
Does the Addition of Pain Neurophysiology Education to a Therapeutic Exercise Program Improve Physical Function in Women with Fibromyalgia Syndrome? Secondary Analysis of a Randomized Controlled Trial

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Material and Methods
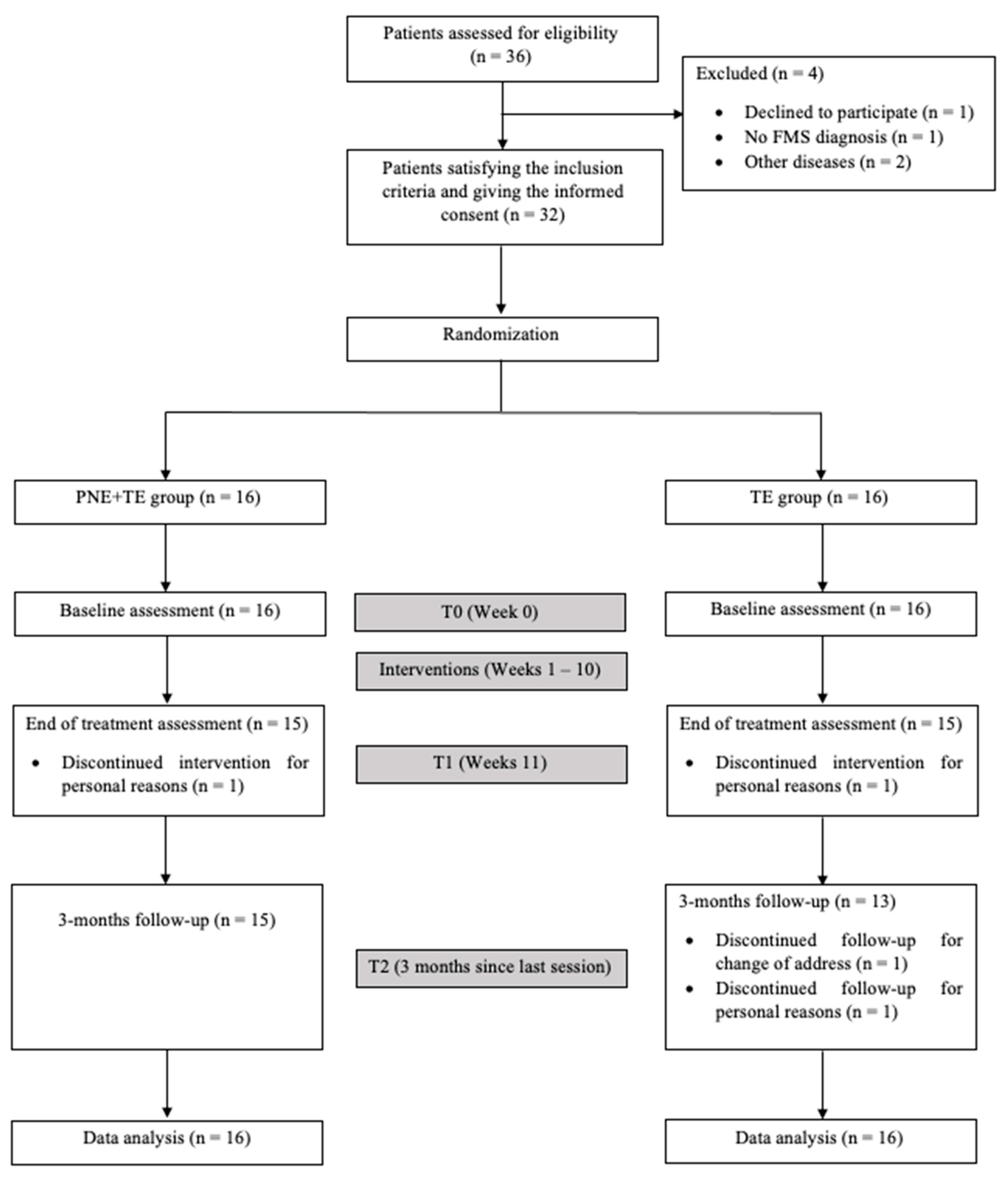
2.1. Study Design
2.2. Participants
2.3. Randomization and Blinding
2.4. Interventions
2.5. Outcome Measures
2.6. General Fatigue and Sleep Disturbances
2.7. Physical Function
2.8. Strength
3. Statistical Analysis
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.A.; Goldenberg, D.L.; Katz, R.S.; Mease, P.; Russell, A.S.; Russell, I.J.; Winfield, J.B.; Yunus, M.B. The American College of Rheumatology preliminary diagnostic criteria for fibromyalgia and measurement of symptom severity. Arthritis Care Res. 2010, 62, 600–610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Climent-Sanz, C.; Morera-Amenós, G.; Bellon, F.; Pastells-Peiró, R.; Blanco-Blanco, J.; Valenzuela-Pascual, F.; Gea-Sánchez, M. Poor Sleep Quality Experience and Self-Management Strategies in Fibromyalgia: A Qualitative Metasynthesis. J. Clin. Med. 2020, 9, 4000. [Google Scholar] [CrossRef]
- Geneen, L.J.; Moore, R.A.; Clarke, C.; Martin, D.; Colvin, L.A.; Smith, B.H. Physical activity and exercise for chronic pain in adults: An overview of Cochrane Reviews. Cochrane Database Syst. Rev. 2017, 1, CD011279. [Google Scholar] [PubMed] [Green Version]
- Turk, D. Suffering and Dysfunction in Fibromyalgia Syndrome. J. Musculoskelet. Pain 2002, 10, 85–96. [Google Scholar] [CrossRef]
- Bennett, R.M.; Clark, S.R.; Goldberg, L.; Nelson, D.; Bonafede, R.P.; Porter, J.; Specht, D. Aerobic fitness in patients with fibrositis. A controlled study of respiratory gas exchange and 133xenon clearance from exercising muscle. Arthritis Rheum. 1989, 32, 454–460. [Google Scholar] [CrossRef] [PubMed]
- Bennett, R.M.; Clark, S.C.; Walczyk, J. A randomized, double-blind, placebo-controlled study of growth hormone in the treatment of fibromyalgia. Am. J. Med. 1998, 104, 227–231. [Google Scholar] [CrossRef]
- Soriano-Maldonado, A.; Ruiz, J.R.; Aparicio, V.A.; Estévez-López, F.; Segura-Jiménez, V.; Álvarez-Gallardo, I.C.; Carbonell-Baeza, A.; Delgado-Fernandez, M.; Ortega, F.B. Association of physical fitness with pain in women with fibromyalgia: The al-Ándalus project. Arthritis Care Res. 2015, 67, 1561–1570. [Google Scholar] [CrossRef] [Green Version]
- Staud, R.; Robinson, M.E.; Vierck, C.J.; Price, D. Diffuse noxious inhibitory controls (DNIC) attenuate temporal summation of second pain in normal males but not in normal females or fibromyalgia patients. Pain 2003, 101, 167–174. [Google Scholar] [CrossRef]
