
Warning Signals of Post-Exertional Malaise in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: A Retrospective Analysis of 197 Patients

 and
and
Abstract
:1. Introduction
2. Patients and Methods
2.1. Ethics
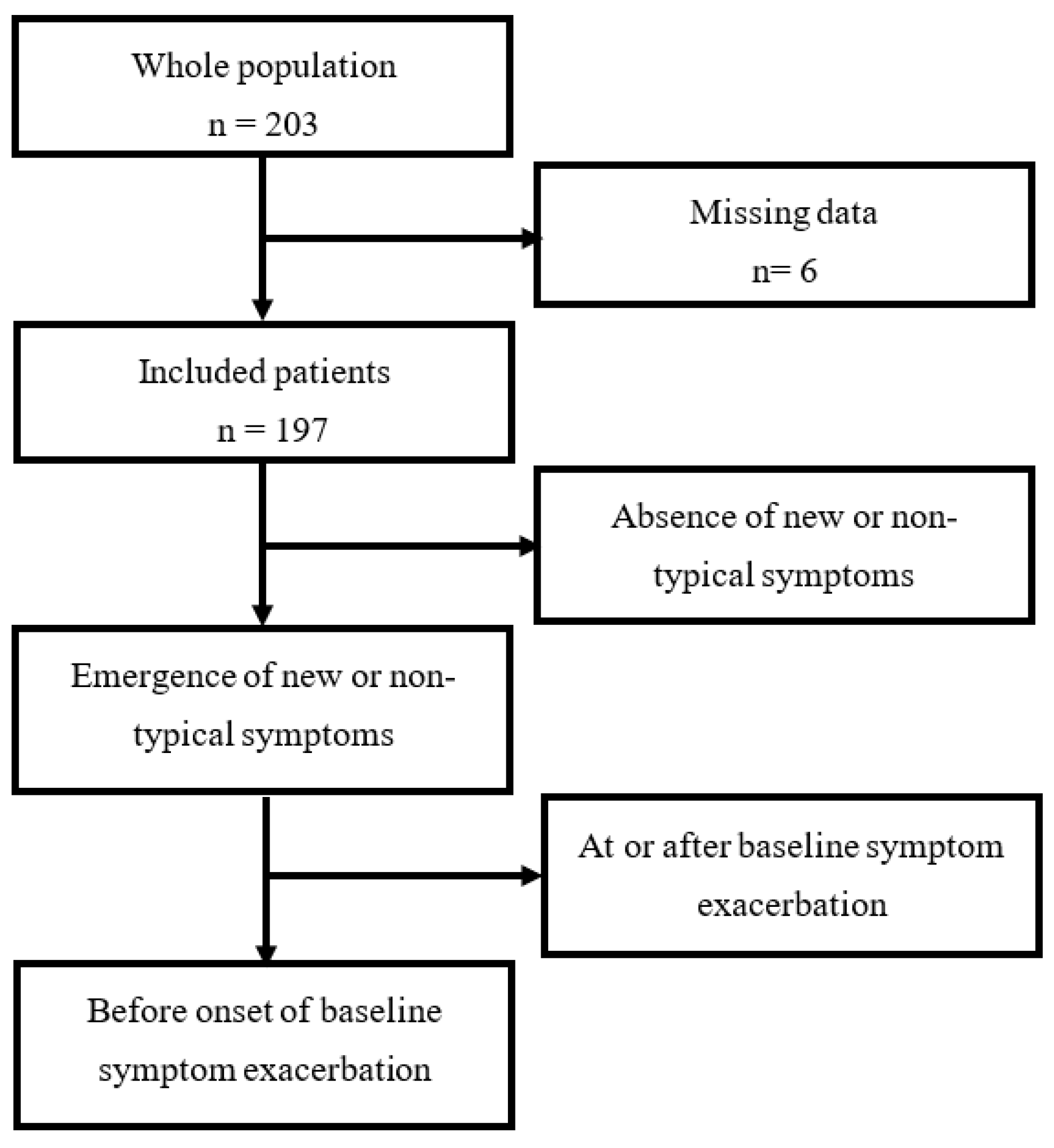
2.2. Study Population
2.3. Exclusion Criteria
2.4. Data Collection and Patients’ Grouping
2.5. Analysis of PEM Features
2.6. Assessment of PEM Severity
2.7. Fatigue Assessment
2.8. Statistical Analysis
3. Results
4. Discussion
Limitations and Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Carruthers, B.M.; van de Sande, M.I.; De Meirleir, K.L.; Klimas, N.G.; Broderick, G.; Mitchell, T.; Staines, D.; Powles, A.C.P.; Speight, N.; Vallings, R.; et al. Myalgic encephalomyelitis: International consensus criteria. J. Intern. Med. 2011, 270, 327–338. [Google Scholar] [CrossRef] [Green Version]
- Committee on the Diagnostic Criteria for Myalgic Encephalomyelitis/Chronic Fatigue Syndrome, Board on the Health of Select Populations, Institute of Medicine. Beyond Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Redefining an Illness; National Academies Press: Washington, DC, USA, 2015. Available online: http://www.ncbi.nlm.nih.gov/books/NBK274235/ (accessed on 22 February 2019).
