
Outcome Prediction in Patients with Severe COVID-19 Requiring Extracorporeal Membrane Oxygenation—A Retrospective International Multicenter Study

 ,
,  , , ,
, , ,  ,
,  , ,
, ,  add
Show full author list
add
Show full author list
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Data Collection and Management
2.3. Definitions
2.4. Statistical Methods
3. Results
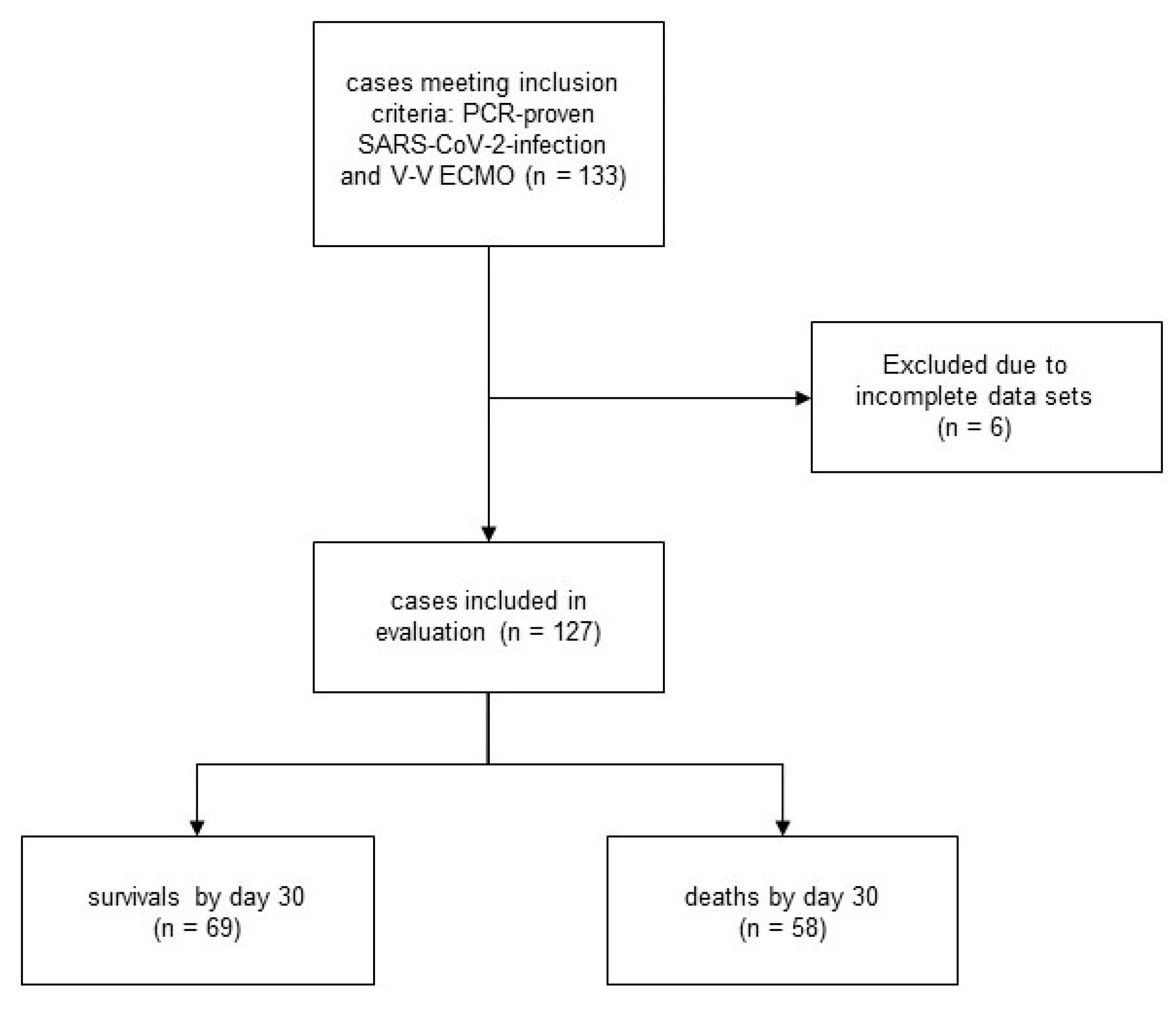
3.1. Patients
3.2. Ventilator Settings Blood Gas Analysis before ECMO
3.3. Pre-Existing Conditions
3.4. Intensive Care and ARDS Treatment
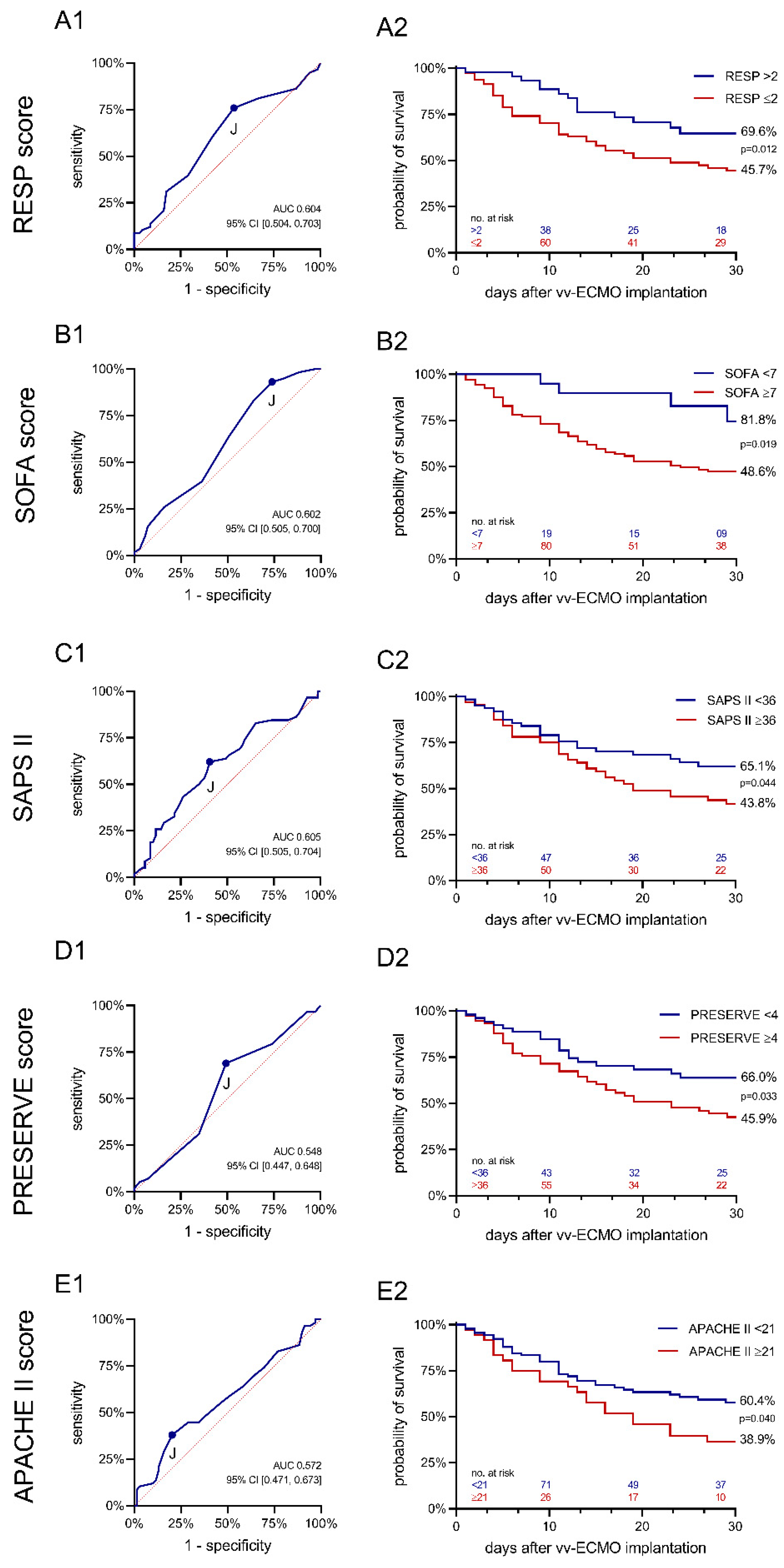
