
Influence of Chronic Ocular Hypertension on Emmetropia: Refractive, Structural and Functional Study in Two Rat Models

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Animals
2.2. Intraocular Pressure
2.3. Optical Coherence Tomography
2.4. Electroretinography
2.5. Statistical Analysis
3. Results
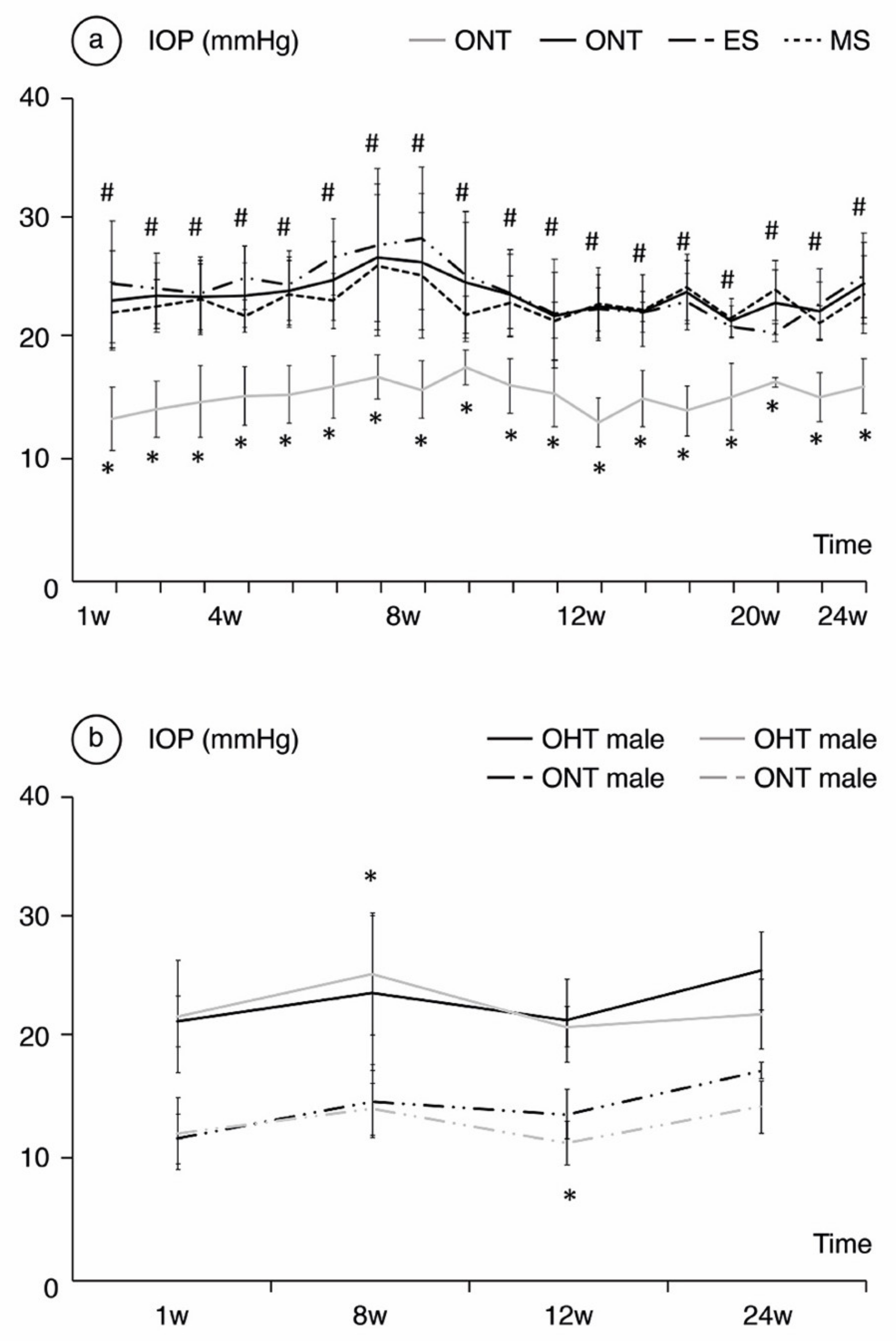
3.1. IOP Analysis
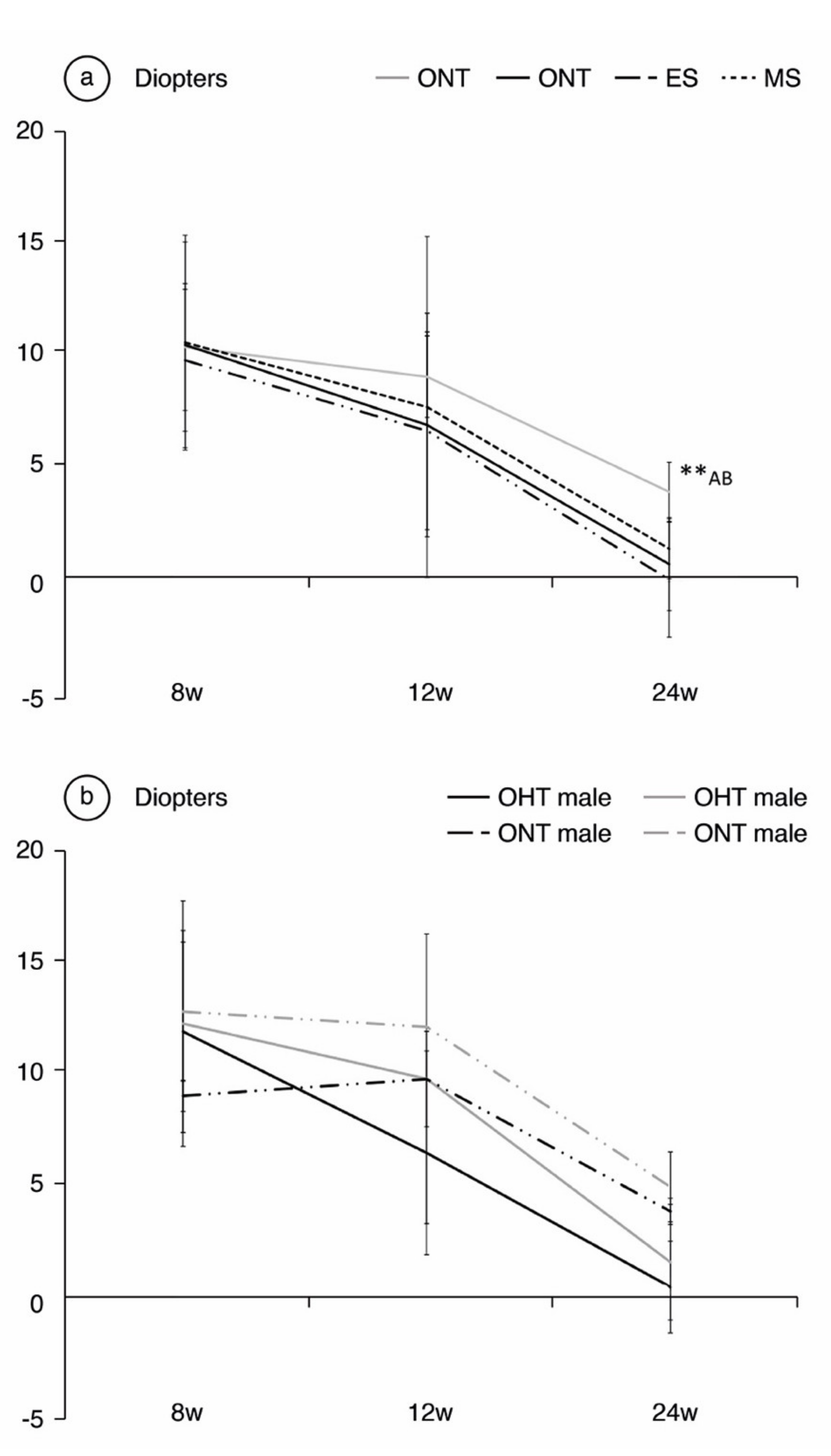
3.2. Refraction
3.3. Analysis of the Correlation between Refraction, Ocular Hypertension, and OCT Parameters
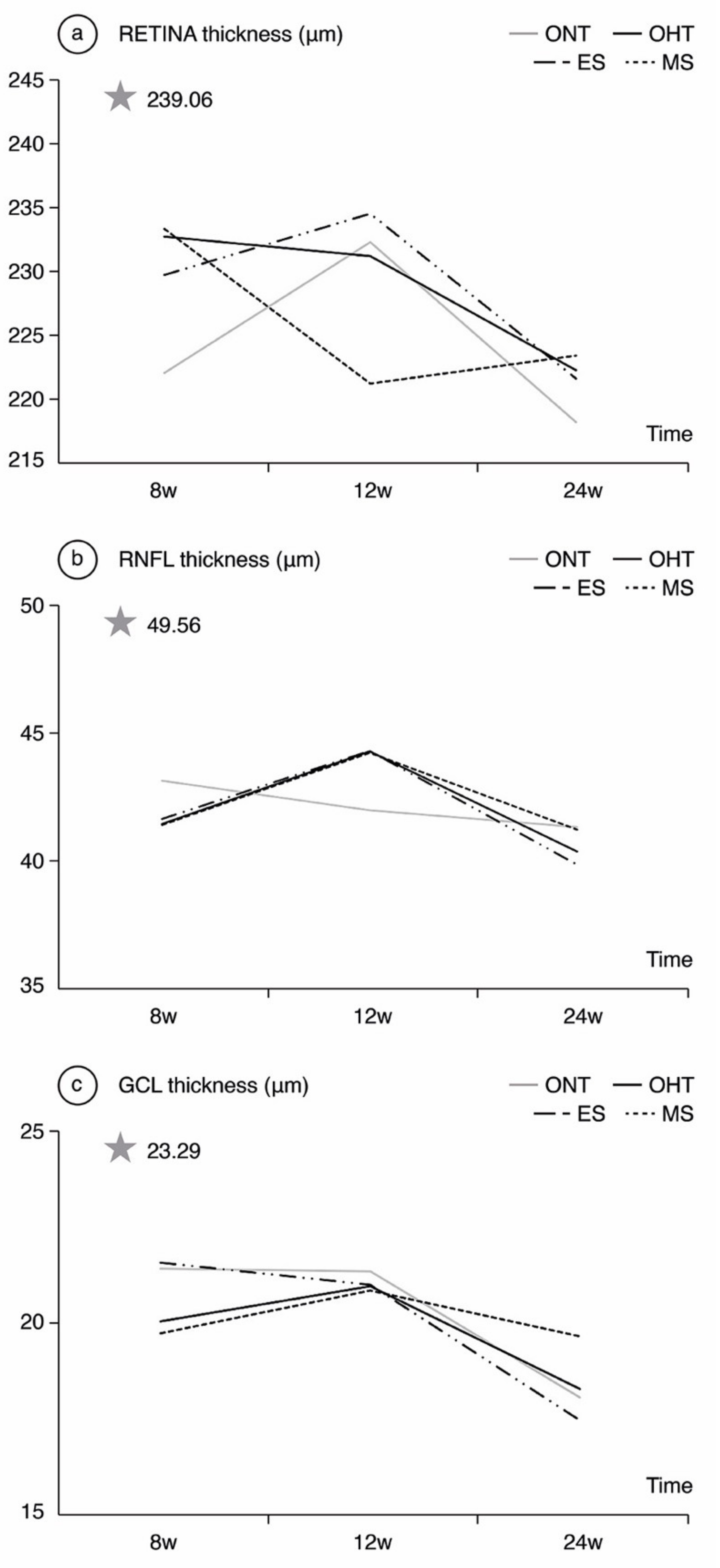
3.4. OCT Analysis
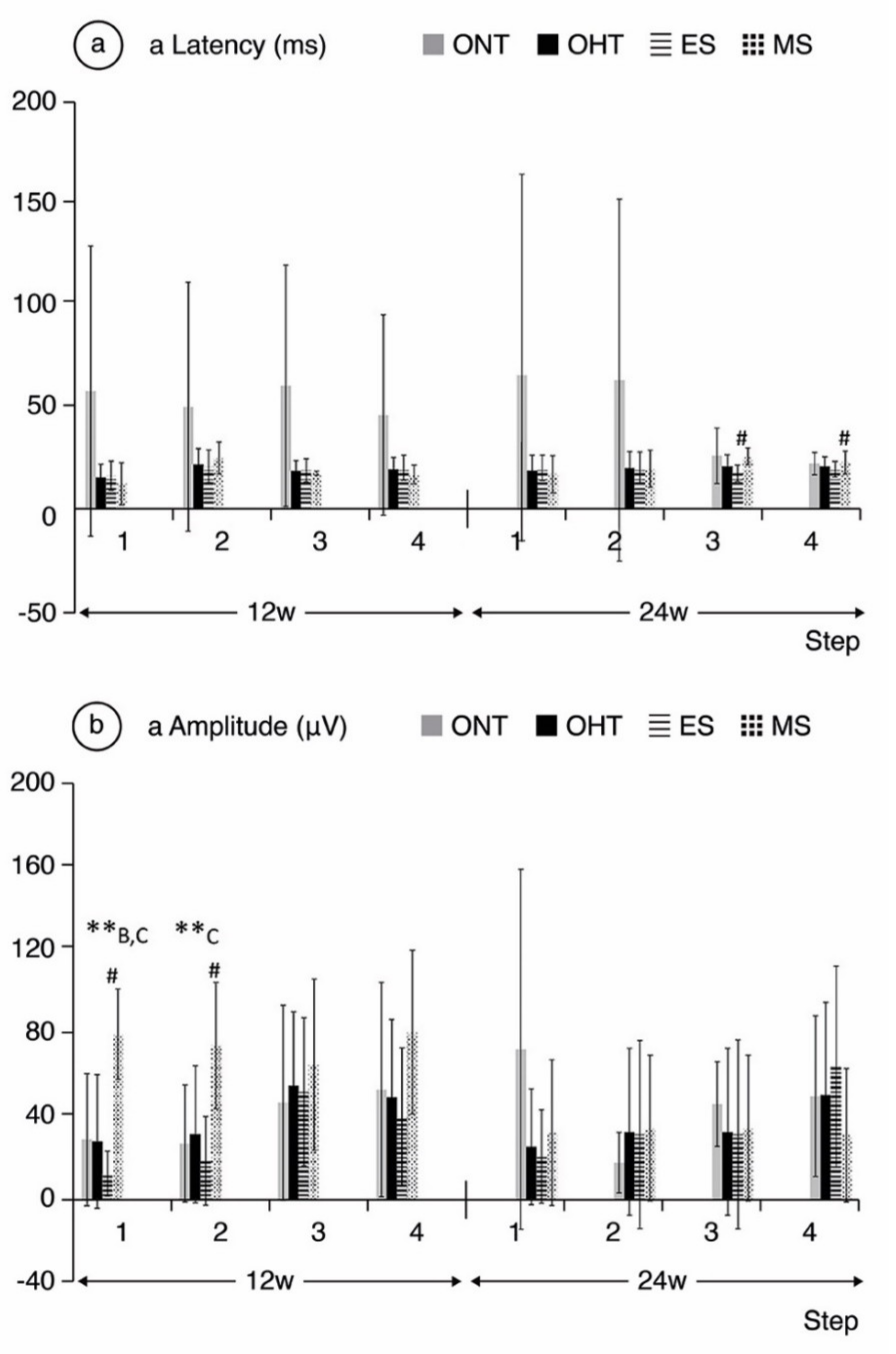
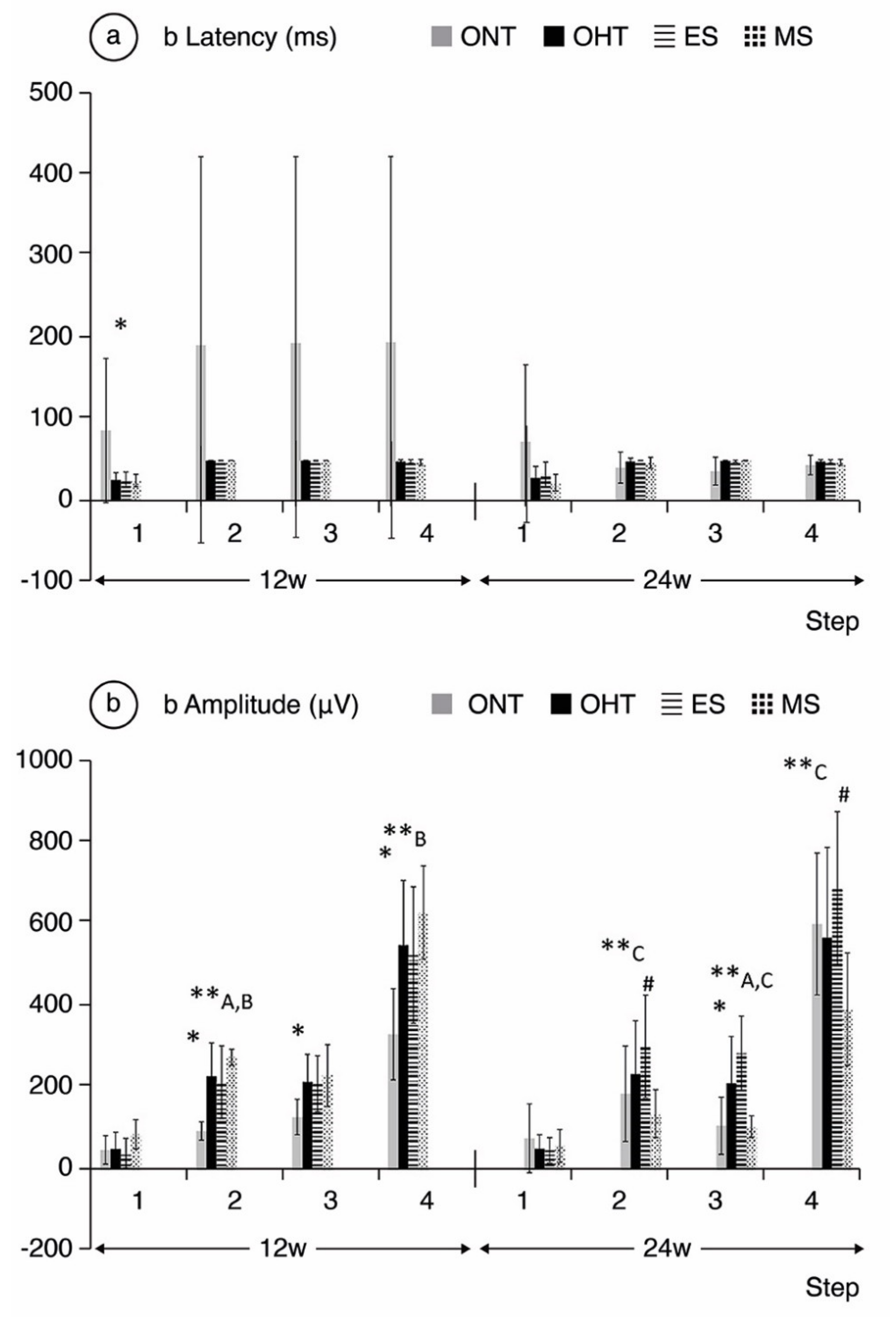
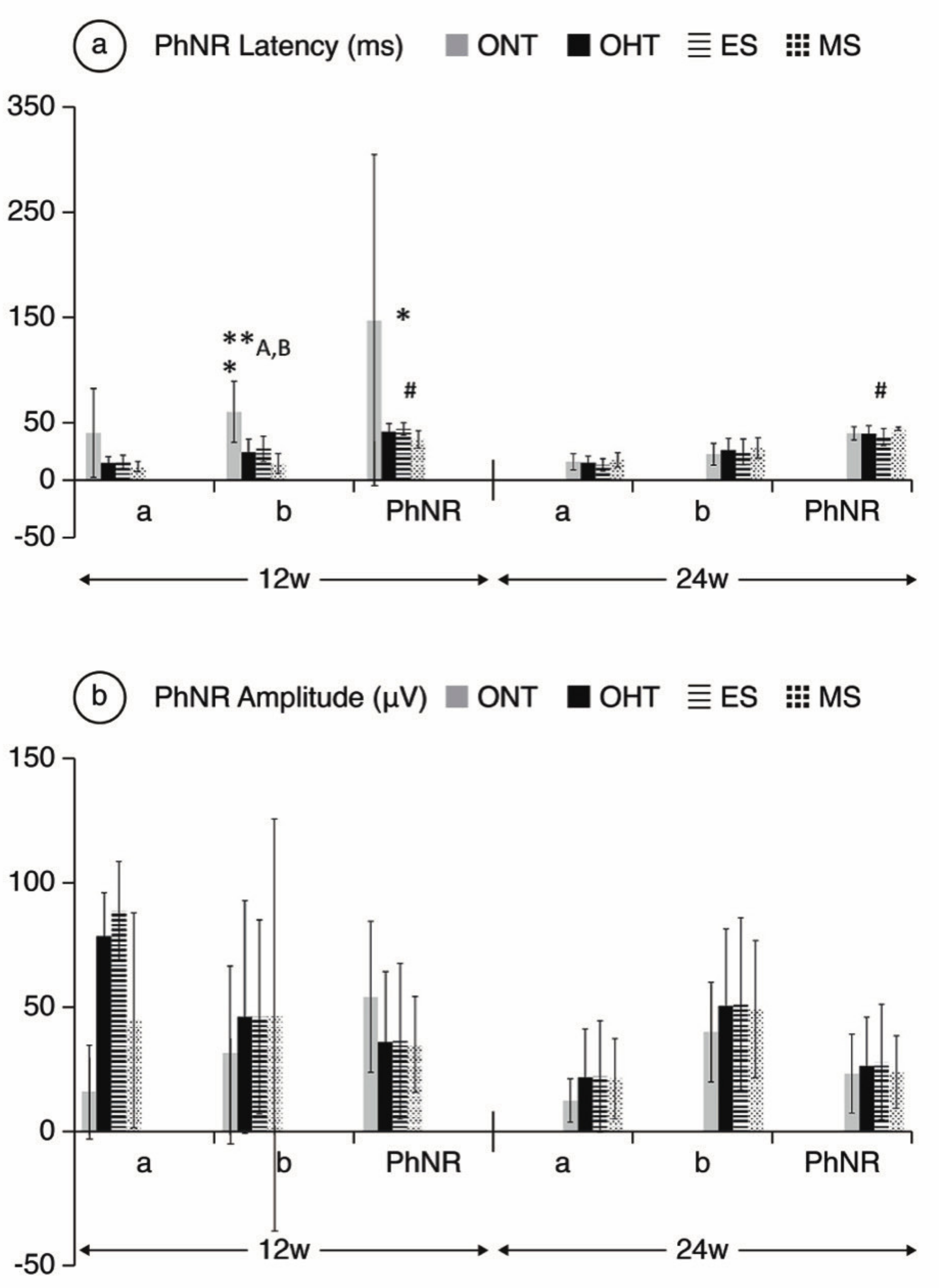
3.5. ERG Analysis
4. Discussion
4.1. Refractive Analysis
4.2. Structural Analysis
4.3. Functional Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Agis Investigators. The Advanced Glaucoma Intervention Study (AGIS): 7. The relationship between control of intraocular pressure and visual field deterioration.The AGIS Investigators. Am. J. Ophthalmol. 2000, 130, 429–440. [Google Scholar] [CrossRef]
- Shim, S.H.; Sung, K.R.; Kim, J.M.; Kim, H.T.; Jeong, J.; Kim, C.Y.; Lee, M.Y.; Park, K.H. Korean Ophthalmological Society the Prevalence of Open-Angle Glaucoma by Age in Myopia: The Korea National Health and Nutrition Examination Survey. Curr. Eye Res. 2017, 42, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Wong, T.Y.; Klein, B.E.K.; Klein, R.; Knudtson, M.; Lee, K.E. Refractive errors, intraocular pressure, and glaucoma in a white population. Ophthalmology 2003, 110, 211–217. [Google Scholar] [CrossRef]
- Xu, L.; Wang, Y.; Wang, S.; Wang, Y.; Jonas, J.B. High myopia and glaucoma susceptibility the Beijing Eye Study. Ophthalmology 2007, 114, 216–220. [Google Scholar] [CrossRef] [PubMed]
- Ikuno, Y. Overview of the Complications of High Myopia. Retina 2017, 37, 2347–2351. [Google Scholar] [CrossRef]
- Saw, S.M.; Gazzard, G.; Shin-Yen, E.C.; Chua, W.H. Myopia and associated pathological complications. Ophthalmic Physiol. Opt. 2005, 25, 381–391. [Google Scholar] [CrossRef]
- Holden, B.A.; Fricke, T.R.; Wilson, D.A.; Jong, M.; Naidoo, K.S.; Sankaridurg, P.; Wong, T.Y.; Naduvilath, T.J.; Resnikoff, S. Global Prevalence of Myopia and High Myopia and Temporal Trends from 2000 through 2050. Ophthalmology 2016, 123, 1036–1042. [Google Scholar] [CrossRef] [Green Version]
- Kim, T.-W.; Kim, M.; Weinreb, R.N.; Woo, S.J.; Park, K.H.; Hwang, J.-M. Optic Disc Change with Incipient Myopia of Childhood. Ophthalmology 2012, 119, 21.e3–26.e3. [Google Scholar] [CrossRef] [PubMed]
- Ng, D.S.C.; Cheung, C.Y.L.; Luk, F.O.; Mohamed, S.; Brelen, M.E.; Yam, J.C.S.; Tsang, C.W.; Lai, T.Y.Y. Advances of optical coherence tomography in myopia and pathologic myopia. Eye 2016, 30, 901–916. [Google Scholar] [CrossRef] [Green Version]
