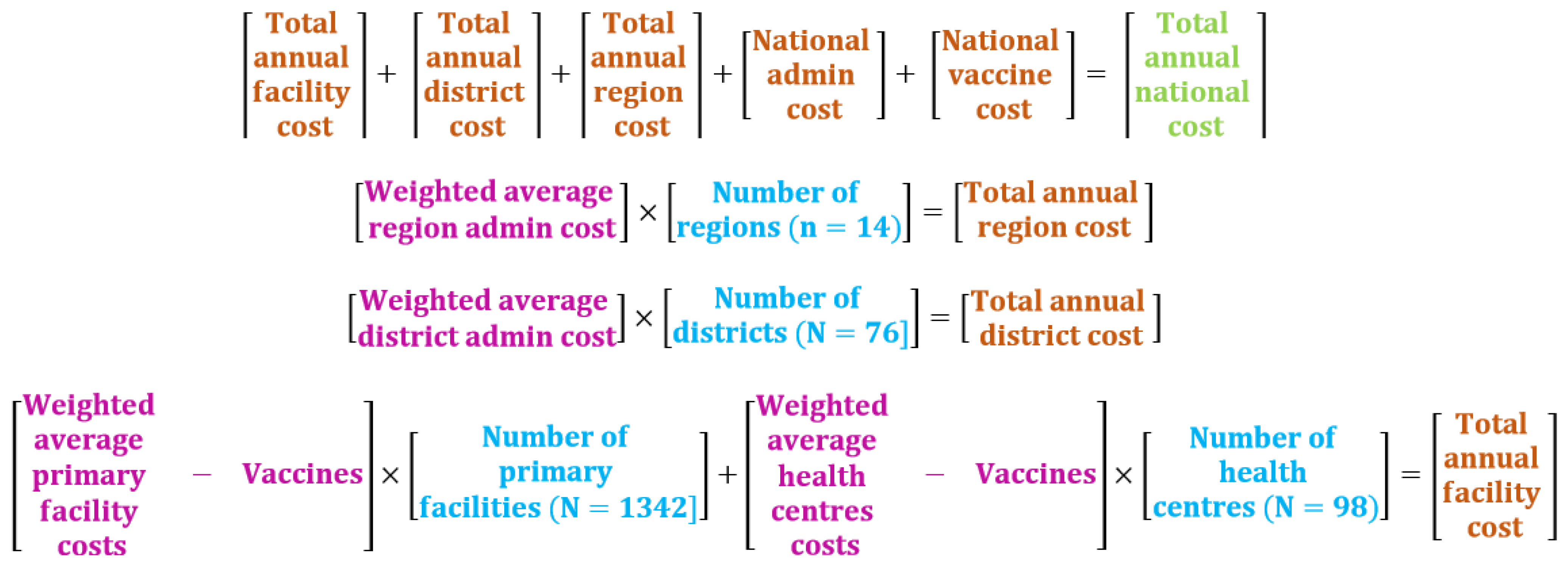
2.3.3. Costs Aggregation to Estimate the Total Annual Costs at the Country Level
2.3.4. Estimation of the Cost per Vaccinated Newborn
3. Results
3.1. Introduction and Implementation of HepB-BD in Senegal
3.1.1. Pre-Introduction Activities
3.1.2. HepB-BD Vaccination Strategy
3.2. Estimations of Weighted Average Costs per Activity
3.3. Costs of HepB-BD Implementation at the Country Level
3.4. Cost per HepB-BD Vaccinated Newborn
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Activities | Regional Health Office | District Health Office | First-Level Health Facilities | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Health Posts | Health Centers | |||||||||
| 2015 (n = 5) | 2016 (n = 5) | 2017 (n = 5) | 2015 (n = 15) | 2016 (n = 15) | 2017 (n = 15) | 2016 (n = 66) | 2017 (n = 69) | 2016 (n = 9) | 2017 (n = 9) | |
| Initial training | 662.3 | 0.0 | 0.0 | 812.4 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 |
| Social mobilization | 0.0 | 438.8 | 0.0 | 0.0 | 380.0 | 4.3 | 1.1 | 0.9 | 6.7 | 16.0 |
| Vaccine administration (excluding the costs of vaccines and safety supplies) | 0.0 | 0.0 | 0.0 | 0.0 | 53.4 | 79.1 | 202.6 | 259.1 | 675.7 | 869.2 |
| Storage | 0.0 | 230.0 | 227.8 | 0.0 | 61.9 | 74.4 | 21.9 | 27.3 | 54.4 | 105.5 |
| Supervision | 0.0 | 1051.9 | 1070.3 | 0.0 | 1110.1 | 1327.6 | 9.4 | 13.9 | 0.0 | 0.0 |
| Distribution | 0.0 | 168.9 | 168.9 | 0.0 | 24.1 | 29.7 | 3.7 | 5.1 | 2.8 | 4.0 |
| Management | 0.0 | 578.0 | 619.6 | 0.0 | 757.8 | 878.7 | 4.0 | 6.8 | 3.0 | 20.3 |
| Waste management | 0.0 | 6.7 | 6.7 | 0.0 | 1.6 | 1.9 | 0.0 | 0.0 | 0.0 | 0.0 |
| Total | 662.3 | 2474.3 | 2093.3 | 812.4 | 2388.8 | 2395.7 | 242.8 | 313.1 | 742.6 | 1015.1 |
References
- World Health Organization. Global Hepatitis Programme Global Hepatitis Report, 2017; World Health Organization: Geneva, Switzerland, 2017; ISBN 978-92-4-156545-5. [Google Scholar]
- Polaris Observatory Collaborators Global Prevalence, Treatment, and Prevention of Hepatitis B Virus Infection in 2016: A Modelling Study. Lancet Gastroenterol. Hepatol. 2018, 3, 383–403. [CrossRef]
