
Relationship of Corpus Callosum Integrity with Working Memory, Planning, and Speed of Processing in Patients with First-Episode and Chronic Schizophrenia

 , , ,
, , ,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Neuropsychological Assessments
2.3. Clinical Assessments
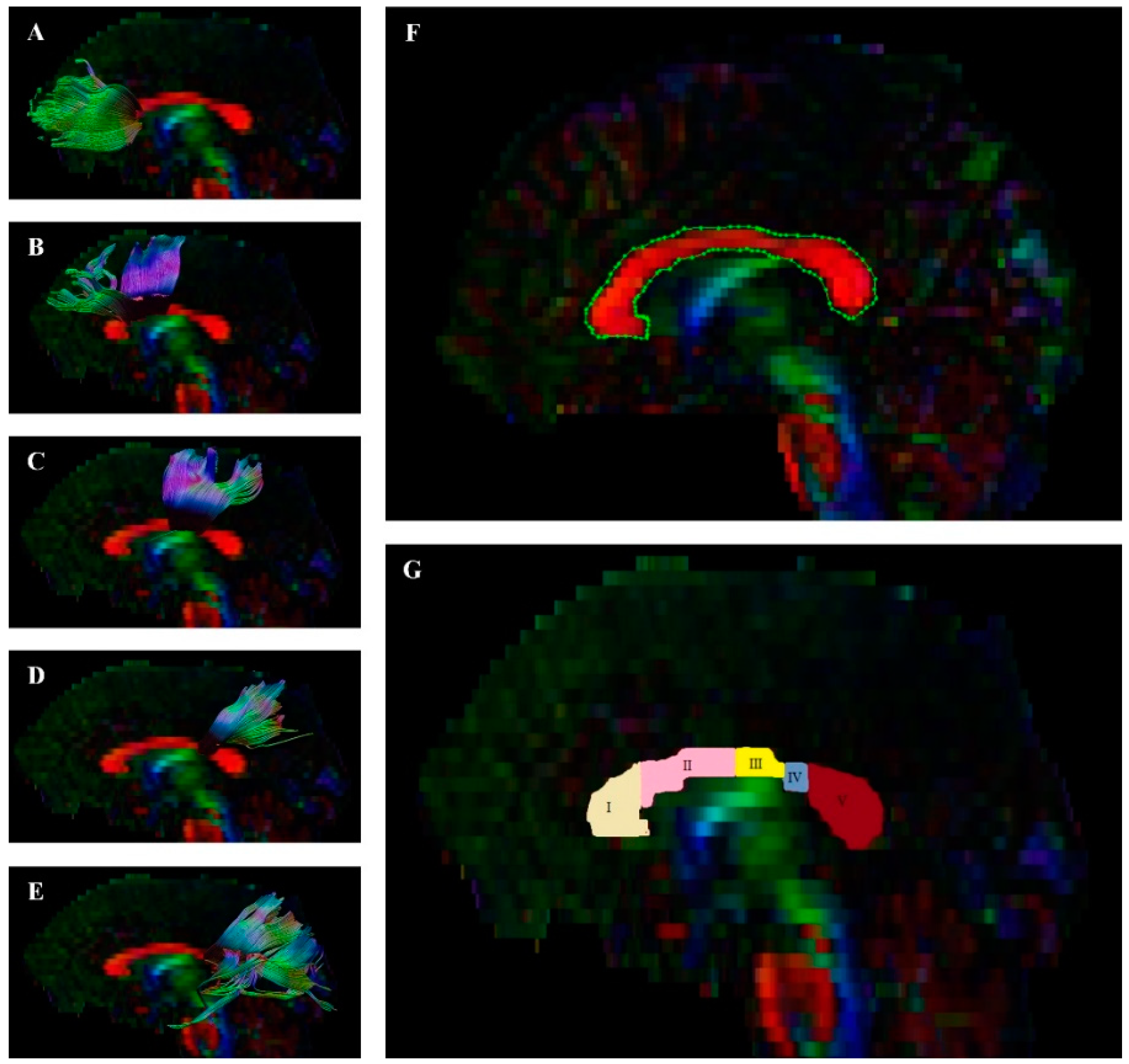
2.4. Acquisition of DTI
2.5. Image Processing and Quality
2.6. Procedure
2.7. Statistical Analysis
3. Results
3.1. Participant Characteristics
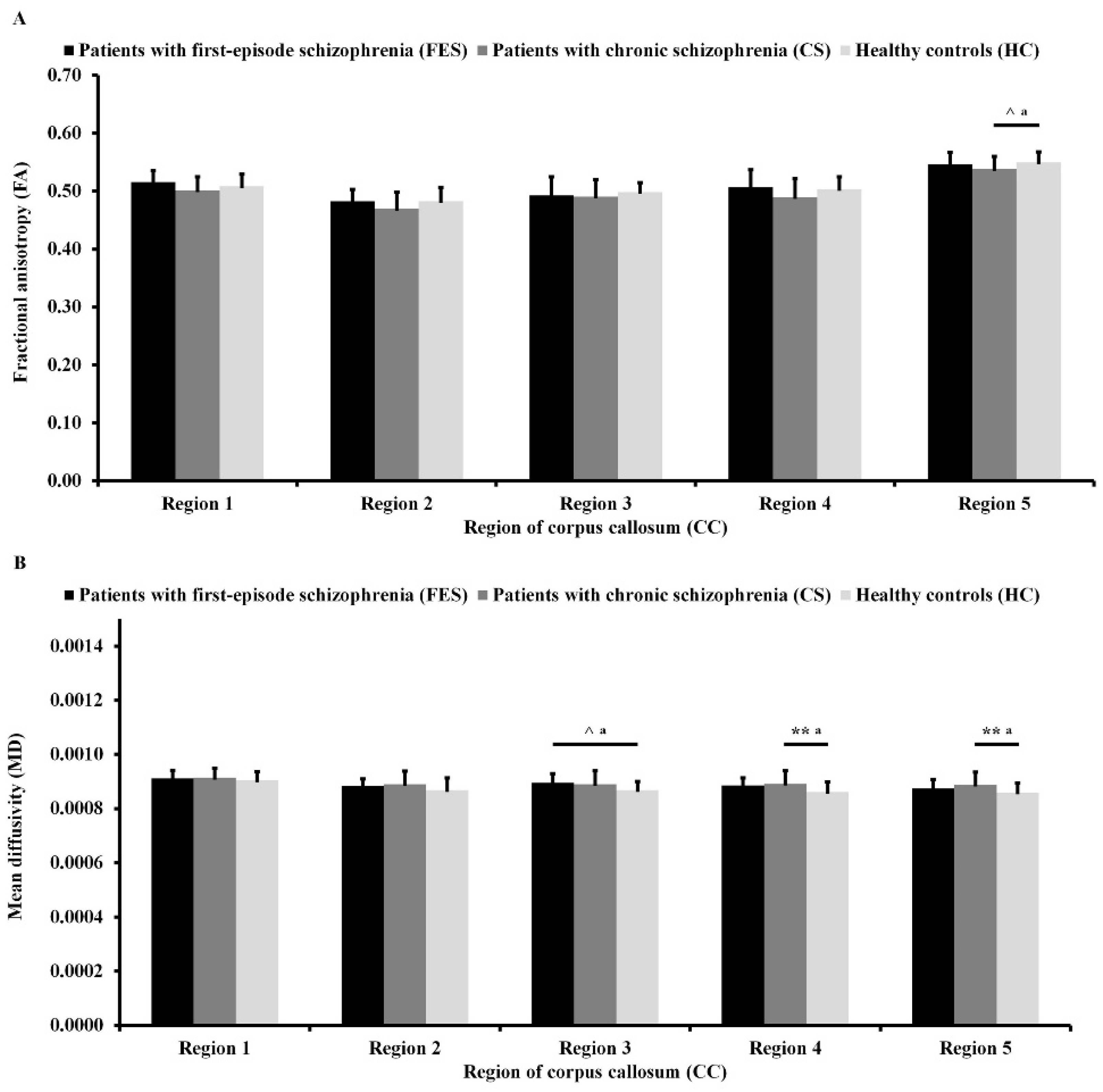
3.2. Differences in DTI Measures
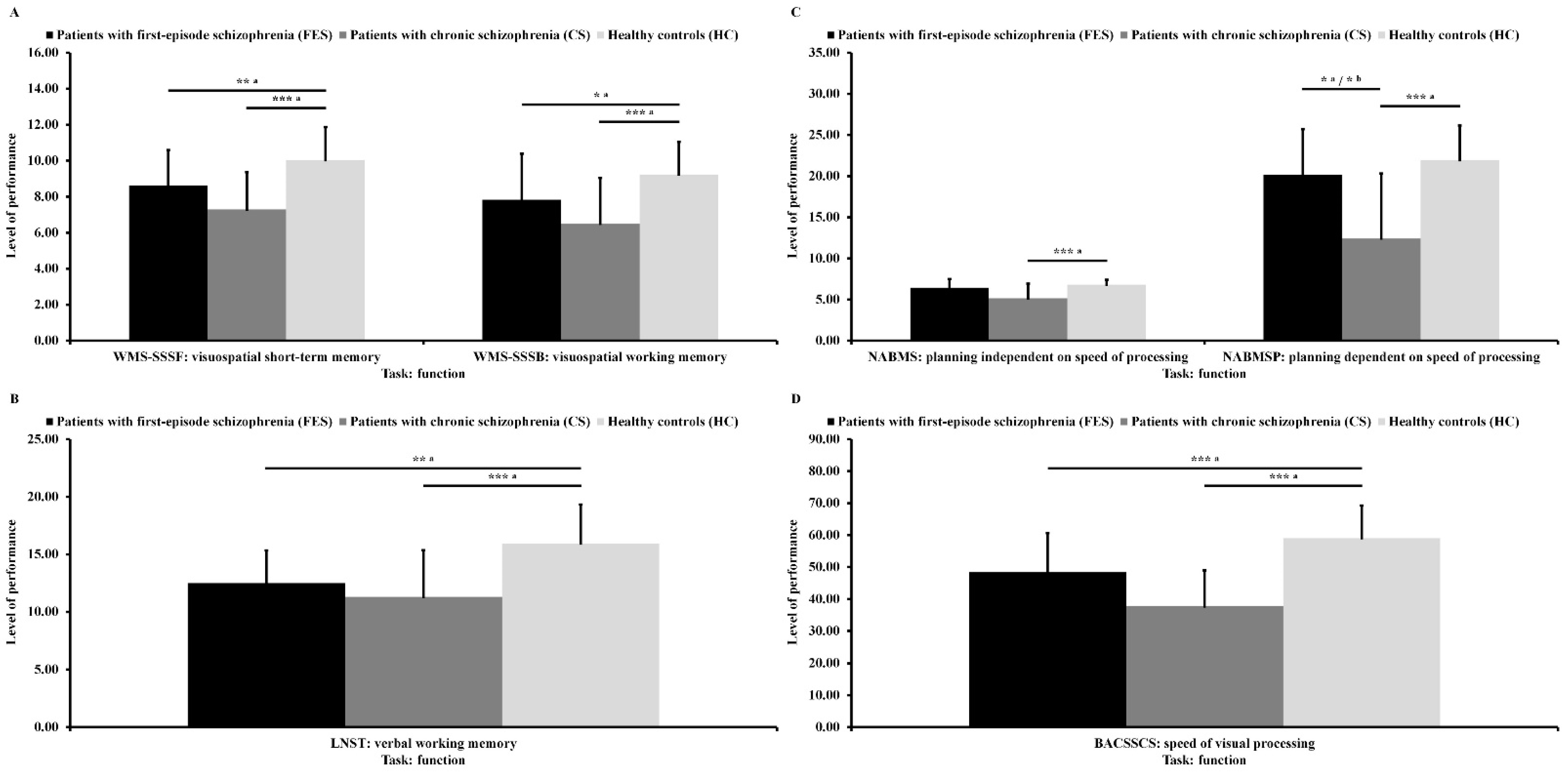
3.3. Differences in Cognitive Functions
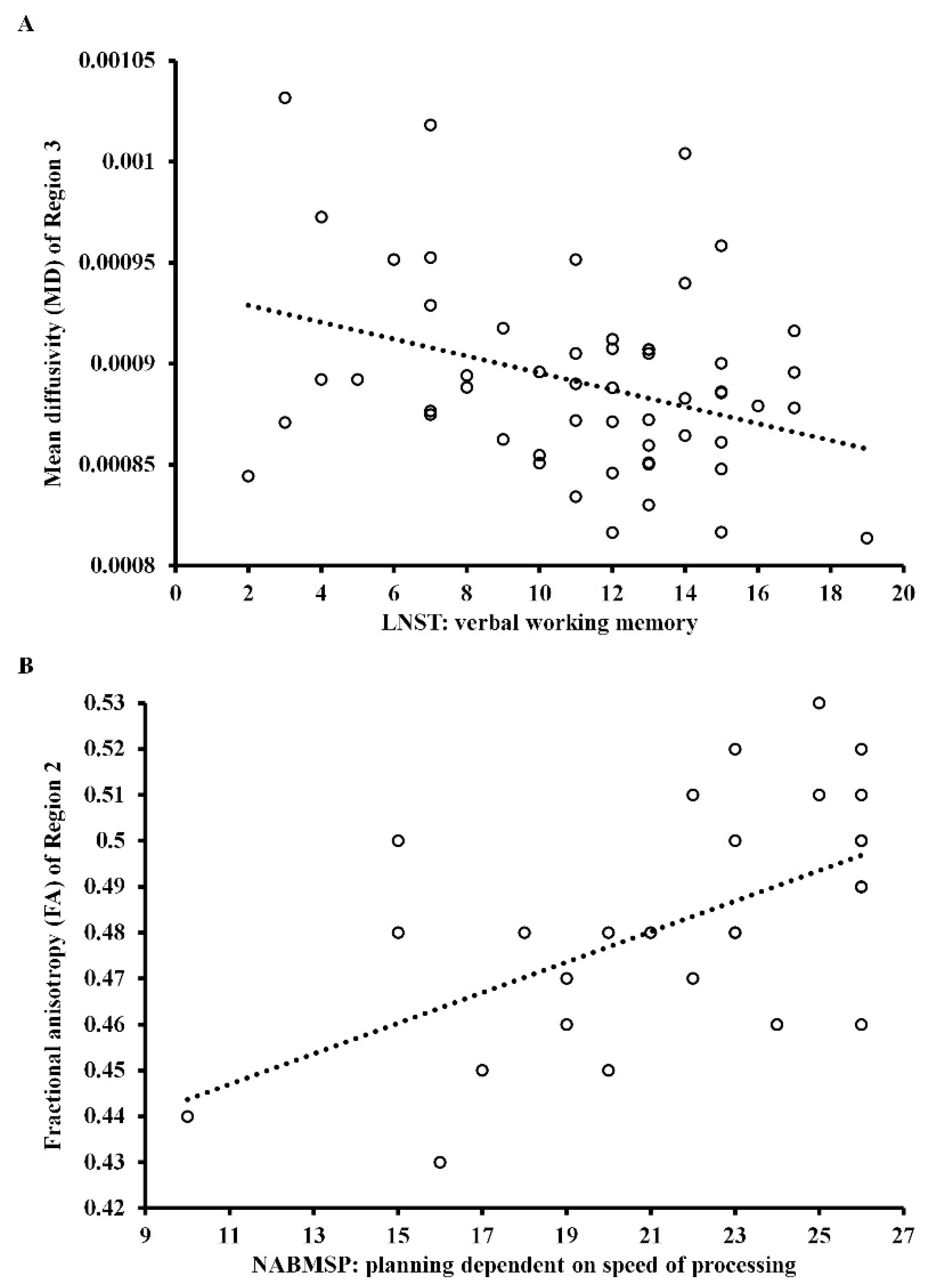
3.4. Relationship between DTI Measures and Cognitive Functions
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kraepelin, E. Dementia Praecox and Paraphrenia; Livingstone: Edinburgh, UK, 1919. [Google Scholar]
- Bleuler, E. Dementia Praecox or the Group of Schizophrenias; International Universities Press: New York, NY, USA, 1950. [Google Scholar]
- Bora, E.; Lin, A.; Wood, S.J.; Yung, A.R.; McGorry, P.D.; Pantelis, C. Cognitive deficits in youth with familial and clinical high risk to psychosis: A systematic review and meta-analysis. Acta Psychiatry Scand. 2014, 130, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Fusar-Poli, P.; Deste, G.; Smieskova, R.; Barlati, S.; Yung, A.R.; Howes, O.; Stieglitz, R.D.; Vita, A.; McGuire, P.; Borgwardt, S. Cognitive functioning in prodromal psychosis: A meta-analysis. Arch. Gen. Psychiatry 2012, 69, 562–571. [Google Scholar] [CrossRef] [PubMed]
- Mesholam-Gately, R.I.; Giuliano, A.J.; Goff, K.P.; Faraone, S.V.; Seidman, L.J. Neurocognition in first-episode schizophrenia: A meta-analytic review. Neuropsychology 2009, 23, 315–336. [Google Scholar] [CrossRef] [Green Version]
- Zhang, H.; Wang, Y.; Hu, Y.; Zhu, Y.; Zhang, T.; Wang, J.; Ma, K.; Shi, C.; Yu, X.; Li, C. Meta-analysis of cognitive function in Chinese first-episode schizophrenia: MATRICS Consensus Cognitive Battery (MCCB) profile of impairment. Gen. Psychiatry 2019, 32, e100043. [Google Scholar] [CrossRef] [Green Version]
- Dickinson, D.; Ramsey, M.E.; Gold, J.M. Overlooking the obvious: A meta-analytic comparison of digit symbol coding tasks and other cognitive measures in schizophrenia. Arch. Gen. Psychiatry 2007, 64, 532–542. [Google Scholar] [CrossRef] [PubMed]
- Fioravanti, M.; Bianchi, V.; Cinti, M.E. Cognitive deficits in schizophrenia: An updated metanalysis of the scientific evidence. BMC Psychiatry 2012, 12, e64. [Google Scholar] [CrossRef] [Green Version]
- Vyas, N.S.; Patel, N.H.; Puri, B.K. Neurobiology and phenotypic expression in early onset schizophrenia. Early Interv. Psychiatry 2011, 5, 3–14. [Google Scholar] [CrossRef] [PubMed]
- Bitanihirwe, B.K.; Mauney, S.A.; Woo, T.U. Weaving a net of neurobiological mechanisms in schizophrenia and unraveling the underlying pathophysiology. Biol. Psychiatry 2016, 80, 589–598. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lesh, T.A.; Niendam, T.A.; Minzenberg, M.J.; Carter, C.S. Cognitive control deficits in schizophrenia: Mechanisms and meaning. Neuropsychopharmacology 2011, 36, 316–338. [Google Scholar] [CrossRef] [Green Version]
- Romme, I.A.; de Reus, M.A.; Ophoff, R.A.; Kahn, R.S.; van den Heuvel, M.P. Connectome disconnectivity and cortical gene expression in patients with schizophrenia. Biol. Psychiatry 2017, 81, 495–502. [Google Scholar] [CrossRef] [Green Version]
