
Locked Away—Prophylaxis and Management of Catheter Related Thrombosis in Hemodialysis

 , ,
, , 
Abstract
:1. Introduction
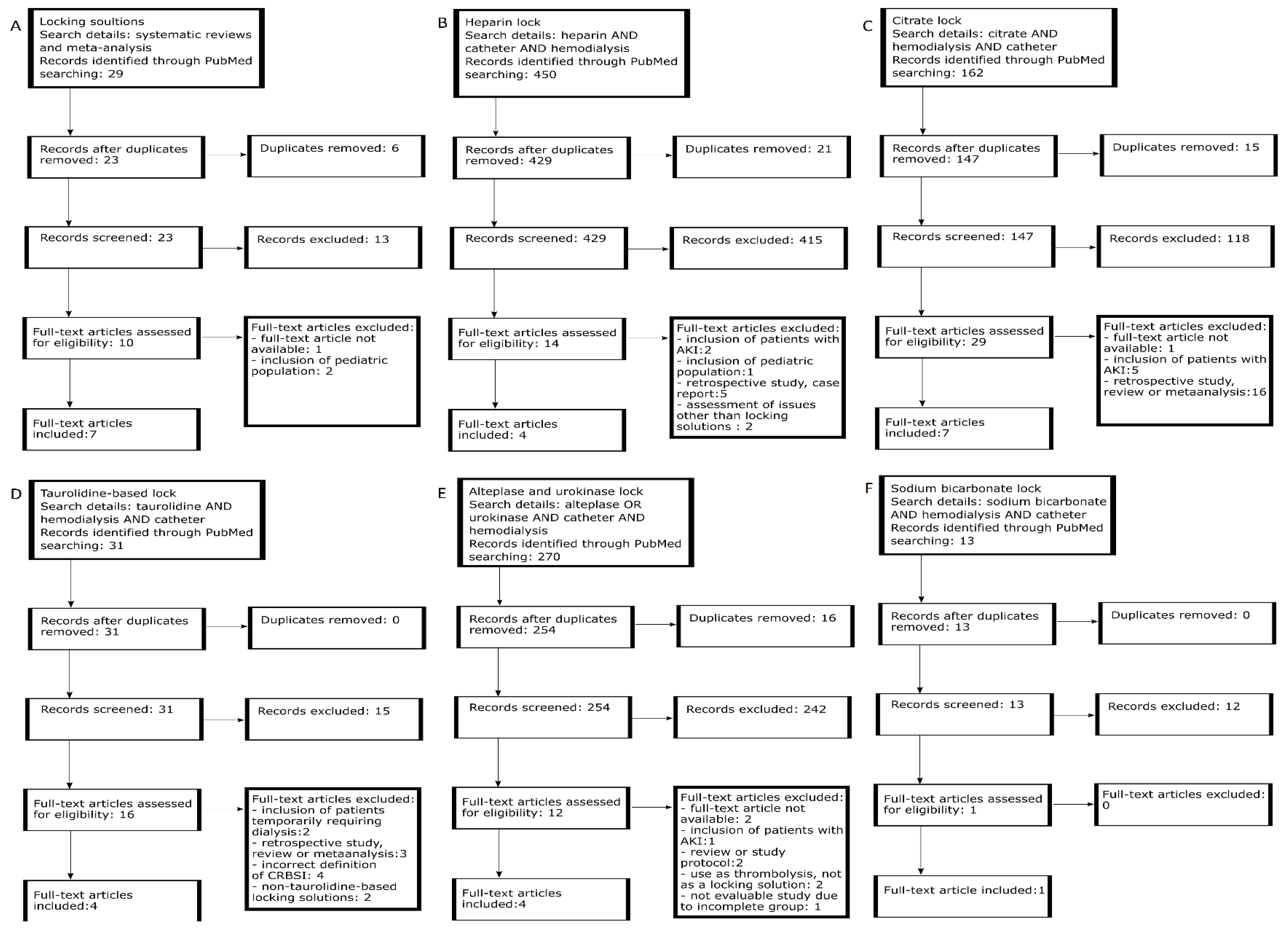
2. Materials and Methods
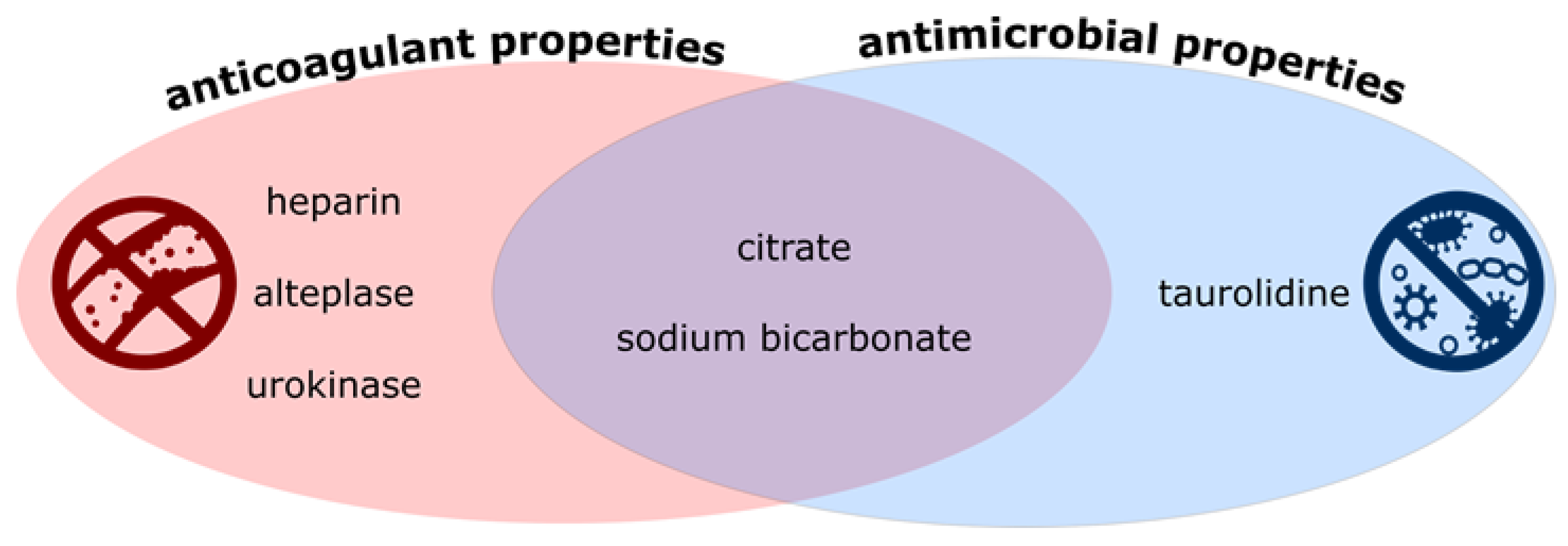
3. Heparin
4. Trisodium Citrate
5. Taurolidine
6. Alteplase and Urokinase
7. Sodium Bicarbonate
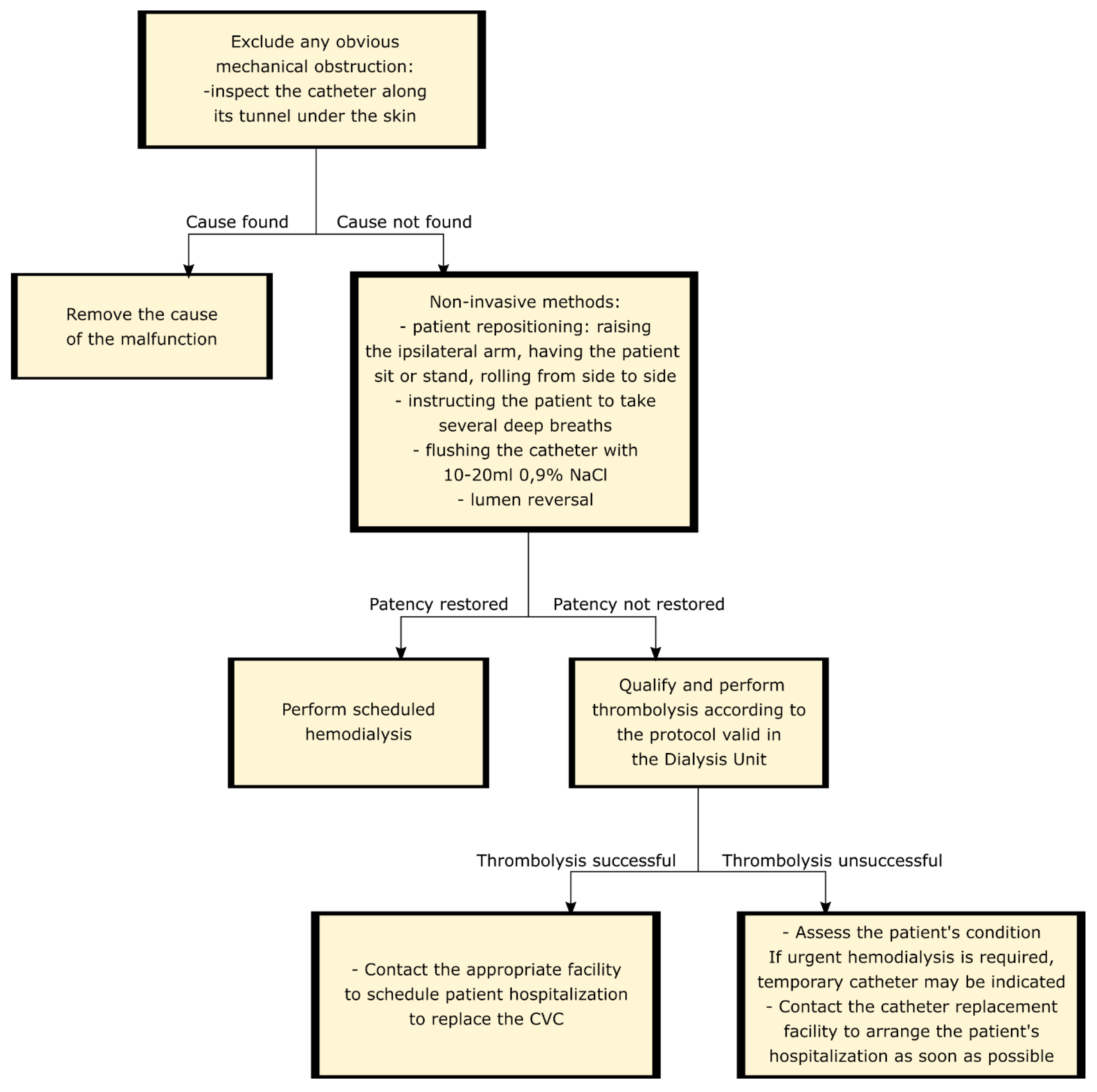
8. Management of Catheter Dysfunction
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lok, C.E.; Huber, T.S.; Lee, T.; Shenoy, S.; Yevzlin, A.S.; Abreo, K.; Allon, M.; Asif, A.; Astor, B.C.; Glickman, M.H.; et al. KDOQI Clinical Practice Guideline for Vascular Access: 2019 Update. Am. J. Kidney Dis. 2020, 75, S1–S164. [Google Scholar] [CrossRef] [Green Version]
- MAHTA Sp. z o.o.; Gellert, R.; Kalinowska, A.; Kowalczyk, M.; Pruszko, C.; Prystacki, T. Dostęp do Świadczeń Nefrologicznych w Polsce; M AHTA Sp. z o.o.: Jozefow, Poland, 2019. [Google Scholar]
- Pisoni, R.L.; Zepel, L.; Port, F.K.; Robinson, B.M. Trends in US Vascular Access Use, Patient Preferences, and Related Practices: An Update from the US DOPPS Practice Monitor with International Comparisons. Am. J. Kidney Dis. 2015, 65, 905–915. [Google Scholar] [CrossRef] [PubMed]
- Ling, X.-C.; Lu, H.-P.; Loh, E.-W.; Lin, Y.-K.; Li, Y.-S.; Lin, C.-H.; Ko, Y.-C.; Wu, M.-Y.; Lin, Y.-F.; Tam, K.-W. A Systematic Review and Meta-Analysis of the Comparison of Performance among Step-Tip, Split-Tip, and Symmetrical-Tip Hemodialysis Catheters. J. Vasc. Surg. 2019, 69, 1282–1292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wadełek, J. Centralne Cewniki Do Hemodializy. Forum Nefrol. 2020, 13, 14–21. [Google Scholar]
- Chapla, K.; Oza-Gajera, B.P.; Yevzlin, A.S.; Shin, J.-I.; Astor, B.C.; Chan, M.R. Hemodialysis Catheter Locking Solutions and the Prevention of Catheter Dysfunction: A Meta-Analysis. J. Vasc. Access 2015, 16, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Niyyar, V.D. Catheter Dysfunction and Lock Solutions: Are We There Yet? Nephrol. Dial. Transplant. 2019, 34, 1626–1628. [Google Scholar] [CrossRef] [PubMed]
- Labriola, L.; Crott, R.; Jadoul, M. Preventing Haemodialysis Catheter-Related Bacteraemia with an Antimicrobial Lock Solution: A Meta-Analysis of Prospective Randomized Trials. Nephrol. Dial. Transplant. 2008, 23, 1666–1672. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jaffer, Y.; Selby, N.M.; Taal, M.W.; Fluck, R.J.; McIntyre, C.W. A Meta-Analysis of Hemodialysis Catheter Locking Solutions in the Prevention of Catheter-Related Infection. Am. J. Kidney Dis. 2008, 51, 233–241. [Google Scholar] [CrossRef] [Green Version]
- Grudzinski, A.; Agarwal, A.; Bhatnagar, N.; Nesrallah, G. Benefits and Harms of Citrate Locking Solutions for Hemodialysis Catheters: A Systematic Review and Meta-Analysis. Can. J. Kidney Health Dis. 2015, 2. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Ivany, J.N.; Perkovic, V.; Gallagher, M.P.; Woodward, M.; Jardine, M.J. Anticoagulants and Antiplatelet Agents for Preventing Central Venous Haemodialysis Catheter Malfunction in Patients with End-stage Kidney Disease. Cochrane Database Syst. Rev. 2016, 2016. [Google Scholar] [CrossRef]
