
Long-Term Outcomes of Patients with Coronavirus Disease 2019 at One Year after Hospital Discharge

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source and Study Variables
2.2. Study Procedures
2.3. Study Procedures
2.4. Ethics
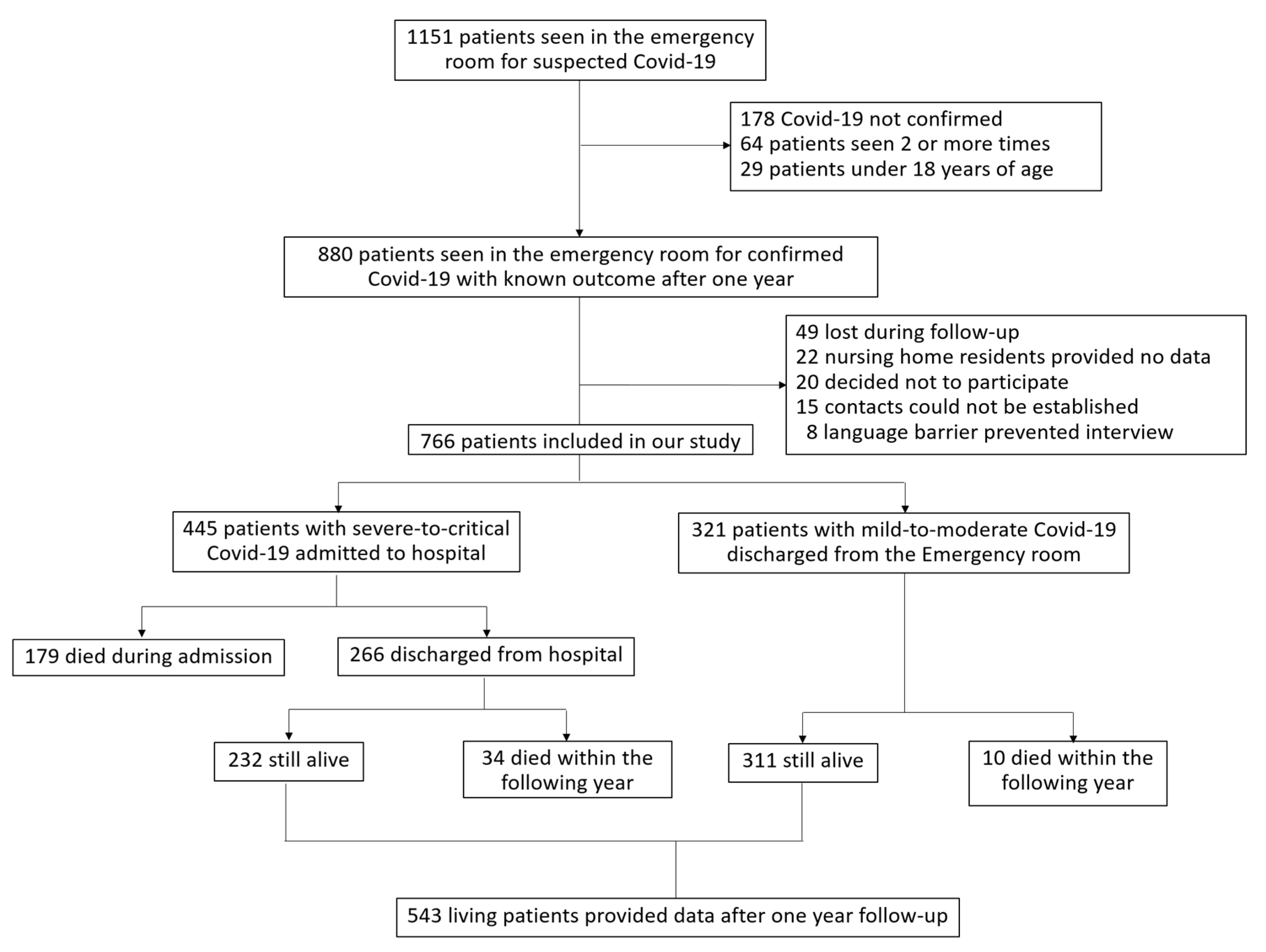
3. Results
3.1. Demographic and Clinical Characteristics of Hospitalized and Discharged Patients
3.2. One-Year Mortality Rates after COVID-19 Discharge and Causes of Death
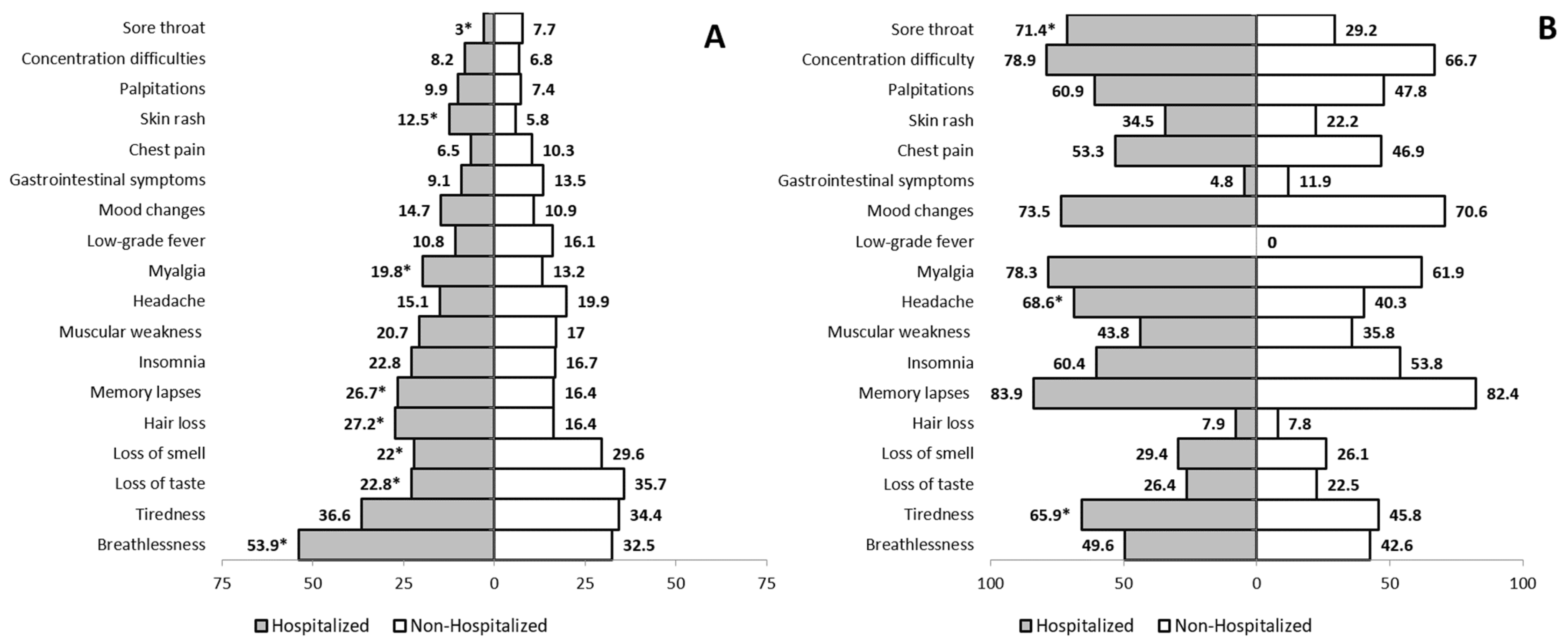
3.3. Recovered and Ongoing Symptoms after COVID-19
3.4. Complications after Acute COVID-19
3.5. Worsening of Concomitant Diseases during the Year after COVID-19
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Li, Q.; Guan, X.; Wu, P.; Wang, X.; Zhou, L.; Tong, Y.; Ren, R.; Leung, K.S.M.; Lau, E.H.Y.; Wong, J.Y.; et al. Early Transmission Dynamics in Wuhan, China, of Novel Coronavirus–Infected Pneumonia. N. Engl. J. Med. 2020, 382, 1199–1207. [Google Scholar] [CrossRef]
- Coronaviridae Study Group of the International Committee on Taxonomy of Viruses. The Species Severe Acute Respiratory Syndrome-Related Coronavirus: Classifying 2019-NCoV and Naming It SARS-CoV-2. Nat. Microbiol. 2020, 5, 536–544. [Google Scholar] [CrossRef] [Green Version]
- Riera, R.; Bagattini, Â.M.; Pacheco, R.L.; Pachito, D.V.; Roitberg, F.; Ilbawi, A. Delays and Disruptions in Cancer Health Care Due to COVID-19 Pandemic: Systematic Review. JCO Glob. Oncol. 2021, 7, 311–323. [Google Scholar] [CrossRef]
- Kiss, P.; Carcel, C.; Hockham, C.; Peters, S.A.E. The Impact of the COVID-19 Pandemic on the Care and Management of Patients with Acute Cardiovascular Disease: A Systematic Review. Eur Heart J. Qual. Care Clin. Outcomes 2021, 7, 18–27. [Google Scholar] [CrossRef]
- Liang, L.; Yang, B.; Jiang, N.; Fu, W.; He, X.; Zhou, Y.; Ma, W.L.; Wang, X. Three-Month Follow-up Study of Survivors of Coronavirus Disease 2019 after Discharge. J. Korean Med. Sci. 2020, 35, e418. [Google Scholar] [CrossRef]