- Leung, C.K.S.; Mohamed, S.; Leung, K.S.; Cheung, C.Y.L.; Chan, S.L.W.; Cheng, D.K.Y.; Lee, A.K.C.; Leung, G.Y.O.; Rao, S.K.; Lam, D.S.C. Retinal nerve fiber layer measurements in myopia: An optical coherence tomography study. Investig. Ophthalmol. Vis. Sci. 2006, 47, 5171–5176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmid, K.L.; Hills, T.; Abbott, M.; Humphries, M.; Pyne, K.; Wildsoet, C.F. Relationship between intraocular pressure and eye growth in chick. Ophthalmic Physiol. Opt. 2003, 23, 25–33. [Google Scholar] [CrossRef] [PubMed]
- Read, S.A.; Collins, M.J.; Annis-Brown, T.; Hayward, N.M.; Lillyman, K.; Sherwin, D.; Stockall, P. The short-term influence of elevated intraocular pressure on axial length. Ophthalmic Physiol. Opt. 2011, 31, 398–403. [Google Scholar] [CrossRef] [PubMed]
- Tokoro, T.; Funata, M.; Akazawa, Y. Influence of intraocular pressure on axial elongation. J. Ocul. Pharmacol. 1990, 6, 285–291. [Google Scholar] [CrossRef] [PubMed]
- McBrien, N.A.; Jobling, A.I.; Gentle, A. Biomechanics of the Sclera in Myopia: Extracellular and Cellular Factors. Optom. Vis. Sci. 2009, 86, E23–E30. [Google Scholar] [CrossRef]
- McMonnies, C.W. An examination of the baropathic nature of axial myopia. Clin. Exp. Optom. 2014, 97, 116–124. [Google Scholar] [CrossRef] [PubMed]
- El-Nimri, N.W.; Wildsoet, C.F. Effects of topical latanoprost on intraocular pressure and myopia progression in young guinea pigs. Invest. Ophthalmol. Vis. Sci. 2018, 59, 2644–2651. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmid, K.L.; Abbott, M.; Humphries, M.; Pyne, K.; Wildsoet, C.F. Timolol lowers intraocular pressure but does not inhibit the development of experimental myopia in chick. Exp. Eye Res. 2000, 70, 659–666. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Wen, D.; Wang, Q.; McAlinden, C.; Flitcroft, I.; Chen, H.; Saw, S.M.; Chen, H.; Bao, F.; Zhao, Y.; et al. Efficacy comparison of 16 interventions for myopia control in children: A network meta-analysis. Ophthalmology 2016, 123, 697–708. [Google Scholar] [CrossRef] [Green Version]
- Patel, N.B.; Garcia, B.; Harwerth, R.S. Influence of anterior segment power on the scan path and RNFL thickness using SD-OCT. Investig. Ophthalmol. Vis. Sci. 2012, 53, 5788–5798. [Google Scholar] [CrossRef] [PubMed]
- Sachidanandam, R.; Ravi, P.; Sen, P. Effect of axial length on full-field and multifocal electroretinograms. Clin. Exp. Optom. 2017, 100, 668–675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biswas, S.; Lin, C.; Leung, C.K.S. Evaluation of a myopic normative database for analysis of retinal nerve fiber layer thickness. JAMA Ophthalmol. 2016, 134, 1032–1039. [Google Scholar] [CrossRef] [Green Version]
- Biswas, S.; Jhanji, V.; Leung, C.K.S. Prevalence of glaucoma in myopic corneal refractive surgery candidates in Hong Kong China. J. Refract. Surg. 2016, 32, 298–304. [Google Scholar] [CrossRef] [PubMed]
- Shoji, T.; Nagaoka, Y.; Sato, H.; Chihara, E. Impact of high myopia on the performance of SD-OCT parameters to detect glaucoma. Graefe’s Arch. Clin. Exp. Ophthalmol. 2012, 250, 1843–1849. [Google Scholar] [CrossRef]
- Neufeld, A.H.; Gachie, E.N. The inherent, age-dependent loss of retinal ganglion cells is related to the lifespan of the species. Neurobiol. Aging 2003, 24, 167–172. [Google Scholar] [CrossRef]
