
Conversion from Venovenous to Venoarterial Extracorporeal Membrane Oxygenation in Adults


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Variables
2.3. Statistical Analysis
2.4. Ethical Considerations
3. Results
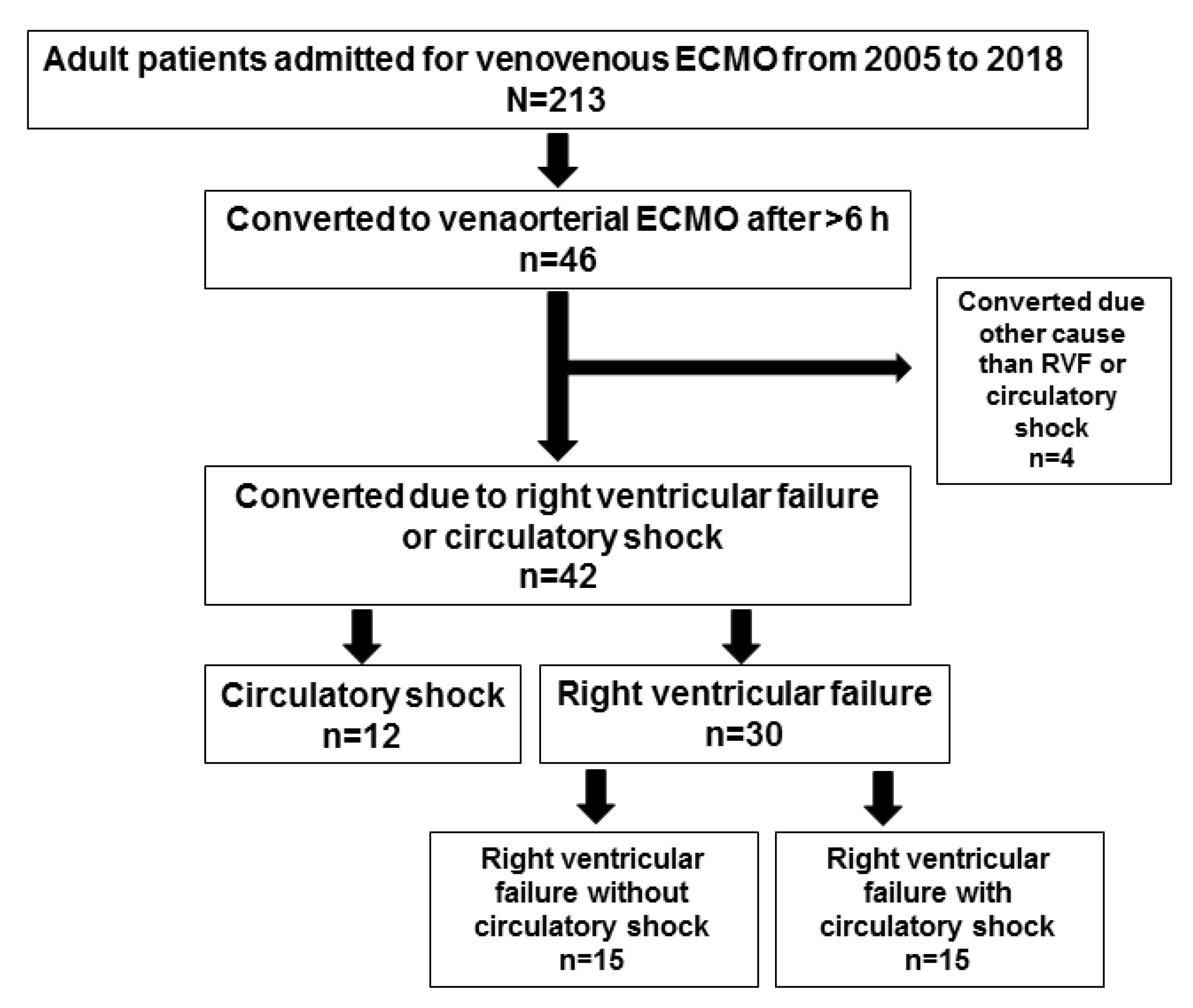
3.1. Subgroup Analyses: Converted Patients
3.2. Right Ventricular Failure
4. Discussion
5. Study Limitations
6. Clinical Implications
- At least 20% of patients subjected to respiratory support with ECMO may need combined cardio-respiratory support, i.e., VA ECMO from the start or during the course of treatment.