- Zhao, Y.; Li, Z.; Zhang, L.; Yang, J.; Yang, Y.; Tang, Y.; Fu, P. Citrate versus Heparin Lock for Hemodialysis Catheters: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Am. J. Kidney Dis. 2014, 63, 479–490. [Google Scholar] [CrossRef] [Green Version]
- Sheng, K.X.; Zhang, P.; Li, J.W.; Cheng, J.; He, Y.C.; Böhlke, M.; Chen, J.H. Comparative Efficacy and Safety of Lock Solutions for the Prevention of Catheter-Related Complications Including Infectious and Bleeding Events in Adult Haemodialysis Patients: A Systematic Review and Network Meta-Analysis. Clin. Microbiol. Infect. 2020, 26, 545–552. [Google Scholar] [CrossRef]
- Lok, C.E.; Appleton, D.; Bhola, C.; Khoo, B.; Richardson, R.M.A. Trisodium Citrate 4%-an Alternative to Heparin Capping of Haemodialysis Catheters. Nephrol. Dial. Transplant. 2007, 22, 477–483. [Google Scholar] [CrossRef] [Green Version]
- Allon, M. Quantification of Complications of Tunneled Hemodialysis Catheters. Am. J. Kidney Dis. 2019, 73, 462–464. [Google Scholar] [CrossRef] [Green Version]
- Hryszko, T.; Brzosko, S.; Mysliwiec, M. Low concentration of heparin used for permanent catheters canal locking is effective and diminishes the risk of bleeding. Int. Urol. Nephrol. 2013, 45, 825–829. [Google Scholar] [CrossRef] [Green Version]
- Chu, G.; Fogarty, G.M.; Avis, L.F.; Bergin, S.; McElduff, P.; Gillies, A.H.; Choi, P. Low dose heparin lock (1000 U/mL) maintains tunnelled hemodialysis catheter patency when compared with high dose heparin (5000 U/mL): A randomised controlled trial. Hemodial. Int. 2016, 20, 385–391. [Google Scholar] [CrossRef] [PubMed]
- Karaaslan, H.; Peyronnet, P.; Benevent, D.; Lagarde, C.; Rince, M.; Leroux-Robert, C. Risk of heparin lock-related bleeding when using indwelling venous catheter in haemodialysis. Nephrol. Dial. Transplant. 2001, 16, 2072–2074. [Google Scholar] [CrossRef] [PubMed]
- Agharazii, M.; Plamondon, I.; Lebel, M.; Douville, P.; Desmeules, S. Estimation of heparin leak into the systemic circulation after central venous catheter heparin lock. Nephrol. Dial. Transplant. 2005, 20, 1238–1240. [Google Scholar] [CrossRef] [Green Version]
- Shanks, R.M.Q.; Sargent, J.L.; Martinez, R.M.; Graber, M.L.; O’Toole, G.A. Catheter lock solutions influence staphylococcal biofilm formation on abiotic surfaces. Nephrol. Dial. Transplant. 2006, 21, 2247–2255. [Google Scholar] [CrossRef] [Green Version]
- Barcellos, F.C.; Nunes, B.P.; Valle, L.J.; Lopes, T.; Orlando, B.; Scherer, C.; Nunes, M.; Duarte, G.A.; Böhlke, M. Comparative effectiveness of 30 % trisodium citrate and heparin lock solution in preventing infection and dysfunction of hemodialysis catheters: A randomized controlled trial (CITRIM trial). Infection 2016, 45, 139–145. [Google Scholar] [CrossRef]
