
Evaluation of Strategies to Fight COVID-19: The French Paradigm

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Governmental Policies against COVID-19
2.2. COVID-Related Mortality in France and Other European Countries
2.3. Excess All-Cause Mortality in France and Other European Countries
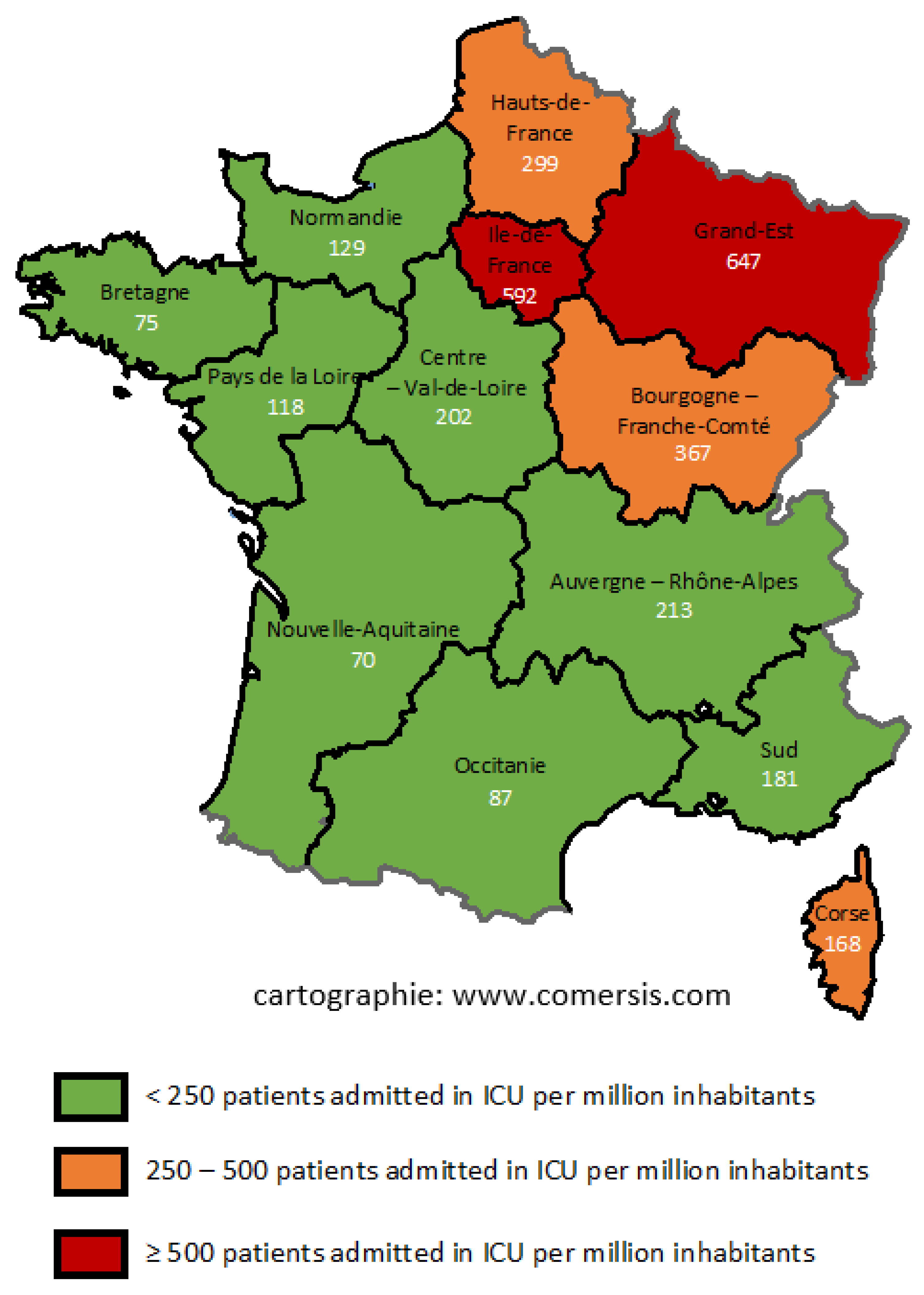
2.4. French Departmental and Regional Data on COVID-19
2.5. Seroprevalences in French Regions and Probability of Mortality
2.6. Marseille Data
2.7. Statistical Analysis
3. Results
3.1. Government Policies against COVID-19
3.2. Overall Analysis and Positioning of France in Relation to Other European Countries
3.3. Comparison of Excess All-Cause Mortality
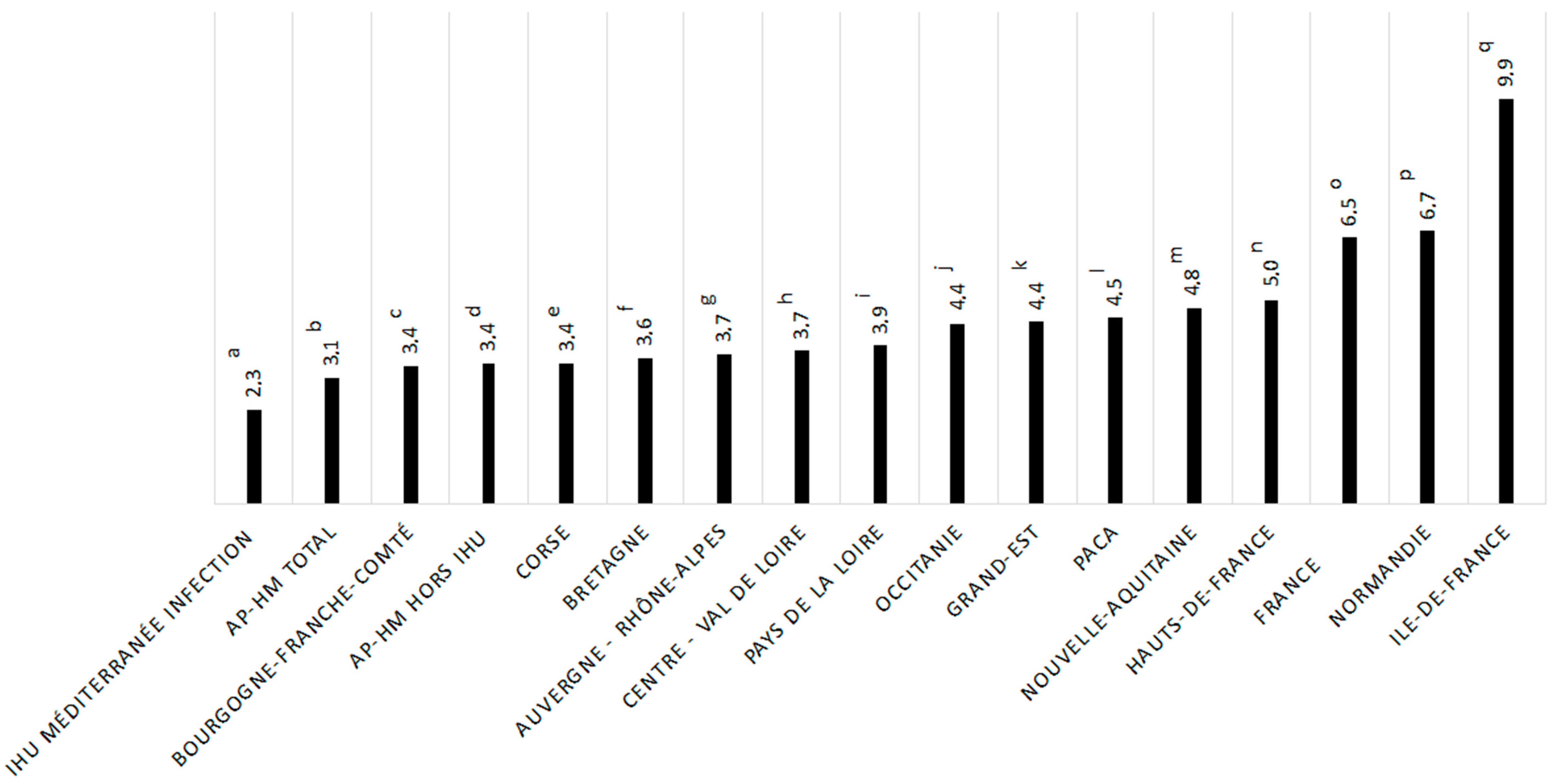
3.4. Mortality Rates Associated with COVID-19 in France
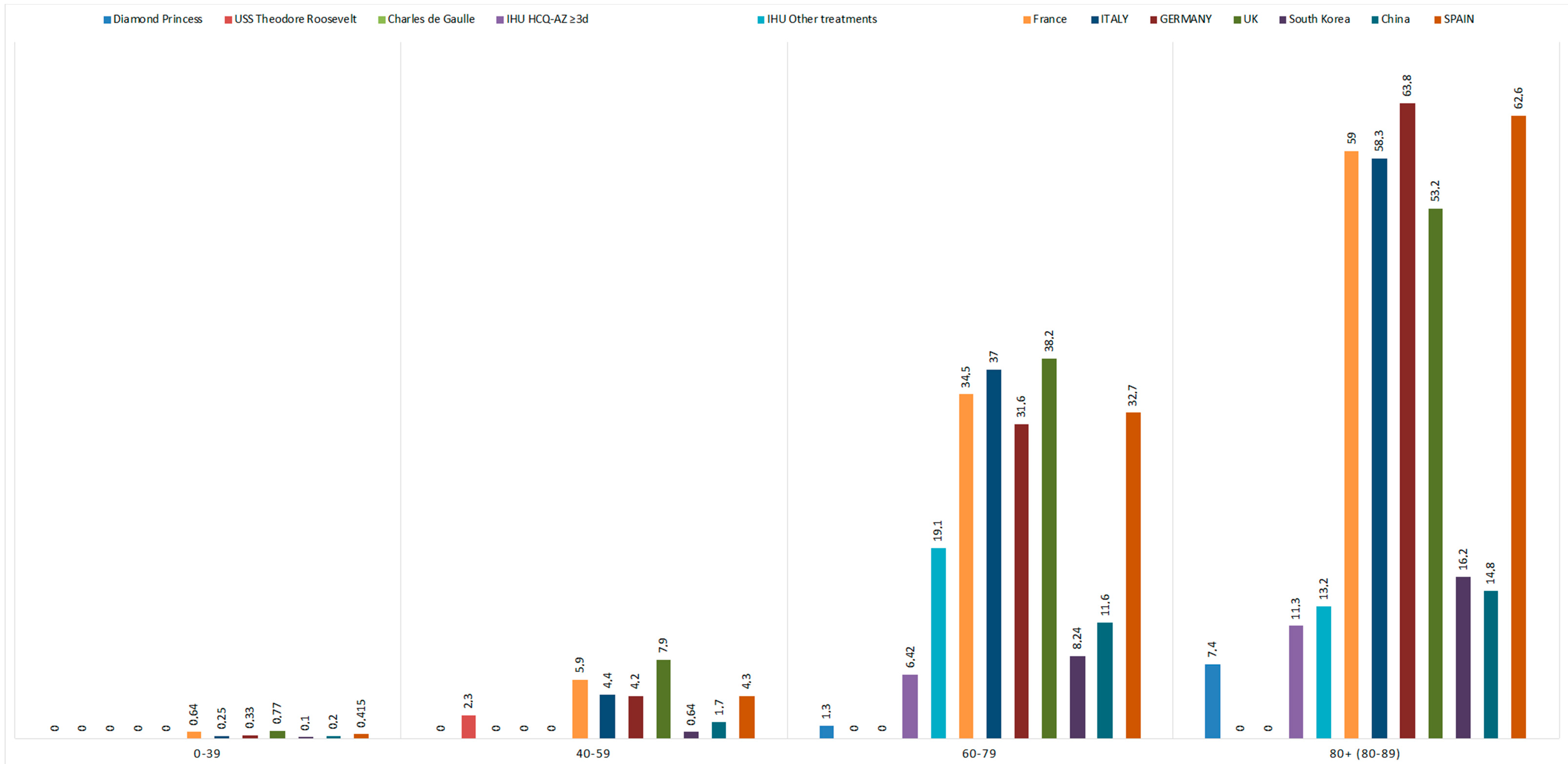
3.5. Mortality Associated with COVID-19 in People under 60 Years of Age