- Bauman, A. Updating the evidence that physical activity is good for health: An epidemiological review 2000–2003. J. Sci. Med. Sport 2004, 7, 6–19. [Google Scholar] [CrossRef]
- Raftery, G.; Bridges, M.; Heslop, P.; Walker, D.J. Are fibromyalgia patients as inactive as they say they are? Clin. Rheumatol. 2009, 28, 711–714. [Google Scholar] [CrossRef]
- Galvez-Sánchez, C.M.; Del Paso, G.A.R. Diagnostic Criteria for Fibromyalgia: Critical Review and Future Perspectives. J. Clin. Med. 2020, 9, 1219. [Google Scholar] [CrossRef] [PubMed]
- Bidonde, J.; Busch, A.J.; Bath, B.; Milosavljevic, S. Exercise for adults with fibromyalgia: An umbrella systematic review with synthesis of best evidence. Curr. Rheumatol. Rev. 2014, 10, 45–79. [Google Scholar] [CrossRef] [PubMed]
- Bidonde, J.; Busch, A.J.; Schachter, C.L.; Overend, T.J.; Kim, S.Y.; Góes, S.M.; Boden, C.; Foulds, H.J.A. Aerobic exercise training for adults with fibromyalgia. Cochrane Database Syst. Rev. 2017, 6, CD012700. [Google Scholar] [CrossRef]
- Naugle, K.M.; Riley, J.L. Self-reported physical activity predicts pain inhibitory and facilitatory function. Med. Sci. Sports Exerc. 2014, 46, 622–629. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rooks, D.S. Talking to patients with fibromyalgia about physical activity and exercise. Curr. Opin. Rheumatol. 2008, 20, 208–212. [Google Scholar] [CrossRef] [PubMed]
- Izquierdo-Alventosa, R.; Inglés, M.; Cortés-Amador, S.; Gimeno-Mallench, L.; Chirivella-Garrido, J.; Kropotov, J.; Serra-Añó, P. Low-Intensity Physical Exercise Improves Pain Catastrophizing and Other Psychological and Physical Aspects in Women with Fibromyalgia: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2020, 17, 3634. [Google Scholar] [CrossRef]
- Clarke, C.L.; Ryan, C.G.; Martin, D.J. Pain neurophysiology education for the management of individuals with chronic low back pain: A systematic review and meta-analysis. Man. Ther. 2011, 16, 544–549. [Google Scholar] [CrossRef]
- García-Ríos, M.C.; Navarro-Ledesma, S.; Tapia-Haro, R.M.; Toledano-Moreno, S.; Casas-Barragán, A.; Correa-Rodríguez, M.; Ferrandiz, M.E.A. Effectiveness of health education in patients with fibromyalgia: A systematic review. Eur. J. Phys. Rehabil. Med. 2019, 55, 301–313. [Google Scholar] [CrossRef] [PubMed]
- Macfarlane, G.J.; Kronisch, C.; Dean, L.E.; Atzeni, F.; Häuser, W.; Flub, E.; Choy, E.; Kosek, E.; Amris, K.; Branco, J.; et al. EULAR revised recommendations for the management of fibromyalgia. Ann. Rheum. Dis. 2017, 76, 318–328. [Google Scholar] [CrossRef]
- Ceballos-Laita, L.; Mingo-Gómez, M.T.; Navas-Cámara, F.; Estébanez-de-Miguel, E.; Caudevilla-Polo, S.; Verde-Rello, Z.; Fernandez-Araque, A.; Jimenez-del-Barrio, S. Therapeutic Exercise and Pain Neurophysiology Education in Female Patients with Fibromyalgia Syndrome: A Feasibility Study. J. Clin. Med. 2020, 9, 3564. [Google Scholar] [CrossRef]