- World Health Organization. Global Health Sector Strategies for Viral Hepatitis 2016–2021; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Edmunds, W.J.; Medley, G.F.; Nokes, D.J.; Hall, A.J.; Whittle, H.C. The Influence of Age on the Development of the Hepatitis B Carrier State. Proc. Biol. Sci. 1993, 253, 197–201. [Google Scholar] [CrossRef] [PubMed]
- Shimakawa, Y.; Yan, H.-J.; Tsuchiya, N.; Bottomley, C.; Hall, A.J. Association of Early Age at Establishment of Chronic Hepatitis B Infection with Persistent Viral Replication, Liver Cirrhosis and Hepatocellular Carcinoma: A Systematic Review. PLoS ONE 2013, 8, e69430. [Google Scholar] [CrossRef] [PubMed]
- Shimakawa, Y.; Lemoine, M.; Bottomley, C.; Njai, H.F.; Ndow, G.; Jatta, A.; Tamba, S.; Bojang, L.; Taal, M.; Nyan, O.; et al. Birth Order and Risk of Hepatocellular Carcinoma in Chronic Carriers of Hepatitis B Virus: A Case-Control Study in The Gambia. Liver Int. 2015, 35, 2318–2326. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Hepatitis Programme Guidelines for the Prevention, Care, and Treatment of Persons with Chronic Hepatitis B Infection; World Health Organization: Geneva, Switzerland, 2015; ISBN 978-92-4-154905-9. [Google Scholar]
- Spearman, C.W.; Afihene, M.; Ally, R.; Apica, B.; Awuku, Y.; Cunha, L.; Dusheiko, G.; Gogela, N.; Kassianides, C.; Kew, M.; et al. Hepatitis B in Sub-Saharan Africa: Strategies to Achieve the 2030 Elimination Targets. Lancet Gastroenterol. Hepatol. 2017, 2, 900–909. [Google Scholar] [CrossRef] [Green Version]
- Peck, M.; Gacic-Dobo, M.; Diallo, M.S.; Nedelec, Y.; Sodha, S.V.; Wallace, A.S. Global Routine Vaccination Coverage, 2018. Mmwr. Morb. Mortal. Wkly. Rep. 2019, 68, 937–942. [Google Scholar] [CrossRef] [PubMed]
- Miyahara, R.; Jasseh, M.; Gomez, P.; Shimakawa, Y.; Greenwood, B.; Keita, K.; Ceesay, S.; D’Alessandro, U.; Roca, A. Barriers to Timely Administration of Birth Dose Vaccines in The Gambia, West Africa. Vaccine 2016, 34, 3335–3341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bassoum, O.; Kimura, M.; Tal Dia, A.; Lemoine, M.; Shimakawa, Y. Coverage and Timeliness of Birth Dose Vaccination in Sub-Saharan Africa: A Systematic Review and Meta-Analysis. Vaccines 2020, 8, 301. [Google Scholar] [CrossRef] [PubMed]