- Early realization of the need for VA ECMO probably improves patient prognosis, in the best case decision for VA is made already on admission. These patients may be identified on admission by a negative (-) RESP score. These patients need daily assessments.
- Patients converted to VA due to cardio-circulatory failure during VV ECMO are usually recognized within the first days.
- Patients who develop RVF are more difficult to recognize since typical features take up to two weeks to be present clinically. These patients cannot be distinguished from the general VV population at the time of admission for ECMO. Daily organ function assessments, including echocardiography and the trend of vasoactive support, are important tools to identify these subjects earlier.
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Paden, M.L.; Conrad, S.A.; Rycus, P.T.; Thiagarajan, R.R. Extracorporeal Life Support Organization Registry Report 2012. J. Am. Soc. Artif. Intern. Organs 2013, 59, 202–210. [Google Scholar] [CrossRef]
- Extracorporeal, Life, Support, Organization. International ECLS Registry Report. 2019. Available online: www.elso.org/Portals/0/Files/Reports/2019/International%20Summary%20July%202019.pdf (accessed on 1 November 2020).
- Gerke, A.K.; Tang, F.; Cavanaugh, J.E.; Doerschug, K.C.; Polgreen, P.M. Increased trend in extracorporeal membrane oxygenation use by adults in the United States since 2007. BMC Res. Notes 2015, 8, 686. [Google Scholar] [CrossRef] [Green Version]
- Peek, G.J.; Mugford, M.; Tiruvoipati, R.; Wilson, A.; Allen, E.; Thalanany, M.M.; Hibbert, C.L.; Truesdale, A.; Clemens, F.; Cooper, N.; et al. Efficacy and economic assessment of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR): A multicentre randomised controlled trial. Lancet 2009, 374, 1351–1363. [Google Scholar] [CrossRef]
- Sauer, C.M.; Yuh, D.D.; Bonde, P. Extracorporeal membrane oxygenation use has increased by 433% in adults in the United States from 2006 to 2011. J. Am. Soc. Artif. Intern. Organs 2015, 61, 31–36. [Google Scholar] [CrossRef]
- Brogan, T.V.; Lequier, L.; Lorusso, R.; MacLaren, G.; Peek, G. Extracorporeal Life Support: The ELSO Red Book, 5th ed.; Extracorporeal Life Support Organization: Ann Arbor, MI, USA, 2017. [Google Scholar]
- Conrad, S.A.; Broman, L.M.; Taccone, F.S.; Lorusso, R.; Malfertheiner, M.V.; Pappalardo, F.; Di Nardo, M.; Belliato, M.; Grazioli, L.; Barbaro, R.P.; et al. The Extracorporeal Life Support Organization Maastricht Treaty for Nomenclature in Extracorporeal Life Support. A Position Paper of the Extracorporeal Life Support Organization. Am. J. Respir. Crit. Care Med. 2018. [Google Scholar] [CrossRef] [PubMed]
- Bunge, J.J.H.; Caliskan, K.; Gommers, D.; Reis Miranda, D. Right ventricular dysfunction during acute respiratory distress syndrome and veno-venous extracorporeal membrane oxygenation. J. Thorac. Dis. 2018, 10, S674–S682. [Google Scholar] [CrossRef] [PubMed]