- Polkinghorne, K.R. How Can the Complications of Central Vein Catheters Be Reduced? Semin. Dial. 2016, 29, 197–198. [Google Scholar] [CrossRef]
- Luiz, M.V.S.J.; Scavone, C.; Tzanno, C. The CLOCK trial, a double-blinded randomized controlled trial: Trisodium citrate 30% and minocycline 3 mg/mL plus EDTA 30 mg/mL are effective and safe for catheter patency maintenance among CKD 5D patients on hemodialysis. Hemodial. Int. 2016, 21, 294–304. [Google Scholar] [CrossRef]
- Schilcher, G.; Scharnagl, H.; Horina, J.H.; Ribitsch, W.; Rosenkranz, A.R.; Stojakovic, T.; Polaschegg, H.-D. Trisodium citrate induced protein precipitation in haemodialysis catheters might cause pulmonary embolism. Nephrol. Dial. Transplant. 2012, 27, 2953–2957. [Google Scholar] [CrossRef] [Green Version]
- Power, A.; Duncan, N.; Singh, S.K.; Brown, W.; Dalby, E.; Edwards, C.; Lynch, K.; Prout, V.; Cairns, T.; Griffith, M.; et al. Sodium Citrate versus Heparin Catheter Locks for Cuffed Central Venous Catheters: A Single-Center Randomized Controlled Trial. Am. J. Kidney Dis. 2009, 53, 1034–1041. [Google Scholar] [CrossRef] [Green Version]
- Meeus, G.; Kuypers, D.R.; Claes, K.; Evenepoel, P.; Maes, B.; Vanrenterghem, Y. A Prospective, Randomized, Double-Blind Crossover Study on the Use of 5% Citrate Lock versus 10% Citrate Lock in Permanent Hemodialysis Catheters. Blood Purif. 2005, 23, 101–105. [Google Scholar] [CrossRef]
- Macrae, J.M.; Dojcinovic, I.; Djurdjev, O.; Jung, B.; Shalansky, S.; Levin, A.; Kiaii, M. Citrate 4% versus Heparin and the Reduction of Thrombosis Study (CHARTS). Clin. J. Am. Soc. Nephrol. 2008, 3, 369–374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gallieni, M.; Giordano, A.; Rossi, U.; Cariati, M. Optimization of Dialysis Catheter Function. J. Vasc. Access 2016, 17, S42–S46. [Google Scholar] [CrossRef]
- Hendrickx, L.; Kuypers, D.; Evenepoel, P.; Maes, B.; Messiaen, T.; Vanrenterghem, Y. A comparative prospective study on the use of low concentrate citrate lock versus heparin lock in permanent dialysis catheters. Int. J. Artif. Organs 2001, 24, 208–211. [Google Scholar] [CrossRef]
- Vanholder, R.; Canaud, B.; Fluck, R.; Jadoul, M.; Labriola, L.; Marti-Monros, A.; Tordoir, J.; van Biesen, W. Diagnosis, prevention and treatment of haemodialysis catheter-related bloodstream infections (CRBSI): A position statement of European Renal Best Practice (ERBP). Clin. Kidney J. 2010, 3, 234–246. [Google Scholar] [CrossRef]
- Hernández, M.J.; Soriano, A.; Filella, X.; Calvo, M.; Coll, E.; Rebled, J.M.; Poch, E.; Graterol, F.; Compte, M.T.; Maduell, F.; et al. Impact of locking solutions on conditioning biofilm formation in tunnelled haemodialysis catheters and inflammatory response activation. J. Vasc. Access 2020. [Google Scholar] [CrossRef]
- Liu, H.; Liu, H.; Deng, J.; Chen, L.; Yuan, L.; Wu, Y. Preventing Catheter-Related Bacteremia with Taurolidine-Citrate Catheter Locks: A Systematic Review and Meta-Analysis. Blood Purif. 2014, 37, 179–187. [Google Scholar] [CrossRef]