- Raman, B.; Cassar, M.P.; Tunnicliffe, E.M.; Filippini, N.; Griffanti, L.; Alfaro-Almagro, F.; Okell, T.; Sheerin, F.; Xie, C.; Mahmod, M.; et al. Medium-Term Effects of SARS-CoV-2 Infection on Multiple Vital Organs, Exercise Capacity, Cognition, Quality of Life and Mental Health, Post-Hospital Discharge. EClinicalMedicine 2021, 31, 100683. [Google Scholar] [CrossRef] [PubMed]
- Gautam, N.; Madathil, S.; Tahani, N.; Bolton, S.; Parekh, D.; Stockley, J.; Goyal, S.; Qureshi, H.; Yasmin, S.; Cooper, B.G.; et al. Medium-Term Outcome of Severe to Critically Ill Patients with SARS-CoV-2 Infection. Clin. Infect. Dis. 2021, ciab341. [Google Scholar] [CrossRef]
- Carfì, A.; Bernabei, R.; Landi, F.; Gemelli Against COVID-19 Post-Acute Care Study Group. Persistent Symptoms in Patients After Acute COVID-19. JAMA 2020, 324, 603–605. [Google Scholar] [CrossRef] [PubMed]
- Mandal, S.; Barnett, J.; Brill, S.E.; Brown, J.S.; Denneny, E.K.; Hare, S.S.; Heightman, M.; Hillman, T.E.; Jacob, J.; Jarvis, H.C.; et al. “Long-COVID”: A Cross-Sectional Study of Persisting Symptoms, Biomarker and Imaging Abnormalities Following Hospitalisation for COVID-19. Thorax 2020. [Google Scholar] [CrossRef]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-Month Consequences of COVID-19 in Patients Discharged from Hospital: A Cohort Study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical Course and Risk Factors for Mortality of Adult Inpatients with COVID-19 in Wuhan, China: A Retrospective Cohort Study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Cares-Marambio, K.; Montenegro-Jiménez, Y.; Torres-Castro, R.; Vera-Uribe, R.; Torralba, Y.; Alsina-Restoy, X.; Vasconcello-Castillo, L.; Vilaró, J. Prevalence of Potential Respiratory Symptoms in Survivors of Hospital Admission after Coronavirus Disease 2019 (COVID-19): A Systematic Review and Meta-Analysis. Chron. Respir. Dis. 2021, 18, 14799731211002240. [Google Scholar] [CrossRef]