- Holzgraefe, B.; Broome, M.; Kalzen, H.; Konrad, D.; Palmer, K.; Frenckner, B. Extracorporeal membrane oxygenation for pandemic H1N1 2009 respiratory failure. Minerva Anestesiol. 2010, 76, 1043–1051. [Google Scholar] [PubMed]
- Patroniti, N.; Bonatti, G.; Senussi, T.; Robba, C. Mechanical ventilation and respiratory monitoring during extracorporeal membrane oxygenation for respiratory support. Ann. Transl. Med. 2018, 6, 386. [Google Scholar] [CrossRef]
- Klein, M.D.; Andrews, A.F.; Wesley, J.R.; Toomasian, J.; Nixon, C.; Roloff, D.; Bartlett, R.H. Venovenous perfusion in ECMO for newborn respiratory insufficiency. A clinical comparison with venoarterial perfusion. Ann. Surg. 1985, 201, 520–526. [Google Scholar] [CrossRef]
- Shanley, C.J.; Hirschl, R.B.; Schumacher, R.E.; Overbeck, M.C.; Delosh, T.N.; Chapman, R.A.; Coran, A.G.; Bartlett, R.H. Extracorporeal life support for neonatal respiratory failure. A 20-year experience. Ann. Surg. 1994, 220, 269–280. [Google Scholar] [CrossRef]
- Dimmitt, R.A.; Moss, R.L.; Rhine, W.D.; Benitz, W.E.; Henry, M.C.; Vanmeurs, K.P. Venoarterial versus venovenous extracorporeal membrane oxygenation in congenital diaphragmatic hernia: The Extracorporeal Life Support Organization Registry, 1990–1999. J. Pediatric Surg. 2001, 36, 1199–1204. [Google Scholar] [CrossRef]
- Kovler, M.L.; Garcia, A.V.; Beckman, R.M.; Salazar, J.H.; Vacek, J.; Many, B.T.; Rizeq, Y.; Abdullah, F.; Goldstein, S.D. Conversion From Venovenous to Venoarterial Extracorporeal Membrane Oxygenation Is Associated With Increased Mortality in Children. J. Surg. Res. 2019, 244, 389–394. [Google Scholar] [CrossRef] [PubMed]
- Kon, Z.N.; Bittle, G.J.; Pasrija, C.; Pham, S.M.; Mazzeffi, M.A.; Herr, D.L.; Sanchez, P.G.; Griffith, B.P. Venovenous Versus Venoarterial Extracorporeal Membrane Oxygenation for Adult Patients With Acute Respiratory Distress Syndrome Requiring Precannulation Hemodynamic Support: A Review of the ELSO Registry. Ann. Thorac. Surg. 2017, 104, 645–649. [Google Scholar] [CrossRef] [Green Version]
- Falk, L.; Hultman, J.; Broman, L.M. Extracorporeal Membrane Oxygenation for Septic Shock. Crit. Care Med. 2019, 47, 1097–1105. [Google Scholar] [CrossRef] [PubMed]
- von Bahr, V.; Hultman, J.; Eksborg, S.; Frenckner, B.; Kalzen, H. Long-Term Survival in Adults Treated With Extracorporeal Membrane Oxygenation for Respiratory Failure and Sepsis. Crit. Care Med. 2017, 45, 164–170. [Google Scholar] [CrossRef]
- Broman, L.M.; Holzgraefe, B.; Palmer, K.; Frenckner, B. The Stockholm experience: Interhospital transports on extracorporeal membrane oxygenation. Crit. Care 2015, 19, 278. [Google Scholar] [CrossRef] [Green Version]
- Fletcher-Sandersjoo, A.; Frenckner, B.; Broman, M. A Single-Center Experience of 900 Interhospital Transports on Extracorporeal Membrane Oxygenation. Ann. Thorac. Surg. 2018. [Google Scholar] [CrossRef] [Green Version]