- Harman, A.M.; MacDonald, A.; Meyer, P.; Ahmat, A. Numbers of neurons in the retinal ganglion cell layer of the rat do not change throughout life. Gerontology 2003, 49, 350–355. [Google Scholar] [CrossRef]
- Levkovitch-Verbin, H.; Vander, S.; Makarovsky, D.; Lavinsky, F. Increase in retinal ganglion cells’ susceptibility to elevated intraocular pressure and impairment of their endogenous neuroprotective mechanism by age. Mol. Vis. 2013, 19, 2011–2022. [Google Scholar] [PubMed]
- Rodrigo, M.J.; Martinez-Rincon, T.; Subias, M.; Mendez-Martinez, S.; Luna, C.; Pablo, L.E.; Polo, V.; Garcia-Martin, E. Effect of age and sex on neurodevelopment and neurodegeneration in the healthy eye: Longitudinal functional and structural study in the Long–Evans rat. Exp. Eye Res. 2020, 200, 108208. [Google Scholar] [CrossRef] [PubMed]
- Cuenca, N.; Fernández-Sánchez, L.; Sauvé, Y.; Segura, F.J.; Martínez-Navarrete, G.; Tamarit, J.M.; Fuentes-Broto, L.; Sanchez-Cano, A.; Pinilla, I. Correlation between SD-OCT, immunocytochemistry and functional findings in an animal model of retinal degeneration. Front. Neuroanat. 2014, 8, 1–20. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Martin, E.; Pablo, L.E.; Bambo, M.P.; Alarcia, R.; Polo, V.; Larrosa, J.M.; Vilades, E.; Cameo, B.; Orduna, E.; Ramirez, T.; et al. Comparison of peripapillary choroidal thickness between healthy subjects and patients with Parkinson’s disease. PLoS ONE 2017, 12, e0177163. [Google Scholar] [CrossRef]
- Garcia-Martin, E.; Pueyo, V.; Martin, J.; Almarcegui, C.; Ara, J.R.; Dolz, I.; Honrubia, F.M.; Fernandez, F.J. Progressive changes in the retinal nerve fiber layer in patients with multiple sclerosis. Eur. J. Ophthalmol. 2010, 20, 167–173. [Google Scholar] [CrossRef]
- Ramirez, A.I.; de Hoz, R.; Salobrar-Garcia, E.; Salazar, J.J.; Rojas, B.; Ajoy, D.; López-Cuenca, I.; Rojas, P.; Triviño, A.; Ramírez, J.M. The role of microglia in retinal neurodegeneration: Alzheimer’s disease, Parkinson, and glaucoma. Front. Aging Neurosci. 2017, 9, 1–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parisi, V. Correlation between morphological and functional retinal impairment in patients affected by ocular hypertension, glaucoma, demyelinating optic neuritis and Alzheimer’s disease. Semin. Ophthalmol. 2003, 18, 50–57. [Google Scholar] [CrossRef]
- Chouhan, A.K.; Guo, C.; Hsieh, Y.-C.; Ye, H.; Senturk, M.; Zuo, Z.; Li, Y.; Chatterjee, S.; Botas, J.; Jackson, G.R.; et al. Uncoupling neuronal death and dysfunction in Drosophila models of neurodegenerative disease. Acta Neuropathol. Commun. 2016, 4, 62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moschos, M.M.; Markopoulos, I.; Chatziralli, I.; Rouvas, A.; Papageorgiou, S.G.; Ladas, I.; Vassilopoulos, D. Structural and Functional Impairment of the Retina and Optic Nerve in Alzheimer’s Disease. Curr. Alzheimer Res. 2012, 9, 782–788. [Google Scholar] [CrossRef] [PubMed]
- Rodrigo, M.J.; Garcia-Herranz, D.; Subias, M.; Martinez-Rincón, T.; Mendez-Martínez, S.; Bravo-Osuna, I.; Carretero, A.; Ruberte, J.; Garcia-Feijoo, J.; Pablo, L.E.; et al. Chronic Glaucoma Using Biodegradable Microspheres to Induce Intraocular Pressure Elevation. Six-Month Follow-Up. Biomedicines 2021, 9, 682. [Google Scholar] [CrossRef]