- Busch, A.J.; Webber, S.C.; Brachaniec, M.; Bidonde, J.; Bello-Haas, V.D.; Danyliw, A.D.; Overend, T.J.; Richards, R.S.; Sawant, A.; Schachter, C.L. Exercise Therapy for Fibromyalgia. Curr. Pain Headache Rep. 2011, 15, 358–367. [Google Scholar] [CrossRef] [Green Version]
- Butler, D.S.; Moseley, G.L. Explain Pain, 2nd ed.; Noigroup Publications: Adelaide, Australia, 2013; 116p. [Google Scholar]
- Lee, K.A.; Hicks, G.; Nino-Murcia, G. Validity and reliability of a scale to assess fatigue. Psychiatry Res. 1991, 36, 291–298. [Google Scholar] [CrossRef]
- Ericsson, A.; Mannerkorpi, K. Assessment of fatigue in patients with fibromyalgia and chronic widespread pain. Reliability and validity of the Swedish version of the MFI-20. Disabil. Rehabil. 2007, 29, 1665–1670. [Google Scholar] [CrossRef]
- Crawford, B.K.; Piault, E.C.; Lai, C.; Bennett, R.M. Assessing fibromyalgia-related fatigue: Content validity and psychometric performance of the Fatigue Visual Analogue Scale in adult patients with fibromyalgia. Clin. Exp. Rheumatol. 2011, 29, S34–S43. [Google Scholar] [PubMed]
- Álvarez-Gallardo, I.C.; Carbonell-Baeza, A.; Segura-Jiménez, V.; Soriano-Maldonado, A.; Intemann, T.; Aparicio, V.A.; Estévez-López, F.; Moirón, D.C.; Herrador-Colmenero, M.; Ruiz, J.R.; et al. Physical fitness reference standards in fibromyalgia: The al-Ándalus project. Scand. J. Med. Sci. Sports 2017, 27, 1477–1488. [Google Scholar] [CrossRef] [PubMed]
- Hesseberg, K.; Bentzen, H.; Bergland, A. Reliability of the Senior Fitness Test in Community-dwelling Older People with Cognitive Impairment. Physiother. Res. Int. 2015, 20, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Carbonell-Baeza, A.; Álvarez-Gallardo, I.; Segura-Jiménez, V.; Castro-Piñero, J.; Ruiz, J.; Delgado-Fernández, M.; Aparicio, V. Reliability and Feasibility of Physical Fitness Tests in Female Fibromyalgia Patients. Int. J. Sports Med. 2014, 36, 157–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trampisch, U.S.; Franke, J.; Jedamzik, N.; Hinrichs, T.; Platen, P. Optimal Jamar Dynamometer Handle Position to Assess Maximal Isometric Hand Grip Strength in Epidemiological Studies. J. Hand Surg. 2012, 37, 2368–2373. [Google Scholar] [CrossRef]
- Boomershine, C.S.; Emir, B.; Zlateva, G.; Wang, Y. Simplifying fibromyalgia assessment: The VASFIQ Brief Symptom Scale. Ther. Adv. Musculoskelet. Dis. 2011, 3, 215–226. [Google Scholar] [CrossRef] [Green Version]