- Prins, J.B.; van der Meer, J.W.M.; Bleijenberg, G. Chronic fatigue syndrome. Lancet 2006, 367, 346–355. [Google Scholar] [CrossRef]
- Collin, S.M.; Bakken, I.J.; Nazareth, I.; Crawley, E.; White, P.D. Health care resource use by patients before and after a diagnosis of chronic fatigue syndrome (CFS/ME): A clinical practice research datalink study. BMC Fam. Pract. 2017, 18, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Myalgic Encephalomyelitis/Chronic Fatigue Syndrome | NINDS Common Data Elements [Internet]. Available online: https://www.commondataelements.ninds.nih.gov/Myalgic%20Encephalomyelitis/Chronic%20Fatigue%20Syndrome (accessed on 25 May 2020).
- Morris, G.; Maes, M. Myalgic encephalomyelitis/chronic fatigue syndrome and encephalomyelitis disseminata/multiple sclerosis show remarkable levels of similarity in phenomenology and neuroimmune characteristics. BMC Med. 2013, 11, 205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leonard, A.J.; Marcie, L.Z.; Mark, A.Z. Myalgic encephalomyelitis: Symptoms and biomarkers. Curr. Neuropharmacol. 2015, 13, 701–734. [Google Scholar]
- Chu, L.; Valencia, I.J.; Garvert, D.W.; Montoya, J.G. Deconstructing post-exertional malaise in myalgic encephalomyelitis/chronic fatigue syndrome: A patient-centered, cross-sectional survey. PLoS ONE 2018, 13, e0197811. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holtzman, C.S.; Bhatia, S.; Cotler, J.; Jason, L.A. Assessment of post-exertional malaise (PEM) in patients with myalgic encephalomyelitis (ME) and chronic fatigue syndrome (CFS): A patient-driven survey. Diagnostics 2019, 9, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nyland, M.; Naess, H.; Birkeland, J.S.; Nyland, H. Longitudinal follow-up of employment status in patients with chronic fatigue syndrome after mononucleosis. BMJ Open 2014, 4, e005798. [Google Scholar] [CrossRef] [Green Version]
- Taylor, R.R.; Jason, L.A.; Curie, C.J. Prognosis of chronic fatigue in a community-based sample. Psychosom. Med. 2002, 64, 319–327. [Google Scholar] [CrossRef] [Green Version]
- Fava, G.A.; Kellner, R. Prodromal symptoms in affective disorders. Am. J. Psychiatry 1991, 148, 823–830. [Google Scholar] [PubMed]
- Kelman, L. The premonitory symptoms (prodrome): A tertiary care study of 893 migraineurs. Headache 2004, 44, 865–872. [Google Scholar] [CrossRef]
- Larson, M.K.; Walker, E.F.; Compton, M.T. Early signs, diagnosis and therapeutics of the prodromal phase of schizophrenia and related psychotic disorders. Expert Rev. Neurother. 2010, 10, 1347–1359. [Google Scholar] [CrossRef] [Green Version]
- Howes, O.D.; Lim, S.; Theologos, G.; Yung, A.R.; Goodwin, G.M.; McGuire, P. A comprehensive review and model of putative prodromal features of bipolar affective disorder. Psychol. Med. 2011, 41, 1567–1577. [Google Scholar] [CrossRef]
- Graham, M.M.; Westerhout, C.M.; Kaul, P.; Norris, C.M.; Armstrong, P.W. Sex differences in patients seeking medical attention for prodromal symptoms before an acute coronary event. Am. Heart J. 2008, 156, 1210–1216.e1. [Google Scholar] [CrossRef] [PubMed]