3.5. Clinical Scores
4. Discussion
4.1. Limitations
4.2. Conclusions
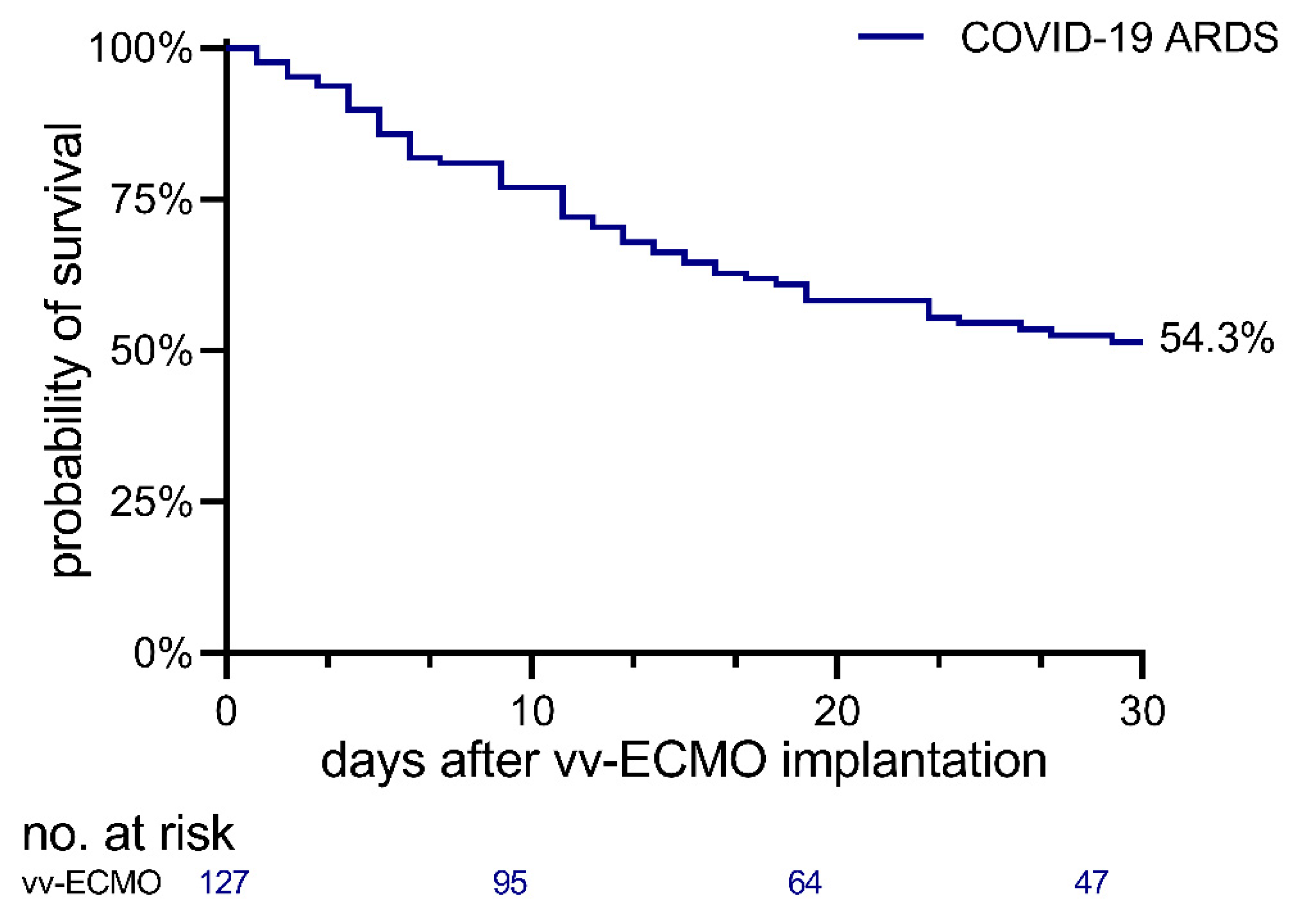
- Thirty-day-survival in COVID-19 patients treated with V-V ECMO and evaluated in our registry is 54 percent, encouraging further clinical research and application.