- Morrison, J.C.; Moore, C.G.; Deppmeier, L.M.H.; Gold, B.G.; Meshul, C.K.; Johnson, E.C. A rat model of chronic pressure-induced optic nerve damage. Exp. Eye Res. 1997, 64, 85–96. [Google Scholar] [CrossRef]
- Garcia-Herranz, D.; Rodrigo, M.J.; Subias, M.; Martinez-Rincon, T.; Mendez-Martinez, S.; Bravo-Osuna, I.; Bonet, A.; Ruberte, J.; Garcia-Feijoo, J.; Pablo, L.; et al. Novel Use of PLGA Microspheres to Create an Animal Model of Glaucoma with Progressive Neuroretinal Degeneration. Pharmaceutics 2021, 13, 237. [Google Scholar] [CrossRef]
- Rodrigo, M.J.; Cardiel, M.J.; Fraile, J.M.; Mendez-Martinez, S.; Martinez-Rincon, T.; Subias, M.; Polo, V.; Ruberte, J.; Ramirez, T.; Vispe, E.; et al. Brimonidine-LAPONITE® intravitreal formulation has an ocular hypotensive and neuroprotective effect throughout 6 months of follow-up in a glaucoma animal model. Biomater. Sci. 2020, 8, 6246–6260. [Google Scholar] [CrossRef]
- Ding, C.; Wang, P.; Tian, N. Effect of general anesthetics on IOP in elevated IOP mouse model. Exp. Eye Res. 2011, 92, 512–520. [Google Scholar] [CrossRef] [Green Version]
- Nadal-Nicolás, F.M.; Vidal-Sanz, M.; Agudo-Barriuso, M. The aging rat retina: From function to anatomy. Neurobiol. Aging 2018, 61, 146–168. [Google Scholar] [CrossRef]
- Liu, X.; Wang, C.H.; Dai, C.; Camesa, A.; Zhang, H.F.; Jiao, S. Effect of contact lens on optical coherence tomography imaging of rodent retina. Curr. Eye Res. 2013, 38, 1235–1240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pang, I.H.; Clark, A.F. Inducible rodent models of glaucoma. Prog. Retin. Eye Res. 2020, 75. [Google Scholar] [CrossRef]
- Choh, V.; Gurdita, A.; Tan, B.; Prasad, R.C.; Bizheva, K.; Joos, K.M. Short-term moderately elevated intraocular pressure is associated with elevated scotopic electroretinogram responses. Investig. Ophthalmol. Vis. Sci. 2016, 57, 2140–2151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, B.; Gurdita, A.; Choh, V.; Joos, K.M.; Prasad, R.; Bizheva, K. Morphological and functional changes in the rat retina associated with 2 months of intermittent moderate intraocular pressure elevation. Sci. Rep. 2018, 8, 7727. [Google Scholar] [CrossRef] [PubMed]
- Summers Rada, J.A.; Shelton, S.; Norton, T.T. The sclera and myopia. Exp. Eye Res. 2006, 82, 185–200. [Google Scholar] [CrossRef] [PubMed]
- Harper, A.R.; Summers, J.A. The Dynamic Sclera: Extracellular Matrix Remodeling in Normal Ocular Growth and Myopia Development. Exp. Eye Res. 2015, 133, 100–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, B.; MacLellan, B.; Mason, E.; Bizheva, K. Structural, functional and blood perfusion changes in the rat retina associated with elevated intraocular pressure, measured simultaneously with a combined OCT+ERG system. PLoS ONE 2018, 13, e0193592. [Google Scholar] [CrossRef] [Green Version]