- Moturi, E.; Tevi-Benissan, C.; Hagan, J.E.; Shendale, S.; Mayenga, D.; Murokora, D.; Patel, M.; Hennessey, K.; Mihigo, R. Implementing a Birth Dose of Hepatitis B Vaccine in Africa: Findings from Assessments in 5 Countries. J. Immunol. Sci. 2018, 5, 31–40. [Google Scholar] [CrossRef] [Green Version]
- World Bank Data World Bank. Available online: https://data.worldbank.org/country/SN (accessed on 9 April 2021).
- World Bank Data World Bank. Available online: https://data.worldbank.org/indicator/SH.XPD.CHEX.PC.CD?locations=SN (accessed on 9 April 2021).
- WHO. UNICEF Senegal: WHO and UNICEF Estimates of Immunization Coverage: 2019 Revision; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Brenzel, L. Common Approach for the Costing and Financing Analyses of Routine Immunization and New Vaccine Introduction Costs (NUVI). Working paper. 2013. Available online: http://static1.squarespace.com/static/556deb8ee4b08a534b8360e7/t/55970258e4b03cf942da51ac/1435959896232/WEBSITE_Common+Approach.pdf (accessed on 17 May 2021).
- World Health Organization. Guidelines for Estimating Costs of Introducing New Vaccines into the National Immunization System 2002; World Health Organization: Geneva, Switzerland, 2002. [Google Scholar]
- Data World Bank Official Exchange Rate. Available online: https://databank.worldbank.org/reports.aspx?source=2&series=PA.NUS.FCRF&country= (accessed on 16 April 2021).
- Ministry of Health of Senegal. Rapport Annuel Sur Les Performances En Matière de Vaccination Pour La Période Comprise Entre Janvier et Décembre 2017. Internal report: Unpublished. 2017. [Google Scholar]
- Gosset, A.; Diallo, M.Y.; Betsem, E.; Schaeffer, L.; Meda, N.; Vray, M.; Sombie, R.; Shimakawa, Y.; Boyer, S. Cost-Effectiveness of Adding a Birth Dose of Hepatitis B Vaccine in Burkina Faso, West Africa. Vaccine 2021. under review. [Google Scholar]
- Brenzel, L.; Young, D.; Walker, D.G. Costs and Financing of Routine Immunization: Approach and Selected Findings of a Multi-Country Study (EPIC). Vaccine 2015, 33 (Suppl. 1), A13–A20. [Google Scholar] [CrossRef] [PubMed]
- GAVI the Vaccine Alliance. Gavi Board Starts Framing Alliance’s Approach to 2021–2025 Period. Available online: https://www.gavi.org/news/media-room/gavi-board-starts-framing-alliances-approach-2021-2025-period (accessed on 17 April 2021).