- Marijon, E.; Uy-Evanado, A.; Dumas, F.; Karam, N.; Reinier, K.; Teodorescu, C.; Narayanan, K.; Gunson, K.; Jui, J.; Jouven, X.; et al. Warning symptoms are associated with survival from sudden cardiac arrest. Ann. Intern. Med. 2016, 164, 23–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wagner, D.; Nisenbaum, R.; Heim, C.; Jones, J.F.; Unger, E.R.; Reeves, W.C. Psychometric properties of the CDC symptom inventory for assessment of chronic fatigue syndrome. Popul. Health Metr. 2005, 3, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Chalder, T.; Berelowitz, G.; Pawlikowska, T.; Watts, L.; Wessely, S.; Wright, D.; Wallace, E.P. Development of a fatigue scale. J. Psychosom. Res. 1993, 37, 147–153. [Google Scholar] [CrossRef] [Green Version]
- Krupp, L.B.; LaRocca, N.G.; Muir-Nash, J.; Steinberg, A.D. The fatigue severity scale: Application to patients with multiple sclerosis and systemic lupus erythematosus. Arch. Neurol. 1989, 46, 1121–1123. [Google Scholar] [CrossRef]
- Larson, R.D. Psychometric properties of the modified fatigue impact scale. Int. J. MS Care. 2013, 15, 15–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moretti, A.; Gorini, A.; Villa, R.F. Affective disorders, antidepressant drugs and brain metabolism. Mol. Psychiatry 2003, 8, 773–785. [Google Scholar] [CrossRef] [PubMed]
- Maes, M. An intriguing and hitherto unexplained co-occurrence: Depression and chronic fatigue syndrome are manifestations of shared inflammatory, oxidative and nitrosative (IO&NS) pathways. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2011, 35, 784–794. [Google Scholar]
- Twisk, F.N. Accurate diagnosis of myalgic encephalomyelitis and chronic fatigue syndrome based upon objective test methods for characteristic symptoms. World J. Methodol. 2015, 5, 68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Oosterwijck, J.; Nijs, J.; Meeus, M.; Lefever, I.; Huybrechts, L.; Lambrecht, L.; Paul, L. Pain inhibition and postexertional malaise in myalgic encephalomyelitis/chronic fatigue syndrome: An experimental study. J. Intern. Med. 2010, 268, 265–278. [Google Scholar] [CrossRef]
- Cook, D.B.; Light, A.R.; Light, K.C.; Broderick, G.; Shields, M.R.; Dougherty, R.J.; Meyer, J.D.; VanRiper, S.; Stegner, A.J.; Ellingson, L.D.; et al. Neural consequences of post-exertion malaise in myalgic encephalomyelitis/chronic fatigue syndrome. Brain Behav. Immun. 2017, 62, 87–99. [Google Scholar] [CrossRef] [PubMed]
- Shukla, S.K.; Cook, D.; Meyer, J.; Vernon, S.D.; Le, T.; Clevidence, D.; Robertson, C.E.; Schrodi, S.J.; Yale, S.; Frank, D.N. Changes in gut and plasma microbiome following exercise challenge in myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS). PLoS ONE 2015, 10, e0145453. [Google Scholar] [CrossRef] [PubMed]
- Blomberg, J.; Gottfries, C.-G.; Elfaitouri, A.; Rizwan, M.; Rosén, A. Infection elicited autoimmunity and myalgic encephalomyelitis/chronic fatigue syndrome: An explanatory model. Front. Immunol. 2018, 9, 229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Myhill, S.; Booth, N.E.; McLaren-Howard, J. Chronic fatigue syndrome and mitochondrial dysfunction. Int. J. Clin. Exp. Med. 2009, 2, 1. [Google Scholar]
- Lane, R.J.M.; Burgess, A.P.; Flint, J.; Riccio, M.; Archard, L.C. Exercise responses and psychiatric disorder in chronic fatigue syndrome. BMJ 1995, 311, 544–545. [Google Scholar] [CrossRef] [Green Version]
- Ghali, A.; Lacout, C.; Ghali, M.; Gury, A.; Beucher, A.-B.; Lozac’h, P.; Lavigne, C.; Urbanski, G. Elevated blood lactate in resting conditions correlate with post-exertional malaise severity in patients with myalgic encephalomyelitis/chronic fatigue syndrome. Sci. Rep. 2019, 9, 1–9. [Google Scholar] [CrossRef]