- The use of scores for the prediction of mortality cannot be recommended for treatment decisions in severe COVID-19 ARDS and V-V ECMO should be considered if deemed beneficial as long as resources are available. Scoring results below or above a specific cut-off value may be considered as an additional tool in the evaluation of prognosis but cannot be used for triaging this patient population.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yang, X.; Yu, Y.; Xu, J.; Shu, H.; Xia, J.; Liu, H.; Wu, Y.; Zhang, L.; Yu, Z.; Fang, M.; et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: A single-centered, retrospective, observational study. Lancet Respir. Med. 2020, 8, 475–481. [Google Scholar] [CrossRef] [Green Version]
- Cummings, M.J.; Baldwin, M.R.; Abrams, D.; Jacobson, S.D.; Meyer, B.J.; Balough, E.M.; Aaron, J.G.; Claassen, J.; Rabbani, L.E.; Hastie, J.; et al. Epidemiology, clinical course, and outcomes of critically ill adults with COVID-19 in New York City: A prospective cohort study. Lancet 2020, 395, 1763–1770. [Google Scholar] [CrossRef]
- Karagiannidis, C.; Mostert, C.; Hentschker, C.; Voshaar, T.; Malzahn, J.; Schillinger, G.; Klauber, J.; Janssens, U.; Marx, G.; Weber-Carstens, S.; et al. Case characteristics, resource use, and outcomes of 10 021 patients with COVID-19 admitted to 920 German hospitals: An observational study. Lancet Respir. Med. 2020, 8, 853–862. [Google Scholar] [CrossRef]
- Arentz, M.; Yim, E.; Klaff, L.; Lokhandwala, S.; Riedo, F.X.; Chong, M.; Lee, M. Characteristics and Outcomes of 21 Critically Ill Patients With COVID-19 in Washington State. JAMA 2020, 323, 1612–1614. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grasselli, G.; Zangrillo, A.; Zanella, A.; Antonelli, M.; Cabrini, L.; Castelli, A.; Cereda, D.; Coluccello, A.; Foti, G.; Fumagalli, R.; et al. Baseline Characteristics and Outcomes of 1591 Patients Infected With SARS-CoV-2 Admitted to ICUs of the Lombardy Region, Italy. JAMA 2020, 323, 1574–1581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barbaro, R.P.; MacLaren, G.; Boonstra, P.S.; Iwashyna, T.J.; Slutsky, A.S.; Fan, E.; Bartlett, R.H.; Tonna, J.E.; Hyslop, R.; Fanning, J.J.; et al. Extracorporeal membrane oxygenation support in COVID-19: An international cohort study of the Extracorporeal Life Support Organization registry. Lancet 2020, 396, 1071–1078. [Google Scholar] [CrossRef]
- Schmidt, M.; Hajage, D.; Lebreton, G.; Monsel, A.; Voiriot, G.; Levy, D.; Baron, E.; Beurton, A.; Chommeloux, J.; Meng, P.; et al. Extracorporeal membrane oxygenation for severe acute respiratory distress syndrome associated with COVID-19: A retrospective cohort study. Lancet Respir. Med. 2020, 8, 1121–1131. [Google Scholar] [CrossRef]
- Rajagopal, K.; Keller, S.P.; Akkanti, B.; Bime, C.; Loyalka, P.; Cheema, F.H.; Zwischenberger, J.B.; Banayosy, A.E.; Pappalardo, F.; Slaughter, M.S.; et al. Advanced Pulmonary and Cardiac Support of COVID-19 Patients: Emerging Recommendations From ASAIO-A “Living Working Document”. Circ. Heart Fail. 2020, 13, e007175. [Google Scholar] [CrossRef] [PubMed]
- Ramanathan, K.; Antognini, D.; Combes, A.; Paden, M.; Zakhary, B.; Ogino, M.; MacLaren, G.; Brodie, D.; Shekar, K. Planning and provision of ECMO services for severe ARDS during the COVID-19 pandemic and other outbreaks of emerging infectious diseases. Lancet Respir. Med. 2020, 8, 518–526. [Google Scholar] [CrossRef] [Green Version]