- Okenwa, U.J.; Dairo, M.D.; Uba, B.; Ajumobi, O. Maternal Reasons for Non-Receipt of Valid Hepatitis B Birth Dose among Mother-Infant Pairs Attending Routine Immunization Clinics, South-East, Nigeria. Vaccine 2019, 37, 6894–6899. [Google Scholar] [CrossRef] [PubMed]
- UNICEF Percentage of Deliveries in a Health Facility. Available online: https://data.unicef.org/topic/maternal-health/delivery-care/ (accessed on 25 February 2021).
- Xeuatvongsa, A.; Datta, S.S.; Moturi, E.; Wannemuehler, K.; Philakong, P.; Vongxay, V.; Vilayvone, V.; Patel, M.K. Improving Hepatitis B Birth Dose in Rural Lao People’s Democratic Republic through the Use of Mobile Phones to Facilitate Communication. Vaccine 2016, 34, 5777–5784. [Google Scholar] [CrossRef] [PubMed]
- Creati, M.; Saleh, A.; Ruff, T.A.; Stewart, T.; Otto, B.; Sutanto, A.; Clements, C.J. Implementing the Birth Dose of Hepatitis B Vaccine in Rural Indonesia. Vaccine 2007, 25, 5985–5993. [Google Scholar] [CrossRef] [PubMed]
- Seaman, C.P.; Morgan, C.; Howell, J.; Xiao, Y.; Spearman, C.W.; Sonderup, M.; Lesi, O.; Andersson, M.I.; Hellard, M.E.; Scott, N. Use of Controlled Temperature Chain and Compact Prefilled Auto-Disable Devices to Reach 2030 Hepatitis B Birth Dose Vaccination Targets in LMICs: A Modelling and Cost-Optimisation Study. Lancet Glob. Health 2020, 8, e931–e941. [Google Scholar] [CrossRef]
- Klingler, C.; Thoumi, A.I.; Mrithinjayam, V.S. Cost-Effectiveness Analysis of an Additional Birth Dose of Hepatitis B Vaccine to Prevent Perinatal Transmission in a Medical Setting in Mozambique. Vaccine 2012, 31, 252–259. [Google Scholar] [CrossRef] [PubMed]

| Activity | Description | Activity Related to HepB-BD Introduction/Implementation | Input Line Items | Level of the Health System | Comments |
|---|---|---|---|---|---|
| 1. Pre-introduction | Activities carried out to prepare for HepB-BD introduction, including developing the national plan for the introduction, developing training tools needed, updating and printing immunization-related materials (child immunization cards, registers, EPI supervision tools, etc.) | Yes | Recurrent costs: time of salaried labor, per diems, fuel for transportation, stationary, room rental, printing (immunization cards and other immunization related materials) | National | Costs mainly incurred in 2015 and considered as investment costs (annualized over 5 years) Financial costs do not include labor time as no additional staff were hired |
| 2. Initial training | Initial training and supervision specifically for HepB-BD introduction | Yes | Recurrent costs: staff (provision of services), per diems and transport allowances, fuel for transportation, stationary, room rental | National, regional and district | Costs incurred in 2015 and considered as investment costs (annualized over 2 years) |
| 3. Social mobilization | Social mobilization associated with HepB-BD introduction (during the introduction period and after): development of radio publicity spots and communication tools, broadcast of radio spots and TV shows, organization of special events | Yes | Recurrent: staff (provision of services), per diems and transport allowances, fuel for transportation, room rental for special events, radio time and TV shows to broadcast messages, stationery, printing communication tools (flyers, posters, etc.) | All (national, regional, district and primary care facility) | Costs incurred mainly in 2016 (a small number of costs are reported in 2017) |