- Friston, K.; Brown, H.R.; Siemerkus, J.; Stephan, K.E. The dysconnection hypothesis (2016). Schizophr. Res. 2016, 176, 83–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van der Knaap, L.J.; van der Ham, I.J. How does the corpus callosum mediate interhemispheric transfer? A review. Behav. Brain Res. 2011, 223, 211–221. [Google Scholar] [CrossRef]
- Clarke, B. Arthur Wigan and the Duality of the Mind. Psychol. Med. Monogr. Suppl. 1987, 11, 1–52. [Google Scholar] [CrossRef]
- Aboitiz, F.; Scheibel, A.B.; Fisher, R.S.; Zaidel, E. Fiber composition of the human corpus callosum. Brain Res. 1992, 598, 143–153. [Google Scholar] [CrossRef]
- Hofer, S.; Frahm, J. Topography of the human corpus callosum revisited-Comprehensive fiber tractography using diffusion tensor magnetic resonance imaging. Neuroimage 2006, 32, 989–994. [Google Scholar] [CrossRef] [PubMed]
- Gazzaniga, M.S. Cerebral specialization and interhemispheric communication: Does the corpus callosum enable the human condition? Brain 2000, 123, 1293–1326. [Google Scholar] [CrossRef] [Green Version]
- David, A.S. Schizophrenia and the corpus callosum: Developmental, structural and functional relationships. Behav. Brain Res. 1994, 64, 203–211. [Google Scholar] [CrossRef]
- Patel, S.; Mahon, K.; Wellington, R.; Zhang, J.; Chaplin, W.; Szeszko, P.R. A meta-analysis of diffusion tensor imaging studies of the corpus callosum in schizophrenia. Schizophr. Res. 2011, 129, 149–155. [Google Scholar] [CrossRef]
- Podwalski, P.; Szczygieł, K.; Tyburski, E.; Sagan, L.; Misiak, B.; Samochowiec, J. Magnetic resonance diffusion tensor imaging in psychiatry: A narrative review of its potential role in diagnosis. Pharmacol. Rep. 2021, 73, 43–56. [Google Scholar] [CrossRef]
- Williams, M.R.; Hampton, T.; Pearce, R.K.; Hirsch, S.R.; Ansorge, O.; Thom, M.; Maier, M. Astrocyte decrease in the subgenual cingulate and callosal genu in schizophrenia. Eur. Arch. Psychiatry Clin. Neurosci. 2013, 263, 41–52. [Google Scholar] [CrossRef]
- Schoonover, K.E.; Farmer, C.B.; Cash, A.E.; Roberts, R.C. Pathology of white matter integrity in three major white matter fasciculi: A post-mortem study of schizophrenia and treatment status. Br. J. Pharmacol. 2019, 176, 1143–1155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walterfang, M.; Wood, S.J.; Velakoulis, D.; Pantelis, C. Neuropathological, neurogenetic and neuroimaging evidence for white matter pathology in schizophrenia. Neurosci. Biobehav. Rev. 2006, 30, 918–948. [Google Scholar] [CrossRef] [PubMed]
- Zhuo, C.; Liu, M.; Wang, L.; Tian, H.; Tang, J. Diffusion tensor MR imaging evaluation of callosal abnormalities in schizophrenia: A meta-analysis. PLoS ONE 2016, 11, e0161406. [Google Scholar] [CrossRef] [PubMed]
- Kelly, S.; Jahanshad, N.; Zalesky, A.; Kochunov, P.; Agartz, I.; Alloza, C.; Andreassen, O.A.; Arango, C.; Banaj, N.; Bouix, S.; et al. Widespread white matter microstructural differences in schizophrenia across 4322 individuals: Results from the ENIGMA Schizophrenia DTI Working Group. Mol. Psychiatry 2018, 23, 1261–1269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Madigand, J.; Tréhout, M.; Delcroix, N.; Dollfus, S.; Leroux, E. Corpus callosum microstructural and macrostructural abnormalities in schizophrenia according to the stage of disease. Psychiatry Res. Neuroimaging 2019, 291, 63–70. [Google Scholar] [CrossRef]
- Keller, A.; Jeffries, N.O.; Blumenthal, J.; Clasen, L.S.; Liu, H.; Giedd, J.N.; Rapoport, J.L. Corpus callosum development in childhood-onset schizophrenia. Schizophr. Res. 2003, 62, 105–114. [Google Scholar] [CrossRef]