- Li, C.; Hou, X.; Tong, Z.; Qiu, H.; Li, Y.; Li, A. Chinese Society of Extracorporeal Life S. Extracorporeal membrane oxygenation programs for COVID-19 in China. Crit. Care 2020, 24, 317. [Google Scholar] [CrossRef]
- Bartlett, R.H.; Ogino, M.T.; Brodie, D.; McMullan, D.M.; Lorusso, R.; MacLaren, G.; Stead, C.M.; Rycus, P.; Fraser, J.F.; Belohlavek, J.; et al. Initial ELSO Guidance Document: ECMO for COVID-19 Patients with Severe Cardiopulmonary Failure. ASAIO J. 2020, 66, 472–474. [Google Scholar] [CrossRef]
- Abrams, D.; Ferguson, N.D.; Brochard, L.; Fan, E.; Mercat, A.; Combes, A.; Pellegrino, V.; Schmidt, M.; Slutsky, A.S.; Brodie, D. ECMO for ARDS: From salvage to standard of care? Lancet Respir. Med. 2019, 7, 108–110. [Google Scholar] [CrossRef]
- Vincent, J.L.; Moreno, R.; Takala, J.; Willatts, S.; De Mendonca, A.; Bruining, H.; Reinhart, C.K.; Suter, P.M.; Thijs, L.G. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996, 22, 707–710. [Google Scholar] [CrossRef]
- Lambden, S.; Laterre, P.F.; Levy, M.M.; Francois, B. The SOFA score-development, utility and challenges of accurate assessment in clinical trials. Crit. Care 2019, 23, 374. [Google Scholar] [CrossRef] [Green Version]
- Knaus, W.A.; Draper, E.A.; Wagner, D.P.; Zimmerman, J.E. APACHE II: A severity of disease classification system. Crit. Care Med. 1985, 13, 818–829. [Google Scholar] [CrossRef]
- Le Gall, J.R.; Lemeshow, S.; Saulnier, F. A new Simplified Acute Physiology Score (SAPS II) based on a European/North American multicenter study. JAMA 1993, 270, 2957–2963. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, M.; Bailey, M.; Sheldrake, J.; Hodgson, C.; Aubron, C.; Rycus, P.T.; Scheinkestel, C.; Cooper, D.J.; Brodie, D.; Pellegrino, V.; et al. Predicting survival after extracorporeal membrane oxygenation for severe acute respiratory failure. The Respiratory Extracorporeal Membrane Oxygenation Survival Prediction (RESP) score. Am. J. Respir. Crit. Care Med. 2014, 189, 1374–1382. [Google Scholar] [CrossRef]
- Schmidt, M.; Zogheib, E.; Roze, H.; Repesse, X.; Lebreton, G.; Luyt, C.E.; Trouillet, J.L.; Brechot, N.; Nieszkowska, A.; Dupont, H.; et al. The PRESERVE mortality risk score and analysis of long-term outcomes after extracorporeal membrane oxygenation for severe acute respiratory distress syndrome. Intensive Care Med. 2013, 39, 1704–1713. [Google Scholar] [CrossRef] [PubMed]
- Benchimol, E.I.; Smeeth, L.; Guttmann, A.; Harron, K.; Moher, D.; Petersen, I.; Sorensen, H.T.; Von Elm, E.; Langan, S.M.; Committee, R.W. The REporting of studies Conducted using Observational Routinely-collected health Data (RECORD) statement. PLoS Med. 2015, 12, e1001885. [Google Scholar] [CrossRef] [PubMed]
- Sendagire, C.; Lipnick, M.S.; Kizito, S.; Kruisselbrink, R.; Obua, D.; Ejoku, J.; Ssemogerere, L.; Nakibuuka, J.; Kwizera, A. Feasibility of the modified sequential organ function assessment score in a resource-constrained setting: A prospective observational study. BMC Anesthesiol. 2017, 17, 12. [Google Scholar] [CrossRef] [Green Version]
- Vincent, J.L.; Rello, J.; Marshall, J.; Silva, E.; Anzueto, A.; Martin, C.D.; Moreno, R.; Lipman, J.; Gomersall, C.; Sakr, Y.; et al. International study of the prevalence and outcomes of infection in intensive care units. JAMA 2009, 302, 2323–2329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Combes, A.; Hajage, D.; Capellier, G.; Demoule, A.; Lavoue, S.; Guervilly, C.; Da Silva, D.; Zafrani, L.; Tirot, P.; Veber, B.; et al. Extracorporeal Membrane Oxygenation for Severe Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2018, 378, 1965–1975. [Google Scholar] [CrossRef] [PubMed]