| 4. Vaccine administration | Routine facility-based administration of HepB-BD vaccine and outreach vaccination | Yes | Recurrent costs: time taken for a salaried worker to administer the HepB-BD vaccine (6 min per infant), vaccines (number of doses administered), vaccine injection and safety supplies (syringes and safety boxes, etc.), per diems and fuel for outreach vaccination Capital costs: vehicles | National level for vaccines and supplies costs District and first-level health facility levels for labor time related to vaccine administration | Costs incurred in 2016 and 2017 Financial costs do not include labor time as no additional staff were hired |
| 5. Vaccine storage | Cold chain storage of vaccines and storage of injection and safety supplies | No (EPI costs allocated to the HepB-BD based on the share of the HepB-BD volume relative to the total volume for all current vaccines | Recurrent costs: cold chain maintenance and cold chain energy (electricity, gas, ice packs, etc.) Capital costs: cold chain equipment | All (national, regional, district and first-level health facility) | Costs incurred in 2016 and 2017 Financial costs only include annualized costs of new cold chain equipment purchased in 2015 and 2016 |
| 6. Vaccine distribution | Transportation of vaccines, injection and safety supplies | No (EPI costs allocated to the HepB-BD based on the share of the HepB-BD volume relative to the total volume for all current vaccines | Recurrent costs: per diems, fuel for transportation of vaccines and supplies, vehicle maintenance Capital costs: vehicles | All (national, regional, district and first-level health facility) | Costs incurred in 2016 and 2017 Financial costs only include the annualized costs of new vehicles purchased in 2015 and 2016 |
| 7. Supervision, monitoring and surveillance | Routine supervision of immunization activities, monitoring and evaluation of immunization data (including surveillance of post-vaccination events) | No: Costs–excluding salary costs-allocated to HepB-BD based on the share of the number of doses for the HepB-BD relative to the total number of vaccines doses in the EPI Salary costs allocated based on time spent | Recurrent costs: time of salaried labor, per diems and transport allowances, fuel for transportation, vehicle maintenance Capital costs: vehicles | All (national, regional, district and first-level health facility) | Costs incurred in 2016 and 2017 No financial costs |
| 8. Management | Planning, budgeting and managing the immunization program (including continuing training) | No: costs-excluding salary costs-allocated to the HepB-BD based on the share of the number of doses for the HepB-BD relative to the total number of vaccines doses in the EPI Salary costs allocated based on time spent | Recurrent costs: time of salaried labor, per diems and transport allowances, fuel for transportation Capital costs: office equipment (computers, printers, etc.) | All (national, regional, district and first-level health facility) | Costs incurred in 2016 and 2017 No financial costs |