3.6. Mortality Estimation According to the Prevalence of Antibodies Tested after the First Outbreak
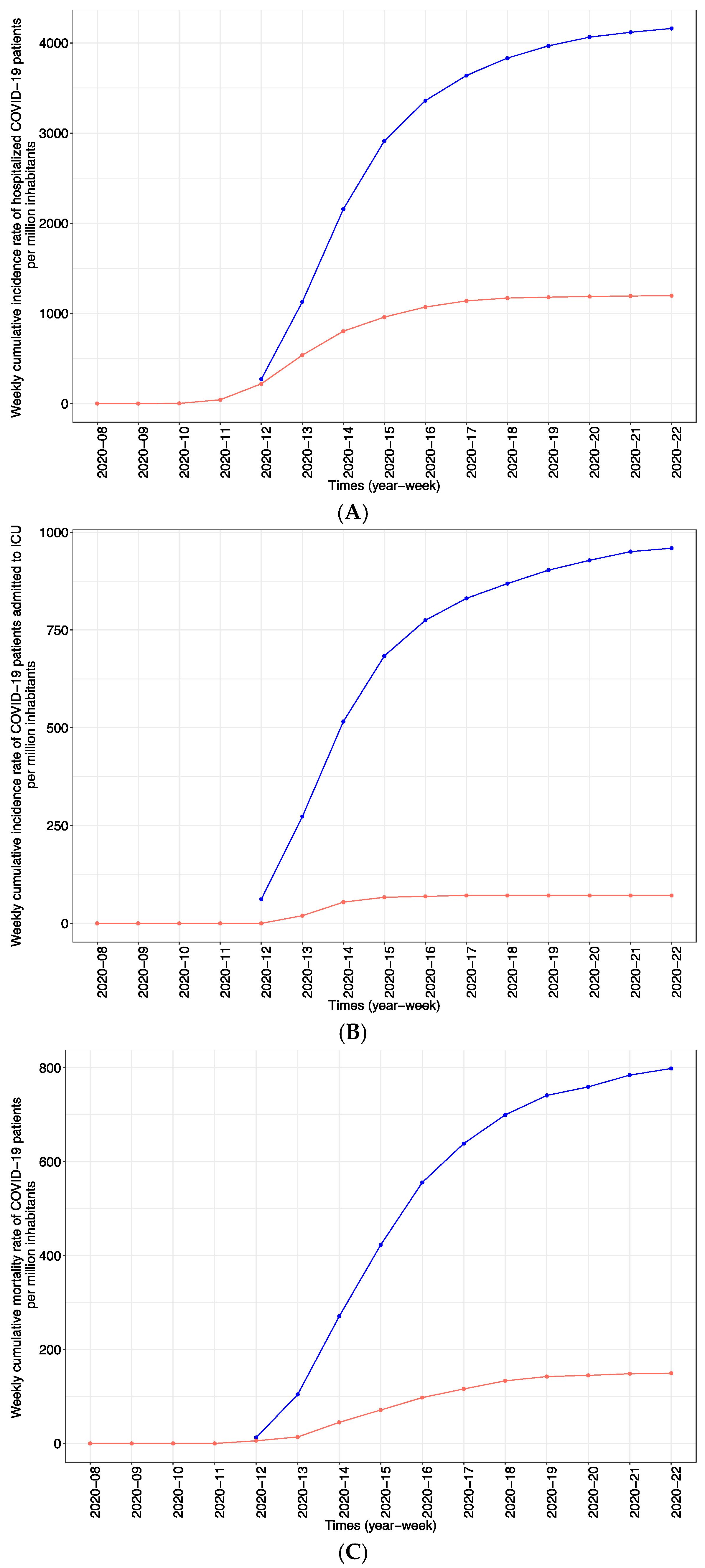
3.7. Focus on Two French Cities: Paris and Marseille
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dong, E.; Du, H.; Gardner, L. An interactive web-based dashboard to track, COVID-19 in real time. Lancet Infect. Dis. 2020, 20, 533–534. [Google Scholar] [CrossRef]
- Vanhems, P. SARS-CoV2 infection and primary school closure. Eurosurveillance 2020, 25, 2000617. [Google Scholar] [CrossRef] [PubMed]
- Moatti, J.P. The French response to COVID-19: Intrinsic difficulties at the interface of science, public health, and policy. Lancet Public Health 2020, 5, e255. [Google Scholar] [CrossRef]
- Décret n 2020-260 du 16 Mars 2020 Portant Réglementation des Déplacements dans le Cadre de la Lutte Contre la Propagation du Virus COVID-19. Available online: https://www.legifrance.gouv.fr/affichTexte.do?cidTexte=JORFTEXT000041728476 (accessed on 11 June 2021).