- Mitelman, S.A.; Nikiforova, Y.K.; Canfield, E.L.; Hazlett, E.A.; Brickman, A.M.; Shihabuddin, L.; Buchsbaum, M.S. A longitudinal study of the corpus callosum in chronic schizophrenia. Schizophr. Res. 2009, 114, 144–153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carletti, F.; Woolley, J.B.; Bhattacharyya, S.; Perez-Iglesias, R.; Fusar Poli, P.; Valmaggia, L.; Broome, M.R.; Bramon, E.; Johns, L.; Giampietro, V.; et al. Alterations in white matter evident before the onset of psychosis. Schizophr. Bull. 2012, 38, 1170–1179. [Google Scholar] [CrossRef]
- Balevich, E.C.; Haznedar, M.M.; Wang, E.; Newmark, R.E.; Bloom, R.; Schneiderman, J.S.; Aronowitz, J.; Tang, C.Y.; Chu, K.W.; Byne, W.; et al. Corpus callosum size and diffusion tensor anisotropy in adolescents and adults with schizophrenia. Psychiatry Res. 2015, 231, 244–251. [Google Scholar] [CrossRef] [Green Version]
- Chaim, T.M.; Schaufelberger, M.S.; Ferreira, L.K.; Duran, F.L.; Ayres, A.M.; Scazufca, M.; Menezes, P.R.; Amaro, E., Jr.; Leite, C.C.; Murray, R.M.; et al. Volume reduction of the corpus callosum and its relationship with deficits in interhemispheric transfer of information in recent-onset psychosis. Psychiatry Res. 2010, 184, 1–9. [Google Scholar] [CrossRef]
- Walterfang, M.; Yung, A.; Wood, A.G.; Reutens, D.C.; Phillips, L.; Wood, S.J.; Chen, J.; Velakoulis, D.; McGorry, P.D.; Pantelis, C. Corpus callosum shape alterations in individuals prior to the onset of psychosis. Schizophr. Res. 2008, 103, 1–10. [Google Scholar] [CrossRef]
- Walterfang, M.; Wood, A.G.; Reutens, D.C.; Wood, S.J.; Chen, J.; Velakoulis, D.; McGorry, P.D.; Pantelis, C. Morphology of the corpus callosum at different stages of schizophrenia: Cross-sectional study in first-episode and chronic illness. Br. J. Psychiatry 2008, 192, 429–434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kong, X.; Ouyang, X.; Tao, H.; Liu, H.; Li, L.; Zhao, J.; Xue, Z.; Wang, F.; Jiang, S.; Shan, B.; et al. Complementary diffusion tensor imaging study of the corpus callosum in patients with first-episode and chronic schizophrenia. J. Psychiatry Neurosci. 2011, 36, 120–125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Friedman, J.I.; Tang, C.; Carpenter, D.; Buchsbaum, M.; Schmeidler, J.; Flanagan, L.; Golembo, S.; Kanellopoulou, I.; Ng, J.; Hof, P.R.; et al. Diffusion tensor imaging findings in first-episode and chronic schizophrenia patients. Am. J. Psychiatry 2008, 165, 1024–1032. [Google Scholar] [CrossRef]
- Collinson, S.L.; Gan, S.C.; San Woon, P.; Kuswanto, C.; Sum, M.Y.; Yang, G.L.; Lui, J.M.; Sitoh, Y.Y.; Nowinski, W.L.; Sim, K. Corpus callosum morphology in first-episode and chronic schizophrenia: Combined magnetic resonance and diffusion tensor imaging study of Chinese Singaporean patients. Br. J. Psychiatry 2014, 204, 55–60. [Google Scholar] [CrossRef] [Green Version]
- Fett, A.K.; Viechtbauer, W.; Penn, D.L.; van Os, J.; Krabbendam, L. The relationship between neurocognition and social cog-nition with functional outcomes in schizophrenia: A meta-analysis. Neurosci. Biobehav. Rev. 2011, 35, 573–588. [Google Scholar] [CrossRef] [Green Version]
- Baddeley, A. Working memory: Theories, models, and controversies. Annu. Rev. Psychol. 2012, 63, 1–29. [Google Scholar] [CrossRef] [Green Version]
- Lezak, M.D.; Howieson, D.B.; Loring, D.W. Neuropsychological Assessment, 4th ed.; Oxford University Press: New York, NY, USA, 2004. [Google Scholar]