- Garg, P.; Arora, U.; Kumar, A.; Wig, N. The “Post-COVID” Syndrome: How Deep Is the Damage? J. Med. Virol. 2021, 93, 673–674. [Google Scholar] [CrossRef]
- Yelin, D.; Wirtheim, E.; Vetter, P.; Kalil, A.C.; Bruchfeld, J.; Runold, M.; Guaraldi, G.; Mussini, C.; Gudiol, C.; Pujol, M.; et al. Long-Term Consequences of COVID-19: Research Needs. Lancet Infect. Dis. 2020, 20, 1115–1117. [Google Scholar] [CrossRef]
- Maestre-Muñiz, M.M.; Arias, Á.; Arias-González, L.; Angulo-Lara, B.; Lucendo, A.J. Prognostic Factors at Admission for In-Hospital Mortality from COVID-19 Infection in an Older Rural Population in Central Spain. J. Clin. Med. 2021, 10, 318. [Google Scholar] [CrossRef] [PubMed]
- National Institutes of Health (NIH). Clinical Spectrum|COVID-19 Treatment Guidelines. Available online: https://www.covid19treatmentguidelines.nih.gov/overview/clinical-spectrum/ (accessed on 24 June 2021).
- WHO Working Group on the Clinical Characterisation and Management of COVID-19 Infection. A Minimal Common Outcome Measure Set for COVID-19 Clinical Research. Lancet Infect. Dis. 2020, 20, e192–e197. [Google Scholar] [CrossRef]
- Bestall, J.C.; Paul, E.A.; Garrod, R.; Garnham, R.; Jones, P.W.; Wedzicha, J.A. Usefulness of the Medical Research Council (MRC) Dyspnoea Scale as a Measure of Disability in Patients with Chronic Obstructive Pulmonary Disease. Thorax 1999, 54, 581–586. [Google Scholar] [CrossRef] [Green Version]
- Global Initiative for Chronic Obstructive Lung Disease. Global Strategy for Prevention, Diagnosis, and Management of Chronic Obstructive Pulmonary Disease. 2021. Available online: https://goldcopd.org (accessed on 23 June 2021).
- Ginasthma.Org. GINA Asthma Treatment Steps for Adults: Global Initiative for Asthma (GINA) 2019 Guidelines for Asthma Management and Prevention. Available online: https://ginasthma.org/reports/ (accessed on 30 May 2021).