| 9. Waste management | Management of HepB-BD vaccine-related waste | No (costs allocated to the HepB-BD based on the share of the HepB-BD volume relative to the total volume for all current vaccines | Recurrent costs: incinerator fuel Capital costs: incinerator | Regional and district levels | Costs incurred in 2016 and 2017 No financial costs |
| Main Data | Description | Source |
|---|---|---|
| Target population (live births) | 541,529 in 2016; 543,126 in 2017 | World Bank |
| HepB-BD coverage rates | 58% in 2016; 72% in 2017 | WHO/UNICEF |
| Total number of HepB-BD administered doses | 379,999 in 2016; 473,643 in 2017 | National database (DVD-MT) used for the management of vaccine stocks in the EPI |
| Total number of HepB-BD administered doses within 24 h after birth | 314,084 in 2016; 391,488 in 2017 | WHO/UNICEF |
| Vaccine type | 10-dose vials (Hepavax-Gene®, Berna Biotech Korea Corp., Incheon, Korea) | Ministry of Health of Senegal |
| Vaccine wastage rates | 5% | Ministry of Health of Senegal |
| Vaccine unit price | USD 0.20 | UNICEF |
| Vaccine administration | Within 24 h after birth | Ministry of Health of Senegal |
| Structures where HepB-BD is delivered |
| Ministry of Health of Senegal |
| Personnel in charge of HepB-BD administration | Nurses | |
| Time needed to administer HepB-BD | 6 min | NéoVac study |
| Discount rate for capital costs | 3% | WHO |
| National | Regional Health Offices | District Health Offices | Health Posts | Health Centers | Total | % per Activity | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2015 | 2016 | 2017 | 2015 | 2016 | 2017 | 2015 | 2016 | 2017 | 2016 | 2017 | 2016 | 2017 | 2015 | 2016 | 2017 | 2015 | 2016 | 2017 | ||
| Pre-introduction | Capital | 0 | 0 | 0 | ||||||||||||||||
| Running | 65,855 | 0 | 0 | |||||||||||||||||
| Total | 65,855 | 65,855 | 0 | 0 | 45.9% | 0.0% | 0.0% | |||||||||||||
| Initial training | Capital | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |||||
| Running | 0 | 0 | 9272 | 0 | 0 | 68,238 | 0 | 0 | 9 | 0 | 0 | 0 | 77,510 | 9 | 0 | |||||
| Total | 0 | 0 | 9272 | 0 | 0 | 68,238 | 0 | 0 | 9 | 0 | 0 | 0 | 77,510 | 9 | 0 | 54.1% | 0.0% | 0.0% | ||
| Social mobilization | Capital | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | ||||||
| Running | 20,653 | 0 | 6143 | 0 | 31,923 | 357 | 1470 | 1189 | 688 | 1645 | 0 | 60,877 | 3191 | |||||||
| Total | 20,653 | 0 | 6143 | 0 | 31,923 | 357 | 1470 | 1189 | 688 | 1645 | 0 | 60,877 | 3191 | 8.0% | 0.4% | |||||
| Vaccine administration | Capital | 0 | 0 | 0 | 0 | 0 | 2118 | 2907 | 17,326 | 23,496 | 0 | 0 | 0 | 19,444 | 26,402 | |||||
| Running | 0 | 98,835 | 123,191 | 0 | 0 | 2367 | 3741 | 245,579 | 313,652 | 69,372 | 89,238 | 0 | 416,152 | 529,821 | ||||||
| Total | 0 | 98,835 | 123,191 | 0 | 0 | 4485 | 6647 | 262,904 | 337,147 | 69,372 | 89,238 | 0 | 435,596 | 556,224 | 57.4% | 63.6% | ||||
| Storage | Capital | 404 | 405 | 2292 | 2292 | 3863 | 4699 | 15,908 | 19,761 | 5351 | 10,520 | 0 | 27,820 | 37,677 | ||||||
| Running | 2651 | 2652 | 928 | 897 | 1333 | 1550 | 12,466 | 15,824 | 232 | 313 | 0 | 17,610 | 21,236 | |||||||
| Total | 3055 | 3057 | 3220 | 3189 | 5197 | 6249 | 28,374 | 35,585 | 5583 | 10,833 | 0 | 45,430 | 58,913 | 6.0% | 6.7% | |||||
| Distribution | Capital | 634 | 635 | 2355 | 2355 | 1984 | 2448 | 2292 | 3070 | 59 | 84 | 0 | 7326 | 8593 | ||||||