- Malfertheiner, M.V.; Broman, L.M.; Belliato, M.; Venti, A.; Bader, A.; Taccone, F.S.; Di Nardo, M.; Maj, G.; Pappalardo, F. Management strategies in venovenous extracorporeal membrane oxygenation: A retrospective comparison from five European centres. Crit. Care Resusc. J. Australas. Acad. Crit. Care Med. 2017, 19, 76–81. [Google Scholar]
- Metnitz, P.G.; Moreno, R.P.; Almeida, E.; Jordan, B.; Bauer, P.; Campos, R.A.; Iapichino, G.; Edbrooke, D.; Capuzzo, M.; Le Gall, J.R. SAPS 3—From evaluation of the patient to evaluation of the intensive care unit. Part 1: Objectives, methods and cohort description. Intensive Care Med. 2005, 31, 1336–1344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moreno, R.P.; Metnitz, P.G.; Almeida, E.; Jordan, B.; Bauer, P.; Campos, R.A.; Iapichino, G.; Edbrooke, D.; Capuzzo, M.; Le Gall, J.R. SAPS 3—From evaluation of the patient to evaluation of the intensive care unit. Part 2: Development of a prognostic model for hospital mortality at ICU admission. Intensive Care Med. 2005, 31, 1345–1355. [Google Scholar] [CrossRef] [Green Version]
- Schmidt, M.; Bailey, M.; Sheldrake, J.; Hodgson, C.; Aubron, C.; Rycus, P.T.; Scheinkestel, C.; Cooper, D.J.; Brodie, D.; Pellegrino, V.; et al. Predicting survival after extracorporeal membrane oxygenation for severe acute respiratory failure. The Respiratory Extracorporeal Membrane Oxygenation Survival Prediction (RESP) score. Am. J. Respir. Crit. Care Med. 2014, 189, 1374–1382. [Google Scholar] [CrossRef] [PubMed]
- Belletti, A.; Lerose, C.C.; Zangrillo, A.; Landoni, G. Vasoactive-Inotropic Score: Evolution, Clinical Utility, and Pitfalls. J. Cardiothorac. Vasc. Anesth. 2020. [Google Scholar] [CrossRef] [PubMed]
- Vincent, J.L.; Moreno, R.; Takala, J.; Willatts, S.; De Mendonca, A.; Bruining, H.; Reinhart, C.K.; Suter, P.M.; Thijs, L.G. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996, 22, 707–710. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, M.; Burrell, A.; Roberts, L.; Bailey, M.; Sheldrake, J.; Rycus, P.T.; Hodgson, C.; Scheinkestel, C.; Cooper, D.J.; Thiagarajan, R.R.; et al. Predicting survival after ECMO for refractory cardiogenic shock: The survival after veno-arterial-ECMO (SAVE)-score. Eur. Heart J. 2015, 36, 2246–2256. [Google Scholar] [CrossRef] [PubMed]
- Beghetti, M. Echocardiographic Evaluation of Pulmonary Pressures and Right Ventricular Function after Pediatric Cardiac Surgery: A Simple Approach for the Intensivist. Front. Pediatrics 2017, 5, 184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rudski, L.G.; Lai, W.W.; Afilalo, J.; Hua, L.; Handschumacher, M.D.; Chandrasekaran, K.; Solomon, S.D.; Louie, E.K.; Schiller, N.B. Guidelines for the echocardiographic assessment of the right heart in adults: A report from the American Society of Echocardiography endorsed by the European Association of Echocardiography, a registered branch of the European Society of Cardiology, and the Canadian Society of Echocardiography. J. Am. Soc. Echocardiogr. Off. Publ. Am. Soc. Echocardiogr. 2010, 23, 685–713. [Google Scholar] [CrossRef]