- Winnicki, W.; Herkner, H.; Lorenz, M.; Handisurya, A.; Kikić, Ž.; Bielesz, B.; Schairer, B.; Reiter, T.; Eskandary, F.; Sunder-Plassmann, G.; et al. Taurolidine-based catheter lock regimen significantly reduces overall costs, infection, and dysfunction rates of tunneled hemodialysis catheters. Kidney Int. 2018, 93, 753–760. [Google Scholar] [CrossRef]
- Al-Ali, F.; Hamdy, A.F.; Hamad, A.; Elsayed, M.; Iqbal, Z.Z.; Elsayed, A.; Ibrahim, R.; Tolba, H.; Buanan, H.; Fawzy, A. Safety and efficacy of taurolidine/urokinase versus taurolidine/heparin as a tunneled catheter lock solution in hemodialysis patients: A prospective, randomized, controlled study. Nephrol. Dial. Transplant. 2017, 33, 619–626. [Google Scholar] [CrossRef] [Green Version]
- Reidenberg, B.E.; Wanner, C.; Polsky, B.; Castanheira, M.; Shelip, A.; Stalleicken, D.; Pfaffle, A.E. Postmarketing experience with Neutrolin® (taurolidine, heparin, calcium citrate) catheter lock solution in hemodialysis patients. Eur. J. Clin. Microbiol. Infect. Dis. 2017, 37, 661–663. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hemmelgarn, B.R.; Manns, B.J.; Soroka, S.D.; Levin, A.; Macrae, J.; Tennankore, K.; Wilson, J.-A.S.; Weaver, R.G.; Ravani, P.; Quinn, R.R.; et al. Effectiveness and Cost of Weekly Recombinant Tissue Plasminogen Activator Hemodialysis Catheter Locking Solution. Clin. J. Am. Soc. Nephrol. 2018, 13, 429–435. [Google Scholar] [CrossRef] [Green Version]
- Hemmelgarn, B.R.; Moist, L.M.; Lok, C.E.; Tonelli, M.; Manns, B.J.; Holden, R.M.; Leblanc, M.; Faris, P.; Barre, P.; Zhang, J.; et al. Prevention of Dialysis Catheter Malfunction with Recombinant Tissue Plasminogen Activator. N. Engl. J. Med. 2011, 364, 303–312. [Google Scholar] [CrossRef] [PubMed]
- Schenk, P.; Rosenkranz, A.R.; Wölfl, G.; Hörl, W.H.; Traindl, O. Recombinant tissue plasminogen activator is a useful alternative to heparin in priming Quinton Permcath. Am. J. Kidney Dis. 2000, 35, 130–136. [Google Scholar] [CrossRef]
- Manns, B.J.; Scott-Douglas, N.; Tonelli, M.; Ravani, P.; Leblanc, M.; Dorval, M.; Holden, R.; Moist, L.; Lok, C.; Zimmerman, D.; et al. An Economic Evaluation of rt-PA Locking Solution in Dialysis Catheters. J. Am. Soc. Nephrol. 2014, 25, 2887–2895. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El-Hennawy, A.S.; Frolova, E.; A Romney, W. Sodium bicarbonate catheter lock solution reduces hemodialysis catheter loss due to catheter-related thrombosis and blood stream infection: An open-label clinical trial. Nephrol. Dial. Transplant. 2019, 34, 1739–1745. [Google Scholar] [CrossRef]
- Poinen, K.; Quinn, R.R.; Clarke, A.; Ravani, P.; Hiremath, S.; Miller, L.M.; Blake, P.G.; Oliver, M.J. Complications from Tunneled Hemodialysis Catheters: A Canadian Observational Cohort Study. Am. J. Kidney Dis. 2019, 73, 467–475. [Google Scholar] [CrossRef] [PubMed]