- Gudbjartsson, D.F.; Helgason, A.; Jonsson, H.; Magnusson, O.T.; Melsted, P.; Norddahl, G.L.; Saemundsdottir, J.; Sigurdsson, A.; Sulem, P.; Agustsdottir, A.B.; et al. Spread of SARS-CoV-2 in the Icelandic Population. N. Engl. J. Med. 2020, 382, 2302–2315. [Google Scholar] [CrossRef] [PubMed]
- Kwon, K.T.; Ko, J.H.; Shin, H.; Sung, M.; Kim, J.Y. Drive-Through Screening Center for COVID-19: A Safe and Efficient Screening System against Massive Community Outbreak. J. Korean Med. Sci. 2020, 35, e123. [Google Scholar] [CrossRef] [PubMed]
- Définition de cas d’infection au SARS-CoV-2 (COVID-19) Mise à jour le 13 Mars 2020 (n.d.). Available online: http://splf.fr/wp-content/uploads/2020/03/COVID-19_definition_cas_20200313.pdf (accessed on 5 June 2020).
- Gautret, P.; Lagier, J.C.; Parola, P.; Meddeb, L.; Mailhe, M.; Doudier, B.; Courjon, J.; Giordanengo, V.; Vieira, V.E.; Dupont, H.T.; et al. Hydroxychloroquine and azithromycin as a treatment of COVID-19: Results of an open-label non-randomized clinical trial. Int. J. Antimicrob. Agents 2020, 56, 105949. [Google Scholar] [CrossRef]
- Décret n 2020-314 du 25 Mars 2020 Prescrivant les Mesures Générales Nécessaires Pour Faire Face à l’épidémie COVID-19 dans le Cadre de L’état D’urgence Sanitaire. Available online: https://www.legifrance.gouv.fr/affichTexte.do?cidTexte=JORFTEXT000041755775&categorieLien=id (accessed on 11 June 2021).
- Our World in Data. Daily COVID-19 Tests per Thousand People. Available online: https://ourworldindata.org/coronavirus-testing (accessed on 5 August 2020).
- Coronavirus Government Response Tracker | Blavatnik School of Government. (n.d.) Available online: https://www.bsg.ox.ac.uk/research/research-projects/coronavirus-government-response-tracker#data (accessed on 5 June 2020).