| Running | 701 | 658 | 9 | 9 | 40 | 49 | 2473 | 3577 | 233 | 327 | 0 | 3455 | 4620 | |||||||
| Total | 1335 | 1293 | 2364 | 2364 | 2024 | 2496 | 4766 | 6647 | 292 | 412 | 0 | 10,781 | 13,213 | 0.0% | 1.4% | 1.5% | ||||
| Supervision | Capital | 1585 | 1586 | 7367 | 7367 | 16,943 | 23,252 | 7309 | 11,694 | 0 | 0 | 0 | 33,204 | 43,898 | ||||||
| Running | 4856 | 1333 | 7360 | 7617 | 76,303 | 88,262 | 4925 | 6332 | 0 | 0 | 0 | 93,443 | 103,544 | |||||||
| Total | 6441 | 2918 | 14,726 | 14,984 | 93,246 | 111,515 | 12,234 | 18,026 | 0 | 0 | 0 | 126,648 | 147,443 | 16.7% | 16.8% | |||||
| Management | Capital | 94 | 94 | 159 | 159 | 513 | 775 | 1431 | 1600 | 222 | 261 | 0 | 2419 | 2888 | ||||||
| Running | 2442 | 2442 | 7933 | 8515 | 63,142 | 73,037 | 3822 | 7293 | 84 | 1824 | 0 | 77,422 | 93,111 | |||||||
| Total | 2535 | 2536 | 8092 | 8675 | 63,654 | 73,812 | 5252 | 8892 | 306 | 2085 | 0 | 79,841 | 96,000 | 10.5% | 11.1% | |||||
| Waste management | Capital | 94 | 94 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 94 | 94 | ||||||||
| Running | 0 | 0 | 132 | 162 | 0 | 0 | 0 | 0 | 0 | 132 | 162 | |||||||||
| Total | 94 | 94 | 132 | 162 | 0 | 0 | 0 | 0 | 0 | 226 | 256 | 0.0% | 0.0% | 0.0% | ||||||
| Total | 65,855 | 132,854 | 132,995 | 9272 | 34,640 | 29,306 | 68,238 | 200,660 | 201,239 | 315,010 | 407,487 | 76,241 | 104,213 | 143,364 | 759,406 | 875,240 | 100.0% | 100.0% | 100.0% | |
| % per site type | 45.9% | 17.5% | 15.2% | 6.5% | 4.6% | 3.3% | 47.6% | 26.4% | 23.0% | 41.5% | 46.6% | 10.0% | 11.9% | 100.0% | 100.0% | 100.0% | ||||
| National | Regional Health Offices | District Health Offices | Health Posts | Health Centers | Total | % per Activity | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2015 | 2016 | 2017 | 2015 | 2016 | 2017 | 2015 | 2016 | 2017 | 2016 | 2017 | 2016 | 2017 | 2015 | 2016 | 2017 | 2015 | 2016 | 2017 | ||
| Pre-introduction | Capital | 0 | 0 | 0 | 0 | |||||||||||||||
| Running | 50,226 | 50,226 | 0 | 0 | ||||||||||||||||
| Total | 50,226 | 50,226 | 0 | 0 | 39.3% | |||||||||||||||
| Initial training | Capital | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |||||||
| Running | 0 | 0 | 9272 | 0 | 0 | 68,238 | 0 | 0 | 9 | 0 | 0 | 0 | 77,519 | |||||||
| Total | 0 | 0 | 9272 | 0 | 0 | 68,238 | 0 | 0 | 9 | 0 | 0 | 0 | 77,519 | 60.7% | ||||||
| Social mobilization | Capital | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |||||
| Running | 20,653 | 0 | 6143 | 0 | 0 | 31,923 | 357 | 1470 | 1189 | 688 | 1645 | 0 | 60,877 | 3192 | ||||||
| Total | 20,653 | 0 | 0 | 6143 | 0 | 0 | 31,923 | 357 | 1470 | 1189 | 688 | 1645 | 0 | 60,877 | 3192 | 74.3% | 10.7% | |||
| Vaccine administration | Capital | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |||||
| Running | 0 | 0 | 0 | 0 | 0 | 0 | 2367 | 3741 | 16,829 | 20,875 | 0 | 0 | 0 | 19,195 | 24,616 | |||||
| Total | 0 | 0 | 0 | 0 | 0 | 0 | 2367 | 3741 | 16,829 | 20,875 | 0 | 0 | 19,195 | 24,616 | 23.4% | 82.3% | ||||
| Storage | Capital | 152 | 152 | 0 | 182 | 182 | 0 | 197 | 226 | 159 | 161 | 799 | 928 | 0 | 1490 | 1649 | ||||
| Running | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |||||
| Total | 152 | 152 | 0 | 182 | 182 | 0 | 197 | 226 | 159 | 161 | 799 | 928 | 0 | 1490 | 1649 | 1.8% | 5.5% | |||
| Distribution | Capital | 0 | 0 | 0 | 0 | 0 | 0 | 362 | 439 | 14 | 17 | 2 | 2 | 0 | 378 | 458 | ||||