- Aparicio, V.A.; Segura-Jiménez, V.; Álvarez-Gallardo, I.C.; Soriano-Maldonado, A.; Castro-Piñero, J.; Delgado-Fernández, M.; Carbonell-Baeza, A. Fitness testing in the fibromyalgia diagnosis: The al-Andalus project. Med. Sci. Sports Exerc. 2014, 47, 451–459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larsson, A.; Palstam, A.; Löfgren, M.; Ernberg, M.; Bjersing, J.; Bileviciute-Ljungar, I.; Gerdle, B.; Kosek, E.; Mannerkorpi, K. Resistance exercise improves muscle strength, health status and pain intensity in fibromyalgia—A randomized controlled trial. Arthritis Res. Ther. 2015, 17, 1–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simister, H.D.; Tkachuk, G.A.; Shay, B.L.; Vincent, N.; Pear, J.J.; Skrabek, R.Q. Randomized Controlled Trial of Online Acceptance and Commitment Therapy for Fibromyalgia. J. Pain 2018, 19, 741–753. [Google Scholar] [CrossRef]
- Gowans, S.E.; Dehueck, A.; Voss, S.; Silaj, A.; Abbey, S.E.; Reynolds, W.J. Effect of a randomized, controlled trial of exercise on mood and physical function in individuals with fibromyalgia. Arthritis Rheum. 2001, 45, 519–529. [Google Scholar] [CrossRef]
- Avlund, K. Fatigue in older adults: An early indicator of the aging process? Aging Clin. Exp. Res. 2010, 22, 100–115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zengarini, E.; Ruggiero, C.; Pérez-Zepeda, M.U.; Hoogendijk, E.; Vellas, B.; Mecocci, P.; Cesari, M. Fatigue: Relevance and implications in the aging population. Exp. Gerontol. 2015, 70, 78–83. [Google Scholar] [CrossRef]
- Nicassio, P.M.; Moxham, E.G.; Schuman, C.E.; Gevirtz, R.N. The contribution of pain, reported sleep quality, and depressive symptoms to fatigue in fibromyalgia. Pain 2002, 100, 271–279. [Google Scholar] [CrossRef]
- Nijs, J.; Van Houdenhove, B. From acute musculoskeletal pain to chronic widespread pain and fibromyalgia: Application of pain neurophysiology in manual therapy practice. Man Ther. 2009, 14, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Moseley, G.L.; Nicholas, M.K.; Hodges, P. A Randomized Controlled Trial of Intensive Neurophysiology Education in Chronic Low Back Pain. Clin. J. Pain 2004, 20, 324–330. [Google Scholar] [CrossRef] [PubMed]
- Thomas, J.S.; France, C.R.; Sha, D.; Wiele, N.V. The influence of pain-related fear on peak muscle activity and force generation during maximal isometric trunk exertions. Spine 2008, 33, 342–348. [Google Scholar] [CrossRef]
- Duenas, M.; Ojeda, B.; Salazar, A.; A Mico, J.; Failde, I. A review of chronic pain impact on patients, their social environment and the health care system. J. Pain Res. 2016, 9, 457–467. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| PNE + TE Group (n = 16) | TE Group (n = 16) | p Value | |
|---|---|---|---|
| Age (years) | 52.13 ± 10.31 | 53.00 ± 10.68 | t= 0.218 0.818 |
| Height (cm) | 159.66 ± 5.08 | 159.35 ± 5.87 | t = 0.385 0.874 |
| BMI (kg/cm2) | 30.10 ± 6.69 | 26.17 ± 4.99 | t= 2.154 0.070 |
| VAS-F | 7.15 ± 1.68 | 6.44 ± 2.29 | t = 1 p = 0.324 |
| VAS-S | 7.11 ± 2.82 | 6.04 ± 2.69 | U= 92 p = 0.184 |
| TUG | 10.18 ± 3.19 | 9.25 ± 1.83 | U = 118.5 p = 0.724 |