- Frankfort, B.J.; Kareem Khan, A.; Tse, D.Y.; Chung, I.; Pang, J.J.; Yang, Z.; Gross, R.L.; Wu, S.M. Elevated intraocular pressure causes inner retinal dysfunction before cell loss in a mouse model of experimental glaucoma. Investig. Ophthalmol. Vis. Sci. 2013, 54, 762–770. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campbell, I.C.; Hannon, B.G.; Read, A.T.; Sherwood, J.M.; Schwaner, S.A.; Ethier, C.R. Quantification of the efficacy of collagen cross-linking agents to induce stiffening of rat sclera. J. R. Soc. Interface 2017, 14, 20170014. [Google Scholar] [CrossRef]
- Cone-Kimball, E.; Nguyen, C.; Oglesby, E.N.; Pease, M.E.; Steinhart, M.R.; Quigley, H.A. Scleral structural alterations associated with chronic experimental intraocular pressure elevation in mice. Mol. Vis. 2013, 19, 2023–2039. [Google Scholar]
- Pruett, R.C. Progressive myopia and intraocular pressure: What is the linkage? A literature review. Acta Ophthalmol. Suppl. 1988, 185, 117–127. [Google Scholar] [CrossRef]
- Shen, L.; You, Q.S.; Xu, X.; Gao, F.; Zhang, Z.; Li, B.; Jonas, J.B. Scleral and Choroidal Thickness in Secondary High Axial Myopia. Retina 2016, 36, 1579–1585. [Google Scholar] [CrossRef]
- Jonas, J.B.; Holbach, L.; Panda-Jonas, S. Histologic differences between primary high myopia and secondary high myopia due to congenital glaucoma. Acta Ophthalmol. 2016, 94, 147–153. [Google Scholar] [CrossRef] [Green Version]
- Yassin, S.A. Long-Term Visual Outcomes in Children with Primary Congenital Glaucoma. Eur. J. Ophthalmol. 2017, 27, 705–710. [Google Scholar] [CrossRef]
- Liu, B.; McNally, S.; Kilpatrick, J.I.; Jarvis, S.P.; O’Brien, C.J. Aging and ocular tissue stiffness in glaucoma. Surv. Ophthalmol. 2018, 63, 56–74. [Google Scholar] [CrossRef]
- Downs, J.C. Optic nerve head biomechanics in aging and disease. Exp. Eye Res. 2015, 133, 19–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nissirios, N.; Chanis, R.; Johnson, E.; Morrison, J.; Cepurna, W.O.; Jia, L.; Mittag, T.; Danias, J. Comparison of anterior segment structures in two rat glaucoma models: An ultrasound biomicroscopic study. Invest. Ophthalmol. Vis. Sci. 2008, 49, 2478–2482. [Google Scholar] [CrossRef] [Green Version]
- Morrison, J.C.; Cepurna, W.O.; Johnson, E.C. Modeling glaucoma in rats by sclerosing aqueous outflow pathways to elevate intraocular pressure. Exp. Eye Res. 2015, 141, 23–32. [Google Scholar] [CrossRef] [Green Version]
- Sudhalkar, A.; Bilgic, A.; Vasavada, S.; Kodjikian, L.; Mathis, T.; De Ribot, F.M.; Papakostas, T.; Vasavada, V.; Vasavada, V.; Srivastava, S.; et al. Current intravitreal therapy and ocular hypertension: A review. Indian J. Ophthalmol. 2021, 69, 236–243. [Google Scholar] [CrossRef] [PubMed]
- Hoguet, A.; Chen, P.P.; Junk, A.K.; Mruthyunjaya, P.; Nouri-Mahdavi, K.; Radhakrishnan, S.; Takusagawa, H.L.; Chen, T.C. The Effect of Anti-Vascular Endothelial Growth Factor Agents on Intraocular Pressure and Glaucoma: A Report by the American Academy of Ophthalmology. Ophthalmology 2019, 126, 611–622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rebolleda, G.; Puerto, B.; De Juan, V.; Gómez-Mariscal, M.; Muñoz-Negrete, F.J.; Casado, A. Optic nerve head biomechanic and IOP changes before and after the injection of aflibercept for neovascular age-related macular degeneration. Investig. Ophthalmol. Vis. Sci. 2016, 57, 5688–5695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guggenheim, J.A.; Creer, R.C.; Qin, X.J. Postnatal refractive development in the Brown Norway rat: Limitations of standard refractive and ocular component dimension measurement techniques. Curr. Eye Res. 2004, 29, 369–376. [Google Scholar] [CrossRef]