- Henry, B.M. COVID-19, ECMO, and lymphopenia: A word of caution. Lancet Respir. Med. 2020, 8, e24. [Google Scholar] [CrossRef]
- Henry, B.M.; Lippi, G. Poor survival with extracorporeal membrane oxygenation in acute respiratory distress syndrome (ARDS) due to coronavirus disease 2019 (COVID-19): Pooled analysis of early reports. J. Crit. Care 2020, 58, 27–28. [Google Scholar] [CrossRef]
- Angouras, D.C.; Kollias, V.D.; Dougenis, D. Adding Inflammation to the Perfect Cytokine Storm: Concerns Related to Extracorporeal Membrane Oxygenation for COVID-19 Patients. ASAIO J. 2020, 66, e110. [Google Scholar] [CrossRef]
- Vincent, J.L.; Creteur, J. Ethical aspects of the COVID-19 crisis: How to deal with an overwhelming shortage of acute beds. Eur. Heart J. Acute Cardiovasc. Care 2020, 9, 248–252. [Google Scholar] [CrossRef]
- Ackermann, M.; Verleden, S.E.; Kuehnel, M.; Haverich, A.; Welte, T.; Laenger, F.; Vanstapel, A.; Werlein, C.; Stark, H.; Tzankov, A.; et al. Pulmonary Vascular Endothelialitis, Thrombosis, and Angiogenesis in Covid-19. N. Engl. J. Med. 2020, 383, 120–128. [Google Scholar] [CrossRef]
- Munshi, L.; Walkey, A.; Goligher, E.; Pham, T.; Uleryk, E.M.; Fan, E. Venovenous extracorporeal membrane oxygenation for acute respiratory distress syndrome: A systematic review and meta-analysis. Lancet Respir. Med. 2019, 7, 163–172. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Center | Country | Number of Cases |
|---|---|---|
| Methodist Hospital, San Antonio, Texas | United States | 21 |
| University Clinic Freiburg | Germany | 15 |
| Hôpital Erasme—ULB, Brussels | Belgium | 15 |
| Clinic Heilbronn | Germany | 14 |
| Clinic Ludwigsburg | Germany | 11 |
| Saarland University Medical Center | Germany | 9 |
| University Clinic Zurich | Switzerland | 9 |
| Clinic Ibbenbueren * | Germany | 8 |
| University Clinic Halle (Saale) | Germany | 8 |
| University of Pittsburgh Medical Center (UPMC) | United States | 8 |
| UCLA Healthcare System, Los Angeles | United States | 5 |
| LMU Hospital Munich | Germany | 4 |
| Istituto Clinico Sant’Ambrogio, University of Milan | Italy | 3 |
| Marien Hospital Hamburg | Germany | 2 |
| Asklepios Clinic North, Hamburg | Germany | 1 |
| Total number of cases | 133 | |
| Total | Non-Survivors (n = 58) | Survivors (n = 69) | p | |
|---|---|---|---|---|
| Patients | ||||
| Number of patients, No. (%) | 127 (100) | 58 (46) | 69 (54) | -- |
| Female sex, No. (%) | 27 (21) | 10 (17) | 17 (25) | 0.314 |
| Age [years], median (IQR) | 59 (53–66) | 61 (54–70) | 58 (51–64) | 0.019 |
| BMI [kg/m2], median (IQR) | 29 (26–35) | 29 (26–35) | 30 (25–34.4) | 0.701 |
| Evidence of SARS-CoV-2 (PCR), No. (%) | 127 (100) | 58 (100) | 69 (100) | -- |
| Ventilation parameters and blood gas analysis before ECMO, median (IQR) | ||||
| FiO2 [%] | 100 (80–100) | 100 (80–100) | 96 (80–100) | 0.929 |
| PEEP [mbar] | 14 (10–16) | 15 (10–17) | 13 (10–15) | 0.077 |
| Plateau pressure [mbar] | 32 (26–35) | 32 (28–35) | 32 (24.5–34) | 0.116 |
| Driving pressure [mbar] | 17 (13–21) | 17 (13.75–21.25) | 16 (12.5–20) | 0.283 |
| Breathing rate [1/min] | 25 (21–30) | 25.5 (20.5–32.5) | 24 (20.5–30) | 0.372 |
| pH | 7.3 (7.2–7.5) | 7.3 (7.2–7.4) | 7.3 (7.2–7.4) | 0.980 |
| pO2 [mmHg] | 64 (52–76) | 64 (53–78) | 64 (52–76) | 0.867 |
| pCO2 [mmHg] | 57 (45–67) | 58 (45–70) | 57 (44–64) | 0.290 |