| 6MWT | 390.37 ± 105.64 | 397.06 ± 64.27 | U = 117.5 p = 0.696 |
| CS | 10.06 ± 4.36 | 8.62 ± 2.22 | U = 97.5 p = 0.254 |
| AC | 10.44 ± 4.27 | 8.75 ± 3.22 | t = 1.262 p = 0.217 |
| CSR | −9.00 ± 11.56 | −4.37 ± 12.34 | U = 87.5 p = 0.128 |
| BST | −9.06 ± 11.56 | −4.38 ± 12.34 | U = 77.5 p = 0.056 |
| Handgrip D | 26.00 ± 11.07 | 21.35 ± 5.37 | U = 87.5 p = 0.128 |
| Handgrip ND | 23.31 ± 10.26 | 20.56 ± 7.42 | U = 118.5 p = 0.724 |
| Baseline (T0) Mean ± SD (95% CI) | Postintervention (T1) Mean ± SD (95% CI) | Within-Group Changes p-Values | Between-Groups p-Value | 3 Months Follow-Up (T2) Mean ± SD (95% CI) | Within-Group Changes p-Values | Between-Groups p-Value | |
|---|---|---|---|---|---|---|---|
| VAS-F (0–10) | |||||||
| PNE + TE group | 7.15 ± 1.68 | 5.11 ± 3.81 | 2.04 (0.48, 3.59) <0.013 | F = 0.21 0.648 | 5.45 ± 2.66 | 1.70 (0.20, 3.19) <0.028 | F = 1.04 0.315 |
| TE group | 6.44 ± 2.29 | 4.78 ± 2.99 | 1.65 (0.73, 2.57) 0.002 | 5.6 ± 2.38 | 0.83 (−0.2, 1.86) 0.107 | ||
| VAS-S (0–10) | |||||||
| PNE + TE group | 7.11 ± 2.82 | 4.71 ± 3.52 | 2.40 (0.30, 4.50) 0.027 | F = 2.68 0.112 | 5.00 ± 2.95 | 2.01 (0.03, 3.05) 0.040 | F = 1.00 0.324 |
| TE group | 6.04 ± 2.69 | 5.53 ± 2.90 | 0.51 (−0.76, 1.79) 0.405 | 3.67 ± 2.57 | 2.37 (1.40, 3.33) <0.001 | ||
| TUG | |||||||
| PNE + TE group | 10.18 ± 3.19 | 7.53 ± 1.97 | 2.65 (1.70, 3.50) 0.010 | F = 4.51 0.042 | 7.65 ± 2.16 | 2.53 (1.69, 3.36) <0.001 | F = 3.81 0.060 |
| TE group | 9.25 ± 1.83 | 8.63 ± 2.86 | 0.62 (−1.17, 2.42) 0.472 | 7.72 ± 1.87 | 0.83 (0.83, 2.23) <0.001 | ||
| 6MWT | |||||||
| PNE + TE group | 390.37 ± 105.64 | 463.31 ± 120.05 | −72.93 (−98.94, −46.91) <0.001 | F = 2.63 0.115 | 435.24 ± 122.73 | −44.86 (−76.94, −12.78) 0.009 | F = 0.32 0.575 |
| TE group | 397.06 ± 64.27 | 445.71 ± 74.34 | −48.65 (−67.04, −30.25) <0.001 | 432.79 ± 59.53 | −35.72 (−48.10, −23.34) <0.001 | ||
| CS | |||||||
| PNE + TE group | 10.06 ± 4.36 | 12.47 ± 4.27 | −2.40 (−3.14, −1.67) < 0.001 | F = 1.03 0.316 | 12.26 ± 5.12 | −2.20 (−3.13, −1.26) <0.001 | F = 0.06 0.803 |
| TE group | 8.62 ± 2.22 | 10.49 ± 2.82 | −1.86 (−2.73, −0.99) 0.001 | 10.69 ± 2.24 | −2.06 (−2.75, −1.37) <0.001 | ||
| AC | |||||||
| PNE + TE group | 10.44 ± 4.27 | 14.97 ± 5.02 | −4.53 (−6.01, −3.05) <0.001 | F = 4.46 0.043 | 15.75 ± 5.76 | −5.31 (−7.34, −3.28) <0.001 | F = 2.69 0.111 |
| TE group | 8.75 ± 3.22 | 11.50 ± 4.37 | −2.75 (−3.77, −1.73) <0.001 | 12.38 ± 4.09 | −3.62 (−4.44, −2.80) <0.001 | ||
| CSR | |||||||
| PNE + TE group | −9.00 ± 11.56 | −5.71 ± 13.59 | −9.66 (−17.05, −2.27) 0.014 | F = 1.36 0.251 | −4.17 ± 15.2 | −11.2 (−20.64, −1.75) 0.023 | F = 3.31 0.079 |
| TE group | −4.37 ± 12.34 | −3.04 ± 9.96 | −4.96 (−9.29, −0.62) 0.028 | −5.76 ± 13.86 | −2.23 (−6.83, 2.37) 0.318 | ||