- Russell, T.W.; Hellewell, J.; Jarvis, C.I.; Van Zandvoort, K.; Abbott, S.; Ratnayake, R.; Flasche, S.; Eggo, R.M.; Edmunds, W.J.; Kucharski, A.J.; et al. Estimating the infection and case fatality ratio for coronavirus disease (COVID-19) using age-adjusted data from the outbreak on the Diamond Princess cruise ship February 2020. Eurosurveillance 2020, 25, 2000256. [Google Scholar] [CrossRef] [Green Version]
- Alvarado, G.R.; Pierson, B.C.; Teemer, E.S.; Gama, H.J.; Cole, R.D.; Jang, S.S. Symptom Characterization and Outcomes of Sailors in Isolation After a COVID-19 Outbreak on a US Aircraft Carrier. JAMA Netw. Open 2020, 3, e2020981. [Google Scholar] [CrossRef]
- Communiqué_Publication des Conclusions des Enquêtes sur la Contamination au COVID-19 au sein du Groupe Aéronaval. (n.d.) Available online: https://www.defense.gouv.fr/salle-de-presse/communiques/communique_publication-des-conclusions-des-enquetes-sur-la-contamination-au-covid-19-au-sein-du-groupe-aeronaval (accessed on 4 November 2020).
- Téléchargement des Fichiers des décès Quotidiens−Nombre de décès Quotidiens|Insee. (n.d.) Available online: https://www.insee.fr/fr/statistiques/4487988?sommaire=4487854 (accessed on 18 June 2020).
- What Is a Z-Score?—EUROMOMO. (n.d.) Available online: https://www.euromomo.eu/how-it-works/what-is-a-z-score/ (accessed on 22 June 2020).
- Données Hospitalières Relatives à L’épidémie de COVID-19-Data.Gouv.fr. (n.d.) Available online: https://www.data.gouv.fr/fr/datasets/donnees-hospitalieres-relatives-a-lepidemie-de-covid-19/#_ (accessed on 5 June 2020).
- Population par Région et Département-Structure de la Population-France-Les Chiffres-Ined-Institut National D’études Démographiques. (n.d.) Available online: https://www.ined.fr/fr/tout-savoir-population/chiffres/france/structure-population/regions-departements/ (accessed on 5 June 2020).
- Géodes-Santé Publique France. (n.d.) Available online: https://geodes.santepubliquefrance.fr/#c=home (accessed on 2 June 2020).
- Carrat, F.; De Lamballerie, X.; Rahib, D.; Blanché, H.; Lapidus, N.; Artaud, F.; Kab, S.; Renuy, A.; de Edelenyi, F.S.; Meyer, L.; et al. Seroprevalence of SARS-CoV-2 among adults in three regions of France following the lockdown and associated risk factors: A multicohort study. MedRxiv 2020. [Google Scholar] [CrossRef]
- Salje, H.; Tran Kiem, C.; Lefrancq, N.; Salje, H.; Kiem, C.T.; Lefrancq, N.; Courtejoie, N.; Bosetti, P.; Paireau, J.; Andronico, A.; et al. Estimating the burden of SARS-CoV-2 in France. Science 2020, 369, 208–211. [Google Scholar] [CrossRef]
- Abat, C.; Chaudet, H.; Colson, P.; Rolain, J.M.; Raoult, D. Real-Time Microbiology Laboratory Surveillance System to Detect Abnormal Events and Emerging Infections Marseille France. Emerg. Infect. Dis. 2015, 21, 1302–1310. [Google Scholar] [CrossRef] [PubMed]
- Colson, P.; Rolain, J.M.; Abat, C.; Charrel, R.; Fournier, P.E.; Raoult, D. EPIMIC: A Simple Homemade Computer Program for Real-Time EPIdemiological Surveillance and Alert Based on MICrobiological Data. PLoS ONE 2015, 10, e0144178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Recensement de la Population| Insee. Available online: https://webcache.googleusercontent.com/search?q=cache:7m-ySsbBFKYJ:https://www.insee.fr/fr/statistiques/fichier/4265439/dep13.pdf+&cd=2&hl=fr&ct=clnk&gl=fr (accessed on 5 June 2020).
- R Core Team. R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing Vienna Austria. Available online: http://www.R-project.org/ (accessed on 11 June 2020).
- Wickham, H. ggplot2: Elegant Graphics for Data Analysis; Springer: New York, NY, USA, 2016. [Google Scholar]
- Pollán, M.; Pérez-Gómez, B.; Pastor-Barriuso, R.; Oteo, J.; Hernán, M.A.; Sanmartín, J.L.; Fernández-García, A.; Cruz, I.; de Larrea, N.F.; Molina, M.; et al. Prevalence of SARS-CoV-2 in Spain (ENE-COVID): A nationwide, population-based seroepidemiological study. Lancet 2020, 396, 535–544. [Google Scholar] [CrossRef]
- Istituto Nazionale di Statistica Ministera della Salute Primi Risultati Dell’indagine di Sieroprevalenza sul SARS-COV2, Comunicato stampa. Available online: https://www.istat.it/it/files//2020/08/ReportPrimiRisultatiIndagineSiero.pdf (accessed on 3 August 2020).