- Moist, L.M. How Can the Complications of Central Vein Catheters Be Reduced? Treating and Preventing Catheter Malfunction. Semin. Dial. 2016, 29, 199–200. [Google Scholar] [CrossRef] [PubMed]
- Goossens, G.A. Flushing and Locking of Venous Catheters: Available Evidence and Evidence Deficit. Nurs. Res. Pr. 2015, 2015, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Kumwenda, M.; Dougherty, L.; Spooner, H.; Jackson, V.; Mitra, S.; Inston, N. Managing dysfunctional central venous access devices: A practical approach to urokinase thrombolysis. Br. J. Nurs. 2018, 27, 4. [Google Scholar] [CrossRef] [PubMed]
- Baskin, J.L.; Pui, C.-H.; Reiss, U.; A Wilimas, J.; Metzger, M.L.; Ribeiro, R.C.; Howard, S.C. Management of occlusion and thrombosis associated with long-term indwelling central venous catheters. Lancet 2009, 374, 159–169. [Google Scholar] [CrossRef] [Green Version]
- Salgado, O.J. Vascular Access for Hemodialysis—Overview and Emphasis on Complications. In Hemodialysis; Suzuki, H., Ed.; InTechOpen: London, UK, 2013; ISBN 978-953-51-0988-4. [Google Scholar] [CrossRef] [Green Version]
- El-Masri, M.M.; El-Nekidy, W.S.; Soong, D.; Kadri, A. Efficacy of alteplase 1 versus 2 mg dose in restoring haemodialysis catheter function (Alte-dose 2): A randomized double-blind controlled study. Nephrology 2019, 25, 491–496. [Google Scholar] [CrossRef]
- Macrae, J.M.; Loh, G.; Djurdjev, O.; Shalansky, S.; Werb, R.; Levin, A.; Kiaii, M. Short and long alteplase dwells in dysfunctional hemodialysis catheters. Hemodial. Int. 2005, 9, 189–195. [Google Scholar] [CrossRef]
- Zacharias, J.M.; Weatherston, C.P.; Spewak, C.R.; Vercaigne, L.M. Alteplase versus Urokinase for Occluded Hemodialysis Catheters. Ann. Pharmacother. 2003, 37, 27–33. [Google Scholar] [CrossRef]
- Van Hulle, F.; Bonkain, F.; de Clerck, D.; Aerden, D.; Vanwijn, I.; Tielemans, C.; Wissing, K.M. Efficacy of urokinase lock to treat thrombotic dysfunction of tunneled hemodialysis catheters: A retrospective cohort study. J. Vasc. Access 2019, 20, 60–69. [Google Scholar] [CrossRef] [PubMed]
- Hilleman, D.; Campbell, J. Efficacy, Safety, and Cost of Thrombolytic Agents for the Management of Dysfunctional Hemodialysis Catheters: A Systematic Review. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2011, 31, 1031–1040. [Google Scholar] [CrossRef]
- Kennard, A.L.; Walters, G.D.; Jiang, S.; Talaulikar, G.S. Interventions for treating central venous haemodialysis catheter malfunction. Cochrane Database Syst. Rev. 2017, 2017, CD011953. [Google Scholar] [CrossRef]
- Little, M.A.; Walshe, J. A longitudinal study of the repeated use of alteplase as therapy for tunneled hemodialysis catheter dysfunction. Am. J. Kidney Dis. 2002, 39, 86–91. [Google Scholar] [CrossRef]