- Schmid, E.; Hilberath, J.N.; Blumenstock, G.; Shekar, P.S.; Kling, S.; Shernan, S.K.; Rosenberger, P.; Nowak-Machen, M. Tricuspid annular plane systolic excursion (TAPSE) predicts poor outcome in patients undergoing acute pulmonary embolectomy. Heartlung Vessel. 2015, 7, 151–158. [Google Scholar]
- Holzgraefe, B.; Andersson, C.; Kalzén, H.; von Bahr, V.; Mosskin, M.; Larsson, E.M.; Palmér, K.; Frenckner, B.; Larsson, A. Does permissive hypoxaemia during extracorporeal membrane oxygenation cause long-term neurological impairment?: A study in patients with H1N1-induced severe respiratory failure. Eur. J. Anaesthesiol. 2017, 34, 98–103. [Google Scholar] [CrossRef] [Green Version]
- Lazzeri, C.; Cianchi, G.; Bonizzoli, M.; Batacchi, S.; Terenzi, P.; Bernardo, P.; Valente, S.; Gensini, G.F.; Peris, A. Right ventricle dilation as a prognostic factor in refractory acute respiratory distress syndrome requiring veno-venous extracorporeal membrane oxygenation. Minerva Anestesiol. 2016, 82, 1043–1049. [Google Scholar]
- Lindfors, M.; Frenckner, B.; Sartipy, U.; Bjallmark, A.; Broome, M. Venous Cannula Positioning in Arterial Deoxygenation During Veno-Arterial Extracorporeal Membrane Oxygenation-A Simulation Study and Case Report. Artif. Organs 2017, 41, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Sakr, Y.; Lobo, S.M.; Moreno, R.P.; Gerlach, H.; Ranieri, V.M.; Michalopoulos, A.; Vincent, J.L. Patterns and early evolution of organ failure in the intensive care unit and their relation to outcome. Crit. Care 2012, 16, R222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Falk, L.; Sallisalmi, M.; Lindholm, J.A.; Lindfors, M.; Frenckner, B.; Broome, M.; Broman, L.M. Differential hypoxemia during venoarterial extracorporeal membrane oxygenation. Perfusion 2019, 34, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Hou, X.; Yang, X.; Du, Z.; Xing, J.; Li, H.; Jiang, C.; Wang, J.; Xing, Z.; Li, S.; Li, X.; et al. Superior vena cava drainage improves upper body oxygenation during veno-arterial extracorporeal membrane oxygenation in sheep. Crit. Care 2015, 19, 68. [Google Scholar] [CrossRef] [Green Version]
- Fuchs, G.; Berg, N.; Broman, L.M.; Prahl Wittberg, L. Flow-induced platelet activation in components of the extracorporeal membrane oxygenation circuit. Sci. Rep. 2018, 8, 13985. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Non-Converted | Converted | p-Value | |
|---|---|---|---|
| Number, n | 167 (missing n = 6) | 46 | |
| Male sex, % | 66 | 65 | 1.0 |
| Age, years | 49 (34.5–59) | 50 (33–60) | 0.74 |
| SAPS-3 | 74 (67–81) | 72 (67–80) | 0.87 |
| RESP * | 2 (0–4) | −2.5 (−4–1) | <0.0001 |
| Tidal volume ** | 288 (150–400) | 200 (55–388) # | 0.11 |
| RVD, % | 28 | 87 | <0.0001 |
| RVF, % | 10 | 72 | <0.0001 |
| Circ. failure, % | 51 | 86 | <0.0001 |
| Circ. Shock, % | 49 | 44 | 0.62 |
| Days on ECMO, n | 6.6 (3–12) | 22 (12–40) | <0.0001 |
| Mortality rate, % | 16 | 61 | <0.0001 |