- The Criteria Committee of the New York Heart Association. Nomenclature and Criteria for Diagnosis of Diseases of the Heart and Great Vessels, 9th ed.; Little, Brown and Company: Boston, MA, USA, 1994. [Google Scholar]
- Wells, G.; Becker, J.-C.; Teng, J.; Dougados, M.; Schiff, M.; Smolen, J.; Aletaha, D.; Van Riel, P.L.C.M. Validation of the 28-Joint Disease Activity Score (DAS28) and European League Against Rheumatism Response Criteria Based on C-Reactive Protein against Disease Progression in Patients with Rheumatoid Arthritis, and Comparison with the DAS28 Based on Erythrocyte Sedimentation Rate. Ann. Rheum Dis. 2009, 68, 954–960. [Google Scholar] [CrossRef]
- Garrett, S.; Jenkinson, T.; Kennedy, L.G.; Whitelock, H.; Gaisford, P.; Calin, A. A New Approach to Defining Disease Status in Ankylosing Spondylitis: The Bath Ankylosing Spondylitis Disease Activity Index. J. Rheumatol. 1994, 21, 2286–2291. [Google Scholar]
- Wade, D.T.; Collin, C. The Barthel ADL Index: A Standard Measure of Physical Disability? Int. Disabil. Stud. 1988, 10, 64–67. [Google Scholar] [CrossRef]
- Graf, C. The Lawton Instrumental Activities of Daily Living Scale. Am. J. Nurs. 2008, 108, 52–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- San José Laporte, A.; Jacas Escarcellé, C.; Selva O’Callaghan, A.; Vilardell Tarrés, M. Protocolo de Valoración Geriátrica. Medicine 1999, 7, 5829–5832. [Google Scholar]
- Reisberg, B.; Ferris, S.H.; De Leon, M.J.; Crook, T. Global Deterioration Scale (GDS). Psychopharmacol. Bull. 1988, 24, 661–663. [Google Scholar]
- Lund, L.C.; Hallas, J.; Nielsen, H.; Koch, A.; Mogensen, S.H.; Brun, N.C.; Christiansen, C.F.; Thomsen, R.W.; Pottegård, A. Post-Acute Effects of SARS-CoV-2 Infection in Individuals Not Requiring Hospital Admission: A Danish Population-Based Cohort Study. Lancet Infect. Dis. 2021. [Google Scholar] [CrossRef]
- Pavli, A.; Theodoridou, M.; Maltezou, H.C. Post-COVID Syndrome: Incidence, Clinical Spectrum, and Challenges for Primary Healthcare Professionals. Arch. Med. Res. 2021. [Google Scholar] [CrossRef] [PubMed]
- Gallo Marin, B.; Aghagoli, G.; Lavine, K.; Yang, L.; Siff, E.J.; Chiang, S.S.; Salazar-Mather, T.P.; Dumenco, L.; Savaria, M.C.; Aung, S.N.; et al. Predictors of COVID-19 Severity: A Literature Review. Rev. Med. Virol. 2021, 31, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Guan, W.; Liang, W.; Zhao, Y.; Liang, H.; Chen, Z.; Li, Y.; Liu, X.; Chen, R.; Tang, C.; Wang, T.; et al. Comorbidity and Its Impact on 1590 Patients with COVID-19 in China: A Nationwide Analysis. Eur. Respir. J. 2020, 55, 2000547. [Google Scholar] [CrossRef] [Green Version]
- Bajgain, K.T.; Badal, S.; Bajgain, B.B.; Santana, M.J. Prevalence of Comorbidities among Individuals with COVID-19: A Rapid Review of Current Literature. Am. J. Infect. Control. 2021, 49, 238–246. [Google Scholar] [CrossRef]
- Medrano Albero, M.J.; Boix Martínez, R.; Cerrato Crespán, E.; Ramírez Santa-Pau, M. Incidencia y Prevalencia de Cardiopatía Isquémica y Enfermedad Cerebrovascular En España: Revisión Sistemática de La Literatura. Rev. Esp. Salud Publica 2006, 80, 5–15. [Google Scholar] [CrossRef] [Green Version]
- Ministry of Health, Consumption and Social Welfare National Health Survey. Spain 2017 Main Results. Available online: https://www.mscbs.gob.es/estadEstudios/estadisticas/encuestaNacional/encuestaNac2017/ENSE2017_notatecnica.pdf (accessed on 30 May 2021).