- Salthouse, T.A. What cognitive abilities are involved in trail-making performance? Intelligence 2011, 39, 222–232. [Google Scholar] [CrossRef] [Green Version]
- Salthouse, T.A. The processing-speed theory of adult age differences in cognition. Psychol. Rev. 1996, 103, 403–428. [Google Scholar] [CrossRef] [Green Version]
- Corigliano, V.; De Carolis, A.; Trovini, G.; Dehning, J.; Di Pietro, S.; Curto, M.; Donato, N.; De Pisa, E.; Girardi, P.; Comparelli, A. Neurocognition in schizophrenia: From prodrome to multi-episode illness. Psychiatry Res. 2014, 220, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Hirt, V.; Schubring, D.; Schalinski, I.; Rockstroh, B. Mismatch negativity and cognitive performance in the course of schizophrenia. Int. J. Psychophysiol. 2019, 145, 30–39. [Google Scholar] [CrossRef] [PubMed]
- Xiong, Y.B.; Bo, Q.J.; Wang, C.M.; Tian, Q.; Liu, Y.; Wang, C.Y. Differential of frequency and duration mismatch negativity and theta power deficits in first-episode and chronic schizophrenia. Front. Behav. Neurosci. 2019, 13, e37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Y.; Wang, G.; Jin, H.; Lyu, H.; Liu, Y.; Guo, W.; Shi, C.; Meyers, J.; Wang, J.; Zhao, J.; et al. Cognitive deficits in subjects at risk for psychosis, first-episode and chronic schizophrenia patients. Psychiatry Res. 2019, 274, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Jimenez, R.; Santos, J.L.; Dompablo, M.; Santabárbara, J.; Aparicio, A.I.; Olmos, R.; Jiménez-López, E.; Sánchez-Morla, E.; Lobo, A.; Palomo, T.; et al. MCCB cognitive profile in Spanish first episode schizophrenia patients. Schizophr. Res. 2019, 211, 88–92. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Liu, Y.; Wang, G.; Hei, G.; Wang, X.; Li, R.; Li, L.; Wu, R.; Zhao, J. Brain-derived neurotrophic factor is associated with cognitive impairments in first-episode and chronic schizophrenia. Psychiatry Res. 2019, 273, 528–536. [Google Scholar] [CrossRef]
- Wu, J.Q.; Tan, Y.L.; Xiu, M.H.; De Yang, F.; Soares, J.C.; Zhang, X.Y. Cognitive impairments in first-episode drug-naive and chronic medicated schizophrenia: MATRICS consensus cognitive battery in a Chinese Han population. Psychiatry Res. 2016, 238, 196–202. [Google Scholar] [CrossRef] [PubMed]
- Carolus, A.M.; Schubring, D.; Popov, T.G.; Popova, P.; Miller, G.A.; Rockstroh, B.S. Functional cognitive and cortical abnormalities in chronic and first-admission schizophrenia. Schizophr. Res. 2014, 157, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Rund, B.R. A review of longitudinal studies of cognitive functions in schizophrenia patients. Schizophr. Bull. 1998, 24, 425–435. [Google Scholar] [CrossRef]
- Harvey, P.D. Cognitive impairment in elderly patients with schizophrenia: Age related changes. Int. J. Geriatr. Psychiatry 2001, 16, 78–85. [Google Scholar] [CrossRef]
- Eberhard, J.; Riley, F.; Levander, S. Premorbid IQ and schizophrenia. Eur. Arch. Psychiatry Clin. Neurosci. 2003, 253, 84–88. [Google Scholar] [CrossRef]
- Seidman, L.J.; Lanca, M.; Kremen, W.S.; Faraone, S.V.; Tsuang, M.T. Organizational and visual memory deficits in schizophrenia and bipolar psychoses using the Rey-Osterrieth complex figure: Effects of duration of illness. J. Clin. Exp. Neuropsychol. 2003, 25, 949–964. [Google Scholar] [CrossRef]
- Ahn, J.I.; Yu, S.T.; Sung, G.; Choi, T.K.; Lee, K.S.; Bang, M.; Lee, S.H. Intra-individual variability in neurocognitive function in schizophrenia: Relationships with the corpus callosum. Psychiatry Res. Neuroimaging 2019, 283, 1–6. [Google Scholar] [CrossRef]