- Twardowski, Z.J. The clotted central vein catheter for haemodialysis. Nephrol. Dial. Transplant. 1998, 13, 2203–2206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, T.; Lok, C.; Vazquez, M.; Moist, L.; Maya, I.; Mokrzycki, M. Minimizing Hemodialysis Catheter Dysfunction: An Ounce of Prevention. Int. J. Nephrol. 2012, 2012, 170857. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Citation | Review Type/Reporting Quality | Description | Key Findings/Conclusions |
|---|---|---|---|
| Hemodialysis catheter locking solutions and the prevention of catheter dysfunction: a meta-analysis [6] | -meta-analysis -met 23 of 24 PRISMA items for meta-analysis | - both tunneled and nontunneled CVC included - both acute and chronic hemodialysis included - only catheter dysfunction assessment - locking solutions included: heparin, citrate (concentrations 2.2–46.7%); rtPA, ethanol, cefotaxime+heparin, tauroldine+citrate, hypertonic saline+heparin - included RCTs and observational studies published from 1980 to December 2013 - met PRISMA reporting criteria except for absence of protocol and registration | -no significant difference in catheter patency between heparin versus any other lock solutions -no statistically significant difference in catheter patency per 1000 days, catheter exchange or use of thrombolytic therapy when comparing locking solutions |
| Preventing haemodialysis catheter-related bacteraemia with an antimicrobial lock solution: a meta-analysis of prospective randomized trials [8] | -meta-analysis -met 23 of 24 PRISMA items for meta-analysis | - both tunneled and nontunneled CVC included - both acute and chronic hemodialysis included - only CRBSI assessment - locking solutions included: heparin 5000 U/mL vs. antimicrobial lock solution (ALS) (i.e.: gentamicin-citrate, gentamicin-heparin, taurolidine-citrate, minocycline-EDTA, citrate 30%, cefotaxime-heparin, cefazolin-gentamicin-heparin - included RCTs and observational studies published from 1999 to March 2007 - met PRISMA reporting criteria except for absence of protocol and registration | - use of an antimicrobial lock solution decreases the risk of CRBSI by approximately a factor 3. Although the under-representation of small studies with a non-significant or negative effect suggests an overestimation of the effect of ALS - no difference between tunneled and nontunneled CVC, possibly because of the under-representation of nontunneled CVC |
| A meta-analysis of hemodialysis catheter locking solutions in the prevention of catheter-related infection [9] | - meta-analysis -met 22 of 24 PRISMA items for meta-analysis | - both tunneled and nontunneled CVC included - both acute and chronic hemodialysis included - CRBSI and CRT assessment - locking solutions included: heparin 5000 U/mL or 1000 U/mL vs. antimicrobial lock solution (i.e.,: gentamicin, cefotaxime, minocycline, cefazolin, taurolidine-citrate, 30% citrate) - met PRISMA reporting criteria except for absence of protocol and registration, and assessment of the risk of bias in individual studies | - CRBSI was 7.72 times less likely when using ALS. Rates of catheter thrombosis did not increase - limitations are short duration of follow-up of the included studies and inclusion of both acute and chronic hemodialysis patients |