- Usui, S.; Ikuno, Y.; Uematsu, S.; Morimoto, Y.; Yasuno, Y.; Otori, Y. Changes in axial length and choroidal thickness after intraocular pressure reduction resulting from trabeculectomy. Clin. Ophthalmol. 2013, 7, 1155–1161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leo, S.W. Scientific Bureau of World Society of Paediatric Ophthalmology and Strabismus (WSPOS) Current approaches to myopia control. Curr. Opin. Ophthalmol. 2017, 28, 267–275. [Google Scholar] [CrossRef] [PubMed]
- Spillmann, L. Stopping the rise of myopia in Asia. Graefe’s Arch. Clin. Exp. Ophthalmol. 2020, 258, 943–959. [Google Scholar] [CrossRef]
- De Jong, P.T.V.M. Myopia: Its historical contexts. Br. J. Ophthalmol. 2018, 102, 1021–1027. [Google Scholar] [CrossRef]
- Kalmann, R.; Mourits, M.P. Prevalence and management of elevated intraocular pressure in patients with Graves’ orbitopathy. Br. J. Ophthalmol. 1998, 82, 754–757. [Google Scholar] [CrossRef] [Green Version]
- Kim, W.S.; Chun, Y.S.; Cho, B.Y.; Lee, J.K. Biometric and refractive changes after orbital decompression in Korean patients with thyroid-associated orbitopathy. Eye 2016, 30, 400–405. [Google Scholar] [CrossRef] [Green Version]
- Huang, A.S.; Li, M.; Yang, D.; Wang, H.; Wang, N.; Weinreb, R.N. Aqueous Angiography in Living Nonhuman Primates Shows Segmental, Pulsatile, and Dynamic Angiographic Aqueous Humor Outflow. Ophthalmology 2017, 124, 793–803. [Google Scholar] [CrossRef] [PubMed]
- Huang, A.S.; Francis, B.A.; Weinreb, R.N. Structural and functional imaging of aqueous humour outflow: A review. Clin. Exp. Ophthalmol. 2018, 46, 158–168. [Google Scholar] [CrossRef] [PubMed]
- Huang, A.S.; Camp, A.; Xu, B.Y.; Penteado, R.C.; Weinreb, R.N.; Huang, A. Aqueous Angiography: Aqueous Humor Outflow Imaging in Live Human Subjects HHS Public Access. Ophthalmology 2017, 124, 1249–1251. [Google Scholar] [CrossRef] [PubMed]
- Lin, K.Y.; Mosaed, S. Ab externo imaging of human episcleral vessels using fiberoptic confocal laser endomicroscopy. J. Ophthalmic Vis. Res. 2019, 14, 275–284. [Google Scholar] [CrossRef]
- Khatib, T.Z.; Meyer, P.A.R.; Lusthaus, J.; Manyakin, I.; Mushtaq, Y.; Martin, K.R. Hemoglobin Video Imaging Provides Novel In Vivo High-Resolution Imaging and Quantification of Human Aqueous Outflow in Patients with Glaucoma. Ophthalmol. Glaucoma 2019, 2, 327–335. [Google Scholar] [CrossRef] [PubMed]
- Jensen, H. Myopia progression in young school children and intraocular pressure. Doc. Ophthalmol. 1992, 82, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Greene, P.R. Mechanical considerations in myopia: Relative effects of accommodation, convergence, intraocular pressure, and the extraocular muscles. Am. J. Optom. Physiol. Opt. 1980, 57, 902–914. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.-Y.; Sun, C.-C.; Lin, Y.-F.; Lin, K.-K. Effects of topical atropine on intraocular pressure and myopia progression: A prospective comparative study. BMC Ophthalmol. 2016, 16, 114. [Google Scholar] [CrossRef] [Green Version]