- Brix, T.H.; Hegedüs, L.; Hallas, J.; Lund, L.C. Risk and Course of SARS-CoV-2 Infection in Patients Treated for Hypothyroidism and Hyperthyroidism. Lancet Diabetes Endocrinol. 2021, 9, 197–199. [Google Scholar] [CrossRef]
- Zhang, S.; Zhang, J.; Wang, C.; Chen, X.; Zhao, X.; Jing, H.; Liu, H.; Li, Z.; Wang, L.; Shi, J. COVID-19 and Ischemic Stroke: Mechanisms of Hypercoagulability (Review). Int. J. Mol. Med. 2021, 47, 21. [Google Scholar] [CrossRef]
- Moreno-Pérez, O.; Merino, E.; Leon-Ramirez, J.-M.; Andres, M.; Ramos, J.M.; Arenas-Jiménez, J.; Asensio, S.; Sanchez, R.; Ruiz-Torregrosa, P.; Galan, I.; et al. Post-Acute COVID-19 Syndrome. Incidence and Risk Factors: A Mediterranean Cohort Study. J. Infect. 2021, 82, 378–383. [Google Scholar] [CrossRef]
- Tenforde, M.W.; Kim, S.S.; Lindsell, C.J.; Billig Rose, E.; Shapiro, N.I.; Files, D.C.; Gibbs, K.W.; Erickson, H.L.; Steingrub, J.S.; Smithline, H.A.; et al. Symptom Duration and Risk Factors for Delayed Return to Usual Health Among Outpatients with COVID-19 in a Multistate Health Care Systems Network—United States, March–June 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 993–998. [Google Scholar] [CrossRef] [PubMed]
- Halpin, S.J.; McIvor, C.; Whyatt, G.; Adams, A.; Harvey, O.; McLean, L.; Walshaw, C.; Kemp, S.; Corrado, J.; Singh, R.; et al. Postdischarge Symptoms and Rehabilitation Needs in Survivors of COVID-19 Infection: A Cross-sectional Evaluation. J. Med. Virol. 2021, 93, 1013–1022. [Google Scholar] [CrossRef] [PubMed]
- Dennis, A.; Wamil, M.; Alberts, J.; Oben, J.; Cuthbertson, D.J.; Wootton, D.; Crooks, M.; Gabbay, M.; Brady, M.; Hishmeh, L.; et al. Multiorgan Impairment in Low-Risk Individuals with Post-COVID-19 Syndrome: A Prospective, Community-Based Study. BMJ Open 2021, 11, e048391. [Google Scholar] [CrossRef] [PubMed]
- Salisbury, R.; Iotchkova, V.; Jaafar, S.; Morton, J.; Sangha, G.; Shah, A.; Untiveros, P.; Curry, N.; Shapiro, S. Incidence of Symptomatic, Image-Confirmed Venous Thromboembolism Following Hospitalization for COVID-19 with 90-Day Follow-Up. Blood Adv. 2020, 4, 6230–6239. [Google Scholar] [CrossRef] [PubMed]
- Modin, D.; Claggett, B.; Sindet-Pedersen, C.; Lassen, M.C.H.; Skaarup, K.G.; Jensen, J.U.S.; Fralick, M.; Schou, M.; Lamberts, M.; Gerds, T.; et al. Acute COVID-19 and the Incidence of Ischemic Stroke and Acute Myocardial Infarction. Circulation 2020, 142, 2080–2082. [Google Scholar] [CrossRef]
- Halushka, M.K.; Vander Heide, R.S. Myocarditis Is Rare in COVID-19 Autopsies: Cardiovascular Findings across 277 Postmortem Examinations. Cardiovasc. Pathol. 2021, 50, 107300. [Google Scholar] [CrossRef]
- López-González, M.-C.; Peral-Garrido, M.L.; Calabuig, I.; Tovar-Sugrañes, E.; Jovani, V.; Bernabeu, P.; García-Sevila, R.; León-Ramírez, J.-M.; Moreno-Perez, O.; Boix, V.; et al. Case Series of Acute Arthritis during COVID-19 Admission. Ann. Rheum. Dis. 2021, 80, e58. [Google Scholar] [CrossRef]
- Di Carlo, M.; Tardella, M.; Salaffi, F. Can SARS-CoV-2 Induce Reactive Arthritis? Clin. Exp. Rheumatol 2021, 39 (Suppl. 128), 25–26. [Google Scholar]
- Doykov, I.; Hällqvist, J.; Gilmour, K.C.; Grandjean, L.; Mills, K.; Heywood, W.E. ‘The Long Tail of Covid-19′—The Detection of a Prolonged Inflammatory Response after a SARS-CoV-2 Infection in Asymptomatic and Mildly Affected Patients. F1000Res 2021, 9, 1349. [Google Scholar] [CrossRef]