| At Admission (Pre-ECMO) | VV ECMO 12 h | p-Value (Pre-ECMO vs. 12 h) | VV Data before Conversion to VA | p-Value (Pre-ECMO vs. Conv.) | p-Value (12 h vs. Conv.) | |
|---|---|---|---|---|---|---|
| pH | 7.28 (7.18–7.35) | 7.38 (7.34–7.45) | <0.0001 | 7.38 (7.31–7.41) | <0.0001 | |
| pCO2, kPa | 7.7 (6.2–8.6) | 5.5 (5.5–5.65) | # | 5.3 (4.8–5.8) | # | |
| PpreCO2, kPa | -- | 5.8 (5.3–6.4) | -- | 5.6 (5.1–8) | -- | |
| pO2, kPa | 7.0 (6.2–8.5) | 7.4 (6.0–7.8) | # | 6.1 (4.9–8.0) | # | |
| PpreO2, kPa | -- | 5.9 (5.5–6.4) | -- | 5.4 (4.8–5.8) | -- | <0.01 |
| SpO2, % | 84 (74–88) | 88 (79–93) | <0.02 | 80 (71–88) | <0.001 | |
| Lactate, mmol/L | 2.3 (1.7–4.3) | 2.1 (1.4–3.4) | 1.8 (1.3–3.4) | |||
| FiO2, % | 100 (100–100) | 50 (40–60) | <0.0001 | 60 (50–70) | <0.0001 | <0.001 |
| PIP, cmH2O | 35 ± 7.7 | 27 ± 4.9 | <0.0001 | 24 ± 4.6 | <0.0001 | |
| PEEP, cmH2O | 14 ± 4.3 | 8.8 ± 3.2 | <0.0001 | 6.4 ± 3.6 | <0.0001 | <0.01 |
| Driving pressure, cmH2O | 20 (16–24) | 18 (14–21) | 18 (15–21) | |||
| Vt, mL | 473 ± 159 | 315 ± 210 | <0.0002 | 188 ± 155 | <0.0001 | <0.003 |
| Vt/kg BW, mL/kg | 6.1 (5.2–7.3) | 3.5 (1.8–5.6) | <0.0001 | 1.8 (0.8–3.8) | <0.0001 | <0.0001 |
| RR, min−1 | 25 ± 7.6 | 20 ± 6.0 | <0.02 | 24 ± 10 | ||
| Mean arterial BP, mmHg | 70 (62–80) | 68 (63–73) | 66 (61–72) | |||
| Hgb, g/L | 111 ± 15.5 | 115 ± 11.4 | 118 ± 13.0 | <0.02 | ||
| ECMO blood flow, L/min | -- | 4.3 (3.85–4.8) | 4.5 (4.1–5.0) | |||
| DecmoO2, mL/min | -- | 224 ± 46 | -- | 243 ± 42 | -- | <0.02 |
| SOFAc | 3 (3–4) | 3 (0–4) | <0.02 | 4 (3–4) | <0.05 | <0.002 |
| No. vasoactive drugs, n | 1 (1–1) | 1 (0–1) | <0.05 | 2 (1–2) | <0.001 | <0.0001 |
| VIS | 12 (5–42) | 5 (0–20) | <0.02 | 19 (10–29) | <0.001 |
| Alive (n = 16) | Deceased (n = 26) | p-Value | |
|---|---|---|---|
| pre-ECMO data | |||
| Male sex, % | 69 | 65 | 1.0 |
| Age, years, (range) | 47.5 ± 17.5 | 48.6 ± 16.7 | 0.39 |
| (19–67) | (23–77) | ||
| Body weight, kg | 76 (72–84) | 77 (70–86) | 0.77 |
| pH | 7.30 (7.21–7.34) | 7.26 (7.18–7.34) | 0.92 |
| pCO2, kPa | 7.7 (5.8–8.6) | 8.0 (6.7–8.6) | 0.47 |
| pO2, kPa | 7 (6.4–9) | 7 (6.3–7.6) | 0.89 |
| SaO2, % | 83 (71–89) | 84 (75–87) | 0.96 |
| FiO2, % | 100 (97.5–100) | 100 (100–100) | 0.045 |
| PIP, cmH2O | 35 ± 8.3 | 35 ± 7.8 | 0.76 |
| PEEP, cmH2O | 14 ± 4.3 | 14 ± 4.4 | 0.86 |
| Vt, mL | 481 ± 199 | 463 ± 133 | 0.74 |
| MAP, mmHg | 78 (64–81) | 70 (63–80) | 0.65 |
| Hemoglobin, g/L | 113 ± 14 | 109 ± 17 | 0.44 |
| Lactate, mmol/L | 2 (1.1–4.6) | 2.4 (1.8–3.4) | 0.20 |
| No. of vasoactive drugs, n | 1 (1–1) * | 1 (1–1) ** | 0.53 |
| VIS | 10 (9–40) | 10.5 (4–44) | 0.94 |
| SOFAin | 11.5 (9–12.3) # | 12 (8.3–13.8) † | 0.88 |
| SOFAc | 3 (2–4) | 3.5 (3–4) | 0.35 |
| SAPS-3 | 71.4 ± 10.0 | 76.4 ± 12.9 | 0.20 |
| RESP score | 0 (−2.3–1) | −4 (−5.8–−0.3) | 0.012 |
| Data at time of conversion to VA ECMO | |||
| Time to conversion, days, (range) | 8.4 (2.1–15) | 6.9 (3.9–13.8) | 0.68 |