- De Larochelambert, Q.; Marc, A.; Antero, J.; Le Bourg, E.; Toussaint, J.F. Covid-19 Mortality: A Matter of Vulnerability Among Nations Facing Limited Margins of Adaptation. Front. Public Health 2020, 8, 604339. [Google Scholar] [CrossRef] [PubMed]
- Bendavid, E.; Oh, C.; Bhattacharya, J.; Ioannidis, J.P.A. Assessing mandatory stay-at-home and business closure effects on the spread of COVID-19. Eur. J. Clin. Investig. 2021, 51, e13484. [Google Scholar]
- Souris, M.; Gonzalez, J.P. COVID-19: Spatial analysis of hospital case-fatality rate in France. PLoS ONE 2020, 15, e0243606. [Google Scholar] [CrossRef]
- OECD. Health at a Glance 2019: OECD Indicators; OECD Publishing: Paris, France, 2019. [Google Scholar] [CrossRef]
- Préparation a la phase épidémique de COVID-19. Ministère des Solidarités et de la Santé 16 March 2020. Available online: https://solidaritessante.gouv.fr/IMG/pdf/guide-covid-19-phaseepidemique-v15-16032020.pdf (accessed on 27 March 2020).
- Why Should I Isolate Myself? Until When Should I Isolate Myself? (n.d.) Available online: https://solidarites-sante.gouv.fr (accessed on 23 November 2020).
- Minni, A.; Ralli, M.; Candelori, F.; Cialente, F.; Ercoli, L.; Parlapiano, C.; Greco, A.; De Vincentiis, M. Lessons learned from COVID-19 pandemic in Italy—A commentary. Bosn. J. Basic Med. Sci. 2021, 21, 117–119. [Google Scholar]
- Siemieniuk, R.A.; Bartoszko, J.J.; Ge, L.; Zeraatkar, D.; Izcovich, A.; Kum, E.; Pardo-Hernandez, H.; Rochwerg, B.; Lamontagne, F.; Han, M.A.; et al. Drug treatments for covid-19: Living systematic review and network meta-analysis. BMJ 2020, 370, m2980. [Google Scholar] [CrossRef]
- Horby, P.; Lim, W.S.; Emberson, J.R.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Brightling, C.; Ustianowski, A.; Elmahi, E.; et al. Dexamethasone in Hospitalized Patients with Covid-19—Preliminary Report. N. Engl. J. Med. 2020, 384, 693–704. [Google Scholar] [CrossRef]
- Wang, Y.; Zhang, D.; Du, G.; Du, R.; Zhao, J.; Jin, Y.; Fu, S.; Gao, L.; Cheng, Z.; Lu, Q.; et al. Remdesivir in adults with severe COVID-19: A randomised, double-blind, placebo-controlled, multicentre trial. Lancet 2020, 395, 1569–1578. [Google Scholar] [CrossRef]
- Young, B.; Tan, T.T.; Leo, Y.S. The place for remdesivir in COVID-19 treatment. Lancet Infect. Dis. 2021, 21, 20–21. [Google Scholar] [CrossRef]
- Sbidian, E.; Josse, J.; Lemaitre, G.; Mayer, I.; Bernaux, M.; Gramfort, A.; Lapidus, N.; Paris, N.; Neuraz, A.; Lerner, I.; et al. Hydroxychloroquine with or without azithromycin and in-hospital mortality or discharge in patients hospitalized for COVID-19 infection: A cohort study of 4642 in-patients in France. MedRxiv 2020. [Google Scholar] [CrossRef]
- Lagier, J.C.; Million, M.; Gautret, P.; Colson, P.; Cortaredona, S.; Giraud-Gatineau, A.; Honoré, S.; Gaubert, J.Y.; Fournier, P.E.; Tissot-Dupont, H.; et al. Outcomes of 3,737 COVID-19 patients treated with hydroxychloroquine/azithromycin and other regimens in Marseille France: A retrospective analysis. Travel Med. Infect. Dis. 2020, 36, 101791. [Google Scholar] [CrossRef]
- Courtejoie, N.; Dubost, C.L. Parcours Hospitaliers des Patients Atteints de la Covid-19 lors de la Première Vague de l’épidémie. Les Dossiers de la. DRESS N°67. 2020. Available online: https://drees.solidarites-sante.gouv.fr/sites/default/files/2020-10/DD67.pdf (accessed on 11 June 2021).