- Ohoshi, Y.; Takahashi, S.; Yamada, S.; Ishida, T.; Tsuda, K.; Tsuji, T.; Terada, M.; Shinosaki, K.; Ukai, S. Microstructural abnormalities in callosal fibers and their relationship with cognitive function in schizophrenia: A tract-specific analysis study. Brain Behav. 2019, 9, e01357. [Google Scholar] [CrossRef]
- Hidese, S.; Ota, M.; Matsuo, J.; Ishida, I.; Hiraishi, M.; Teraishi, T.; Hattori, K.; Kunugi, H. Association between the scores of the Japanese version of the Brief Assessment of Cognition in Schizophrenia and whole-brain structure in patients with chronic schizophrenia: A voxel-based morphometry and diffusion tensor imaging study. Psychiatry Clin. Neurosci. 2017, 71, 826–835. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karbasforoushan, H.; Duffy, B.; Blackford, J.U.; Woodward, N.D. Processing speed impairment in schizophrenia is mediated by white matter integrity. Psychol. Med. 2015, 45, 109–120. [Google Scholar] [CrossRef] [Green Version]
- Gómez-Gastiasoro, A.; Zubiaurre-Elorza, L.; Peña, J.; Ibarretxe-Bilbao, N.; Rilo, O.; Schretlen, D.J.; Ojeda, N. Altered frontal white matter asymmetry and its implications for cognition in schizophrenia: A tractography study. Neuroimage Clin. 2019, 22, e101781. [Google Scholar] [CrossRef] [PubMed]
- Knöchel, C.; Schmied, C.; Linden, D.E.; Stäblein, M.; Prvulovic, D.; de Carvalho, L.D.; Harrison, O.; Junior, P.O.; Carvalho, A.F.; Reif, A.; et al. White matter abnormalities in the fornix are linked to cognitive performance in SZ but not in BD disorder: An exploratory analysis with DTI deterministic tractography. J. Affect. Disord. 2016, 201, 64–78. [Google Scholar] [CrossRef]
- Roalf, D.R.; Ruparel, K.; Verma, R.; Elliott, M.A.; Gur, R.E.; Gur, R.C. White matter organization and neurocognitive performance variability in schizophrenia. Schizophr. Res. 2013, 143, 172–178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roalf, D.R.; Gur, R.E.; Verma, R.; Parker, W.A.; Quarmley, M.; Ruparel, K.; Gur, R.C. White matter microstructure in schizophrenia: Associations to neurocognition and clinical symptomatology. Schizophr. Res. 2015, 161, 42–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peng, X.; Zhang, R.; Yan, W.; Zhou, M.; Lu, S.; Xie, S. Reduced white matter integrity associated with cognitive deficits in patients with drug-naive first-episode schizophrenia revealed by diffusion tensor imaging. Am. J. Transl. Res. 2020, 12, 4410–4421. [Google Scholar]
- Lyall, A.E.; Pasternak, O.; Robinson, D.G.; Newell, D.; Trampush, J.W.; Gallego, J.A.; Fava, M.; Malhotra, A.K.; Karlsgodt, K.H.; Kubicki, M.; et al. Greater extracellular free-water in first-episode psychosis predicts better neurocognitive functioning. Mol. Psychiatry 2018, 23, 701–707. [Google Scholar] [CrossRef]
- Long, Y.; Ouyang, X.; Liu, Z.; Chen, X.; Hu, X.; Lee, E.; Chen, E.Y.; Pu, W.; Shan, B.; Rohrbaugh, R.M. Associations among suicidal ideation, white matter integrity and cognitive deficit in first-episode schizophrenia. Front. Psychiatry 2018, 9, e391. [Google Scholar] [CrossRef]
- Rigucci, S.; Rossi-Espagnet, C.; Ferracuti, S.; De Carolis, A.; Corigliano, V.; Carducci, F.; Mancinelli, I.; Cicone, R.; Tatarelli, R.; Bozzao, A.; et al. Anatomical substrates of cognitive and clinical dimensions in first episode schizophrenia. Acta Psychiatry Scand. 2013, 128, 261–270. [Google Scholar] [CrossRef] [Green Version]