| Benefits and harms of citrate locking solutions for hemodialysis catheters: a systematic review and meta-analysis [10] | - meta-analysis -met 24 of 24 PRISMA items for meta-analysis | - both tunneled and nontunneled CVC included - both acute and chronic hemodialysis included - citrate locking solutions (not combined with other agents) vs heparin - all-cause mortality, bacteremia rates, all-cause hospitalization rates, access-related hospitalization, catheter replacement/exchange events, bleeding, and local/in situ thrombolysis assessment - included RCTs and observational studies published from inception to June 2013 | - low overall quality of evidence due to heterogeneity and small sample sizes - significantly lower risk of bleeding in citrate group - rates of death and bacteremia tended to be lower with citrate but not statistically significant - no difference in hospitalization or patency-related outcomes |
| Anticoagulants and antiplatelet agents for preventing central venous haemodialysis catheter malfunction in patients with end-stage kidney disease [11] | - meta-analysis -met 24 of 24 PRISMA items for meta-analysis | - both tunneled and nontunneled CVC included - chronic hemodialysis - locking solutions included: heparin 5000 U/mL, low or no dose heparin, alternative anticoagulant locking solutions (i.e.,: citrates, antibiotic locking solutions, rt-PA, ethanol) - also systemic agents included - CVC malfunction, CRBSI, all-cause mortality, adverse events assessment - included RCTs published to January 2016 | - among individual agents, only rt-PA reduced CVC malfunction (in 1 study) - low or no dose heparin may have the same efficacy in preventing catheter malfunction as 5000 U/mL - significant reduction on CRBSI for citrate, antibiotics, rt-PA, but not for ethanol or low dose heparin and systemic agents - additional use of antibiotic locks to citrate has no additional impact on CRBSI - no significant effect on all-cause mortality - reporting of safety outcomes was infrequent |
| Citrate versus heparin lock for hemodialysis catheters: a systematic review and meta-analysis of randomized controlled trials [12] | -meta-analysis -met 23 of 24 PRISMA items for meta-analysis | - both tunneled and nontunneled CVC included - both acute and chronic hemodialysis included - locking solutions compared: citrate locks vs heparin (5 studies); citrate+other antimicrobial solution vs heparin - CRBSI, exit-site infection, CRT assessment - included RCTs published to March 2013 - met PRISMA reporting criteria except for absence of protocol and registration | - citrate locks concentration 1–7% were associated with decreased CRBSI, whereas high concentrations (30–46.7%) had no effect - addition of antimicrobial substance to citrate was associated with decreased CRBSI - bleeding risk was lower for citrate than heparin - no difference in exit-site infection or CRT |
