



J. Clin. Med. 2023, 12(1), 265; https://doi.org/10.3390/jcm12010265 - 29 Dec 2022
Cited by 1 | Viewed by 2100
Abstract
►
Show Figures
Sudden cardiac death among hemodialysis patients is related to the hemodialysis schedule. Mortality is highest within 12 h before and after the first hemodialysis sessions of a week. We investigated the association of arrhythmia occurrence and heart rate variability (HRV) using an electrocardiogram
[...] Read more.
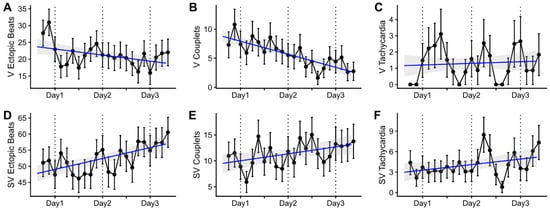
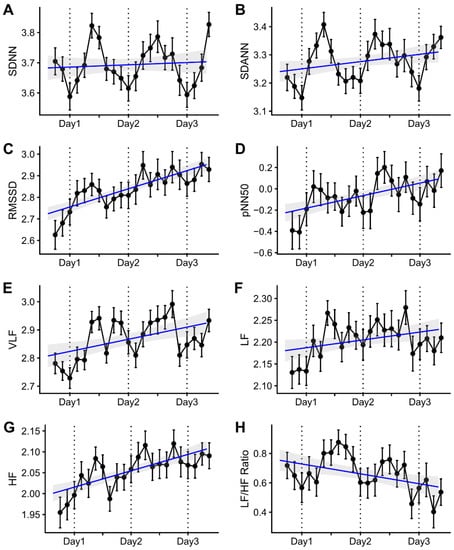
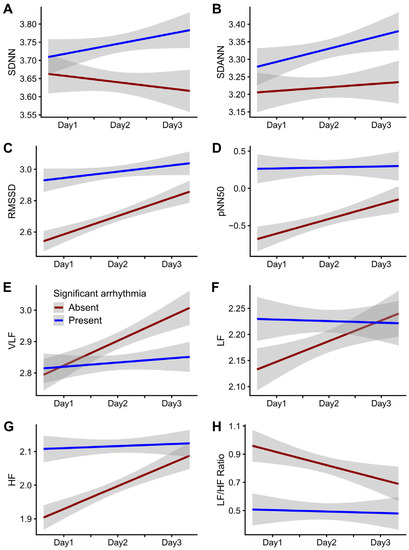
Sudden cardiac death among hemodialysis patients is related to the hemodialysis schedule. Mortality is highest within 12 h before and after the first hemodialysis sessions of a week. We investigated the association of arrhythmia occurrence and heart rate variability (HRV) using an electrocardiogram (ECG) monitoring patch during the long interdialytic interval in hemodialysis patients. This was a prospective observational study with 55 participants on maintenance hemodialysis for at least six months. A patch-type ECG monitoring device was applied to record arrhythmia events and HRV during 72 h of a long interdialytic period. Forty-nine participants with sufficient ECG data out of 55 participants were suitable for the analysis. The incidence of supraventricular tachycardia and ventricular tachycardia did not significantly change over time. The square root of the mean squared differences of successive NN intervals (RMSSD), the proportion of adjacent NN intervals differing by >50 ms (pNN50), and high-frequency (HF) increased during the long interdialytic interval. The gap in RMSSD, pNN50, HF, and the low-frequency/high-frequency (LF/HF) ratio between patients with and without significant arrhythmias increased significantly over time during the long interdialytic interval. The daily changes in RMSSD, pNN50, HF, and the LF/HF ratio were more prominent in patients without significant arrhythmias than in those with significant arrhythmias. The electrolyte fluctuation between post-hemodialysis and subsequent pre-hemodialysis was not considered in this study. The study results suggest that the decreased autonomic response during interdialytic periods in dialysis patients is associated with poor cardiac arrhythmia events.
Full article
Figure 1


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}