- Ruef, A.; Curtis, L.; Moy, G.; Bessero, S.; Bâ, M.B.; Lazeyras, F.; Lövblad, K.O.; Haller, S.; Malafosse, A.; Giannakopoulos, P.; et al. Magnetic resonance imaging correlates of first-episode psychosis in young adult male patients: Combined analysis of grey and white matter. J. Psychiatry Neurosci. 2012, 37, 305–312. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Y.; Liu, J.; Driesen, N.; Womer, F.; Chen, K.; Wang, Y.; Jiang, X.; Zhou, Q.; Bai, C.; Wang, D.; et al. White matter integrity in genetic high-risk individuals and first-episode schizophrenia patients: Similarities and disassociations. Biomed. Res. Int. 2017, 2017, e3107845. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.; Gao, S.; Zhang, X. Cognitive deficits and white matter abnormalities in never-treated first-episode schizophrenia. Transl. Psychiatry 2020, 10, 1–8. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. The ICD-10 Classification of Mental and Behavioural Disorders: Clinical Descriptions and Diagnostic Guidelines; World Health Organization: Geneva, Switzerland, 1992. [Google Scholar]
- Sheehan, D.V.; Lecrubier, Y.; Sheehan, K.H.; Amorim, P.; Janavs, J.; Weiller, E.; Hergueta, T.; Baker, R.; Dunbar, G.C. The Mini-International Neuropsychiatric Interview (MINI): The development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J. Clin. Psychiatry 1998, 59, 22–33. [Google Scholar]
- Jędrasik-Styła, M.; Ciołkiewicz, A.; Styła, R.; Linke, M.; Parnowska, D.; Gruszka, A.; Denisiuk, M.; Jarema, M.; Green, M.F.; Wichniak, A. The Polish academic version of the MATRICS Consensus Cognitive Battery (MCCB): Evaluation of psychometric properties. Psychiatr. Q. 2015, 8, 435–447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nuechterlein, K.H.; Green, M.F.; Kern, R.S.; Baade, L.E.; Barch, D.M.; Cohen, J.D.; Essock, S.; Fenton, W.S.; Frese, F.J., 3rd; Gold, J.M.; et al. The MATRICS Consensus Cognitive Battery, part 1: Test selection, reliability, and validity. Am. J. Psychiatry 2008, 165, 203–213. [Google Scholar] [CrossRef] [Green Version]
- Cornoldi, C.; Mammarella, I.C. A comparison of backward and forward spatial spans. Q. J. Exp. Psychol. 2008, 61, 674–682. [Google Scholar] [CrossRef] [PubMed]
- Lace, J.W.; Grant, A.F.; Ruppert, P.; Kaufman, D.A.; Teague, C.L.; Lowell, K.; Gfeller, J.D. Detecting noncredible performance with the neuropsychological assessment battery, screening module: A simulation study. Clin. Neuropsychol. 2021, 35, 572–596. [Google Scholar] [CrossRef] [PubMed]
- Kay, S.R.; Fiszbein, A.; Opler, L.A. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr. Bull. 1987, 13, 261–276. [Google Scholar] [CrossRef] [PubMed]
- Shafer, A.; Dazzi, F. Meta-analysis of the positive and Negative Syndrome Scale (PANSS) factor structure. J. Psychiatry Res. 2019, 115, 113–120. [Google Scholar] [CrossRef] [PubMed]
- Hall, R.C. Global assessment of functioning: A modified scale. Psychosomatics 1995, 36, 267–275. [Google Scholar] [CrossRef]
- Leemans, A.; Jeurissen, B.; Sijbers, J.; Jones, D.K. ExploreDTI: A graphical toolbox for processing, analyzing, and visualizing diffusion MR data. Proc. Intl. Soc. Mag. Reason. Med. 2009, 17, e3537. [Google Scholar]
- Podwalski, P.; Tyburski, E.; Szczygieł, K.; Waszczuk, K.; Rek-Owodziń, K.; Mak, M.; Plichta, P.; Bielecki, M.; Rudkowski, K.; Kucharska-Mazur, J.; et al. White Matter Integrity of the Corpus Callosum and Psychopathological Dimensions in Deficit and Non-Deficit Schizophrenia Patients. J. Clin. Med. 2021, 10, e2225. [Google Scholar] [CrossRef]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef]