- Malik, M.I.; Fox, N.; Chopra, A.; Hughes, H.Y.; Washburn, R.; Huggins, J.T. Positive Pleural Fluid RT-PCR for Virus Detection in SARS-CoV-2 Pneumonia. QJM Int. J. Med. 2020, 113, 888–889. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.; Wang, X.; Ren, J.; Sun, Y.; Yu, R.; Li, K.; Zheng, L.; Yang, J. Risk Factors and Prognosis for COVID-19-Induced Acute Kidney Injury: A Meta-Analysis. BMJ Open 2020, 10, e042573. [Google Scholar] [CrossRef] [PubMed]
- Chan, K.W.; Hung, I.F.-N.; Tsang, O.T.-Y.; Wu, T.C.; Tso, E.Y.-K.; Lung, K.C.; Lam, C.M.; Chan, G.C.-W.; Wong, S.S.-H.; Yu, K.Y.; et al. Mass Screening Is Associated with Low Rates of Acute Kidney Injury among COVID-19 Patients in Hong Kong. Am. J. Nephrol. 2021, 52, 161–172. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.; Li, X.; Song, Q.; Hu, C.; Su, F.; Dai, J.; Ye, Y.; Huang, J.; Zhang, X. Assessment of Hypokalemia and Clinical Characteristics in Patients with Coronavirus Disease 2019 in Wenzhou, China. JAMA Netw. Open 2020, 3, e2011122. [Google Scholar] [CrossRef]
- Weir, M.R.; Rolfe, M. Potassium Homeostasis and Renin-Angiotensin-Aldosterone System Inhibitors. Clin. J. Am. Soc. Nephrol. 2010, 5, 531–548. [Google Scholar] [CrossRef] [Green Version]
- Nuzzi, V.; Castrichini, M.; Collini, V.; Roman-Pognuz, E.; Di Bella, S.; Luzzati, R.; Berlot, G.; Confalonieri, M.; Merlo, M.; Stolfo, D.; et al. Impaired Right Ventricular Longitudinal Strain Without Pulmonary Hypertension in Patients Who Have Recovered From COVID-19. Circ. Cardiovasc. Imaging 2021, 14, e012166. [Google Scholar] [CrossRef]
- Pagnesi, M.; Baldetti, L.; Beneduce, A.; Calvo, F.; Gramegna, M.; Pazzanese, V.; Ingallina, G.; Napolano, A.; Finazzi, R.; Ruggeri, A.; et al. Pulmonary Hypertension and Right Ventricular Involvement in Hospitalised Patients with COVID-19. Heart 2020, 106, 1324–1331. [Google Scholar] [CrossRef]
- Cortés-Telles, A.; López-Romero, S.; Figueroa-Hurtado, E.; Pou-Aguilar, Y.N.; Wong, A.W.; Milne, K.M.; Ryerson, C.J.; Guenette, J.A. Pulmonary Function and Functional Capacity in COVID-19 Survivors with Persistent Dyspnoea. Respir. Physiol. Neurobiol. 2021, 288, 103644. [Google Scholar] [CrossRef]
- Ahmed, H.; Patel, K.; Greenwood, D.; Halpin, S.; Lewthwaite, P.; Salawu, A.; Eyre, L.; Breen, A.; O’Connor, R.; Jones, A.; et al. Long-Term Clinical Outcomes in Survivors of Severe Acute Respiratory Syndrome and Middle East Respiratory Syndrome Coronavirus Outbreaks after Hospitalisation or ICU Admission: A Systematic Review and Meta-Analysis. J. Rehabil. Med. 2020. [Google Scholar] [CrossRef]
- Celli, B.; Fabbri, L.M. Urgent need of a management plan for survivors of COVID-19. Eur. Respir. J. 2020, 55, 2000764. [Google Scholar] [CrossRef] [Green Version]
- Yasin, R.; Gomaa, A.A.K.; Ghazy, T.; Hassanein, S.A.; Ibrahem, R.A.L.; Khalifaet, M.H. Predicting lung fibrosis in post-COVID-19 patients after discharge with follow-up chest CT findings. Egypt J. Radiol. Nucl. Med. 2021, 52, 118. [Google Scholar] [CrossRef]
- Rai, D.K.; Sharma, P.; Kumar, R. Post covid 19 pulmonary fibrosis. Is it real threat? Indian J. Tuberc. 2021, 68, 330–333. [Google Scholar] [CrossRef]
- Hayden, M.R. An Immediate and Long-Term Complication of COVID-19 May Be Type 2 Diabetes Mellitus: The Central Role of β-Cell Dysfunction, Apoptosis and Exploration of Possible Mechanisms. Cells 2020, 9, 2475. [Google Scholar] [CrossRef] [PubMed]