| Running | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | ||||||
| Total | 0 | 0 | 0 | 0 | 0 | 0 | 362 | 439 | 14 | 17 | 2 | 2 | 0 | 378 | 458 | 0.5% | 1.5% | |||
| Supervision | Capital | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | ||||
| Running | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |||||
| Total | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |||||
| Management | Capital | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | ||||
| Running | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |||||
| Total | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |||||
| Waste management | Capital | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | ||||
| Running | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |||||
| Total | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |||||
| Total | 50,226 | 20,804 | 152 | 9272 | 6325 | 182 | 68,238 | 34,849 | 4763 | 18,481 | 22,243 | 1490 | 2575 | 127,745 | 81,940 | 29,915 | 100% | 100% | 100% | |
| % site type | 39.3% | 25.4% | 0.5% | 7.3% | 7.7% | 0.6% | 53.4% | 42.5% | 15.9% | 22.6% | 74.4% | 1.8% | 8.6% | 100% | 100% | 100% | ||||
| Total Annual Economic Cost | Total Annual Financial Cost | Economic Cost/Vaccinated Children (Irrespective of Timing) | Economic Cost/Vaccinated Children within 24 h | Financial Cost/Vaccinated Children (Irrespective of Timing) | Financial Cost/Vaccinated Children within 24 h | ||
|---|---|---|---|---|---|---|---|
| Costs, excluding the annualized costs of initial investment | 2016 | 759 406 | 81 940 | 2.00 | 2.42 | 0.22 | 0.26 |
| 2017 | 875 240 | 29 915 | 1.85 | 2.24 | 0.06 | <0.01 | |
| Costs, including the annualized costs of initial investment | 2016 | 809 819 | 130 745 | 2.13 | 2.58 | 0.34 | 0.42 |
| 2017 | 924 185 | 78 720 | 1.95 | 2.36 | 0.17 | 0.20 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gosset, A.; Nishimwe, M.L.; Diallo, M.Y.; Deroo, L.; Diallo, A.; Ba, E.H.; Carrieri, P.M.; Sokhna, C.; Vray, M.; Shimakawa, Y.; et al. The Costs of Introducing the Hepatitis B Birth Dose Vaccine into the National Immunization Programme in Senegal (NéoVac Study). Vaccines 2021, 9, 521. https://doi.org/10.3390/vaccines9050521
Gosset A, Nishimwe ML, Diallo MY, Deroo L, Diallo A, Ba EH, Carrieri PM, Sokhna C, Vray M, Shimakawa Y, et al. The Costs of Introducing the Hepatitis B Birth Dose Vaccine into the National Immunization Programme in Senegal (NéoVac Study). Vaccines. 2021; 9(5):521. https://doi.org/10.3390/vaccines9050521
Chicago/Turabian StyleGosset, Andréa, Marie Libérée Nishimwe, Mamadou Yaya Diallo, Lucas Deroo, Aldiouma Diallo, El Hadji Ba, Patrizia Maria Carrieri, Cheikh Sokhna, Muriel Vray, Yusuke Shimakawa, and et al. 2021. "The Costs of Introducing the Hepatitis B Birth Dose Vaccine into the National Immunization Programme in Senegal (NéoVac Study)" Vaccines 9, no. 5: 521. https://doi.org/10.3390/vaccines9050521
APA StyleGosset, A., Nishimwe, M. L., Diallo, M. Y., Deroo, L., Diallo, A., Ba, E. H., Carrieri, P. M., Sokhna, C., Vray, M., Shimakawa, Y., & Boyer, S. (2021). The Costs of Introducing the Hepatitis B Birth Dose Vaccine into the National Immunization Programme in Senegal (NéoVac Study). Vaccines, 9(5), 521. https://doi.org/10.3390/vaccines9050521