| Comparative efficacy and safety of lock solutions for the prevention of catheter-related complications including infectious and bleeding events in adult haemodialysis patients: a systematic review and network meta-analysis [13] | -meta-analysis -met 23 of 24 PRISMA items for meta-analysis | - both tunneled and nontunneled CVC included - both acute and chronic hemodialysis included - different locking solutions: heparin 5000 U/mL; low-dose heparin, antibiotics (e.g., cloxacillin, cefotaxime, linezolid, vancomycin, gentamicin) combined with anticoagulants (e.g., heparin, citrate, EDTA, urokinase) minocycline, taurolidine), ethanol - CRBSI, bleeding events, CVC malfunction, exit-site infection, all-cause mortality assessment - included RCTs published from the date of databases inception to August 2018 - met PRISMA reporting criteria except for absence results of individual studies | - ethanol and antibiotics combined with anticoagulant were more effective in preventing CRBSI compared to heparin - low-dose heparin and citrate had lower bleeding risk than heparin - using of gentamicin was connected to development of bacterial resistance after 6 months and to ototoxicity - no effect on CVC malfunction or all-cause mortality |
| Locking Solution | Vial Volume | Price in PLN/vial | Price in € |
|---|---|---|---|
| Heparin | 25,000 IU/5 mL | 15.04 | 3.3 |
| Citrate 4% | 5 mL | 9.91 | 2.17 |
| Citrate 30% | 5 mL | 7.64 | 1.67 |
| Citrate 46.7% | 5 mL | 11.78 | 2.58 |
| Taurolidine | 6 mL | 26.42 | 5.79 |
| Taurolidine+heparine 500 IU | 10 mL | 40.82 | 8.95 |
| Taurolidine+urokinase 25,000 IU | 5 mL | 146.72 | 32.15 |
| Alteplase 10 mg | 10 mg/10 mL | 553.39 | 121.28 |
| Urokinase | 250,000 IU | 627.41 | 137.5 |
| NaHCO3 | 20 mL | 3.40 | 0.75 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Szymańska, J.; Kakareko, K.; Rydzewska-Rosołowska, A.; Głowińska, I.; Hryszko, T. Locked Away—Prophylaxis and Management of Catheter Related Thrombosis in Hemodialysis. J. Clin. Med. 2021, 10, 2230. https://doi.org/10.3390/jcm10112230
Szymańska J, Kakareko K, Rydzewska-Rosołowska A, Głowińska I, Hryszko T. Locked Away—Prophylaxis and Management of Catheter Related Thrombosis in Hemodialysis. Journal of Clinical Medicine. 2021; 10(11):2230. https://doi.org/10.3390/jcm10112230
Chicago/Turabian StyleSzymańska, Joanna, Katarzyna Kakareko, Alicja Rydzewska-Rosołowska, Irena Głowińska, and Tomasz Hryszko. 2021. "Locked Away—Prophylaxis and Management of Catheter Related Thrombosis in Hemodialysis" Journal of Clinical Medicine 10, no. 11: 2230. https://doi.org/10.3390/jcm10112230
APA StyleSzymańska, J., Kakareko, K., Rydzewska-Rosołowska, A., Głowińska, I., & Hryszko, T. (2021). Locked Away—Prophylaxis and Management of Catheter Related Thrombosis in Hemodialysis. Journal of Clinical Medicine, 10(11), 2230. https://doi.org/10.3390/jcm10112230