- Yam, J.C.; Jiang, Y.; Tang, S.M.; Law, A.K.P.; Chan, J.J.; Wong, E.; Ko, S.T.; Young, A.L.; Tham, C.C.; Chen, L.J.; et al. Low-Concentration Atropine for Myopia Progression (LAMP) Study: A Randomized, Double-Blinded, Placebo-Controlled Trial of 0.05%, 0.025%, and 0.01% Atropine Eye Drops in Myopia Control. Ophthalmology 2019, 126, 113–124. [Google Scholar] [CrossRef]
- Biswas, S.; Wan, K.H. Review of rodent hypertensive glaucoma models. Acta Ophthalmol. 2019, 97, e331–e340. [Google Scholar] [CrossRef]
- Schmidl, D.; Schmetterer, L.; Garhöfer, G.; Popa-Cherecheanu, A. Gender Differences in Ocular Blood Flow. Curr. Eye Res. 2015, 40, 201–212. [Google Scholar] [CrossRef] [Green Version]
- Zhou, X.; Xie, J.; Shen, M.; Wang, J.; Jiang, L.; Qu, J.; Lu, F. Biometric measurement of the mouse eye using optical coherence tomography with focal plane advancement. Vis. Res. 2008, 48, 1137–1143. [Google Scholar] [CrossRef] [Green Version]
- Jiang, M.; Wu, P.C.; Fini, M.E.; Tsai, C.L.; Itakura, T.; Zhang, X.; Jiao, S. Single-shot dimension measurements of the mouse eye using SD-OCT. Ophthalmic Surg. Lasers Imaging 2012, 43, 252–256. [Google Scholar] [CrossRef] [PubMed]
- Chou, T.H.; Kocaoglu, O.P.; Borja, D.; Ruggeri, M.; Uhlhorn, S.R.; Manns, F.; Porciatti, V. Postnatal elongation of eye size in DBA/2J mice compared with C57BL/6J mice: In vivo analysis with whole-eye OCT. Investig. Ophthalmol. Vis. Sci. 2011, 52, 3604–3612. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.-H.; Chen, R.I.; Lin, S.C. Myopia and glaucoma: Sorting out the difference. Curr. Opin. Ophthalmol. 2015, 26, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Suwan, Y.; Rettig, S.; Park, S.C.; Tantraworasin, A.; Geyman, L.S.; Effert, K.; Silva, L.; Jarukasetphorn, R.; Ritch, R. Effects of Circumpapillary Retinal Nerve Fiber Layer Segmentation Error Correction on Glaucoma Diagnosis in Myopic Eyes. J. Glaucoma 2018, 27, 1. [Google Scholar] [CrossRef]
- Kansal, V.; Armstrong, J.J.; Pintwala, R.; Hutnik, C. Optical coherence tomography for glaucoma diagnosis: An evidence based meta-analysis. PLoS ONE 2018, 13, e0190621. [Google Scholar] [CrossRef]
- Lozano, D.C.; Twa, M.D. Development of a rat schematic eye from in vivo biometry and the correction of lateral magnification in SD-OCT imaging. Investig. Ophthalmol. Vis. Sci. 2013, 54, 6446–6455. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Westall, C.A.; Dhaliwal, H.S.; Panton, C.M.; Sigesmun, D.; Levin, A.V.; Nischal, K.K.; Héon, E. Values of electroretinogram responses according to axial length. Doc. Ophthalmol. 2001, 102, 115–130. [Google Scholar] [CrossRef]
- Liu, H.-H.; He, Z.; Nguyen, C.T.O.; Vingrys, A.J.; Bui, B.V. Reversal of functional loss in a rat model of chronic intraocular pressure elevation. Ophthalmic Physiol. Opt. 2017, 37, 71–81. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Time | OCT Protocol | Sector | ONT (Mean ± SD in μm) | OHT (Mean ± SD in μm) | D% | p * | OHT Groups (Mean ± SD in μm) | p † | |