- Thiese, M.S.; Ronna, B.; Ott, U. p value interpretations and considerations. J. Thorac. Dis. 2016, 8, e928. [Google Scholar] [CrossRef] [Green Version]
- Garver, D.L.; Holcomb, J.A.; Christensen, J.D. Compromised myelin integrity during psychosis with repair during remission in drug-responding schizophrenia. Int. J. Neuropsychopharmacol. 2008, 11, 49–61. [Google Scholar] [CrossRef] [Green Version]
- Winterer, G.; Konrad, A.; Vucurevic, G.; Musso, F.; Stoeter, P.; Dahmen, N. Association of 5′ end neuregulin-1 (NRG1) gene variation with subcortical medial frontal microstructure in humans. Neuroimage 2008, 40, 712–718. [Google Scholar] [CrossRef]
- Fitzsimmons, J.; Kubicki, M.; Shenton, M.E. Review of functional and anatomical brain connectivity findings in schizophrenia. Curr. Opin. Psychiatry 2013, 26, 172–187. [Google Scholar] [CrossRef] [PubMed]
- Kochunov, P.; Coyle, T.R.; Rowland, L.M.; Jahanshad, N.; Thompson, P.M.; Kelly, S.; Du, X.; Sampath, H.; Bruce, H.; Chiappelli, J.; et al. Association of white matter with core cognitive deficits in patients with schizophrenia. JAMA Psychiatry 2017, 74, 958–966. [Google Scholar] [CrossRef]
- Uddin, L.Q.; Yeo, B.T.; Spreng, R.N. Towards a universal taxonomy of macro-scale functional human brain networks. Brain Topogr. 2019, 32, 926–942. [Google Scholar] [CrossRef]
- Marvel, C.L.; Morgan, O.P.; Kronemer, S.I. How the motor system integrates with working memory. Neurosci. Biobehav. Rev. 2019, 102, 184–194. [Google Scholar] [CrossRef] [PubMed]
- Voineskos, A.N.; Rajji, T.K.; Lobaugh, N.J.; Miranda, D.; Shenton, M.E.; Kennedy, J.L.; Pollock, B.G.; Mulsant, B.H. Age-related decline in white matter tract integrity and cognitive performance: A DTI tractography and structural equation modeling study. Neurobiol. Aging 2012, 33, 21–34. [Google Scholar] [CrossRef] [Green Version]
- Hinkley, L.B.; Marco, E.J.; Findlay, A.M.; Honma, S.; Jeremy, R.J.; Strominger, Z.; Bukshpun, P.; Wakahiro, M.; Brown, W.S.; Paul, L.K.; et al. The role of corpus callosum development in functional connectivity and cognitive processing. PLoS ONE 2012, 7, e39804. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fatemi, S.H.; Folsom, T.D. The neurodevelopmental hypothesis of schizophrenia, revisited. Schizophr. Bull. 2009, 35, 528–548. [Google Scholar] [CrossRef] [PubMed]
- Weinberger, D.R. Implications of normal brain development for the pathogenesis of schizophrenia. Arch. Gen. Psychiatry 1987, 44, 660–669. [Google Scholar] [CrossRef]
- Andreasen, N.C. The lifetime trajectory of schizophrenia and the concept of neurodevelopment. Dialogues Clin. Neurosci. 2010, 12, 409–415. [Google Scholar] [CrossRef]
- Dell’Acqua, F.; Catani, M. Structural human brain networks: Hot topics in diffusion tractography. Curr. Opin. Neurol. 2012, 25, 375–383. [Google Scholar] [CrossRef] [Green Version]
- Ackerman, P.L.; Beier, M.E.; Boyle, M.O. Working memory and intelligence: The same or different constructs? Psychol. Bull. 2005, 131, 30–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ardila, A. Is intelligence equivalent to executive functions. Psicothema 2018, 30, 159–164. [Google Scholar] [CrossRef]