{kind=link}
| Patients with Prodromal New or Non-Typical Symptoms a | The Rest of the Study Population | p | |
|---|---|---|---|
| Epidemiological characteristics | |||
| Patients, n (%) | 27 (13.7) | 170 (86.3) | |
| Female, n (%) | 21 (77.8) | 125 (73.5) | 0.64 |
| BMI b, kg/m2 | 22.2 (19.8–24.5) | 23.1 (20–26.2) | 0.40 |
| Age at data collection, years | 43 (33.5–50) | 42 (34.3–50.5) | 0.92 |
| Age at onset, years | 36 (24.5–43.5) | 32 (25–40) | 0.42 |
| Age at diagnosis, years | 40 (30.5–47.5) | 40 (32.3–48) | 0.81 |
| Delay in diagnosis, months | 43 (23–95) | 47 (22–102) | 0.40 |
| Family history of fatigue | 3 (11.1) | 11 (6.5) | 0.41 |
| Fatigue assessment | |||
| Fatigue severity scale | 5.8 (4.5–6.5) (n = 24) | 5.7 (5.1–6.4) (n = 128) | 0.47 |
| Fatigue scale | 24 (19–26.8) (n = 18) | 24 (20–28) (n = 138) | 0.31 |
| MFIS c physical | 28.5 (26.3–31) (n = 18) | 30 (26–33) (n = 137) | 0.69 |
| MFIS cognitive | 30 (27.3–34.5) (n = 18) | 26 (21–32) (n = 137) | 0.07 |
| MFIS psychosocial | 6 (5–6) (n = 18) | 6 (4.8–7) (n = 137) | 0.88 |
| PEM d assessment | |||
| PEM frequency | 3 (3–3) | 3 (3–3) | 0.93 |
| PEM intensity | 2.5 (2.5–4) | 4 (2.5–4) | 0.004 |
| PEM severity | 7.5 (7.5–12) | 12 (7.5–12) | 0.03 |
| Comorbidities, n (%) | 16 (59.3) | 124 (72.9) | 0.15 |
| Reactional depression | 7 (25.9) | 64 (37.6) | 0.24 |
| Hashimoto’s thyroiditis | 2 (7.4) | 12 (6.9) | >0.99 |
| Fibromyalgia | 2 (7.4) | 30 (17.6) | 0.26 |
| Irritable bowel syndrome | 13 (48.1) | 67 (39.4) | 0.39 |
| N° of Patients (%) | 27/197 (13.7) |
|---|---|
| Headaches | 6 (22.2) |
| Myalgia | 2 (7.4) |
| Arthralgia | 1 (3.7) |
| Paresthesia | 6 (22.2) |
| Motor disturbances b | 2 (7.4) |
| Flulike | 1 (3.7) |
| Nausea | 8 (29.6) |
| Abdominal pain | 1(0.5) |
| Palpitations | 2 (7.4) |
| Collapse | 3 (11.1) |
| Vertigo | 3 (11.1) |
| Shortness of breath | 3 (11.1) |
| Cold extremities | 1 (3.7) |
| Mood disorders | 10 (37) |
| Skin rash +/− pruritus | 2 (7.4) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ghali, A.; Lacout, C.; Ghali, M.; Gury, A.; Delattre, E.; Lavigne, C.; Urbanski, G. Warning Signals of Post-Exertional Malaise in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: A Retrospective Analysis of 197 Patients. J. Clin. Med. 2021, 10, 2517. https://doi.org/10.3390/jcm10112517
Ghali A, Lacout C, Ghali M, Gury A, Delattre E, Lavigne C, Urbanski G. Warning Signals of Post-Exertional Malaise in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: A Retrospective Analysis of 197 Patients. Journal of Clinical Medicine. 2021; 10(11):2517. https://doi.org/10.3390/jcm10112517
Chicago/Turabian StyleGhali, Alaa, Carole Lacout, Maria Ghali, Aline Gury, Estelle Delattre, Christian Lavigne, and Geoffrey Urbanski. 2021. "Warning Signals of Post-Exertional Malaise in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: A Retrospective Analysis of 197 Patients" Journal of Clinical Medicine 10, no. 11: 2517. https://doi.org/10.3390/jcm10112517
APA StyleGhali, A., Lacout, C., Ghali, M., Gury, A., Delattre, E., Lavigne, C., & Urbanski, G. (2021). Warning Signals of Post-Exertional Malaise in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: A Retrospective Analysis of 197 Patients. Journal of Clinical Medicine, 10(11), 2517. https://doi.org/10.3390/jcm10112517