|---|---|---|---|---|---|---|---|---|---|
| 8 W | R | Central | 277.20 ± 17.86 | 263.21 ± 22.03 | −5.05 | 0.022 | MS | 263.80 ± 22.89 | 0.022 |
| ES | 260.30 ± 17.86 | ||||||||
| Temporal Inner | 244.70 ± 8.35 | 251.90 ± 18.50 | +2.86 | 0.047 | MS | 250.78 ± 14.82 | 0.047 | ||
| ES | 257.50 ± 31.74 | ||||||||
| Inferior Outer | 239.90 ± 6.19 | 250.50 ± 11.13 | +4.23 | 0.003 | MS | 251.40 ± 11.34 | 0.003 | ||
| ES | 246.00 ± 9.30 | ||||||||
| Nasal Outer | 243.30 ± 4.34 | 253.60 ± 12.85 | +4.06 | 0.002 | MS | 253.96 ± 11.84 | 0.002 | ||
| ES | 251.90 ± 17.60 | ||||||||
| Superior Outer | 246.30 ± 4.19 | 256.86 ± 17.28 | +4.13 | 0.017 | MS | 257.04 ± 16.69 | 0.017 | ||
| ES | 256.00 ± 20.89 | ||||||||
| Temporal Outer | 245.00 ± 6.48 | 254.10 ± 16.10 | +3.58 | 0.013 | MS | 253.12 ± 12.17 | 0.013 | ||
| ES | 259.00 ± 29.37 | ||||||||
| GCL | Central | 19.80 ± 3.39 | 17.03 ± 3.34 | −13.99 | 0.014 | MS | 16.78 ± 3.27 | 0.014 | |
| ES | 18.30 ± 3.62 | ||||||||
| Superior Inner | 24.10 ± 1.85 | 20.91 ± 4.03 | −13.24 | 0.004 | MS | 20.53 ± 4.04 | 0.004 | ||
| ES | 22.80 ± 3.61 | ||||||||
| 12 W | R | Central | 285.33 ± 18.90 | 266.00 ± 16.73 | −6.76 | 0.039 | MS | 267.33 ± 17.21 | 0.039 |
| ES | 265.56 ± 17.61 | ||||||||
| 24 W | RNFL | Nasal Superior | 39.27 ± 7.25 | 28.88 ± 11.99 | −26.46 | 0.036 | MS | 31.00 ± 10.66 | 0.050 |
| ES | 27.60 ± 13.10 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mendez-Martinez, S.; Martínez-Rincón, T.; Subias, M.; Pablo, L.E.; García-Herranz, D.; Feijoo, J.G.; Bravo-Osuna, I.; Herrero-Vanrell, R.; Garcia-Martin, E.; Rodrigo, M.J. Influence of Chronic Ocular Hypertension on Emmetropia: Refractive, Structural and Functional Study in Two Rat Models. J. Clin. Med. 2021, 10, 3697. https://doi.org/10.3390/jcm10163697
Mendez-Martinez S, Martínez-Rincón T, Subias M, Pablo LE, García-Herranz D, Feijoo JG, Bravo-Osuna I, Herrero-Vanrell R, Garcia-Martin E, Rodrigo MJ. Influence of Chronic Ocular Hypertension on Emmetropia: Refractive, Structural and Functional Study in Two Rat Models. Journal of Clinical Medicine. 2021; 10(16):3697. https://doi.org/10.3390/jcm10163697
Chicago/Turabian StyleMendez-Martinez, Silvia, Teresa Martínez-Rincón, Manuel Subias, Luis E. Pablo, David García-Herranz, Julian García Feijoo, Irene Bravo-Osuna, Rocío Herrero-Vanrell, Elena Garcia-Martin, and María J. Rodrigo. 2021. "Influence of Chronic Ocular Hypertension on Emmetropia: Refractive, Structural and Functional Study in Two Rat Models" Journal of Clinical Medicine 10, no. 16: 3697. https://doi.org/10.3390/jcm10163697
APA StyleMendez-Martinez, S., Martínez-Rincón, T., Subias, M., Pablo, L. E., García-Herranz, D., Feijoo, J. G., Bravo-Osuna, I., Herrero-Vanrell, R., Garcia-Martin, E., & Rodrigo, M. J. (2021). Influence of Chronic Ocular Hypertension on Emmetropia: Refractive, Structural and Functional Study in Two Rat Models. Journal of Clinical Medicine, 10(16), 3697. https://doi.org/10.3390/jcm10163697