- Colson, P.; Levasseur, A.; Gautret, P.; Fenollar, F.; Thuan Hoang, V.; Delerce, J.; Bitam, I.; Saile, R.; Maaloum, M.; Padane, A.; et al. Introduction into the Marseille geographical area of a mild SARS-CoV-2 variant originating from sub-Saharan Africa: An investigational study. Travel Med. Infect. Dis. 2021, 40, 101980. [Google Scholar] [CrossRef]
- Fournier, P.E.; Colson, P.; Levasseur, A.; Devaux, C.A.; Gautret, P.; Bedotto, M.; Delerce, J.; Brechard, L.; Pinault, L.; Lagier, J.C.; et al. Emergence and outcomes of the SARS-CoV-2 ‘Marseille-4’ variant. Int. J. Infect. Dis. 2021, 106, 228–236. [Google Scholar] [CrossRef] [PubMed]
- Wise, J. Covid-19: New coronavirus variant is identified in UK. BMJ 2020, 371, m4857. [Google Scholar] [CrossRef]
- Makoni, M. South Africa responds to new SARS-CoV-2 variant. Lancet 2021, 397, 267. [Google Scholar] [CrossRef]
- Jain, A.; Rophina, M.; Mahajan, S.; Krishnan, B.B.; Sharma, M.; Mandal, S.; Fernandez, T.; Sultanji, S.; Jolly, B.; Mathew, S.; et al. Analysis of the potential impact of genomic variants in global SARS-CoV-2 genomes on molecular diagnostic assays. Int. J. Infect. Dis. 2021, 102, 460–462. [Google Scholar] [CrossRef]
- Arlotto, S.; Gares, A.; Giraud-Gatineau, A.; Lagier, J.-C.; Jimeno, M.T.; Peretti-Watel, P.; Million, M.; Parola, P.; Brouqui, P.; Raoult, D.; et al. Life-Years Lost by COVID-19 Patients in Public Hospitals of Marseille (APHM- South-Eastern France): A Limited Death Toll. Available online: https://www.mediterranee-infection.com/wp-content/uploads/2020/04/2021-01-26bis-DEATHCOVID.pdf (accessed on 25 May 2021).
- Brouqui, P.; Amrane, S.; Million, M.; Cortaredona, S.; Parola, P.; Lagier, J.C.; Raoult, D. Asymptomatic hypoxia in COVID-19 is associated with poor outcome. Int. J. Infect. Dis. 2020, 102, 233–238. [Google Scholar] [CrossRef] [PubMed]
- Camoin-Jo, L.; Gautret, P.; Colson, P.; Lagier, J.C.; Tissot-Dupont, H.; Million, M.; Giraud-Gatineau, A.; Boudjema, S.; Chaudet, H.; Raoult, D.; et al. High Prevalence of Lupus Anticoagulant in Ambulatory COVID-19 Patients: Interest of Hydroxychloroquine?-IHU. (n.d.) Available online: https://www.mediterranee-infection.com/high-prevalence-of-lupus-anticoagulant-in-ambulatory-covid-19-patients-interest-of-hydroxychloroquine/ (accessed on 19 November 2020).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Countries | Number of COVID-19 Tests per 1000 Inhabitants | Lockdown | Overall Government Response Severity Index | Date Where the Severity Index Is Max |
|---|---|---|---|---|
| Italy | 64.7 | Require not leaving house with minimal exceptions (e.g., allowed to leave once a week, or only one person can leave at a time, etc.) | 93.52 | 12 April 2020 |
| France | 13 | Require not leaving house with exceptions for daily exercise, grocery shopping, and “essential” trips | 90.74 | 17 March 2020 |
| Spain | 54.2 | Require not leaving house with exceptions for daily exercise, grocery shopping, and “essential” trips | 85.19 | 30 March 2020 |
| Belgium | 60.2 | Require not leaving house with exceptions for daily exercise, grocery shopping, and “essential” trips | 81.48 | 20 March 2020 |
| Netherlands | 20.4 | Require not leaving house with exceptions for daily exercise, grocery shopping, and “essential” trips | 79.63 | 31 March 2020 |
| Norway | 45.3 | No measures | 75.93 | 24 March 2020 |
| United Kingdom | 31.6 | Require not leaving house with exceptions for daily exercise, grocery shopping, and “essential” trips | 75.93 | 26 March 2020 |
| Germany | 47.2 | Require not leaving house with exceptions for daily exercise, grocery shopping, and “essential” trips | 73.15 | 22 March 2020 |
| Denmark | 91.3 | Recommend not leaving house | 72.22 | 18 March 2020 |
| Finland | 33.4 | Recommend not leaving house | 68.52 | 28 March 2020 |
| Iceland | 179.0 | No measures | 53.7 | 20 March 2020 |
| Sweden | 23.7 | No measures | 46.3 | 24 April 2020 |
| 2020 vs. 2018 | ||||||||||
| Sud | Ile-de-France | Grand-Est | New-Aquitaine | France | ||||||
| n | Number of Excess Deaths (% Excess) | n | Number of Excess Deaths (% Excess) | n | Number of Excess Deaths (% Excess) | n | Number of Excess Deaths (% Excess) | n | Number of Excess Deaths (% Excess) | |