- McCabe, D.P.; Roediger, H.L., III; McDaniel, M.A.; Balota, D.A.; Hambrick, D.Z. The relationship between working memory capacity and executive functioning: Evidence for a common executive attention construct. Neuropsychology 2010, 24, 222–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaytor, N.; Schmitter-Edgecombe, M. The ecological validity of neuropsychological tests: A review of the literature on everyday cognitive skills. Neuropsychol. Rev. 2003, 13, 181–197. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients with First-Episode Schizophrenia (FES) (n = 18) | Patients with Chronic Schizophrenia (CS) (n = 55) | HealthyControls (HC) (n = 30) | F/χ2/t | |
|---|---|---|---|---|
| Age: M (SD) | 28.39 (6.98) | 39.09 (6.92) | 37.30 (8.24) | 14.58 *** a |
| Years of education: M (SD) | 13.28 (3.16) | 13.24 (2.61) | 14.53 (2.60) | 2.40 a |
| Sex: female/male | 13/5 | 26/29 | 16/14 | 3.39 b |
| Antipsychotic medications: | ||||
| Atypical: n (%) | 14 (77.78) | 37 (67.27) | - | 2.55 b |
| Atypical and typical: n (%) | 2 (11.12) | 15 (27.27) | - | |
| Typical: n (%) | 1 (5.55) | 2 (3.64) | - | |
| No medications: n (%) | 1 (5.55) | 1 (1.82) | - | |
| Chlorpromazine equivalent (mg): M (SD) | 470.17 (331.53) | 644.96 (301.72) | - | −2.08 c |
| Duration of illness: M (SD) | 0.44 (0.32) | 14.73 (5.47) | - | −19.27 *** c |
| Exacerbation: M (SD) | 1.11 (0.32) | 6.11 (3.89) | - | −9.43 *** c |
| Global functioning in GAF: M (SD) | 60.89 (14.73) | 58.51 (13.80) | - | 0.63 c |
| Psychopathological symptoms in PANSS: | ||||
| Positive symptoms: M (SD) | 11.61 (3.73) | 7.85 (3.83) | - | 3.64 ** c |
| Negative symptoms: M (SD) | 16.89 (5.96) | 16.42 (6.30) | - | 0.28 c |
| Disorganization: M (SD) | 13.78 (4.43) | 11.64 (3.74) | - | 2.01 c |
| Affect: M (SD) | 10.67 (4.26) | 9.36 (3.63) | - | 1.27 c |
| Resistance: M (SD) | 5.72 (2.16) | 4.78 (2.23) | - | 1.57 c |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tyburski, E.; Podwalski, P.; Waszczuk, K.; Rek-Owodziń, K.; Mak, M.; Plichta, P.; Bielecki, M.; Rudkowski, K.; Szelepajło, M.; Kucharska-Mazur, J.; et al. Relationship of Corpus Callosum Integrity with Working Memory, Planning, and Speed of Processing in Patients with First-Episode and Chronic Schizophrenia. J. Clin. Med. 2021, 10, 3158. https://doi.org/10.3390/jcm10143158
Tyburski E, Podwalski P, Waszczuk K, Rek-Owodziń K, Mak M, Plichta P, Bielecki M, Rudkowski K, Szelepajło M, Kucharska-Mazur J, et al. Relationship of Corpus Callosum Integrity with Working Memory, Planning, and Speed of Processing in Patients with First-Episode and Chronic Schizophrenia. Journal of Clinical Medicine. 2021; 10(14):3158. https://doi.org/10.3390/jcm10143158
Chicago/Turabian StyleTyburski, Ernest, Piotr Podwalski, Katarzyna Waszczuk, Katarzyna Rek-Owodziń, Monika Mak, Piotr Plichta, Maksymilian Bielecki, Krzysztof Rudkowski, Michał Szelepajło, Jolanta Kucharska-Mazur, and et al. 2021. "Relationship of Corpus Callosum Integrity with Working Memory, Planning, and Speed of Processing in Patients with First-Episode and Chronic Schizophrenia" Journal of Clinical Medicine 10, no. 14: 3158. https://doi.org/10.3390/jcm10143158
APA StyleTyburski, E., Podwalski, P., Waszczuk, K., Rek-Owodziń, K., Mak, M., Plichta, P., Bielecki, M., Rudkowski, K., Szelepajło, M., Kucharska-Mazur, J., Andrusewicz, W., Misiak, B., Kerestey, M., Bober, A., Wietrzyński, K., Michalczyk, A., Więdłocha, M., Marcinowicz, P., Samochowiec, J., & Sagan, L. (2021). Relationship of Corpus Callosum Integrity with Working Memory, Planning, and Speed of Processing in Patients with First-Episode and Chronic Schizophrenia. Journal of Clinical Medicine, 10(14), 3158. https://doi.org/10.3390/jcm10143158