| (0.9–31.3) | (1.1–33.8) | ||
| Time from recognition of RVF or circulatory shock to conversion, days, (range) | 0.6 (0.0–1.0) | 0 (0–0.8) | 0.92 |
| (0–8) | (0–3) | ||
| pH | 7.37 (7.30–7.40) | 7.38 (7.32–7.42) | 0.41 |
| SaO2; SpO2, % | 82 (70–86) | 77 (71–88) | 0.95 |
| FiO2 (%) | 60 (50–70) | 60 (50–60) | 0.78 |
| PIP, cmH2O | 24 ± 5.6 | 25 ± 4.2 | 0.49 |
| PEEP, cmH2O | 6.2 ± 4.2 | 6.1 ± 3.4 | 0.92 |
| Vt, mL | 183 ± 143 | 180 ± 156 | 0.95 |
| MAP, mmHg | 66 (64–71) | 67 (60–73) | 0.75 |
| Hemoglobin, g/L | 117 ± 16 | 118 ± 11 | 0.86 |
| ECMO blood flow, L/min | 4.8 (4–5.3) | 4.4 (4.1–5) | 0.71 |
| Lactate, mmol/L | 1.5 (1.3–2.1) | 1.7 (1.2–3.8) | 0.07 |
| No. of vasoactive drugs, n | 2 (1–2.2)* | 1 (1–2) ** | 0.45 |
| VIS | 26 (11–31) | 14 (6–26) | 0.16 |
| SOFAconv | 14 (12.8–16.3)# | 15 (14–17) † | 0.23 |
| SOFAdelta | 2.5 (1–4) | 3 (2–6) | 0.25 |
| SOFAc | 4 (3–4) | 4 (3–4) | 0.70 |
| SAVE score at conversion | −6.5 (−10–−4) | −9 (−10.8–−7) | 0.08 |
| Days on ECMO, n | 23.3 (13.1–45.9) | 25.5 (12.1–40.1) | 0.78 |
| Circulatory Shock (n = 12) | p-Value (Circ Shock vs. RVF all) | RVF all (n = 30) | RVF Presented with Shock (n = 15) | RVF not Presented with Shock (n = 15) | p-Value (RVF, w vs. w/o Shock) | |
|---|---|---|---|---|---|---|
| pre-ECMO data in patients who later were converted to VA ECMO | ||||||
| Male sex, % | 67 | 1.0 | 67 | 53 | 80 | 0.25 |
| Age, years, (range) | 44.9 ± 19.5 | 0.66 | 47.5 ± 16.2 | 47.5 ± 13.7 | 47.6 ± 18.8 | 0.98 |
| (19–74) | (19–78) | (19–66) | (22–78) | |||
| Body weight, kg | 74 (69–82) | 0.44 | 77 (71–86) | 73 (66–82) | 83 (77–89) | 0.08 |
| pH | 7.21 (7.18–7.32) | 0.20 | 7.31 (7.21–7.37) | 7.34 (7.24–7.36) | 7.29 (7.19–7.36) | 0.52 |
| pCO2, kPa | 7.9 (6.4–8.1) | 0.60 | 7.9 (6.2–8.8) | 8.1 (6.4–8.7) | 7.6 (6.1–9) | 0.60 |
| pO2, kPa | 7.1 (6.3–7.8) | 0.71 | 7.0 (6.2–8.5) | 6.8 (6–8.1) | 7.2 (6.7–8.5) | 0.34 |
| SaO2, % | 80 (70–84) | 0.14 | 84 (75–88) | 84 (76–89) | 84 (78–87) | 0.90 |
| FiO2, % | 100 (100–100) | 0.77 | 100 (100–100) | 100 (100–100) | 100 (100–100) | 0.92 |
| PIP, cmH2O | 35 ± 4.6 | 0.76 | 35 ± 9.1 | 35 ± 11 | 35 ± 7.7 | 0.93 |
| PEEP, cmH2O | 15 ± 4 | 0.32 | 14 ± 4.4 | 12 ± 4.7 | 14 ± 4.0 | 0.22 |
| Vt, mL | 491 ± 194 | 0.60 | 461 ± 145 | 495 ± 125 | 431 ± 158 | 0.26 |
| MAP, mmHg | 61 (58–74) | 0.006 | 78 (69–86) | 71 (65–90) | 80 (73–82) | 0.64 |
| Hemoglobin, g/L | 120 ± 14 | 0.01 | 107 ± 15 | 112 ± 16 | 101 ± 12 | 0.06 |
| Lactate, mmol/L | 4.4 (2.4–6.6) | 0.002 | 2.1 (1.2–2.4) | 2.3 (1.2–3.0) | 1.9 (1.2–2.2) | 0.37 |
| No. of vasoactive drugs, n | 1(1–1) * | 0.22 | 1(1–1) ** | 1 (1–1) | 1(1–1) | 0.96 |
| VIS | 36 (9–60) | 0.04 | 9.7 (3–33) | 11 (3.4–38) | 9.4 (2.6–12) | 0.54 |
| SOFAin | 13 (12–14.5) # | < 0.0001 | 11 (8.3–12) † | 11 (9–12.5) ‡ | 11 (8–12) $ | 0.53 |
| SOFAc | 4 (3–4) | 0.15 | 3 (0.5–4) | 3 (0–4) | 3 (2.5–4) | 0.59 |
| SAPS-3 | 76.3 ± 15.0 | 0.53 | 73.7 ± 10.8 | 75.3 ± 10.8 | 72.1 ± 11.0 | 0.42 |