- Baker, H.A.; Safavynia, S.A.; Evered, L.A. The ‘Third Wave’: Impending Cognitive and Functional Decline in COVID-19 Survivors. Br. J. Anaesth. 2021, 126, 44–47. [Google Scholar] [CrossRef]
- Walle-Hansen, M.M.; Ranhoff, A.H.; Mellingsæter, M.; Wang-Hansen, M.S.; Myrstad, M. Health-Related Quality of Life, Functional Decline, and Long-Term Mortality in Older Patients Following Hospitalisation Due to COVID-19. BMC Geriatr. 2021, 21, 199. [Google Scholar] [CrossRef] [PubMed]
- Miskowiak, K.; Johnsen, S.; Sattler, S.; Nielsen, S.; Kunalan, K.; Rungby, J.; Lapperre, T.; Porsberg, C. Cognitive Impairments Four Months after COVID-19 Hospital Discharge: Pattern, Severity and Association with Illness Variables. Eur. Neuropsychopharmacol. 2021, 46, 39–48. [Google Scholar] [CrossRef] [PubMed]
- Tam, M.T.; Dosso, J.A.; Robillard, J.M. The Impact of a Global Pandemic on People Living with Dementia and Their Care Partners: Analysis of 417 Lived Experience Reports. JAD 2021, 80, 865–875. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Total (n = 766) | Discharged from the Emergency Room (n = 321) | Admitted to Hospital (n = 445) | p-Value | ||
|---|---|---|---|---|---|
| Mean age at admission, years (SD; rank) | 65.1 (17.5; 18–98) | 56.2 (17.8; 18–96) | 71.5 (14.3; 20–98) | <0.001 | |
| Age group | Over 65 years old, n (%) | 418 (54.6%) | 104 (32.4%) | 314 (70.6%) | <0.001 |
| Younger than 65 years old, n (%) | 348 (45.4%) | 217 (67.6%) | 131 (29.4%) | ||
| Sex | Male, n (%) | 388 (50.7) | 177 (55.1) | 201 (45.2) | 0.006 |
| Female, n (%) | 378 (49.3) | 144 (44.9) | 244 (54.8) | ||
| Nursing home residents, n (%) | 75 (9.8) | 11 (3.4) | 64 (14.4) | <0.001 | |
| Previous comorbidities | Arterial hypertension, n (%) | 401 (52.3) | 101 (31.5) | 300 (67.4) | <0.001 |
| Diabetes, n (%) | 189 (24.7) | 39 (12.1) | 150 (33.7) | <0.001 | |
| Dyslipidemia, n (%) | 184 (24) | 48 (15) | 136 (30.6) | <0.001 | |
| Obesity, n (%) | 139 (18.1) | 45 (14) | 94 (21.1) | 0.012 | |
| Chronic kidney disease, n (%) | 70 (9.1) | 9 (2.8) | 61 (13.7) | <0.001 | |
| Cognitive impairment, n (%) | 69 (9) | 15 (4.7) | 54 (12.1) | <0.001 | |
| Ischemic heart disease, n (%) | 66 (8.6%) | 7 (2.2%) | 59 (13.3) | <0.001 | |
| Oncological disease, n (%) | 66 (8.6%) | 18 (5.6%) | 48 (10.8%) | 0.012 | |
| Sleep apnea/hypopnea syndrome, n (%) | 62 (8.1%) | 17 (5.3%) | 45 (10.1%) | 0.016 | |
| Hypothyroidism, n (%) | 61 (8%) | 22 (6.9%) | 39 (8.8%) | 0.335 | |
| Cerebrovascular diseases, n (%) | 56 (7.3%) | 9 (2.8%) | 47 (10.6%) | <0.001 | |
| Depressive syndrome, n (%) | 54 (7%) | 18 (5.6%) | 36 (8.1%) | 0.185 | |
| Chronic obstructive pulmonary disease, n (%) | 53 (6.9%) | 11 (3.4%) | 42 (9.4%) | 0.001 | |
| Bronchial asthma, n (%) | 51 (6.7%) | 25 (7.8%) | 26 (5.8%) | 0.287 | |
| Anemia, n (%) | 37 (4.8%) | 8 (2.5%) | 29 (6.5%) | 0.010 | |
| Chronic liver disease, n (%) | 34 (4.4%) | 8 (2.5%) | 26 (5.8%) | 0.026 | |
| Congestive heart failure, n (%) | 34 (4.4%) | 3 (0.9%) | 31 (7%) | <0.001 | |
| Connective tissue disorder, n (%) | 26 (3.4%) | 12 (3.7%) | 14 (3.1%) | 0.655 | |
| Blood dyscrasias, n (%) | 26 (3.4%) | 5 (1.6%) | 21 (4.7%) | 0.017 | |
| Peripheral vascular disease, n (%) | 18 (2.3%) | 3 (0.9%) | 15 (3.4%) | 0.028 | |
| Hyperuricemia, n (%) | 26 (3.4%) | 8 (2.5%) | 18 (4%) | 0.242 | |
| Any previous comorbidity, n (%) | 596 (77.8%) | 196 (61.1%) | 400 (89.9%) | <0.001 | |
| Complication | Total (n = 543) | Discharged from the Emergency Room (n = 311) | Admitted to Hospital (n = 232) | p-Value |