| Deaths from all causes | 34,176 | 321 (0.9%) | 50,386 | 10,966 (21.8%) | 36,194 | 4150 (11.5%) | 44,017 | −1175 (−2.7%) | 411,271 | 18,983 (4.6%) |
| Deaths from all causes in public or private hospitals | 17,695 | −1039 (−5.9%) | 30,790 | 4622 (15.0%) | 21,099 | 1017 (4.8%) | 22,485 | −1063 (−4.7%) | 219,669 | −1104 (−0.5%) |
| Deaths from all causes in hospice or among dependent elderly residents in retirement homes | 3981 | 190 (4.8%) | 5196 | 2493 (48.0%) | 5078 | 1463 (28.8%) | 6859 | −3 (0.0%) | 51,634 | 5908 (11.4%) |
| Deaths from all causes at home | 9721 | 597 (6.1%) | 10,674 | 3119 (29.2%) | 7979 | 1083 (13.6%) | 10,931 | 100 (0.9%) | 98,624 | 7060 (7.2%) |
| 2020 vs. 2019 | ||||||||||
| Sud | Ile-de-France | Grand-Est | New-Aquitaine | France | ||||||
| n | Number of Excess Deaths (% Excess) | n | Number of Excess Deaths (% Excess) | n | Number of Excess Deaths (% Excess) | n | Number of Excess Deaths (% Excess) | n | Number of Excess Deaths (% Excess) | |
| Deaths from all causes | 34,267 | 230 (0.7%) | 50,556 | 10,796 (21.4%) | 35,654 | 4690 (13.2%) | 43,791 | −949 (−2.2%) | 409,835 | 20,419 (5.0%) |
| Deaths from all causes in public or private hospital | 17,784 | −1128 (−6.3%) | 31,045 | 4367 (14.1%) | 20,534 | 1582 (7.7%) | 22,266 | −844 (−3.8%) | 217,409 | 1156 (0.5%) |
| Deaths from all causes in hospice or among dependent elderly residents in retirement homes | 4135 | 36 (0.9%) | 4952 | 2737 (55.3%) | 4862 | 1679 (34.5%) | 6473 | 383 (5.9%) | 49,578 | 7964 (16.1%) |
| Deaths from all causes at home | 9659 | 659 (6.8%) | 10,843 | 2950 (27.2%) | 7976 | 1086 (13.6%) | 10,686 | 345 (3.2%) | 96,429 | 9255 (9.6%) |
| Region | Population Size (Inhabitants) | Seroprevalence (%) | Number of Estimated COVID-19 Cases on the Basis of Seroprevalence | Number of Estimated Deaths Using a 0.5% Probability of Death | Estimated COVID-19 Mortality per Million Inhabitants | Number of Observed Deaths (as of 2 June) | Ratio of Estimated to Observed Deaths | COVID-19 Mortality per Million Inhabitants |
|---|---|---|---|---|---|---|---|---|
| Ile-de-France | 12,278,210 | 10 | 1,227,821 | 6139 | 500 | 7273 | 0.84 | 592 |
| Grand-Est | 5,511,747 | 9 | 496,057 | 2480 | 450 | 3565 | 0.70 | 647 |
| New-Aquitaine | 5,999,982 | 3.1 | 185,999 | 930 | 155 | 420 | 2.21 | 70 |
| Bouches-du-Rhône | 2,034,469 | 7.96 | 161,944 | 810 | 398 | 535 | 1.51 | 263 |
| 2020 vs. 2018 | 2020 vs. 2019 | |||||||
|---|---|---|---|---|---|---|---|---|
| Paris | Marseille | Paris | Marseille | |||||
| n | Number of Excess Deaths (% Excess) | n | Number of Excess Deaths (% excess) | n | Number of Excess Deaths (% Excess) | n | Number of Excess Deaths (% Excess) | |
| Deaths from all causes | 9243 | 1961 (21.2%) | 5015 | 384 (7.7%) | 9192 | 2012 (21.9%) | 5028 | 371 (7.4%) |
| Deaths from all causes in public or private hospitals | 5960 | 806 (13.5%) | 2852 | −164 (−5.8%) | 5830 | 936 (16.1%) | 2761 | −73 (−2.6%) |
| Deaths from all causes in hospice or among dependent elderly residents in retirement homes | 565 | 400 (70.8%) | 248 | 59 (23.8%) | 597 | 368 (61.6%) | 302 | 5 (1.7%) |
| Deaths from all causes at home | 2319 | 737 (31.8) | 1732 | 70 (4.0%) | 2426 | 630 (26.0%) | 1812 | −10 (0.6%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giraud-Gatineau, A.; Gautret, P.; Colson, P.; Chaudet, H.; Raoult, D. Evaluation of Strategies to Fight COVID-19: The French Paradigm. J. Clin. Med. 2021, 10, 2942. https://doi.org/10.3390/jcm10132942
Giraud-Gatineau A, Gautret P, Colson P, Chaudet H, Raoult D. Evaluation of Strategies to Fight COVID-19: The French Paradigm. Journal of Clinical Medicine. 2021; 10(13):2942. https://doi.org/10.3390/jcm10132942
Chicago/Turabian StyleGiraud-Gatineau, Audrey, Philippe Gautret, Philippe Colson, Hervé Chaudet, and Didier Raoult. 2021. "Evaluation of Strategies to Fight COVID-19: The French Paradigm" Journal of Clinical Medicine 10, no. 13: 2942. https://doi.org/10.3390/jcm10132942
APA StyleGiraud-Gatineau, A., Gautret, P., Colson, P., Chaudet, H., & Raoult, D. (2021). Evaluation of Strategies to Fight COVID-19: The French Paradigm. Journal of Clinical Medicine, 10(13), 2942. https://doi.org/10.3390/jcm10132942