| BST | |||||||
| PNE + TE group | −9.06 ± 11.56 | −8.99 ± 14.20 | −0.06 (−4.95, 4.82) 0.977 | F = 0.020 0.887 | −7.59 ± 13.20 | −1.46 (−5.64, 2.71) 0.466 | F = 1.09 0.304 |
| TE group | −4.38 ± 12.34 | −3.94 ± 12.78 | −0.43(−3.02, 2.15) 0.724 | −5.2 ± 14.81 | 0.83 (−1.29, 2.95) 0.427 | ||
| Handgrip D | |||||||
| PNE + TE group | 26.00 ± 11.07 | 29.47 ± 10.07 | −3.46 (−7.42, 0.49) 0.082 | F = 1.77 0.193 | 29.40 ± 10.34 | −3.46 (−8.04, 1.10) 0.127 | F = 0.963 0.334 |
| TE group | 21.35 ± 5.37 | 21.78 ± 8.08 | −0.53 (−3.06, 2.00) 0.661 | 22.28 ± 7.98 | −1.03 (−3.66, 1.58) 0.130 | ||
| Handgrip ND | |||||||
| PNE + TE group | 23.31 ± 10.26 | 27.51 ± 9.31 | −4.20 (−7.14, −1.21) 0.008 | F = 3.6 0.067 | 27.3 ± 10.35 | −3.98 (−7.73, −0.24) 0.038 | F = 4.86 0.036 |
| TE group | 20.56 ± 7.42 | 21.63 ± 6.99 | −1.06 (−2.99, 0.86) 0.259 | 20.66 ± 7.63 | −0.1 (−0.51, 0.31) 0.611 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ceballos-Laita, L.; Mingo-Gómez, M.T.; Estébanez-de-Miguel, E.; Bueno-Gracia, E.; Navas-Cámara, F.J.; Verde-Rello, Z.; Fernández-Araque, A.; Jiménez-del-Barrio, S. Does the Addition of Pain Neurophysiology Education to a Therapeutic Exercise Program Improve Physical Function in Women with Fibromyalgia Syndrome? Secondary Analysis of a Randomized Controlled Trial. J. Clin. Med. 2021, 10, 2518. https://doi.org/10.3390/jcm10112518
Ceballos-Laita L, Mingo-Gómez MT, Estébanez-de-Miguel E, Bueno-Gracia E, Navas-Cámara FJ, Verde-Rello Z, Fernández-Araque A, Jiménez-del-Barrio S. Does the Addition of Pain Neurophysiology Education to a Therapeutic Exercise Program Improve Physical Function in Women with Fibromyalgia Syndrome? Secondary Analysis of a Randomized Controlled Trial. Journal of Clinical Medicine. 2021; 10(11):2518. https://doi.org/10.3390/jcm10112518
Chicago/Turabian StyleCeballos-Laita, Luis, María Teresa Mingo-Gómez, Elena Estébanez-de-Miguel, Elena Bueno-Gracia, Francisto José Navas-Cámara, Zoraida Verde-Rello, Ana Fernández-Araque, and Sandra Jiménez-del-Barrio. 2021. "Does the Addition of Pain Neurophysiology Education to a Therapeutic Exercise Program Improve Physical Function in Women with Fibromyalgia Syndrome? Secondary Analysis of a Randomized Controlled Trial" Journal of Clinical Medicine 10, no. 11: 2518. https://doi.org/10.3390/jcm10112518
APA StyleCeballos-Laita, L., Mingo-Gómez, M. T., Estébanez-de-Miguel, E., Bueno-Gracia, E., Navas-Cámara, F. J., Verde-Rello, Z., Fernández-Araque, A., & Jiménez-del-Barrio, S. (2021). Does the Addition of Pain Neurophysiology Education to a Therapeutic Exercise Program Improve Physical Function in Women with Fibromyalgia Syndrome? Secondary Analysis of a Randomized Controlled Trial. Journal of Clinical Medicine, 10(11), 2518. https://doi.org/10.3390/jcm10112518