| RESP score | −2 (−6–3.3) | 0.61 | −3 (−4–0.8) | −3 (−5.5–−1.5) | 0 (−4–1) | 0.026 |
| Data at time of conversion to VA ECMO | ||||||
| Time to conversion, days, (range) | 2.1 (1.3–4.1) | <0.001 | 11.1 (5.4–15) | 12.3 (4.1–15) | 10.4 (6.6–17.2) | 0.98 |
| (1–18.9) | (1–40.9) | (1–40.9) | (3.8–34.2) | |||
| Time from recognition of RVF or circulatory shock to conversion, days, (range) | 0 (0–0.5) | 0.12 | 0.9 (0–1) | 1 (0.4–1.5) | 0.7 (0–1) | 0.058 |
| (0–2) | (0–8) | (0–8) | (0–1.6) | |||
| pH | 7.33 (7.29–7.39) | 0.12 | 7.39 (7.33–7.42) | 7.40 (7.34–7.44) | 7.37 (7.34–7.40) | 0.21 |
| SaO2; SpO2, % | 85 (76–90) | 0.11 | 77 (70–85) | 78 (74–88) | 73 (66–82) | 0.18 |
| FiO2, % | 60 (60–72) | 0.17 | 50 (50–62) | 50 (50–60) | 60 (50–65) | 0.30 |
| PIP, cmH2O | 25 ± 4.9 | 0.47 | 24 ± 4.7 | 24 ± 2.9 | 25 ± 5.8 | 0.57 |
| PEEP, cmH2O | 8.6 ± 4.3 | 0.005 | 5.1 ± 2.8 | 4.9 ± 2.9 | 5.2 ± 2.8 | 0.80 |
| Vt, mL | 216 ± 142 | 0.37 | 166 ± 152 | 178 ± 132 | 156 ± 172 | 0.61 |
| MAP, mmHg | 67 (64–72) | 0.87 | 66 (60–73) | 66 (56–71) | 70 (64–74) | 0.16 |
| b-Hemoglobin, g/L | 114 ± 17 | 0.18 | 119 ± 11 | 122 ± 9 | 116 ± 12 | 0.02 |
| ECMO blood flow, L/min | 4.5 (4–5.1) | 0.73 | 4.5 (4.2–5.1) | 4.5 (4–4.8) | 5.1 (4.2–5.5) | 0.07 |
| p-Lactate, mmol/L | 3.8 (2.2–7.0) | < 0.0001 | 1.4 (1.1–1.8) | 1.2 (1.1–1.4) | 1.7 (1.4–2.5) | 0.02 |
| No. of vasoactive drugs, n | 2 (1–3) * | 0.21 | 1 (1–2) ** | 1 (1–2) | 1(1–2) | 0.07 |
| VIS | 29 (23–52) | 0.006 | 12 (6–26) | 10 (4.5–13) | 18 (10.5–27) | 0.06 |
| SOFAconv | 16 (14.8–18) # | 0.07 | 14 (12.3–16.8) † | 13 (11.5–14.5) ‡ | 15 (14–17) $ | 0.07 |
| SOFAdelta | 2.5 (1–4.3) | 0.61 | 3 (1–5.8) | 3 (0.5–4) | 4 (2–7.5) | 0.09 |
| SOFAc | 4 (4–4) | 0.29 | 4 (3–4) | 3 (3–4) | 4 (3–4) | 0.07 |
| SAVE score at conversion | −9.5 (−10.5–−4.8) | 0.86 | −8 (−10–−6) | −7 (−10–−6) | −8 (−12–−6) | 0.47 |
| Days on ECMO, n | 10.4 (5.9–29.1) | 0.048 | 29.6 (17.3–42.1) | 34.3 (22.2–46.9) | 22.8 (13–33.9) | 0.09 |
| Mortality rate, % | 50 | 0.48 | 67 | 67 | 67 | 1.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Falk, L.; Fletcher-Sandersjöö, A.; Hultman, J.; Broman, L.M. Conversion from Venovenous to Venoarterial Extracorporeal Membrane Oxygenation in Adults. Membranes 2021, 11, 188. https://doi.org/10.3390/membranes11030188
Falk L, Fletcher-Sandersjöö A, Hultman J, Broman LM. Conversion from Venovenous to Venoarterial Extracorporeal Membrane Oxygenation in Adults. Membranes. 2021; 11(3):188. https://doi.org/10.3390/membranes11030188
Chicago/Turabian StyleFalk, Lars, Alexander Fletcher-Sandersjöö, Jan Hultman, and Lars Mikael Broman. 2021. "Conversion from Venovenous to Venoarterial Extracorporeal Membrane Oxygenation in Adults" Membranes 11, no. 3: 188. https://doi.org/10.3390/membranes11030188
APA StyleFalk, L., Fletcher-Sandersjöö, A., Hultman, J., & Broman, L. M. (2021). Conversion from Venovenous to Venoarterial Extracorporeal Membrane Oxygenation in Adults. Membranes, 11(3), 188. https://doi.org/10.3390/membranes11030188