|---|---|---|---|---|
| Deep venous thrombosis | 13 (2.4%) | 5 (1.6%) | 8 (3.4%) | 0.165 |
| Pulmonary thromboembolism | 9 (1.7%) | 4 (1.3%) | 5 (2.2%) | 0.507 |
| High blood pressure onset | 12 (2.2%) | 8 (2.6%) | 4 (1.7%) | 0.506 |
| Diabetes debut | 6 (1.1%) | 3 (1%) | 3 (1.3%) | 0.704 |
| Pleural effusion | 4 (0.7%) | 1 (0.3%) | 3 (1.3%) | 0.318 |
| Acute myocardial infarction | 8 (1.5%) | 6 (1.9%) | 2 (0.9%) | 0.476 |
| Myocarditis or pericarditis | 2 (0.4%) | 1 (0.3%) | 1 (0.4%) | >0.999 |
| Stroke | 7 (1.3%) | 4 (1.3%) | 3 (1.3%) | >0.999 |
| Encephalitis | 1 (0.2%) | 0 | 1 (0.4%) | 0.427 |
| Renal failure | 4 (0.7%) | 0 | 4 (1.7%) | 0.033 |
| Arthritis | 13 (2.4%) | 7 (2.3%) | 6 (2.6%) | 0.800 |
| Diseases | Global (n = 543) |
|---|---|
| Chronic obstructive pulmonary disease (COPD) | n (%) |
| Newly diagnosed from COPD | 10 (1.8%) |
| Patients with COPD patients alive after one year/at baseline | 28/53 (53%) |
| New need of oxygen | 11/28 (39.3%) |
| Treatment intensification | 7/28 (25%) |
| New need of oxygen or treatment intensification | 17/28 (60.7%) |
| Bronchial asthma | |
| New appearance of asthma | 2 (0.4%) |
| Patients with asthma alive after one year/at baseline | 39/51 (76.5%) |
| Treatment intensification | 8/39 (20.5%) |
| Diabetes | |
| New debut of diabetes | 7 (1.3%) |
| Impaired glycemic control | 11 (2%) |
| Patients with diabetes alive after one year/at baseline | 109/189 (57.7%) |
| Impaired glycemic control | 11/109 (10.1%) |
| Intensification of oral therapy | 10/109 (9.2%) |
| New prescription of insulin | 5/109 (4.6%) |
| Development of peripheral neuropathy | 2/109 (2.7%) |
| Development of retinopathy | 3/109 (1.8%) |
| Heart failure | |
| New development of heart failure | 11 (2%) |
| Treatment intensification | 7 |
| Arthritis/Spondyloarthropathy | |
| New development of Arthritis/Spondyloarthropathy | 4 (0.7%) |
| Worsening pain control | 3 |
| Treatment intensification | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maestre-Muñiz, M.M.; Arias, Á.; Mata-Vázquez, E.; Martín-Toledano, M.; López-Larramona, G.; Ruiz-Chicote, A.M.; Nieto-Sandoval, B.; Lucendo, A.J. Long-Term Outcomes of Patients with Coronavirus Disease 2019 at One Year after Hospital Discharge. J. Clin. Med. 2021, 10, 2945. https://doi.org/10.3390/jcm10132945
Maestre-Muñiz MM, Arias Á, Mata-Vázquez E, Martín-Toledano M, López-Larramona G, Ruiz-Chicote AM, Nieto-Sandoval B, Lucendo AJ. Long-Term Outcomes of Patients with Coronavirus Disease 2019 at One Year after Hospital Discharge. Journal of Clinical Medicine. 2021; 10(13):2945. https://doi.org/10.3390/jcm10132945
Chicago/Turabian StyleMaestre-Muñiz, Modesto M., Ángel Arias, Emilia Mata-Vázquez, María Martín-Toledano, Germán López-Larramona, Ana María Ruiz-Chicote, Bárbara Nieto-Sandoval, and Alfredo J. Lucendo. 2021. "Long-Term Outcomes of Patients with Coronavirus Disease 2019 at One Year after Hospital Discharge" Journal of Clinical Medicine 10, no. 13: 2945. https://doi.org/10.3390/jcm10132945
APA StyleMaestre-Muñiz, M. M., Arias, Á., Mata-Vázquez, E., Martín-Toledano, M., López-Larramona, G., Ruiz-Chicote, A. M., Nieto-Sandoval, B., & Lucendo, A. J. (2021). Long-Term Outcomes of Patients with Coronavirus Disease 2019 at One Year after Hospital Discharge. Journal of Clinical Medicine, 10(13), 2945. https://doi.org/10.3390/jcm10132945