| PaO2/FiO2 [mmHg] | 70.2 (57.1–97.1) | 72.05 (56.6–94.5) | 70.2 (57.1–99.3) | 0.984 |
| Pre-existing conditions, No. (%) | ||||
| Heart failure NYHA IV | 3 (2) | 3 (5) | 0 (0) | 0.056 |
| Chronic lung disease | 13 (10) | 9 (16) | 4 (6) | 0.072 |
| Dialysis-dependent kidney failure | 11 (9) | 4 (7) | 7 (10) | 0.517 |
| Hematologic malignancy | 6 (5) | 4 (7) | 2 (3) | 0.290 |
| Solid malignant tumor | 3 (2) | 2 (3) | 1 (1) | 0.460 |
| Metastatic cancer | 1 (1) | 0 (0) | 1 (1) | 0.357 |
| Solid organ transplant | 0 (0) | 0 (0) | 0 (0) | -- |
| HIV | 1 (1) | 1 (2) | 0 (0) | 0.274 |
| Liver cirrhosis | 0 (0) | 0 (0) | 0 (0) | -- |
| Immunosuppressive therapy | 8 (6) | 5 (9) | 3 (4) | 0.324 |
| Intensive care and ARDS treatment, No. (%) | ||||
| Prone positioning before ECMO | 94 (74) | 45 (78) | 49 (71) | 0.404 |
| Duration of invasive ventilation before ECMO [days], median (IQR) | 5.0 (2.0–9.0) | 6.0 (3.75–11.25) | 3.0 (1.0–8.0) | 0.006 |
| Nitric oxide use before ECMO | 6 (5) | 4 (7) | 2 (3) | 0.290 |
| Bicarbonate use before ECMO | 11 (9) | 7 (12) | 4 (6) | 0.211 |
| Neuromuscular blockers before ECMO | 67 (53) | 33 (57) | 34 (49) | 0.392 |
| On day 30 after ECMO initiation still on ECMO | 24 (19) | 0 (0) | 24 (35) | -- |
| On day 30 after ECMO initiation still on ICU | 47 (37) | 0 (0) | 47 (68) | -- |
| Renal replacement therapy before ECMO | 24 (19) | 11 (19) | 13 (19) | 0.986 |
| Renal replacement therapy during ECMO | 73 (57) | 38 (66) | 33 (48) | 0.016 |
| Scores, median (IQR) | ||||
| SOFA | 9 (7–10) | 9 (8–11) | 9 (6–10) | 0.045 |
| RESP | 1 (0–4) | 1 (-1–2) | 2 (0–4) | 0.051 |
| PRESERVE | 4 (3–5) | 4 (3–5) | 3 (2–5) | 0.389 |
| SAPS II | 36 (29–44) | 38.5 (30–48) | 34 (28–41) | 0.042 |
| APACHE II | 17 (12–21) | 17 (12–22) | 16 (12–20) | 0.164 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Supady, A.; DellaVolpe, J.; Taccone, F.S.; Scharpf, D.; Ulmer, M.; Lepper, P.M.; Halbe, M.; Ziegeler, S.; Vogt, A.; Ramanan, R.; et al. Outcome Prediction in Patients with Severe COVID-19 Requiring Extracorporeal Membrane Oxygenation—A Retrospective International Multicenter Study. Membranes 2021, 11, 170. https://doi.org/10.3390/membranes11030170
Supady A, DellaVolpe J, Taccone FS, Scharpf D, Ulmer M, Lepper PM, Halbe M, Ziegeler S, Vogt A, Ramanan R, et al. Outcome Prediction in Patients with Severe COVID-19 Requiring Extracorporeal Membrane Oxygenation—A Retrospective International Multicenter Study. Membranes. 2021; 11(3):170. https://doi.org/10.3390/membranes11030170
Chicago/Turabian StyleSupady, Alexander, Jeff DellaVolpe, Fabio Silvio Taccone, Dominik Scharpf, Matthias Ulmer, Philipp M. Lepper, Maximilian Halbe, Stephan Ziegeler, Alexander Vogt, Raj Ramanan, and et al. 2021. "Outcome Prediction in Patients with Severe COVID-19 Requiring Extracorporeal Membrane Oxygenation—A Retrospective International Multicenter Study" Membranes 11, no. 3: 170. https://doi.org/10.3390/membranes11030170
APA StyleSupady, A., DellaVolpe, J., Taccone, F. S., Scharpf, D., Ulmer, M., Lepper, P. M., Halbe, M., Ziegeler, S., Vogt, A., Ramanan, R., Boldt, D., Stecher, S. -S., Montisci, A., Spangenberg, T., Marggraf, O., Kunavarapu, C., Peluso, L., Muenz, S., Buerle, M., ... Staudacher, D. L. (2021). Outcome Prediction in Patients with Severe COVID-19 Requiring Extracorporeal Membrane Oxygenation—A Retrospective International Multicenter Study. Membranes, 11(3), 170. https://doi.org/10.3390/membranes11030170